
Abstract
Rheumatoid arthritis (RA) is a chronic, inflammatory autoimmune disease marked by joint destruction and functional impairment. Tumor necrosis factor (TNF) plays a critical role in RA pathogenesis. Although TNF-targeting drugs are clinically effective, their need for frequent and long-term administration often results in poor patient adherence and suboptimal outcomes. This study developed a gene therapy approach using engineered adeno-associated virus (AAV) vectors to deliver an anti-TNF agent directly into the joint cavity of RA animal models. Animals receiving this therapy demonstrated sustained improvement in clinical scores, inflammatory markers, and joint tissue health. Immunofluorescence staining revealed that AAV vectors could transduce various cell types, including T cells, type A synoviocytes, and dendritic cells. Our results indicate that a single administration of this gene therapy provided long-term efficacy. This suggests that AAV-mediated anti-TNF gene therapy can offer prolonged relief from clinical symptoms and reduce inflammatory damage in a mouse model of RA. This innovative approach presents a promising new therapy with significant clinical prospects to treat patients with RA.
INTRODUCTION
Rheumatoid arthritis (RA) is a chronic autoimmune disease characterized by the production of autoantibodies against IgG, known as rheumatoid factor. 1 Epidemiological data suggest that RA has a prevalence of approximately 0.5–1.0% for RA, with no significant variation across populations. 2,3 However, the prevalence is approximately 2–3 times higher in females than in males. 4 Despite significant advancements in RA treatment, achieving ideal outcomes remains challenging due to the chronic nature of the disease, which requires long-term and regular treatment.
RA is a systemic disease, but it primarily affects the joints, with the synovium playing a key role. The proliferation and activation of synoviocytes leads to synovial hyperplasia, resulting in the production of various cytokines and proteases, such as IL-1, IL-6, and TNF, 5,6 triggering local inflammation within the joint cavity and surrounding tissues. In addition, many adaptive immune cells, predominantly CD4+ T cells, infiltrate the synovial sublining and adjacent tissues, forming ectopic germinal centers where mature B cells proliferate and induce the production of rheumatoid factor and anticitrullinated protein antibodies. The characteristic pathological hallmark of RA is the synovial invasion into adjacent articular structures, manifesting as synovial hyperplasia and enhanced vascularity, which ultimately results in the degradation of cartilage and bone. 7,8 Consequently, patients experience significant pain and restricted joint movement, leading to an increased risk of mortality. 9
Currently, there is no cure for RA. Therapeutic approaches primarily focus on reducing joint swelling, alleviating pain, and controlling disease progression. 10 Nonsteroidal anti-inflammatory drugs (NSAIDs), steroids, and chemical and biological disease-modifying antirheumatic drugs (DMARDs) are commonly used. 11 Among these, targeted biological agents exhibit higher specificity, with anti-TNF agents being the most widely utilized. However, the need for frequent and long-term administration leads to poor patient compliance and suboptimal treatment outcomes. Furthermore, biological DMARDs may pose risks of inducing serious infections and lung disease in certain circumstances, 12 –14 raising safety concerns, especially with systemic use. Therefore, treatment modalities with low adverse effects are urgently needed in clinical practice.
Gene therapy is one of the most promising therapeutic approaches that is being developed. It involves delivering target genes into the patient’s cells to achieve long-term and effective disease relief. While many gene therapies are delivered systemically, they can be administered locally to deliver therapeutic genes directly to the disease site and minimize effects on other organs. Adeno-associated virus (AAV) belongs to the parvoviridae family and has been successfully applied in clinical therapies with numerous clinical trials underway. 15 AAV vectors have been shown to deliver therapeutic genes which can achieve long-term gene expression. 16 Both natural and engineered AAVs exhibit tissue-specific transduction to a certain extent. One approach to delivering RA gene therapy is engineering capsids to target bone and joint tissues while de-targeting other tissues, which could allow vectors to be administered systemically. However, local administration of AAV vectors is better able to confine tranduction to the lesion sites, allowing therapeutic agents to achieve high local concentrations and reducing exposure of other organs to the vector, which minimizes side effects and can lessen the need for additional medications such as immunosuppressants. This approach significantly enhances the safety of treatment while ensuring therapeutic efficacy.
METHODS AND MATERIALS
Cell lines
HEK293 cells were purchased from the American Type Culture Collection (ATCC; CCL-131) and maintained in Eagle’s Minimum Essential Medium (ATCC 30–2003) supplemented with 10% fetal bovine serum (FBS, HyClone). Cells were cultured in a humidified 37°C/5% CO2 incubator. For in vitro expression assays with different anti-TNF cDNA constructs, cells were seeded 18–24 h before transfection at a density of 5 × 105 cells/well in a six-well plate. Cells were transfected with Lipofectamine 2000 (Thermo Fisher Scientific) in accordance with the manufacturer’s instructions. Cells were harvested 72 h post-transfection and the cell culture media was collected and prepared for enzyme-linked immunosorbant assay (ELISA) analysis.
Viral vector production
The recombinant AAV vector was produced using a triple-plasmid transfection approach 17 and HEK293 cells were used as the packaging cell line. The pHelper pRC plasmids encoding AAV2 Rep and Cap proteins for AAV5, 6, 8 or AAV.v128 and the cis-plasmids carrying anti-TNF-α or luciferase/mCherry transgenes were used to generate the AAV vectors in this study. All transgenes were driven by the chicken beta-actin (CB) promoter.
The cells were seeded in 150 mm plates overnight and then co-transfected with the pHelper, pRC, and cis plasmids at a molar ratio of 1:1:1. The cells were harvested 72 h after transfection by centrifugation at 1,500 × g at 4°C for 15 min. The cell pellet was resuspended in the lysis buffer (150 mM NaCl, 20 mM EDTA, and 20 mM Tris-HCl) and the rAAV particles were released by three freeze-thaw cycles. The crude lysate was treated with Benzonase and 10% deoxycholic acid at 37°C for 1 h to remove the unpackaged rAAV DNA. The lysate was centrifuged at 10,000 × g for 30 min to remove the cellular debris. Affinity chromatography (Thermo, USA, POROS™ CaptureSelect™ AAVX Affinity Resin, #A36745) and subsequent anion exchange chromatography were used to purify the recombinant AAV vectors. Vector preparations (vg/mL) were titered by digital droplet polymerase chain reaction (ddPCR).
Animals
DBA/1 mice and New Zealand rabbits were purchased from Charles River Laboratores. Animal husbandry and all animal experiments were conducted at the Beijing Match Medicine Research Institute Co., Ltd. All animal experiment were approved by the Institutional Animal Care and Use Committee of this Institute.
Animals were housed in standard animal rooms with a temperature range of 20–26°C, humidity of 40–70%, and a 12 h light:12 h dark photoperiod. Food and water were provided ad libitum. Male mice aged 6–8 weeks were used for the experiments and were randomly assigned to groups.
Under sterile conditions, type II collagen (CII; Chondrex, catalog #: 20022) was emulsified with an equal volume of complete Freund’s adjuvant (Chondrex, catalog #: 7008) to prepare a CII collagen emulsion. Each mouse received a subcutaneous injection of 100 μL of the CII collagen emulsion (containing 0.1 mg of CII) at the base of the tail on day 1. On day 21, a booster immunization of CII collagen emulsion was injected subcutaneously at the same site with the same volume. The control group was not treated. Successful model establishment was indicated by observing varying degrees of redness and swelling in the mice’s ankle joints, wrist joints, and paws after the booster immunization.
AAV vectors were administrated in a 10 μL volume by either intra-articular injection directly into the ankle joint or intramuscular injection into the tibialis muscle and Adalimumab was injected subcutaneously in a volume of 100 μL. Mice were monitored daily and the clinical score of each animal was determined following previously published criteria. 18 The primary indicators of RA in this model include the appearance of the erythema as well as the degree and extent of swelling (please refer to Supplementary Table S1 for detailed information). The Digital Radiography (DR) clinical score was evaluated as well, briefly each mouse underwent X-ray imaging using the Digital Veterinary X-Ray System (VDR-1800, Suzhou VetRay Medical Equipment Co., Ltd.). Radiological analysis was evaluated based on joint swelling, bone erosion, and joint space, using a scoring system ranging from 0 to 3 (0 = normal, 1 = mild changes, 2 = moderate changes, 3 = severe changes). 19 The radiological assessments were scored by independent observers who were blind to the treatment groups.
Male New Zealand rabbits aged 12–13 weeks were used. Intra-articular injections were administered using a syringe, with a volume of 50 μL per injection. Synovial fluid was extracted from the joint cavities at different time points for analysis.
In vivo bioluminescence imaging
Mice were injected with AAV-Luciferase into the tibialis muscle at dosage of 8.08E9 vg/mouse or into the ankle joint at dosage of 1E11 vg/joint. Animals were anesthetized with ketamine/xylazine before bioluminescence imaging. A volume of 200 μL D-Luciferin (Thermo Fisher, catalog #: L2916) at a dose of 150 mg/kg was administered intraperitoneally into each mouse and bioluminescence images were captured 10 minutes later with the animals still under ketamine/xylazine anesthesia using a luminescence imager (Xenogen, IVIS Imaging System 200). In vivo bioluminescence imaging was performed from day 4 to day 235 post-vector injection.
Tissue collection and staining
At the end of the experiment mice were euthanized, then the ankle joints were collected and immediately fixed in 10% formaldehyde for 24 h. Afterwards, the samples were dehydrated in a sucrose solution and embeded in paraffin. Tissue sections (6 μm) were cut from each tissue block and staining was performed.
For the H&E staining
The paraffin slides were dewaxed by placing them in xylene I solution and xylene II solution 5 min each. Then, the slices were incubated in 100%, 95%, 80%, and 75% ethanol solutions for 5 min each, rinsed with distilled water, and dried. The paraffin sections were stained with hematoxylin for 3–5 min, rinsed with water for 15 min, and then dried. Slices were immersed in hematoxylin staining solution for 3–5 min, rinsed with water, then incubated in 1% hydrochloric acid ethanol differentiation liquid solution for 5–30 s until the sample started turning red, then rinsed with tap water again, counterstained in fast green solution, and rinsed under running water. Slices were transferred into a 95% alcohol for dehydration for 1 min, then stained in eosin staining solution for 15 s.
Slices were sequentially transferred into 100% ethanol I for 2 min, 100% ethanol II for 2 min, 100% ethanol III for 2 min, isopropanol I for 2 min, isopropanol II for 2 min, xylene I for 2 min, xylene II for 2 min for transparency, and finally mounted with neutral mounting medium.
Anti-tartaric-resistant acid phosphatase staining
Tartrate-resistant acid phosphatase (TRAP) staining was performed by using a commercial kit (Wuhan Servicebio Technology CO., LTD, catalog #: G1050). After dewaxing, the slides were put into a wet box and incubated with distilled water at 37°C for 2 h. The distilled water was removed and samples were incubated in a TRAP solution 37°C for 20 min. The dye solution was removed and samples were washed, then incubated in hematoxylin solution to restain the nucleus for 15 s. The slides were then incubated with differentiation fluid and ammonia. Finally, the sampels were dehydrated and sealed with neutral gum.
Safranin O-fast green staining
After dewaxing, the slides were stained in fast green dye solution (Wuhan Servicebio Technology CO., LTD, catalog #: G1053) for 1–5 min, then the excess dye solution was washed away until the cartilage was colorless and samples were incubated in 1% hydrochloric acid and alcohol for 10 s, then washed with tap water. The slides were stained in saffron dye solution for 1–5 s, and then incubated in four absolute ethanol solutions for 5, 2, and 10 s, then kept in the fourth solution. The slides were then immersed in xylene for transparency for 5 min and sealed with neutral gum.
Immunofluorescence staining
After dewaxing, unmasking was performed by placing slides into citrate buffer (catalog #: S2369, Dako) and heating them for 4 min at 100°C. Slides were immersed in a blocking solution (X0909, Dako) for 1 h at room temperature. Then slides were subjected to incubation respectively with rabbit anti-mouse CD68 (catalog #: ab303565, Abcam), rabbit anti-mouse Vimentin (catalog #: ab92547, Abcam), rabbit anti-mouse SOX9 (catalog #: ab185966, Abcam), mouse anti-mouse CD11c (catalog #: ab254183, Abcam), rabbit anti-mouse CD3 (catalog #: ab135372, Abcam), or Goat anti-EGFP (catalog #: OSE00036W, Invitrogen) primary antibodies for 16 h at 4°C. After washing with phosphate-buffered saline (PBS) three times, slides were incubated with a fluorescence conjugated secondary antibody (Alexa Fluor 594 donkey anti-Rabbit IgG, catalog #: A-21207, Invitrogen; Alexa Fluor 488 Donkey Anti-Goat IgG, ab150129, Abcam; Alexa Fluor 594 Goat Anti-Mouse, catalog #: ab150116, Abcam) for 1 h. Samples were then washed in PBS three times, dried, and sealed with coverslips. The slides were imaged using a fluorescence microscope system (Zeiss).
Flow cytometry analysis
Animals’ ankle joint fluid and popliteal lymph nodes were collected and the M1, M2 macrophage and CD4+ T cell counts were determined by using flow cytometry assay. The lymph nodes were cut into small pieces and gently pressed through a strainer. Samples were resuspended in PBS buffer and centrifuged at 1,000 rpm for 10 min at 4°C. The cell pellet was disaggregated by adding 5 mL of ACK lysis buffer, followed by resuspension and incubation on ice for 5 min to lyse red blood cells. All processed lymph nodes samples and joint fluid samples were washed with cold 1× PBS and resuspended in 10 mL of 1X PBS with 10% FBS. For staining, cells were incubated with antibodies: PE anti-mouse F4/80 (BioLegend, catalog #: 111603), PerCP-Cy5.5 anti-mouse CD11b (BioLegend, catalog #: 101227), APC anti-Nos2 20 (BioLegend, catalog #: 696807), and FITC anti-mouse CD206 (BioLegend, catalog #: 141703) for macrophages; FITC anti-mouse CD3 (BioLegend, catalog #: 100230) and APC anti-mouse CD4 (BioLegend, catalog #: 100411) for CD4+ T cells. Samples were incubated for 30 min at 4°C, then washed with 10% bovine serum albumin (BSA) in 1× PBS. After being stained, cells were fixed with 4% paraformaldehyde (PFA) at 4°C for 20 min followed by being washed twice with 10% BSA in 1× PBS. Stained cells were analyzed with a FACScanto Flow Cytometer and the results were processed with FlowJo software.
ELISA assay
Animals’ ankle joint tissues were immediately snap-frozen in liquid nitrogen, tissues were ground in liquid nitrogen and homogenized after being collected. After centrifugation, the pellet was discarded and then IL-6 (BioLegend, catalog #: 431307) and IL-1β (BioLegend, catalog #: 432604) kits were used to measure the cytokine levels in the supernatant.
Statistical analysis
All quantitative data are presented as mean ± standard error of the mean (SEM). GraphPad Prism 8 software was used to visualize the data. For data that are normally distributed and have homogeneity of variance, one-way analysis of variance (ANOVA) was used for statistical testing. For data that are not normally distributed or have heterogeneity of variance, the Kruskal–Wallis H test was used for statistical analysis. The Mann–Whitney U test was used to compare differences between groups. Values of p ≤0.05 were considered to be statistically significant.
RESULTS
In situ delivery of an AAV vector confers persistent expression of anti-TNF in animal joints
We developed a variety of constructs containing the full-length anti-TNF cDNA driven by the CB promoter. The anti-TNF amino acid sequences were identical to those in adalimumab or etanercept, and the anti-TNF cDNA sequences were codon-optimized for enhanced expression efficiencies (Fig. 1A). These constructs were transiently transfected into HEK293 cells to assess expression efficiency, and the construct with the highest expression of the etanercept protein was selected for further experiments (Fig. 1B).

Local injection of AAV gene therapy vectors confer persistent transgene expression in mice. (
AAV serotypes exhibit varied tissue tropisms, meaning that different AAV serotypes transduce tissues with different efficiencies. Thus, identifying an AAV serotype with high transduction efficiency for the target tissue is crucial. To date, AAV5, 6, and 8 have been to show to transduce multiple tissues to varying extents, but show superior transduction efficiencies in the cartilage tissue. 21 Previously, we developed a novel AAV capsid (AAV.v128) through rational design, which demonstrated high transduction efficiency in multiple tissues. 22 We sought to evaluate transduction efficiencies of this novel capsid compared to AAV5, 6, and 8, and so we packaged the licuferase reporter gene into these capsids. These AAV vectors were injected into the tibialis muscle of the mice and the transduction efficiencies were monitored over 235 days by live fluorescence imaging. Our results indicate that AAV.v128 had the highest transduction efficiency among the AAV serotypes tested. Subsequently, these AAV serotypes were injected into the ankle joints of mice and fluorescence was measured for 2 months, and AAV.v128 again showed the highest transduction efficiency. Notably, the luciferase signal was confined to the injection site and surrounding areas in both experiments, with no significant spread to other tissues or organs. (Fig. 1C and D).
The anti-TNF expression cassette was packaged into the AAV.v128 capsid to create the AAV.v128-anti-TNF recombinant vector, which was designated as KH656. In clinical practice, therapeutic drugs are typically delivered locally into the diseased joint. 23 Thus, we directly injected this vector into the knee joint cavity of New Zealand rabbits (1E11 vg/joint, Fig. 1E). The anti-TNF expression level in animals’ joint fluid was monitored over a 9 months, and showed successful and stable expression of the anti-TNF protein in the knee joint cavity (Fig. 1F). This result indicates that intra-articular injection of the AAV.v128 vector is an effective strategy for delivering a transgene into joint tissue, which has great potential for treating RA.
Intra-articular injection of AAV.v128 vector primarily transduce type a synovial cells, dendritic cells (DCs), and T cells
The joint cavity is mainly composed of chondrocytes, type A synovial cells, type B synovial cells, and immune cells, including DCs and T cells. 24,25 To determine which cell types are transduced by this engineered AAV, we packaged the reporter gene mCherry into the AAV.v128 capsid and injected it into the ankle joint cavity of mice. After 2 weeks, we harvested the ankle joint tissues and conducted immunofluorescence staining. The results indicate that AAV.v128 primarily transduces type A synovial cells, DCs, and T cells, whereas it shows little ability to transduce chondrocytes or type B synovial cells (Fig. 2).
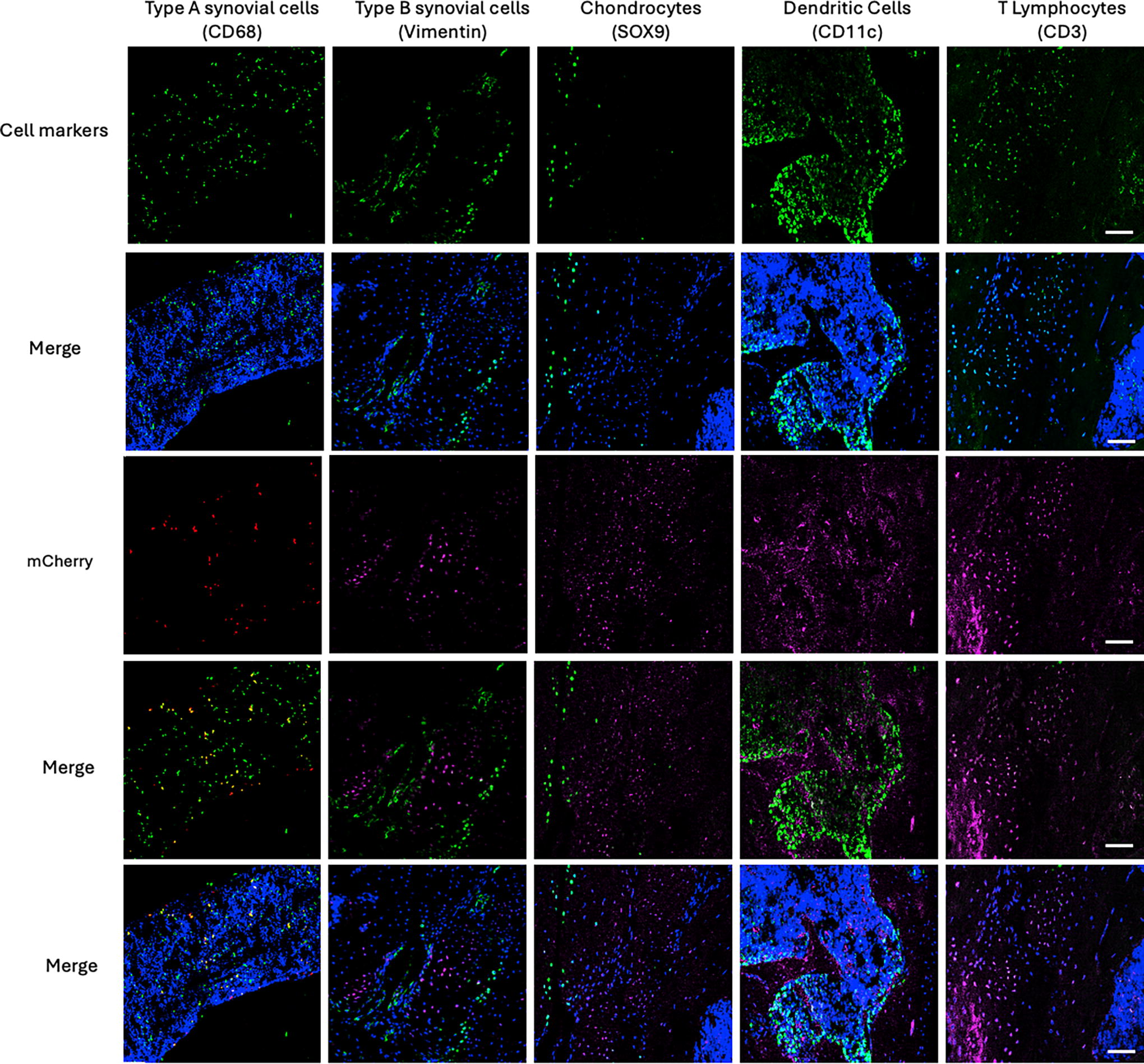
Intra-articular injection of AAV.v128 vector primarily transduces type A synovial cells, DCs, and T cells in ankle joint tissues of mice. A gene encoding mCherry was packaged into the AAV.v128 capsid to create the AAV.v128-mCherry, this vector was injected into mice ankle joint cavities. Two weeks later, animals’ ankle joint tissues were collected and immunofluorescence staining was performed with cell markers to examine transgene expression in different cell types. Images are representative of five independent experiments. Red: mCherry; Green: indicated cell markers. Scale bar = 50 μm. AAV, adeno-associated virus; DCs, dendritic cells.
Anti-TNF gene therapy greatly inhibited inflammation response in a collagen-induced RA animal model
We next established a collagen-induced RA model to test the therapeutic potency of our KH656 gene therapy approach. We treated each mouse with collagen for 21 days to induce RA-like symptoms, then administrated KH656 at a dosage of 1E11 vg/joint and adalimumab, a widely used monoclonal antibody that is widely used in clinical treatment of RA, as a positive control. We established two groups: one received intramuscular (i.m) injection into the tibialis muscle and the other received intra-articular (i.a) injection directly into the ankle joint on day 22. The control group received subcutaneous injection of adalimumab twice on days 22 and 37 (Fig. 3A).
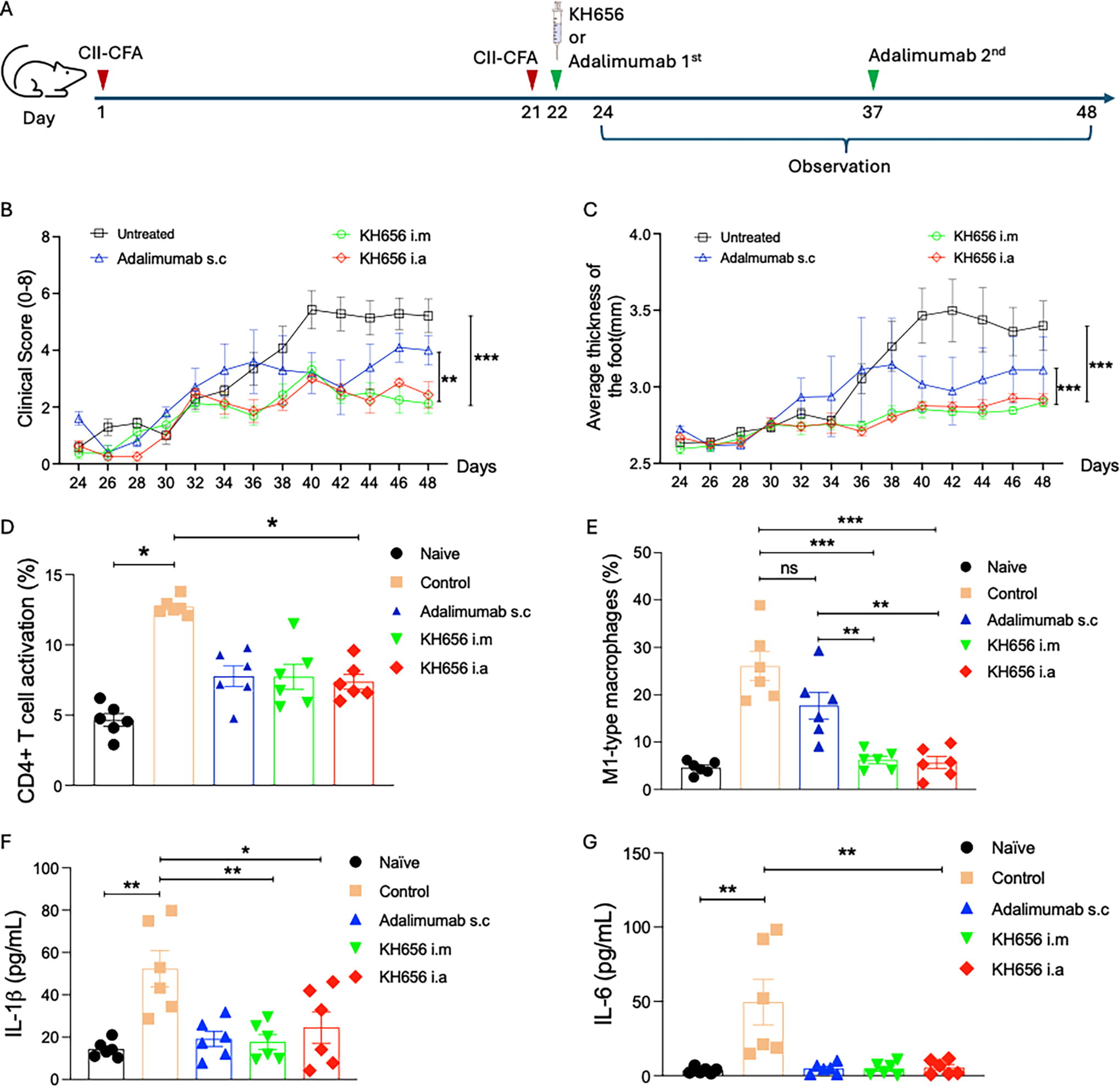
AAV.v128-anti-TNF gene therapy greatly inhibited inflammation response in a collagen-induced RA mice model. (
Both KH656-treated groups showed reduced symptoms, as evidenced by assessment of clinical scores and average paw thickness on day 36. In contrast, the adalimumab-treated group did not show any therapeutic benefit until the second injection (day 38). At the end of the observation period (day 48), the KH656-treated groups (both i.m and i.a) maintained persistent clinical benefit and demonstrated better therapeutic outcomes than the adalimumab-treated group (Fig. 3B, C).
We determined the levels of inflammatory markers, including macrophage infiltration, CD4+ T cell activation, and secretion of IL-6 and IL-1β. Our results show that the collagen treatment induced significant macrophage infiltration and cytokine secretion in the ankle joint tissues along with CD4+ T cell proliferation in adjacent lymph nodes. The treatment group exhibited only slight increases in these inflammatory biomarkers (Fig. 3D–G). Notably, KH656-treated animals showed lower macrophage infiltration compared to the adalimumab-treated group (Fig. 3E). These data indicate that local gene delivery of an anti-TNF factor efficiently combated the inflammatory response in animals’ ankle joints.
Ankle joints were collected at the endpoint and examined using H&E staining to assess pathological changes. As shown in Figure 4A, we noticed that collagen treatment resulted in significant pathologies including damaged tissues structures, neutrophils and lymphocytes infiltration (red arrows), synovial, moderate connective tissue proliferation, and neovascularization in the ankle joint cavities (green arrows). Necrotic foci were occasionally seen in the synovium and talus along with necrosis of the connective tissue and goblet cells and nuclear debris (blue arrows). There was connective tissue proliferation around the periosteum (purple arrow), which was accompanied by neutrophil infiltration. These pathological features closely resemble clinical RA. 24 Treatment with our KH656 vector or adalimumab significantly ameliorated these pathologies, resulting in a cleaner joint cavity, smoother cartilage surface, and abundant, orderly chondrocytes, which are observed in healthy tissue (Fig. 4A top row).
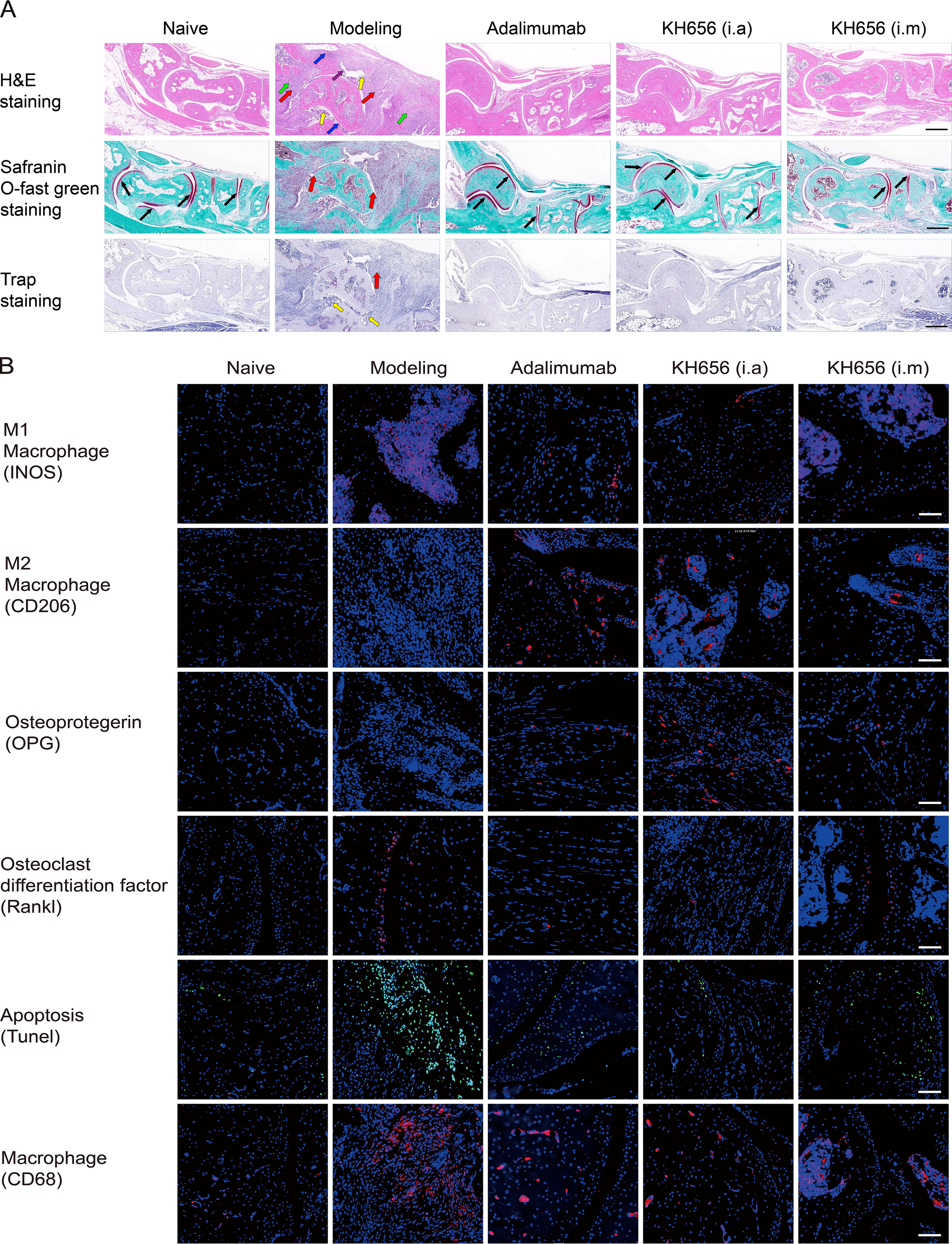
AAV.v128-anti-TNF gene therapy prevented ankle joint tissue damage in RA mice models. Animals were sacrificed at day 48 and the ankle joint tissues were collected. (
Safranin O-fast green staining was conducted to assess cartilage damage in mouse ankle joints. In the collagen-treated group, articular cartilage showed surface irregularities, decreased faintly red chondrocytes (red arrows), reduced extracellular matrix, irregular arrangement, and tissue debris. Post-treatment, the ankle joints showed richly stained red chondrocytes in a regular arrangement with no detectable debris and smooth cartilage surface. There were no significant pathological differences between the adalimumab group and the two KH656 treatment groups (Fig. 4A middle row).
TRAP staining was performed to assess changes in osteoclasts in animals’ ankle joints. In collagen-treated mice, pale red osteoclasts were noted on the cartilage surface, with increased numbers and irregular arrangement (yellow and red arrows). Mice treated with adalimumab or KH656 showed no significant differences from the control group (Fig. 4A bottom row).
In RA patients, inflammation usually leads to increased macrophage levels where M1 macrophages secrete pro-inflammatory cytokines and M2 macrophages secrete anti-inflammatory cytokines. 26 Collagen-treated mice exhibited a significant increase in ankle joint macrophages, whcih were predominantly M1 macrophages. Following treatment, total and M1 macrophages decreased markedly, whereas M2 macrophages increased (Fig. 4B). This effect was more pronounced in the KH656 treatment group compared to the adalimumab group, with no significant difference between the i.a and i.m subgroups. Osteoprotegerin and osteoclast differentiation factor are crucial biomarkers reflecting bone destruction. Osteoprotegerin inhibits osteoclast differentiation, suppresses bone resorption, and prevents apoptosis, indicating bone activity. Conversely, osteoclast differentiation factor promotes osteoclast precursor growth and proliferation, enhances osteoclast activity, and increases cell apoptosis. 20 We found a significant increase in osteoprotegerin staining in the ankle joints of the KH656 treatment group compared to the modeling group, with the i.a subgroup showing higher levels than the i.m subgroup and the adalimumab group. The RA model group showed a significant increase in osteoclast differentiation factor and apoptotic cell count compared to untreated healthy mice, and these indicators were significantly inhibited in all of the treatment groups, with no significant difference among the three groups. These results demonstrate that AAV-based gene therapy for RA effectively alleviates clinical symptoms and suppresses immune responses in mouse ankle joints (Fig. 4B).
AAV-anti-TNF gene therapy substantially alleviate clinical symptoms in animal models
We next conducted a series of experiments to determine the dosage and the therapeutic window. On day 1, various doses of the KH656 vector were injected directly into the ankle joint cavities of mice: a low-dose group (5E10 vg/joint), a medium-dose group of (1E11 vg/joint), and a high-dose group (2E11 vg/joint). Adalimumab was injected subcutaneously as a positive control three times per week at a dosage of 0.3 mg/kg. Disease modeling was induced by injection of collagen on days 14 and 21. All treated mice were observed daily and paw swelling was measured every other day. DR 27 scores were assessed on day 42 (Fig. 5A).
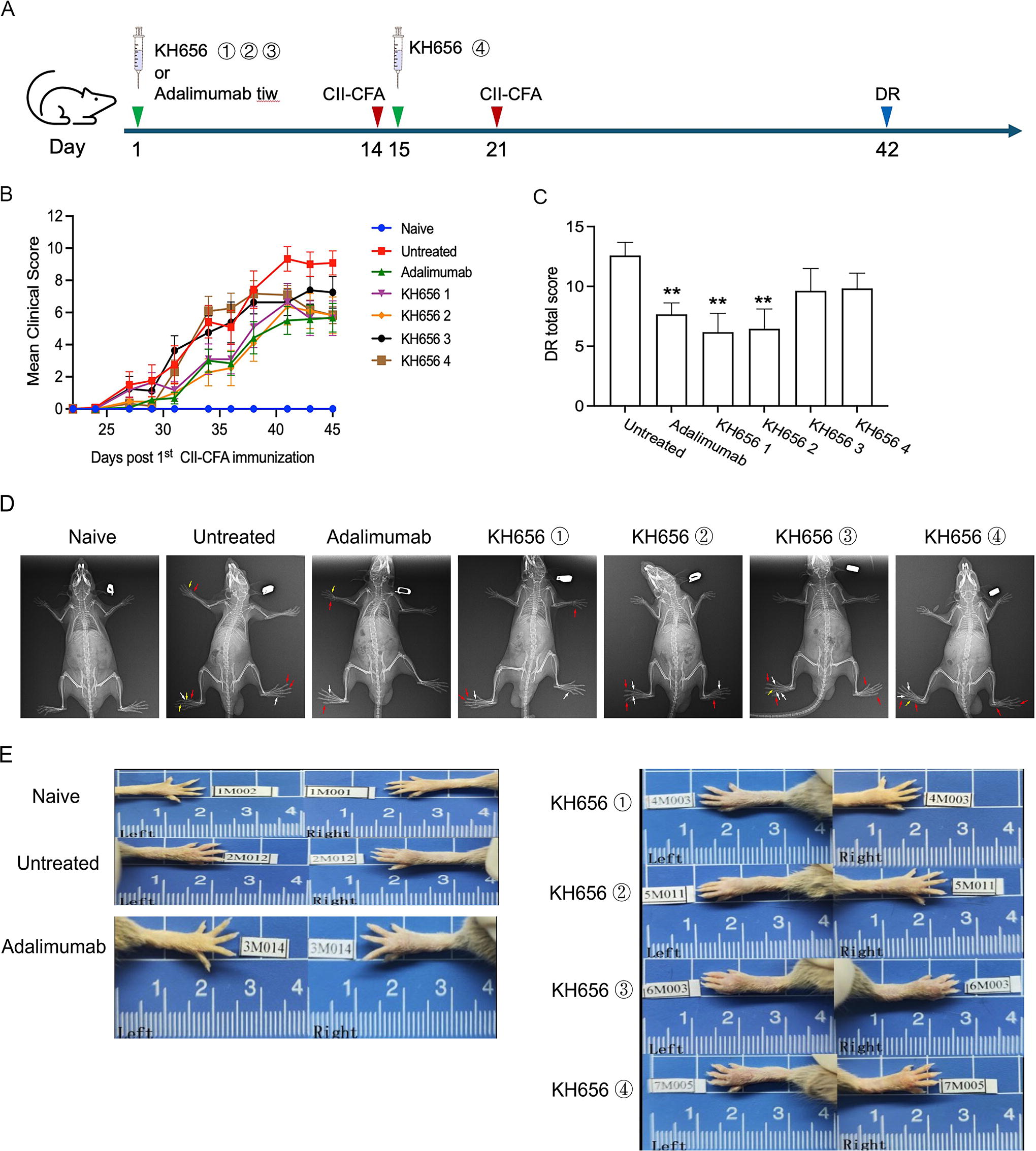
AAV.v128-anti-TNF gene therapy substantially alleviated clinical symptoms in a mouse model. (A) Schematic diagram of the study. Animals were randomly divided into seven groups. We set up four AAV.v128 treatment groups: animals were injected with AAV-anti-TNF at a dosage of 5E10 (Group ①), 1E11 (Group ②), or 2E11 (Group ③) vg/joint directly into the ankle joint cavities on day 1; animals in group ④ were injected on day 15 with dose of 1E11vg/joint also directly into the ankle joint cavities. Animals in the positive control group were treated with adalimumab with 0.3 mg/kg three times per week via subcutaneous injection. Animals were immunized on day 14 and day 21 to induce the RA-like symptoms. Clinical observation was performed daily and DR scores were assessed on day 42. (
The mice began to show varying degrees of paw swelling seven days after collagen induction. Compared to the control group, the collagen-induced mice exhibited significant swelling in their paws and toes. However, all three treatment groups showed remarkable symptom relief compared to the disease modeling controls. Notably, the KH656 low-dose group exhibited the mildest swelling and the best therapeutic effect, whereas the high-dose group showed relatively less efficacy, potentially owing to a host immune response triggered by the high dose of the AAV vector.
The collagen-induced mice began to exhibit redness and swelling of the paws and toes from day 24, with statistically significant difference from the normal control group observed from days 31 to 45 (p < 0.05). In contrast, the treatment groups showed a delayed onset of redness and swelling starting on day 27 for the high-dose KH656 group and the positive control group. These symptoms appeared only from days 41 to 45 in the low-dose treatment group and from days 34 to day 45 in the medium-dose treatment group, with significantly lower clinical scores compared to the modeling control group (p < 0.05), indicating a significant alleviation of the disease (Fig. 5B). The results indicate that all of the treatments could alleviate the increase in paw thickness and the positive control group showed the best therapeutic effect. All KH656 vector-treated mice also experienced a degree of alleviation in paw thickness, with the low-dose group showing the best effect (Fig. 5E).
For DR scoring, the total scores (including joint swelling, bone erosion, and joint space) in the RA modeling group were significantly higher than those in the healthy control group, indicating that pathological changes were induced with the collagen injection. All treatments resulted in symptom relief, such as reduced bone erosion and improved joint space (Fig. 5D), with statistically significant differences observed when comparing the untreated group with the the positive control, low-dose, and moderate-dose groups (Fig. 4C).
In this experiment, we included another group was (group ④) in which collagen was administrated on day 14 and 21 as with other groups, but the KH656 vector was injected into the ankle joint cavities on the day after modeling (day 15) at a dose of 1E11 vg/joint (Fig. 5A). The purpose of this experiment was to investigate whether vector treatment could have a therapeutic effect when administered soon after joint damage had occurred. This treatment also alleviated clinical scores, DR scores, and paw thickness, though not as significantly as the other treatment groups.
In summary, our gene therapy vector KH656 significantly alleviated the progression of RA in a collagen-induced animal model and the efficacy of this approach was comparable to that of the adalimumab antibody. Unexpectedly, the high-dose group showed less effectiveness than the lower dose groups. We hypothesize that in an inflammatory disease state, tissues are hypersensitive and high doses of AAV may induce a tissue immune response, which exacerbates inflammation. Our anti-inflammatory therapy may not fully suppress this immune damage, suggesting that careful dosage selection is necessary when translating AAV gene therapy into clinical applications to balance the therapeutic effects and minimize unwanted side effects.
DISCUSSION
RA is a multifaceted disease primarily driven by the dysregulation of inflammatory cytokines, with Receptor Activator for Nuclear Factor-κ B Ligand (RANKL) playing a pivotal role. RANKL, also known as TNF-related activation-induced cytokine, osteoprotegerin ligand, and osteoclast differentiation factor, is integral to the disease’s progression. 28 In RA, excessive expression of cytokines such as TNF-α, IL-1, IL-6, IL-8, and chemokines via RANKL activates osteoclasts, chondrocytes, and synoviocytes, leading to bone and joint destruction. 29 These cytokines are effective targets for RA treatment, as evidenced by successful treatments using biologics such as Adalimumab and Etanercept, which target TNF-α.
Despite the success of protein-based therapies, the limitations of current RA treatments have prompted the exploration of alternative therapies. RNA silencing technology has led to the development of siRNA-based drugs targeting TNF. Clinical studies of subcutaneously injected siRNAs have shown a 20% reduction in disease activity, with over half of the patients achieving clinical benefits at day 169. Unfortunately, three months after treatment this treatment was not as effective as anti-TNF biologics, indicating that the potency of siRNA is short-lived. 30 In addition, siRNA carries risks of off-target effects and its safety needs to be rigorously evaluated before it can be applied as a possible therapy. Moreover, siRNA can only act at the mRNA level, limiting its impact on TNF protein in joint fluid. Another approach involved using a retroviral vector to introduce an IL1Ra gene into synovial fibroblasts collected from patients’ joints ex vivo and then returned the cells to the metacarpophalangeal joints. 31 Although this relieved clinical symptoms in human trials, safety concerns regarding retroviral vectors halted its progress. 32
AAV-mediated gene therapy has emerged as a promising strategy for RA treatment. Studies have utilized AAV5 to deliver TNF inhibitors and observed positive efficacy in rat models. Researchers have also employed AAV to deliver CD39/CD73 to modulate immune responses as an approach to treat RA. 27 ART-102, which was developed by the Academic Medical Center University of Amsterdam, uses AAV5 to deliver a gene encoding IFN-β and is considered to be a promising gene therapy product. In clinical trials, single intra-articular injections of 0.3E12–1.2E13 vector genomes were administered to the affected hand joints of the patients. However, adverse events such as tenosynovitis occurred in the treated hands, leading to the termination of the trial. Subsequent studies found that patients developed antibodies against AAV5 and IFN-β’s dual role as an anti-inflammatory and pro-inflammatory factor may have contributed to adverse events. 33 Other researchers have attempted to deliver a cDNA equivalent to the biological drug etanercept with AAV vectors, which is considered safe and feasible, 34 and clinical benefits have been observed compared to the control group. 35 However, two severe adverse reactions occurred in clinical trials which resulted in the termination of the trial, even though these adverse reactions were deemed unrelated to the treatment. 36
The success of AAV gene therapies such as Glybera, Luxturna, Zolgensma, Upstaza, Roctavian, Hemgenix, and Elevidys has established that AAV vectors can be safe and effictive, which builds confidence in their potential use for RA treatment. Local joint administration is a promising gene delivery approach for the treatment of RA, as it achieves effective therapeutic concentration at the lesion site and avoids side effects that occur with systemic administration, but acieving high transduction efficiency remains a challenge in intra-articular gene therapy. In our study, we compared the transduction efficiency of multiple AAV capsids in the joint cavity, and our data indicate that our novel AAV.v128 capsid exhibited superior transduction efficiency compared to AAV6 and AAV8. Importantly, it did not show significant leakage to other tissues. We also investigated the cell types that were transduced and found that AAV.v128 effectively transduced type A synovial cells, DCs, and T cells, providing sustained transgene expression for several months. This indicates that it could be a candidate for gene therapy strategies to treat RA.
The collagen-induced arthritis model used in this study closely mirrors human RA pathology. 37 Following collagen induction, untreated mice develop joint swelling and tissue damage along with increased cytokine secretion. Administering KH656 at 5E10 or 1E11 vg/joint before collagen induction effectively suppressed the inflammatory response, alleviating clinical symptoms and pathological damage. AAV was able to achieve sustained expression of the delivered gene, which is necessary for long-lasting treatment of the disease. Higher doses (2E11 vg/joint) partially alleviated symptoms but might induce an immune response, which exacerbates joint inflammation and compromises therapeutic efficacy. Administering the vector after disease establishment reduced its efficacy owing to pre-existing pathological damage, underscoring the importance of timely administration.
Current RA treatment, including glucocorticoids, NSAIDs, and biologics, control symptoms and slow disease progression, but have severe disadvantages such as requiring repeated administration, which imposes a considerable economic burden on patients. Poor medication adherence further compromises therapeutic outcomes, leading to disease relapse and cartilage destruction. These drugs also cause substantial side effects, including immunosuppression, increasing the risk of opportunistic infections and tumors. 38 Gene therapy offers a promising alternative by delivering therapeutic genes directly to the lesion site, enabling endogenous production of anti-inflammatory factors. Mammalian joints have poor regenerative properties, 39 which is beneficial for gene therapy strategies for long-term expression of a transgene because it is not diluted by cell proliferation, providing continuous therapeutic effects and minimizing tissue damage. Gene therapy can be administered locally to minimize affecting other tissues and organs and avoid side effects of systemic administration. Delivery of therapeutic genes directly into the joints affected by RA has the potential to address many of the challenges posed by current treatment strategies.
CONCLUSIONS
Our study highlights the potential of AAV-mediated anti-TNF gene therapy for RA, demonstrating significant alleviation of clinical symptoms in animal models. The novel AAV.v128 capsid’s high transduction efficiency and sustained transgene expression provide a reliable vector choice for gene therapy, paving the way for future clinical applications.
Footnotes
ACKNOWLEDGMENT
The authors acknowledge Chengdu Origen Biotechnology Co., Ltd for providing funding for this study.
AUTHOR DISCLOSURE
X.K., Q.Z., and S.L. are inventors on patents with potential royalties licensed to Chengdu Origen Biotechnology Co., Ltd. The remaining authors declare no competing interests.
FUNDING INFORMATION
No funding was received for this article.
SUPPLEMENTARY MATERIAL
Supplementary Table S1
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.