
Abstract

At Strata Oncology, we won't rest until every patient with cancer gets their best possible therapy.
Our approach to achieving this audacious goal is to develop innovative, highly quantitative, DNA- and RNA-based multivariate predictive treatment selection biomarker algorithms that span therapeutic modalities.
From the very beginning, we have partnered with diverse health systems across the United States to provide routine clinical testing with our integrated molecular tumor profiling platform through an observational clinical trial protocol called the Strata Trial.1
With data from tens of thousands of patients collected under this protocol, we are discovering, validating, and demonstrating clinical utility for multiple new bio-marker algorithms (see box for example).
Prospective-retrospective analyses: efficient and reliable
In an ideal world, there would be time and resources to conduct large randomized controlled trials for every question in medicine.
However, it is not generally ethical to randomize a late-stage cancer patient to placebo or a treatment with known and minimal benefit. Patients with cancer simply do not have time to wait for the ideal, especially when trial designs that can more efficiently provide reliable evidence for clinical utility are available.
One such design that is well-suited for biomarker evaluation is a “prospective-retrospective” study, in which prospectively defined hypotheses are tested in archived specimens not collected specifically for that purpose. This is the method by which many widely used biomarkers for cancer therapy selection have been validated and shown to have clinical utility.
For example, the association of wild-type but not mutated KRAS with positive treatment response to anti-EGFR monoclonal antibody therapies in colorectal cancer was based on retrospective analysis of samples from efficacy studies.2
In another example, the pan-tumor approval for pembrolizumab based on tumor mutational burden (TMB) was based on retrospective analysis of samples from the Keynote-158 study.3
While the biomarker examples cited above relied upon studies conducted on samples collected during the course of controlled interventional trials, use of samples from well-designed observational cohort studies (whereby a group of patients are identified and followed over time for outcomes) can provide strong evidence for a given hypothesis.4
Regardless of the source of samples, the key is to ensure that important design biases are avoided and/or accounted for so as to achieve the goal of demonstrating the biomarker and outcome association are true and not due to other unknown factors.
In our studies utilizing Strata Trial data, multiple strategies are leveraged to reduce and/or eliminate bias. For example: standardized eligibility criteria, which include the intended use population for the biomarker under study; standardized procedures for sample collection, processing and shipment; a single laboratory processing all samples; harmonized data entry standards; and time-based outcomes anchored on a specific exposure (e.g., relevant medication start and post-sample collection) to better mimic the controlled start of an intervention as in a controlled trial.
Real-world data for real-world patients
In two important ways I would argue that developing new biomarkers using prospective-retrospective analyses of Strata Trial data is as good as if we were relying upon archived samples from randomized controlled trials.
First, the patients who participate in the Strata Trial are more representative of the overall population of patients with cancer than those who take part in randomized controlled interventional trials, who represent less than 5% of U.S. adults with cancer and who are younger, healthier, and less diverse than the other 95% of patients with cancer.5
The inclusion criteria for Strata Trial is very broad—any patient 18 years of age or older with a documented advanced or metastatic solid tumor is eligible to enroll. Additionally, many of the trial sites are in the community (vs. academic medical centers), where more than 80% of patients receive care.6
Second, thanks to the longitudinal nature of our data collection (treatment data collected from all lines, going back to time of diagnosis), we are able to conduct within-subject comparative effectiveness studies (aka case-crossover) to assess the biomarker's ability to predict benefit between therapies. We control by patient—every patient serves as their own control—as an effective alternative to randomization for testing many clinical associations.
For example, for our Immunotherapy Response Score (see box), we confirmed the predictive (vs. prognostic) nature of the biomarker across tumor types by assessing patients who had received a previous line of non-immunotherapy systemic therapy prior to pembrolizumab monotherapy.7
The new standard for cancer care
The powerful clinical-molecular database of uniformly collected test results and treatment outcomes we have assembled through the Strata Trial is fueling new discoveries and new hope.
By utilizing an efficient yet robust method for analysis of archived samples, we are driving a paradigm shift in the treatment of people with cancer. We are expanding and optimizing the use of cancer therapies and delivering patients access to more options.
Brad Ziegler/Strata Oncology

Pan-Tumor Predictive Biomarker for Checkpoint Inhibitor Immunotherapy Benefit
Current pan-tumor biomarkers for PD-1/PD-L1 checkpoint inhibitor treatments identify only a fraction of responsive patients, meaning far too many people who could benefit from these therapies are not being identified. Additionally, immunotherapy is often combined with chemotherapy, without clear data on when this is necessary (i.e., when monotherapy would offer similar benefit).
Strata has developed a proprietary Immuno-therapy Response Score (IRS), which meets a significant unmet medical need for an integrative, predictive diagnostic test that better predicts likelihood of benefit from anti-PD-1/PD-L1 checkpoint inhibitor monotherapy, across solid tumor types7.
IRS was developed using treatment data and comprehensive, clinically validated genomic and transcriptomic profiling of tumor tissue from the Strata Trial. The biomarker algorithm, which was validated in an independent cohort of Strata Trial patients, captures the biology of the tumor and its microenvironment by combining tumor mutation burden (TMB) with quantitative expression of PD-L1, PD-1, ADAM12 and TOP2A.
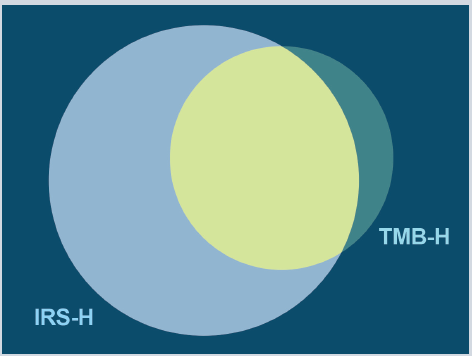
Across more than 24,000 Strata Trial samples, twice as many patients were IRS-H than TMB-H.
Key data:
IRS predicts real-world progression free survival and overall survival in anti-PD-1/PD-L1 monotherapy treated patients across tumor types.
IRS-high status predicts similar duration of benefit as tumor mutational burden (TMB)-high status across tumor types, but identifies twice as many patients who may benefit from checkpoint inhibitor treatment as TMB alone.
In non-small cell lung cancer (NSCLC) patients who were IRS-high, there was no significant benefit of combination therapy (pembrolizumab + chemotherapy) compared to monotherapy (pembrolizumab).