
Abstract
Research data, funding and education have been identified as the main difficulties in Acupuncture research by the World Health Organization and experts in the field. These barriers to the integration of Acupuncture and Herbal Medicine (AHM) in primary care, health coverage and accessibility are interconnected. AHM is a personalized medicine system and research methods applied by biomedical science (BMS) are insufficient in AHM research. This delays AHM integration as policy makers rely on research data for decision making. Changes in AHM education to unify degrees, establish BMS pre-requisites, base the curricula on Classical Chinese Medicine and offer research education, may produce AHM providers who deliver high quality AHM research and benefit all stakeholders. Raising the bar in AHM to offer a sole DAOM and a subsequent clinical and research PhD degree may be the next step in AHM education to improve the overall situation. This literature review explores the current state of AHM research and education to identify opportunities for improvement.
Data Collection Procedures
Only free full articles were used. Searches were performed by hand for English literature.
Database searched: NCBI/Pubmed, Google Scholar, Institutional websites.
Literature reviewed spans the recent 20 years, plus earlier key works.
Types of literature searched include Meta-Analysis, Systematic reviews, RCTs, peer reviewed journals, chief documents, institutional publications and websites.
Selection of relevant articles by keywords addressed in the studies.
Flowchart of selection process.

Introduction
As of 2022 the WHO Global Report on Traditional and Complementary Medicine and WHO Traditional Medicine Strategy 2014–2023 (WHO GRT&TM and TMS) have not been fully implemented and Acupuncture and Herbal Medicine (AHM) is not integral to primary care in the West. 1,2 Statute regulation awaits biomedical science (BMS) to support AHM in primary care and yet BMS has not delivered satisfactory research data. The research methods used do not apply to AHM as an individualized and complex health system which is a barrier to implementation and care. Research in BMS is costly and funding for AHM research is limited although Acupuncture has been widely studied and over 10,000 randomized controlled trials (RCTs) have been published so far. 3 Most research has not been conducted by or with AHM providers with a deep understanding of AHM. However, these providers have not received sufficient training in Classical Chinese Medicine (CCM) or research and there is no dedicated career path to become a professional AHM researcher. In return, BMS researchers have none or very little training in AHM.
The curricula in AHM schools are diversified and little of CCM or research is taught, as biomedical classes occupy a large portion of the hours. Degrees are not unified, six different degrees are currently offered at accredited AHM schools. The variety of professional competencies may not be obvious to the public.
The WHO TMS suggests to “develop appropriate research methodologies consistent with T&CM theories and practice…and encourage investment”. The WHO Guidelines for Clinical Research on Acupuncture state: “The protocol should be deployed by the joint effort of representatives from several disciplines including research subjects (if possible), health workers, acupuncturists and biostatisticians.” (p 16) and “Research education of interested acupuncturists and other health professionals should form an essential first step in developing a research culture within each member state….” (p. 42) “…to foster cooperation between acupuncturists and other health care providers” (p.56).
Improving AHM education may generate AHM providers who develop AHM specific research questions, appropriate research methods and deliver high quality research data. This may further policy making, AHM integration into primary health care and promote funding. Funding could in return advance AHM CCM education and create AHM research facilities. This may assist in reaching the goals of accessibility in health care.
Statement of the Problem
The key issues of research, funding and education in Acupuncture/TCM research have been identified by experts in the field and there has been ongoing debate on which methods are applicable to generate high quality research data in acupuncture research (AR), which may advance access to AHM care. Issues include: research design and methodology, reporting quality, outcomes analysis, placebo, controls, database registration barriers, diagnose pattern identification, funding, infrastructure, access to technology and statistical software, education, research training, publishing opportunities, bias, attitude in the Biomedical and AHM profession.
Progress has been made in the development of documents and guidelines such as Standards for Reporting Interventions in Controlled Trials of Acupuncture and Consolidated Standards of Reporting Trials (CONSORT). Acupuncture is included in the ICD11 (11th International Statistical Classification of Disease and Related Health Problems).
Collaborative dialogue with other disciplines such as Systems Biology, Epigenetics, Anthropology, Physics, Neuroscience are innovating new research methods. The development of new software and technology expands the possibilities of what is measurable in AHM trials.
But the dichotomy between BMS wanting to explore the mechanism of Acupuncture on a bio-molecular level with a RCT structure, and the evidence of AHM in clinical practice calls for a new definition of evidence for stakeholders to move forward. Mirza et al. reviewed RCTs and found “an average 73% exclusion rate and recruitment of less than 10% of patients with the primary diagnosis.” 4 Iyioha describes in “Law's dilemma” as “the nexus between statutory legitimacy and scientific validation of health systems” and calls for “a new regulatory model….in support of a pluralistic health care system balancing the imperative of quality assurance with the need to ensure access.” 5 Baars and Hamre review the factors that promote the integration process of complementary alternative medicine (CAM) 6 and Vickers poses the question of “how much evidence is enough evidence?” 7 A new definition of clinical evidence may emerge from inclusion of AHM providers as professional researchers. CCM education as the base of AHM may provide a vast body of knowledge and bring forth clinically valuable research questions.
Significance of the Study
To inform of the current status in AR and education and inspire constructive dialogue.
Limitations
Data was hand gathered. The data from AHM schools and institutional websites is incomplete or may be out-dated. No analytic or statistical software was available. No collaboration with professional researchers and statisticians was available.
Review of the Literature
Research Issues
Design, methodology, reporting, outcomes analysis
Ho et al. conclude that “most systematic reviews on acupuncture effectiveness are of critically low methodological quality.” 93.4% of 106 systematic reviews (SRs) showed low and critically low methodological quality. Exclusion criteria were absent. 0.9% were found to be of high quality. The authors suggest improvement of publishing protocols and competency of reviewers via classes and education to appraise SR critically. 8
Shuai et al. report design and reporting issues in regards to patient and practitioner criteria, randomization, blinding, controls, and outcome measures. Further insufficient statistical analysis, sample sizes, power calculation, handling of missing data, multiple comparisons, inefficient methods for repeated measurement, cluster data, baseline adjustment, and confounding issues are present. Suggestions are made to develop better design and statistical methods so analysis can show accurate results and improve trial design. 9
Lao et al. discuss “obstacles inherent in the design and statistical analysis of clinical trials of TCM” and demonstrate by application of statistical methodology to a RCT that models of statistical analysis need to become more sophisticated. 10
Wieland et al. report low qualities of RCTs. 11 Manheimer et al. describe most Traditional Chinese Medicine (TCM) reviews as inconclusive (58.57%) with poor methods and heterogeneity. 12 Liu et al. state deficits in reporting of primary outcomes, blinding, and safety. Issues of selective reporting are found to be similar to BMS studies. International requirements at the database are not uniform and methodological data could be missing. 13 Hammerschlag et al. suggest Standards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA) and CONSORT need to be used more widely and should be translated into Chinese. The quality of reporting in regards to practitioner training, adverse events, randomization, and blinding requires improvement. 14 Deng et al. comment on the need for high quality design and Acupuncturist's administration in trials. 15
Diagnostic pattern identification
Liu et al. found <25% use of TCM differential diagnostics in TCM Herbal trials. 13
Bias, controls, placebo
Kaptchuk summarizes placebo effects in AR and states that more research is needed to understand placebo, sham and controls to differentiate between intervention and control. 16
Zheng et al. argue that efficacy outcomes of Acupuncture are still controversial due to lack of consensus on placebo control and encourage utilization of a “blank control” including “no treatment controls, waiting list control and treatment as usual” as possible controls. 17
Birch et al. reviewed the history of use of sham Acupuncture in Acupuncture clinical trials and note “non-inertness of sham acupuncture has been known for more than three decades” and “introduces bias against Acupuncture with risk of underestimating its' effectiveness.” 18
Wieland et al. find that Traditional Eastern Asian Medicine (TEAM) reviews receive low priority. TEAM reviewers have difficulties in understanding and assessing a TEAM intervention. 11 Manheimer et al. list an average of 1139 person-hours per review with little recognition. 12
Deng et al. mention Placebo creates bias. 15
Databases
Wieland et al. describe barriers to registration and conduct of Cochrane SRs as poor understanding of the intervention and low priority of Acupuncture/TCM topics as the main challenge; quality and accessibility of randomized trials as a major concern. “Funding for database access, development of information retrieval expertise, translation and other language assistance activities, and training in systematic review methods specific to TEAM (Traditional East Asian Medicine)” are suggested. 11
Cogo et al. find little overlap beyond major databases. 19
Suggestions made for research data issues
Improve publishing protocols, the competency of reviewers via classes and education to appraise SR critically (Ho et al. 8 and Table 1)
Better trial design and statistical methods for accurate results (Shuai et al. 9 )
Statistical analysis needs sophistication (Lao et al. 10 )
Blank controls, care as usual, waiting list (Zheng et al. 17 )
More placebo research (Kaptchuk 16 )
Funding database access, training, education in SR of TEAM (Wieland et al. 11 )
More research, rigorous RCTs (Manheimer et al. 12 )
More Sham research (Birch et al. 18 )
Search multiple databases beyond Medline, Embase, Cochrane, very little overlap controlled trials in CAM (Cogo et al. 19 )
The need for international standards in trial registration items (Liu et al. 13 )
Acupuncture trials need large sample size (MacPherson et al. 20 )
Wider use of STRICTA, CONSORT, reporting (Hammerschlag et al. 14 )
Design quality, Acupuncture delivery, minimize placebo and bias (Deng et al. 15 )
Multidisciplinary research to advance (Shang 21 )
Research Issues
Acu, Acupuncture; CONSORT, Consolidated Standards of Reporting Trials; STRICTA, Standards for Reporting Interventions in Clinical Trials of Acupuncture; TCM, Traditional Chinese Medicine.
Funding Issues
National Center for Complementary and Integrative Health budget, education, research training
Pritzker and Hui identify three major hurdles in TCM research, one of them obtaining financial support and the small size of the National Institutes of Health (NIH) budget for CAM and Integrative Medicine (IM) research (Table 2). 22 Khalsa and Pearson point out that National Center for Complementary and Integrative Health (NCCIH) awards are not permanent and CAM schools have no research training. 23 Menard et al. recommend to NCCIH that Complementary and Integrated Health (CIH) professionals need research training. 24 Mills et al. list Whole Systems Research (WSR) is not funded by NIH. 25
Funding Issues
CAM, complementary alternative medicine; CIH, Complementary and Integrated Health.
Career development
Khalsa and Pearson show NIH awards for career development are not permanent. 23 Menard et al. recommend funding to promote CIH practitioners. 24
Infrastructure, technology, software
Prtizger and Hui state a small NIH budget for CAM research. 22 Khalsa and Pearson find CAM schools are not affiliated with research facilities. 23 Menard et al. recommend funding for CIH research infrastructure and partnerships. 24
Publishing
Pritzker and Hui show few publishing opportunities for TCM in mainstream medical research journals. 22
Suggestions made for funding issues
Education Issues
For Acupuncturists to be an integral part of AR, research education needs to be included and expanded in AHM schools' curricula. Many schools have recently added some research hours in their programs as prescribed by Accreditation Commission for Acupuncture and Herbal Medicine (ACAHM). There is no obvious career path for Acupuncturists to become a professional researcher and only few schools are associated with a research facility. No data is available on the number of AHM professionals in AHM research.
CIH schools, curriculum
Lam et al. suggest an international TCM curriculum with a joint degree in Western Medicine. 26
Gray et al. reveal the absence of a strategy for research education and a lack of international standards. 27 Wong et al. state the cross-training of TCM and Western Medicine doctors in China. 28 Zhang et al. also note cross-training of TCM and Western Medicine doctors in China. 29 Lam et al. suggest mental health training for TCM clinicians. 26
CIH institutes, research facilities
Gray et al. find only a few active CIH research facilities. 27 Zhang et al. note the importance of the School-Hospital-Axis. 29 Khalsa and Pearson present the financial awards for research training opportunities from the NIH. However, these awards are not permanent. 23
CIH researchers
Bradley et al. refer to the (previous) grants T90 research training for CIH clinicians and R90 for CIH training for Western Medical practitioners. 30 These grants have largely expired and there is no data on the number of AHM providers accepted to participate.
CIH brain drain, career paths
Menard et al. mention brain-drain in CIH. 24 Chung et al. describe poor career perspectives and career paths, low salaries and few employment opportunities. 31
Attitude, bias, collaboration
Bradley et al. describe an inter-professional clinical research training and reference WHO best practices of interprofessional education. 30
Suggestions made for education issues
NIH to expand R25 grants to CIH institutes, practitioners (Menard et al. 24 )
Joint efforts are needed from the government, TCM industry and NGOs (Lam et al. 26 )
More research on CIH education, create agenda and strategy (Gray et al. 27 )
Complex systems research in educational curriculum, networking (Ahn et al. 32 )
Interprofessional training in CIH research and BMS (Bradley et al. 30 )
Interdisciplinary medical education (Wong et al. 28 )
Current CIH education for MDs comprises of: 2 × 45 min. Valentini et al.,
33
45 hours online class, Kligler et al.,
34
a 30-hour class (Amri
35
) Research training is needed in TCM schools (Maiers et al.
36
) Dual training as a base for IM development (Zhang et al.
29
) TCM schools need to seek research grants, evidence-informed practice (EIP) faculty training (Anderson et al.
37
) TCM colleges need to be recognized internationally as Medical colleges (Zhang and Tang
38
) Funding of graduate, postgraduate education and career development (Chung et al.
31
) Western Mental Health training for TCM clinicians (Lam et al.
26
)
Missing data: there is no data available on NIH grants distribution to AHM clinicians. There is no data on distribution of Eastern Medicine, Acupuncture, Asian Herbology, Asian Bodywork (TuiNa) clinicians with research degrees, active in research or having a research career. More research is needed in this area. Most suggestions for improvement were made in the area of education (Tables 3 and 4).
Education Issues
Total of Recommendations from All Three Areas Reviewed (Research Data, Funding, Education)
Educational hours in TCM schools curricula
There are currently 50 TCM schools accredited by ACAHM in the United States (Table 5). The information was hand gathered by reading through each school's website and school catalog, when available. Not every school has made a school catalog available for the public on their website, some of them only allow for viewing of catalog pages but not for downloading a catalog. Some schools send a catalog on demand after gathering personal information for their mailing list, text and phone calls to solicit prospective students. Often educational hours are listed as credit hours or units, a conversion key into clock hours is not always declared.
Education Hours in Traditional Chinese Medicine School Curricula
Eleven schools offer an accredited Doctorate of Acupuncture and Oriental Medicine (DAOM) which is currently the highest accredited degree offered in the United States (Table 6). Forty-four of them offer an accredited Master's degree of Acupuncture and Chinese herbology/Master of Oriental Medicine, which formerly was the standard degree. Five schools offer a Doctorate in Acupuncture, 15schools offer a Doctorate in Acupuncture and Chinese herbology, 26 schools offer a Master of Acupuncture, 11 schools offer a Certificate in Chinese herbology.
Total of Degrees Offered at the Accredited Acupuncture and Herbal Medicine Schools in the United States
Doctorate of Acupuncture and Oriental Medicine
Two of the schools listed the program hours as including Master program hours and it was unclear how many hours comprised the DAOM program alone. One school is teaching out the program and has no information available.
Doctorate, Acupuncture
Two of the schools gave the program hours separate from Master's program hours. One school did not give any data.
Doctorate, Acupuncture and Chinese Herbology
One school listed separate hours. Twelve schools listed total hours including the Master's degree coursework. Five schools did not list research hours and were counted as Zero hours. Two schools did not provide any information.
Master, Acupuncture and Chinese Herbology/Master Oriental Medicine
Five schools gave no or incomplete data. Three schools gave units for research hours without a ratio to clock hours. These units were counted as if they were clock hours in the table.
Master of Acupuncture
Seven schools gave no data. Two schools gave units of research hours without conversion into clock hours and were counted as hours.
Certificate of Chinese Herbology
Two schools gave no data. All schools had zero research hours.
Of 49 schools with available data (Table 7):
Average of Educational Hours by Program
12 schools (24.49%) either are or have access to a research facility.
8 schools (16.33%) listed affiliation with one or more Universities.
10 schools (20.41%) listed affiliation with one or more hospitals.
3 schools (6.12%) listed affiliation with a PhD program abroad.
To date there is no accredited PhD program in the United States.
Accreditation Commission for Acupuncture and Herbal Medicine
Standard 7 “ Program of Study, Criterion 7.02 Minimum Program Length, Credits and Hours” by clock hours (Table 8):
Affiliations of Accredited Traditional Chinese Medicine Schools
Schools with affiliations to or being a research facility.
Prerequisite to enter the Master's study is 60 semester units/90 quarter units of general education with a GPA of 2.5 or higher
Master's Program in Acupuncture (Acu): 1245 didactic/660 clinical, 1905 total
Master's Acupuncture with Chinese herbal medicine (CHM) specialization:
1755 didactic/870 clinical, 2625 total
CHM certificate: 510 didactic/210 clinical, 721 total
Professional Doctoral Acupuncture: 1245 didactic/790 clinical, 2035 total
Professional Doctoral Acupuncture with CHM: 1755 didactic/1000 clinical, 2755 total
Advanced Practice Doctoral DAOM program: 550 didactic/650 clinical, 1200 total (Fig. 1).
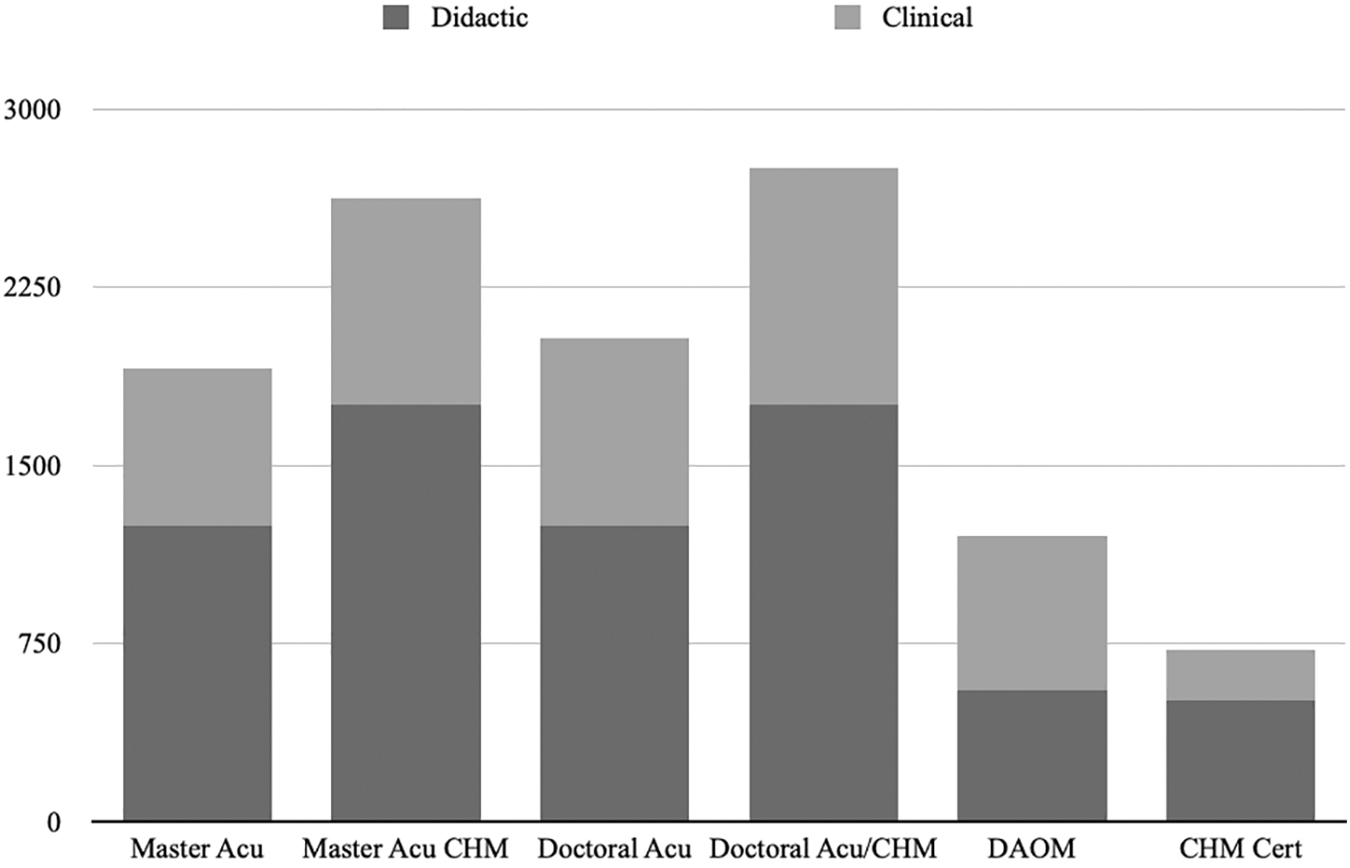
Accreditation Commission for Acupuncture and Herbal Medicine minimum hours required by program.
The Master's program in Acupuncture with CHM and the end degree DAOM together comprise 2305 didactic/1520 clinical, total 3825 hours. This was the original subsequent route of education from a Master's to a DAOM degree.
The AHM schools provide the obligatory educational hours but there is no standard of curricula and professional degrees. For example in the profession of Chiropractor, Doctor of Chiropractic, is the only and terminal degree. This is transparent to the public and regulatory agencies, unifies the profession and facilitates legislative actions. The AHM profession and other stakeholders may benefit from consolidating the number of degrees offered into one terminal degree such as the DAOM degree, which would include the current Master's degree, and a subsequent clinical and research Phd degree, which may promote AHM to become a highly competent and recognized profession. Specialization in diversity of schools of thought and practice of CCM could follow after the DAOM degree to ensure a base standard curriculum to build on.
Literature Examining AHM Schools
Wayne et al. “surveyed the students of two accredited TCM schools in the United States to explore the attitudes and interests towards research. Both schools had received NIH funding to train faculty and students in basic research competencies and induce collaboration with external research facilities. Results showed the students were highly interested in research at the beginning of the curriculum. As clinical hours are introduced later in the program the interest in research declined, possibly due to time constraints. Overall students state the importance of research for stakeholders and policy makers but not as highly relevant to their clinical practice as current research methods do not reflect principles and clinical practice of TCM. Limited research training during CAM education is noted as a significant barrier for CAM clinicians to engage in research.” 39
Anderson et al. “surveyed faculty of an accredited TCM school in the United States to assess research literacy and EIP interest. Responses indicated high interest and support for research. 95% stated TCM clinicians and professors trained in research could make substantial contributions to research. Obstacles were concerns regarding current research paradigms not relating to TCM practice and the co-option and assimilation through biomedical science.” 37
Anderson et al. describe “the training of faculty and development of a Evidence-Informed Practice (EIP) curriculum at the previously surveyed accredited TCM school in the United States. The faculty trained successfully developed and implemented EIP training into the school's curriculum.” Current research standards were identified as an obstacle as they “do not provide a valid treatment approach that acupuncturists can relate to….” 40
Lim et al. describe the status of Acupuncture in China. Higher education in TCM is offered by 46 tertiary Chinese Medicine (CM) Universities, 10 Western medical and 6 non-medical Universities. A Bachelor's degree is earned in five years, the Master's degree in additional three years, and a Phd in another three years. A combined Bachelor's and Master's degree can be earned in seven years. BMS and research training are included. After studies, one year of clinical supervision is required to apply for examination for licensure. Challenges to international research collaborations are identified as the differences of research trends and priorities in the East and West. Western BMS is searching for evidence of the efficacy of TCM using Sham or Placebo controls. Research in the East prioritizes the underlying mechanisms and clinical practice effectiveness and techniques. 41
Givati and Berlinsky analyze over 20 years of Acupuncture education in the United Kingdom titled “The Disenchantment of Traditional Acupuncturists in Higher Education.” 42 This study describes the “rise and decline of Acupuncture training programs in higher education,…efforts to obtain legitimate academic status within a system that is dominated by biomedicine….the gap between institutional demands to standardize and formalize…biomedical adjustments of their programs, while maintaining authenticity..”. It further touches on the underlying matter of colonialism in regards to BMS and CAM therapies, the “persistent and organized scrutiny” Acupuncture is under, and the political rulings affecting the practice of Acupuncture in the United Kingdom. Acupuncture was to “remain self-regulated,which meant that almost anyone can practice Acupuncture regardless of the level of training or qualification.” From 2011–2020 “several Acupuncture programs in Higher Education closed, leaving only four active undergraduate programs of which one stopped recruiting new students.” The “…gap…has not been narrowed by merely the inclusion of biomedical teaching modules within Acupuncture programs.” Student numbers have dropped, “ongoing hostility and marginality…eventually eroded Acupuncture educators….” At the same time Acupuncture educators “demonstrated academic and professional credibility” and “positioned themselves as professional academics within higher education institutions….” 42
Barnes surveys the professional development of Acupuncture and AHM education finding the “growing resemblance to biomedical training”, the TCM (post 1950s) “Americanizing of Chinese Medicine,” tension within the profession, the response from BMS to Acupuncture, and how Acupuncture “has survived by submitting to the authority of biomedicine.” “TCM continues to be the dominant system represented” in AHM education for licensing purposes but some schools value CCM knowledge and “different schools of practice persist.” “Biomedicine, when faced with a paradigm that does not fit its understanding of how things work, has tended to look for whatever pieces of that paradigm can be fitted into its own model and to reject the rest. Either that, or it has found ways to absorb ostensibly contradictory language into its own explanatory system.” “The biomedical community reacted by pursuing two measures. The first involved asserting control over acupuncture's knowledge base through the demand for research and clinical trials; the second entailed regulating….” “ The challenge was to prove that biomedical measures and paradigms could, in fact, explain what was going on.” “It requires the reduction to a single etiological factor and corresponding single intervention, the very premise of RCT is incompatible with Chinese medicine theories and practices.” “…it is more likely that the call for evidence-based outcome studies will reinforce the trend in biomedical circles to conceptualize acupuncture only in the narrowest of terms.” as for example the analgesic aspect of acupuncture has been assimilated and applied in BMS. “Still failing to recognize or understand the paradigms upon which the modality is based, a reductionist version of Chinese medicine was now recognized by hospital and medical school administrations to be a potential source of patient satisfaction and of income.” “The insurance companies, therefore, often paid nothing but created the illusion of openness to complementary and alternative medicine for which the patient still paid out of pocket on top of paying for health insurance. Such policies, it should be noted, continue to restrict use to a largely middle- and upper middle-class patient population…”. “Thus the efforts of the PRC (People's Republic of China) to integrate TCM into state-run services mean something quite different from the attempts of American practitioners to make a place for themselves in the health care marketplace.…” 43
Classical Chinese Medicine
CCM is the original body of AHM which was omitted in the 1950s when TCM was made the new standard. The educational curricula are lacking studies of CCM, research education, career and research opportunities alike. TCM is taught at Acupuncture schools today and is the current regulatory standard. Neither the history of CM, the classical foundations nor the difference between the modern hybrid and the original medicine are mandatory in AHM curricula. Rhonda Chang's work shows “how this has affected AHM education, practice and research alike as the effects of omitting crucial information has led to incoherence and failure and how the assimilation and adaptation of CCM by BMS has allowed for confusion.” Chang explains the “clinical, theoretical and historical difference and disconnections” between Yi (original medicine) and CM (present, TCM). “Since the 1950s the Yi theoretical base and principles of practice have been omitted and replaced with BMS concepts. This has created a schism in the recently created TCM theory and practice.” This new model of CM has been conflicted from the beginning by not not standing on the original foundation, a mixture of modalities being neither one nor the other. 44
Regulatory statutes require health professionals to have basic training in BMS. If BMS were a prerequisite to enter AHM education, the curricula could focus on AHM in its entire body including the original classical foundations. Research education hours could also be increased and a research track could initiate a career in research for interested AHM providers.
Science is examining the post 1950's TCM, which is only partially science based and lacking a full original CM foundation. It is not surprising that research outcomes are not satisfactory and waste in research is generated. With a deep understanding of the classical foundations, meaningful research questions and research methods may develop as AHM professionals distinguish the original from modern versions of CM.
This may clarify which areas of AHM are suitable for which type of research, while also restoring the original medicine in clinical practice.
Career Pathways in Research for Acupuncturists
National Center for Complementary and Integrative Health. NCCIH Strategic Plan FY 2021–2025: Mapping the Pathway to Research on Whole Person Health states “At the individual level, NCCIH supports multiple interdisciplinary opportunities for training of clinician-scientists. For example, NCCIH has partnered with the National Center for Advancing Translational Sciences (NCATS) to provide a research career development pathway for complementary and integrative health clinician-scientists to join careers…” NCCIH Strategic Plan FY 2021–2025
OBJECTIVE 4: Enhance the Complementary and Integrative Health Research Workforce.“development cohorts of other types of clinician-scientists” (p38/39) Yet there are no obvious links for Acupuncturists on the NCCIH's or the National Center for Advancing Translational Sciences's websites to find individual training and funding opportunities.
Further Barriers
As the majority of AHM providers are in private practice (NCCAOM website, accessed December 18, 2022) and not associated with an institution, access to free full text research articles is limited. This is a barrier to enhance clinical practice or to conduct research as a sole AHM provider.
The career outlook for AHM providers with large amounts of student loans is not very encouraging. The cost of AHM education is high and Federal Student Loans in this field are not eligible for loan forgiveness work programs.
The DAOM degree designates providers in some states as primary physicians yet with limited ability to for example order medical tests and laboratory work. Insurance coverage is an ongoing issue and out-of-pocket pay is an obstacle to patient access. The economic burden to become a AHM provider, the non-unified profession, the effort to study BMS and AHM to practice TCM, which is lacking the classical foundation, the lack of career paths, except in private practice, are factors which hinder brilliant research to come from AHM schools, graduates, and their, if existent, affiliated research facilities.
Cultural appropriation, colonialism
Political climate has made the term “Chinese Medicine” and recently “Oriental Medicine” become assimilated into the vagueness of “Acupuncture and Herbal Medicine” which may be a case of cultural and heritage appropriation. Debate on CM history, oral traditions and colonialism are currently not part of AHM school's curricula.
Naming
Frequent name changes within the profession are confusing to the public and may suggest instability and further fragmentation.
Benchmarks for the Training of Acupuncture
The WHO 2020 Benchmarks for the Training of Acupuncture 45 outlines training content for people without a medical background, with a traditional medical background, and with a conventional medical background:
Basic training: 1168 didactic/400 clinical, total 1568 hours.
Advanced: 1968 didactic/500 clinical, total 2468.
The WHO suggests 200 hours basic training for BMS physicians which consists of an introduction to TCM, 201 (of 409 official) Acupuncture points, application in BMS, safety guidelines and treatment techniques. WHO 2020 Benchmarks for the Training of TuiNa (TuiNa is part of AHM training) 45 outlines training content for people without a medical background, with a traditional medical background, with a conventional medical background (Fig. 2).

WHO benchmark outlines acupuncture and TuiNa by hours. Basic level hours: 1104 didactic/400 clinical, 1504 total. Advanced level hours: 1854 didactic/500 clinical, total 2354. There is to date no WHO Benchmark for Chinese Herbal Medicine Training.
AHM Education for Biomedical Physicians
Educational hours in AHM for biomedical Physicians range overall from 90 minutes to 30 hours.
The American Academy of Medical Acupuncture offers basic training in Acupuncture of 150 to up to 300 hours maximum for BMS physicians of which three times 3.5 days are in person.
This is a stark contrast to the BMS and AHM hours required for AHM practitioners.
Summary of Findings and Discussion
The reviewed studies relating to research issues, funding issues and education issues demonstrate the need for improvement, especially in AHM education. BMS is to date not satisfied with the results of its AHM research and AHM is not incorporated into primary care in the West. The reasons may be:
BMS has no or little background in AHM to select applicable research methods and questions
AHM providers have little or no research training
AHM schools are based on TCM with little or no CCM education.
AHM degrees and curricula are currently fractured: there are no BMS pre-medical entry requirements. There is no dual-training as for example in China and the educational requirements in the West are less.
No clinical professional experience is needed to enroll in a AHM Master's or Doctoral program. An AHM student may continue directly from a Master's to a DAOM or Doctoral degree without clinical professional experience,which may be an obstacle to higher level discussions within a Doctoral program. CCM and research education hours in AHM schools are few.
If the portion of BMS taught in AHM schools were a pre-medical entry requirement, for example, a Bachelor's of Science or a medical profession, the curricula could be reserved for CCM and research education instead. A Master's degree within the DAOM (which might soon again be renamed) as only degree may provide coherence and transparency to the public and facilitate patient access to AHM in primary care. Yet to ultimately raise the bar in AHM education a single, direct DAOM degree, followed by a PhD clinical and research degree would bring AHM up to par nationally and internationally. This would further stabilize the profession, eliminate the concern of being co-opted by BMS or encroached on by other professions aiming to use Acupuncture in their scope, and allow for studies of diverse CCM traditions after a solid educational foundation.
Funding may promote the collaboration between AHM schools, hospitals, research facilities, and create career pathways for AHM professionals, becoming the clinical and research experts in their own field. This may facilitate implementation of the WHO TM strategy and ensure patient access.
There is no AHM university teaching and research hospital in the West. A change in AHM curricula, based on CCM with an additional research track, unified degrees such as a DAOM and PhD, may be an attainable next step to improve the current state of AHM research and AHM education and to improve outcomes in and access to patient care. As AHM continues to evolve as a profession in the West, choices can be made to create a complete and emancipated body of medicine and to shape its future accordingly and independently from previous assumptions and limitations. More research on AHM education is needed.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.▪