
Abstract
Abstract
Acute lung injury (ALI) remains a significant source of morbidity and mortality in the critically ill patient population. Defined by a constellation of clinical criteria (acute onset of bilateral pulmonary infiltrates with hypoxemia without evidence of hydrostatic pulmonary edema), ALI has a high incidence (200,000 per year in the US) and overall mortality remains high. Pathogenesis of ALI is explained by injury to both the vascular endothelium and alveolar epithelium. Recent advances in the understanding of pathophysiology have identified several biologic markers that are associated with worse clinical outcomes. Phase III clinical trials by the NHLBI ARDS Network have resulted in improvement in survival and a reduction in the duration of mechanical ventilation with a lung-protective ventilation strategy and fluid conservative protocol. Potential areas of future treatments include nutritional strategies, statin therapy, and mesenchymal stem cells.
Introduction
Definition and Epidemiology
Ashbaugh and colleagues,(3) in 1967, were the first to use the phrase acute respiratory distress syndrome (ARDS) to describe a cohort of 12 critically ill patients with acute respiratory failure. In 1994, after decades of different definitions, the American-European Consensus Conference Committee recommended the adoption of a consensus definition for ALI/ARDS. This definition requires the acute onset of diffuse bilateral pulmonary infiltrates by chest radiograph; a PaO2/FiO2 ≤300 for ALI and ≤200 for ARDS; and a pulmonary artery wedge pressure (PAWP) ≤18 or no clinical evidence of left atrial hypertension.(4) The two primary advantages of this definition were the simplicity of clinical application and the ability to quantify the severity of lung injury. Although this definition has some limitations,(5–8) specifically in variability of chest radiograph interpretation, it has been widely adopted for both clinical and research purposes.
The incidence of ALI/ARDS has been difficult to assess due to nonuniform definitions, etiologic variations, geographical variation, inadequate documentation, and underrecognition of disease entity. In 2003, Goss and colleagues(9) used the NIH-funded ARDS network database to prospectively identify ALI patients from 1996–1999. They estimated an incidence of 64.2 cases per 100,000 person-years after adjusting for biases inherent within their study. More recently, Rubenfeld and colleagues(1) conducted a large prospective, population-based validated cohort study of ALI incidence in King County, Washington. The crude incidence was 78.9 per 100,000 person-years, with an age-adjusted incidence of 86.2 per 100,000 person-years. The strengths of this study were the prospective design, use of the consensus definition, and inclusion of a large number of patients from multiple intensive care units (ICUs) (21 hospitals) for 1 year. When this data was extrapolated to the United States as a whole, the investigators estimated that the incidence of ALI is approximately 200,000 patients with a mortality rate of 40%.(1)
Other factors such as age and associated clinical disorders may impact the incidence of ALI and ARDS. In the Rubenfeld cohort, similar to other studies,(10,11) the incidence of ALI increased with age from 16 per 100,000 person-years for those 15–19 years of age to 306 per 100,000 person-years for those 75–84 years of age.(1) Predisposing clinical factors include sepsis, pneumonia, aspiration, trauma, pancreatitis, blood transfusions, and smoke or toxic gas inhalation.(12) Severe sepsis and multiple transfusions are associated with the highest incidence of ARDS; the lowest rates occur in patients with trauma or drug overdoses.(1,13) For patients with multiple comorbidities, chronic alcohol abuse, or chronic lung disease, the risk for lung injury is higher.(12)
ARDS mortality rate has declined over the last 2 decades. In the 1980s, mortality rates were approximately 64–70%.(14–16) However, these rates must be interpreted with caution, as an ALI/ARDS consensus definition was not adopted until 1994. More recent studies now indicate a mortality risk of 29–42%.(1,17–19) The nature of the underlying clinical disorder is an important determinant of outcome. For example, sepsis has a higher mortality than major trauma (43 vs. 11%), whereas pneumonia and aspiration are intermediate risk factors (36 and 37%, respectively).(20) Other factors that influence mortality appear to be age and race. Rubenfeld and colleagues(1) found that mortality was significantly lower in patients 15–19 years of age (24%) compared to patients 85 years of age or older (60%). This finding was further supported by Flori et al's(21) prospective study of 328 pediatric patients with a reported mortality rate of 22%. Racial inequalities in disease burden also occur in African-Americans and Hispanics who have a higher 60-day mortality rate (33%) compared to Caucasians (27%.)(22) This increased risk of death is independent of age, gender, ventilation strategy, lung injury etiology, comorbidities, or degree of hypoxemia. For African-Americans, the severity of illness at presentation appeared to moderate this higher mortality risk. Despite these different mortality rates in specific age and racial groups, the overall trend has been a decline in mortality over the last 2 decades. The primary factors that seem to explain the reduction in mortality are the use of a lung protective ventilation strategy, a fluid conservative strategy, and other improvements in critical care including perhaps more effective treatment of sepsis. These factors will be discussed more in the section on treatment.
Pathogenesis
Acute lung injury is a disorder of acute inflammation that causes disruption of the lung endothelial and epithelial barriers. The alveolar–capillary membrane is comprised of the microvascular endothelium, interstitium, and alveolar epithelium. Cellular characteristics of ALI include loss of alveolar–capillary membrane integrity, excessive transepithelial neutrophil migration, and release of pro-inflammatory, cytotoxic mediators (Fig. 1).(12,23) Biomarkers found on the epithelium and endothelium and that are involved in the inflammatory and coagulation cascades predict morbidity and mortality in ALI (Table 1).
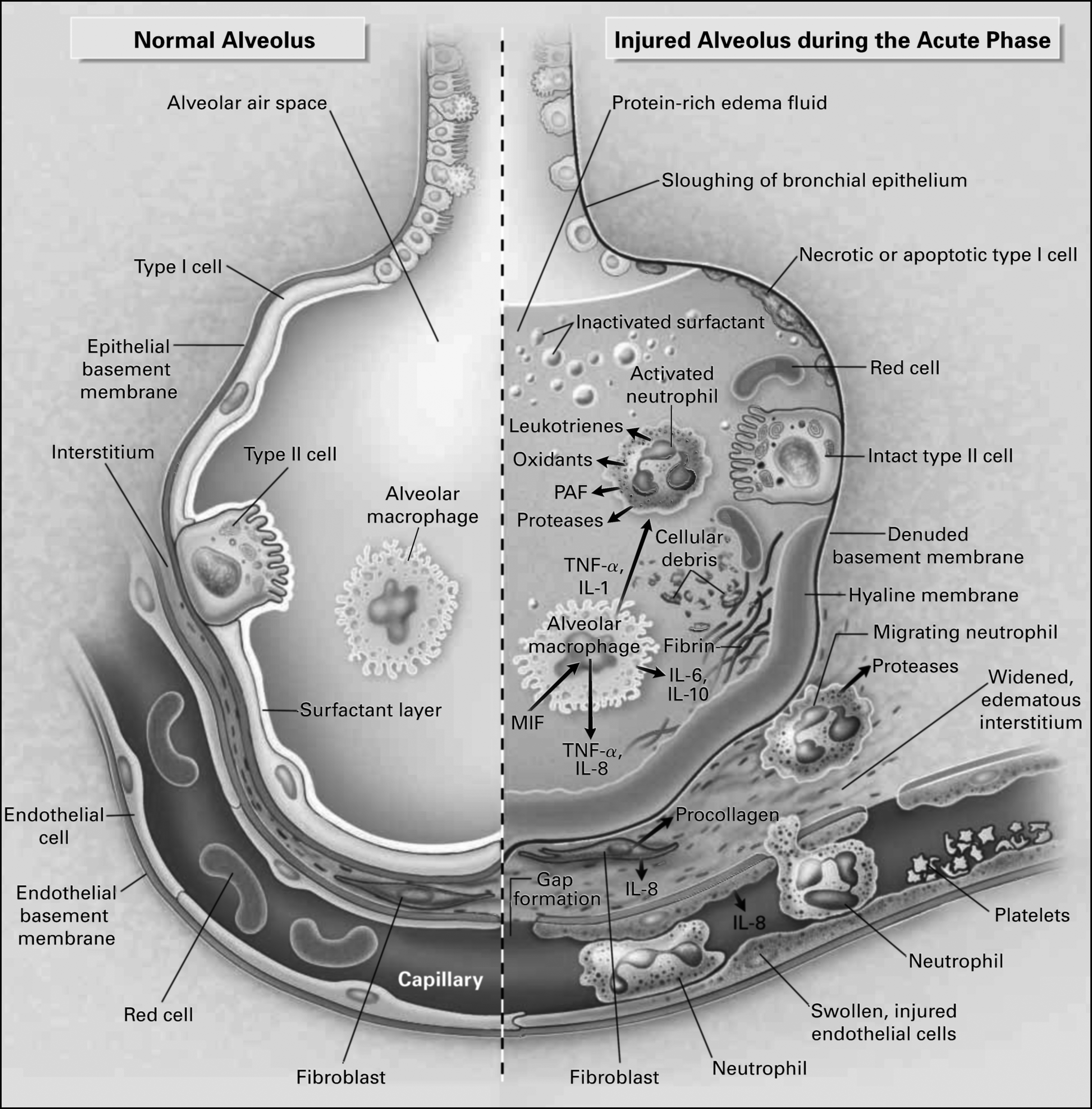
The normal alveolus (left-hand side) and the injured alveolus in the acute phase of ALI and the acute respiratory distress syndrome. In the acute phase of the syndrome (right-hand side), there is sloughing of both the bronchial and alveolar epithelial cell, with the formation of protein-rich hyaline membranes on the denuded basement membrane. Neutrophils are shown adhering to the injured capillary endothelium and marginating through the interstitium into the air space, which is filled with protein-rich edema fluid. In the air space, an alveolar macrophage is secreting cytokines, interleukin (IL)-1, IL-6, IL-8, IL-10, and tumor necrosis factor (TNF)-α, which act locally to stimulate chemotaxis and activate neutrophils. Interleukin-1 can also stimulate the production of extracellular matrix by fibroblasts. Neutrophils can release oxidants, proteases, leukotrienes, and other proinflammatory molecules, such as platelet-activating factor (PAF). A number of anti-inflammatory mediators are also present in the alveolar milieu, including IL-1-receptor antagonists, soluble TNF receptors, autoantibodies against IL-8, and cytokines such as IL-10 and IL-11 (not shown). The influx of protein-rich edema fluid into the alveolus has led to the inactivation of a surfactant. ALI, acute lung injury; MIF, macrophage inhibitory factor. Reprinted with the permission of the publisher.(12) Copyright 2000 Massachusetts Medical Society. All rights reserved.
Notes: VWF, von Willebrand factor antigen; ICAM-1, intercellular adhesion molecule; SP-D, surfactant protein D; RAGE, receptor for advanced glycation end-products; IL-6, IL-8, interleukins-6, -8; PAI-1, plasminogen activator inhibitor-1
Outcomes associated with high-tidal volume cohort only.
Following infection or trauma, upregulation of proinflammatory cytokines occurs as a direct response and/or as a marker of ongoing cellular injury. Meduri et al.(24) found that baseline and persistently elevated plasma levels of interleukin (IL)-6, IL-8, and tumor necrosis factor (TNF)-α were strongly predicative of mortality. This finding was further supported by Parsons and colleagues'(25) large prospective study involving the ARDS Net trial of lower versus higher tidal volume. Even after adjustments for ventilator strategy, severity of illness and organ dysfunction, higher plasma levels of IL-6 and IL-8 were independently associated with fewer organ failure- and ventilator-free days, and elevated IL-6 and IL-8 independently predicted higher mortality. Several studies have demonstrated that lower tidal volume ventilation can attenuate the cytokine responses, potentially reflecting the ability to indirectly modulate the inflammatory response as well as decreasing ventilation-induced lung epithelial injury.(25–28) Alterations in coagulation and fibrinolysis also occur in lung injury, specifically protein C and plasminogen activator inhibitor-1. Ware et al.(29) measured plasma samples of these proteins taken as part of a large, prospective multicenter clinical trial. Compared to controls and patients with acute cardiogenic pulmonary edema, lower plasma levels of protein C and higher plasma levels of plasminogen activator inhibitor-1 were strong independent predictors of mortality, as well as ventilator-free and organ-failure-free days.
Microvascular endothelial injury leads to increased capillary permeability. This alteration in permeability permits the efflux of protein-rich fluid into the peribronchovascular interstitium, ultimately crossing the epithelial barrier into the distal airspaces of the lung.(30) Several studies have documented increased release of von Willebrand factor (vWf )(31–33) and upregulation of intracellular adhesion molecule-1 (ICAM-1)(34–36) following endothelial injury. Both of these biomarkers are independent predictors of mortality.
Transepithelial neutrophil migration is an important feature of acute lung injury because neutrophils are the primary perpetrators of inflammation. Excessive and/or prolonged activation of neutrophils contributes to basement membrane destruction and increased permeability of the alveolar–capillary barrier. Migrating groups of neutrophils result in the mechanical enlargement of paracellular neutrophil migratory paths.(37) Neutrophils also release damaging pro-inflammatory and pro-apoptotic mediators that act on adjacent cells to create ulcerating lesions.(37,38) One of the best studied neutrophil mediators, elastase, appears to degrade epithelial junctional proteins, possess pro-apoptotic properties, and perhaps have direct cytotoxic effects on the epithelium.(39–43) In some animal models, neutrophil depletion can be protective.(37,44–46) However, acute lung injury can also develop in the absence of circulating neutrophils indicating that neutrophil-independent pathways can also cause lung injury.(47)
Normally, type I and type II alveolar epithelial cells form tight junctions with each other, selectively regulating the epithelial barrier. Increased permeability of this membrane during the acute phase of lung injury leads to the influx of protein-rich edema fluid into alveolar space. Type I and II epithelial injury leads to disruption of normal fluid transport via downregulated epithelial Na channels and Na +/K +ATPase pumps, impairing the resolution of alveolar flooding.(12,30) In fact, Lee et al.(48) recently reported that alveolar edema fluid from ALI patients downregulated the expression of ion transport genes responsible for vectorial fluid transport in primary cultures of human alveolar epithelial type II cells. Conversely, gene expression for inflammatory cytokines IL-8, TNF-α, and IL-1β increased by 200, 700, and 900%, respectively. In functional studies, net vectorial fluid transport was also reduced (0.02 ± 0.05 vs. 1.31 ± 0.56 μL/cm2/h, p < 0.02). Alveolar epithelial type II cell injury also leads to a loss of surfactant production,(49) decreasing overall pulmonary compliance. Finally, type II epithelial cells normally drive the epithelial repair process; loss of this function can lead to disorganized, fibrosing repair.(50)
Alveolar epithelial biomarkers including surfactant D (SP-D) and the receptor for advanced glycation end-products (RAGE) are validated biomarkers for lung epithelial injury. SP-D, secreted by type II epithelial cells, has anti-inflammatory properties and promotes pathogen phagocytosis and neutrophil recruitment. A prospective study from the large ARDS Network low tidal volume ventilation cohort (563 patients) reported that higher baseline plasma SP-D levels were independently associated with mortality and fewer ventilator- and organ-failure free days after controlling for severity of illness, clinical covariates, and ventilator strategy.(51) RAGE, a transmembrane immunoglobulin primarily expressed on type I epithelial cells, is elevated in the plasma and edema fluid of patients with ALI compared to those with hydrostatic edema.(52) Calfee and colleagues(53) utilized the ARDS Network plasma samples from the low versus high tidal volume trial to further investigate the relationship of RAGE and ALI. This study reported that higher RAGE levels were associated with increased morbidity and mortality and fewer ventilator-free and organ-failure free days in the higher tidal volume cohort. These findings persisted after adjustment for age, gender, severity of illness, and the presence of sepsis or trauma. RAGE levels declined in both groups; however, there was a 15% greater reduction (p = 0.02) in day 3 RAGE levels in the lower tidal volume cohort.
Resolution of ALI/ARDS is primarily dependent on a timely and orderly repair of the alveolar gas exchange apparatus. For gas exchange to improve, alveolar fluid transport must be upregulated, clearing the airspace of protein-rich edema fluid, and restoring the normal secretion of surface active material from alveolar type II cells (Fig. 2).(23,54)
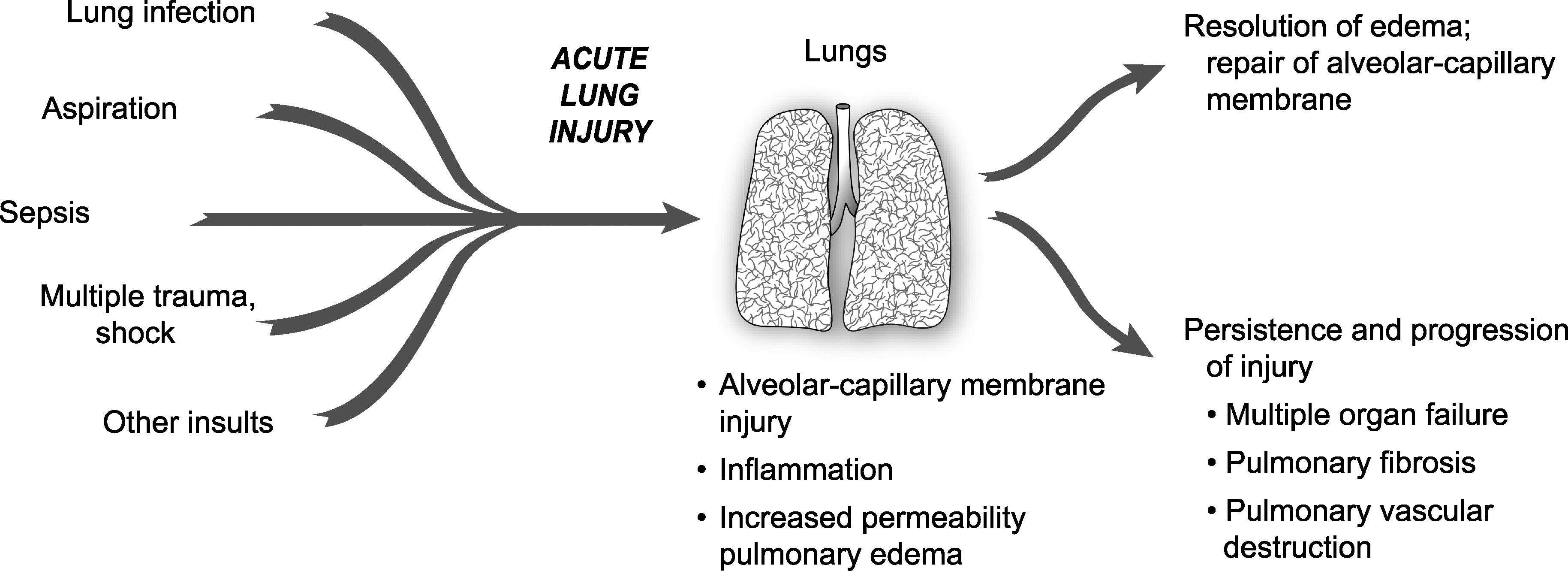
The natural history of ALI/ARDS includes resolution and repair versus persistence and progression. Clinical and epidemiologic studies demonstrate that ALI/ARDS resolves with return of alveolar function to normal or near normal in some patients, whereas in others there is persistence and/or progression of injury. The outcomes of persistence and progression include multiple organ failure, fibrosing alveolitis, pulmonary vascular obliteration with pulmonary hypertension, and death. The genetic, cellular, molecular. and iatrogenic factors that contribute to each of these outcomes remain largely unknown. In addition, rational mechanism-based strategies that favorably influence repair of the alveolar–capillary membrane are undefined. Reprinted with the permission of the publisher.(23) Copyright 2005 American Thoracic Society. All rights reserved.
Treatment
Treatment of acute lung injury is based in both ventilatory and nonventilatory strategies. To date, the most significant advances in the supportive care of lung injury patients have been associated with improved ventilator management. Several clinical trials have shown that a large number of pharmacologic strategies have not been effective in reducing mortality.
The best evidence for the value of a lung protective strategy in patients with ALI is the National Heart, Lung, and Blood Institute (NHLBI) ARDS network's multicenter, randomized controlled trial of 861 patients with ALI/ARDS.(55) In this study, patients were randomized to 6 mL/kg tidal volume versus 12 mL/kg tidal volume with plateau pressure restrictions (<30 vs. <50 cm H2O). Mortality in the low tidal volume group was significantly lower than the high tidal volume group (31 vs. 40%, p = 0.007). Patients ventilated with low tidal volume also had more ventilator free and nonpulmonary organ failure-free days. Clinical risk factors including sepsis, aspiration, pneumonia, and trauma did not affect the efficacy of the low tidal volume strategy.(20) This strategy even attenuated the inflammatory response (IL-6 and IL-8) associated with acute lung injury.(25)
Optimal fluid management has been a controversial topic. In 2006, the NHLBI ARDS Network published the findings of their prospective, randomized controlled trial of fluid conservative versus fluid liberal management strategy.(56) Although there was not a significant difference in mortality, the fluid conservative strategy improved oxygenation and severity of lung injury as well as reduced the duration of mechanical ventilation. The incidence of nonpulmonary organ failure, specifically renal failure, and shock did not increase. These findings match well with previously published animal and human model studies.(56–60) This study also reported that the use of a pulmonary artery catheter (PAC) versus a central venous catheter (CVC) to guide fluid strategy was not associated with improved clinical outcomes.(61)
Recent advances in the understanding of the pathophysiology of acute lung injury have led to investigations of numerous potential pharmacologic treatments. Despite earlier encouraging preclinical evidence, phase III trials have not supported the use of exogenous surfactant, inhaled nitric oxide, intravenous prostaglandin E1, glucocorticoids, Ketoconazole, Lisofylline, N-acetylcysteine, and activated protein C as treatments for ALI (Table 2).
There has been considerable preclinical data supporting the potential value of β-2 agonist therapy for the treatment of ALI.(62–68) These studies reported that β-2 agonists accelerate the resolution of pulmonary edema by decreasing inflammation and upregulating alveolar salt and water transport, hastening the resolution of alveolar edema. Recently, a large, multicenter, randomized clinical trial of an aerosolized β-2 agonist, albuterol, was stopped early for futility. In this NHLBI ARDS Network trial, the aerosolized β-2 agonist may not have been effective due to the severity of alveolar epithelial injury or suboptimal drug delivery to the injured alveoli.(69) There is a large, randomized clinical trial underway in the United Kingdom using intravenous salbutamol, a β-2 agonist. A small, single-center, randomized trial in the UK recently demonstrated that intravenous salbutamol significantly lowered extravascular lung water.(70)
The ARDS Network is currently investigating the potential benefits of initial trophic enteral feeding followed by advancement to full-calorie enteral feeding versus early advancement to full-calorie enteral feeding in patients with ALI/ARDS. Most clinicians agree that enteral nutrition is preferable over parenteral nutrition; however, the optimal timing, composition, and quantity of enteral feeding remains controversial. Some studies suggest enteral feeding within 48 hours of initiation of mechanical ventilation reduces mortality in patients with ARDS, although these findings are not conclusive.(71–73) Low to moderate volumes of enteral feed appear to reduce infections and mortality by maintaining intestinal microvilli height and structure and reducing inflammation by stimulating secretion of brush border enzyme, endogenous peptides, secretory IgA, and bile salts.(74–76)
A novel approach to ALI includes HMG-CoA reductase inhibitors (statins). Normally used for the prevention or treatment of cardiovascular disease, statins also possess significant anti-inflammatory, immunomodulatory, and antioxidant effects. However, it is uncertain how these properties will translate to the human ALI/ARDS population. Several observational studies in the human sepsis model, a known risk factor for ALI, have reported statin users have a decreased severity of sepsis and mortality despite having higher baseline comorbidities.(77–81) Preliminary data from two prospective randomized controlled trials involving statins and sepsis support these observational studies. Choi and colleagues(82) noted that hospital mortality was reduced in the statin group compared to placebo (27.3 vs. 55.9%; p = 0.026). Although Montoya and colleagues(83) did not report a difference in survival, hospital length of stay was shortened and C reactive protein (CRP) levels decreased in the simvastatin group. These findings need to be validated in prospective studies. Kor and colleagues(84) noted no difference in morbidity and mortality in a retrospective observational study of 178 patients with ALI/ARDS, 45% of whom had received statin therapy.
One promising new treatment for ALI is bone marrow-derived mesenchymal stem cells (MSCs). These cells possess the ability to differentiate into many types of cells, including vascular endothelium and alveolar epithelium. MSCs also secrete paracrine factors that reduce the severity of ALI,(85–88) including growth factors, factors that regulate barrier permeability, and anti-inflammatory cytokines. Gupta and colleagues(89) reported the MSCs' anti-inflammatory properties in both in vivo and in vitro. In a mouse model, Escherichia coli endotoxin was instilled into the distal airspaces of the lung, followed by direct intrapulmonary administration of MSCs 4 h later. MSCs decreased extravascular lung water, alveolar–capillary permeability, and mortality. These results were independent of the MSC's ability to engraft into the lung, a property suggestive of a paracrine mechanism of action. The pro-inflammatory response was downregulated, whereas the anti-inflammatory response upregulated. Several investigators are working on translating these experimental studies to phase I and II clinical trials of patients with severe ALI.
Finally, delivery of potential therapies via aerosol to the distal air spaces of the lung remains a viable delivery route for both small molecules and proteins. Depending on the treatment modality, aerosol delivery may avoid systemic effects and more specifically target the lung. Considerable expertise has been developed to optimize delivery of small and large molecules by the aerosol route in mechanically ventilated patients. This delivery method should be considered in future investigations of potential pharmacologic treatments.
Footnotes
Acknowledgments
This work was supported by the NHLBI HL51856 and HL51854 grants (MAM). The authors thank Diana Lim for her assistance.
Author Disclosure Statement
No conflicts of interest exist.