
Abstract
Abstract
Background:
The study objective of this pilot study was to determine the lung delivery of HFA-134a-beclomethasone dipropionate (HFA-BDP; QVAR™) and CFC-beclomethasone dipropionate (CFC-BDP; Becloforte™) with and without the add-on spacers, Aerochamber™, and Volumatic™. The smaller particles of HFA-BDP were presumed to produce greater lung deposition using spacers, with and without a delay [i.e., metered dose inhaler (MDI) actuation into the spacer and subsequent inhalation 0 and 2 sec later], compared with the larger particles of CFC-BDP. The study included a comparison of breathhold effects (i.e., 1 and 10-sec breatholds) on lung deposition.
Methods:
The study was an open-label design and utilized healthy subjects (n = 12 males). Each arm of the study contained three subjects; thus, outcomes were not powered to assess statistical significance. HFA-BDP and CFC-BDP were radiolabeled with technetium-99m and delivered to subjects.
Results:
Results showed that the small particle HFA-BDP lung deposition averaged 52% and was not affected by the use of Aerochamber with or without a spacer delay. The oropharyngeal deposition of HFA-BDP was reduced from approximately 28% to 4% with the Aerochamber. Lung deposition with the large particle CFC-BDP was 3–7% and generally decreased with Aerochamber or Volumatic. A 2-sec time delay between actuation and breath plus the spacer reduced lung deposition slightly but reduced oropharygeal deposition substantially (84% down to 3–20%) using the Aerochamber or Volumatic with and without a spacer delay. HFA-BDP lung deposition was dependent on the breathhold. Lung deposition with HFA-BDP was reduced by 16% with a 1-sec versus 10-sec breathhold. The difference was measured in the increased exhaled fraction, confirming that smaller particles need time to deposit and are exhaled if there is a reduced breathhold. The large particle CFC-BDP lung deposition was not affected by breathhold.
Conclusions:
The use of Aerochamber or Volumatic spacers with HFA-BDP did not alter lung deposition but it did reduce oropharyngeal deposition. However, HFA-BDP displayed reduced oropharyngeal deposition without a spacer.
Introduction
HFA-BDP™ is an MDI formulation of beclomethasone dipropionate (BDP) that uses HFA-134a as a propellant. HFA-BDP is a solution formulation, which together with new valve and actuator designs, produces a small particle of 1.1 microns mass median aerodynamic diameter (MMAD). This small particle size allows for HFA-BDP aerosol to remain suspended in inhaled air, and results in an aerosol being able to penetrate to the small airways of the lungs. Human deposition studies have shown that HFA-BDP produces more than 50% lung deposition compared with less than 10% for CFC-BDP MDIs(6) and less than 15% for fluticasone MDIs.(7) HFA-BDP deposition in airways or spacers is considered more time dependent than the larger particle size MDI formulations where particle impaction occurs immediately. In addition, oropharyngeal deposition is ∼30% with HFA-BDP compared with ∼90% with CFC-BDP, without the use of add-on spacers.(6,7) This increased lung delivery efficiency shown by subsequent clinical efficacy studies(8) is the reason why the formal switch program from CFC-BDP to HFA-BDP recommended reducing the BDP dose by half when switching patients to HFA-BDP.
The study described here compared the use of HFA-BDP and CFC-BDP with and without two marketed spacers (i.e., Aerochamber™ and Volumatic™). The hypothesis was that that the smaller particles of HFA-BDP would produce higher lung deposition values using spacers, with and without a spacer delay (i.e., MDI actuation into the spacer and subsequent inhalation of 0 and 2 sec later), compared with the larger particles of CFC-BDP. This study also compared the effect of breath hold on lung deposition using HFA-BDP and CFC-BDP without spacers. Each of the seven arms of the study contained three subjects not necessarily matched by the same subjects in each arm; thus, outcomes were not powered to assess statistical significance.
Materials and Methods
The inhalers utilized included HFA-BDP (hydrofluoroalkane-134a beclomethasone dipropionate) 40 and 80 μg strengths (ex-actuator) from HFA-BDP press and breathe MDI (QVAR™; 3M Pharmaceuticals, St. Paul, MN, USA) and CFC-BDP (Becloforte™; Allen and Hanburys, Greenwood, UK) 250 μg strength. The spacers utilized in this study were Aerochamber™ (Monaghan Medical, Pittsburgh, New York, USA) and Volumatic™ (Allen and Hanburys, Greenford, UK).
Radiolabeling method
The radiolabeling method has been previously described by Leach et al.(9) The procedure was modified from the methods of Few et al.,(10) Kohler et al.,(11), and Newman et al.(12) Briefly, 99mTc was obtained as Na99mTcO4 (sodium pertechnetate) in saline. The technetium was extracted into chloroform, placed into the appropriate MDI can, and the chloroform evaporated. The formulation from the original product was poured into the radioactive vial and mixed with the technetium. A new valve appropriate for the original test formulation was crimped onto the radioactive vial. The activity of the delivered drug was counted in a well counter, and the mass of the drug was determined by high-performance liquid chromatography (HPLC).
Radiolabel validation
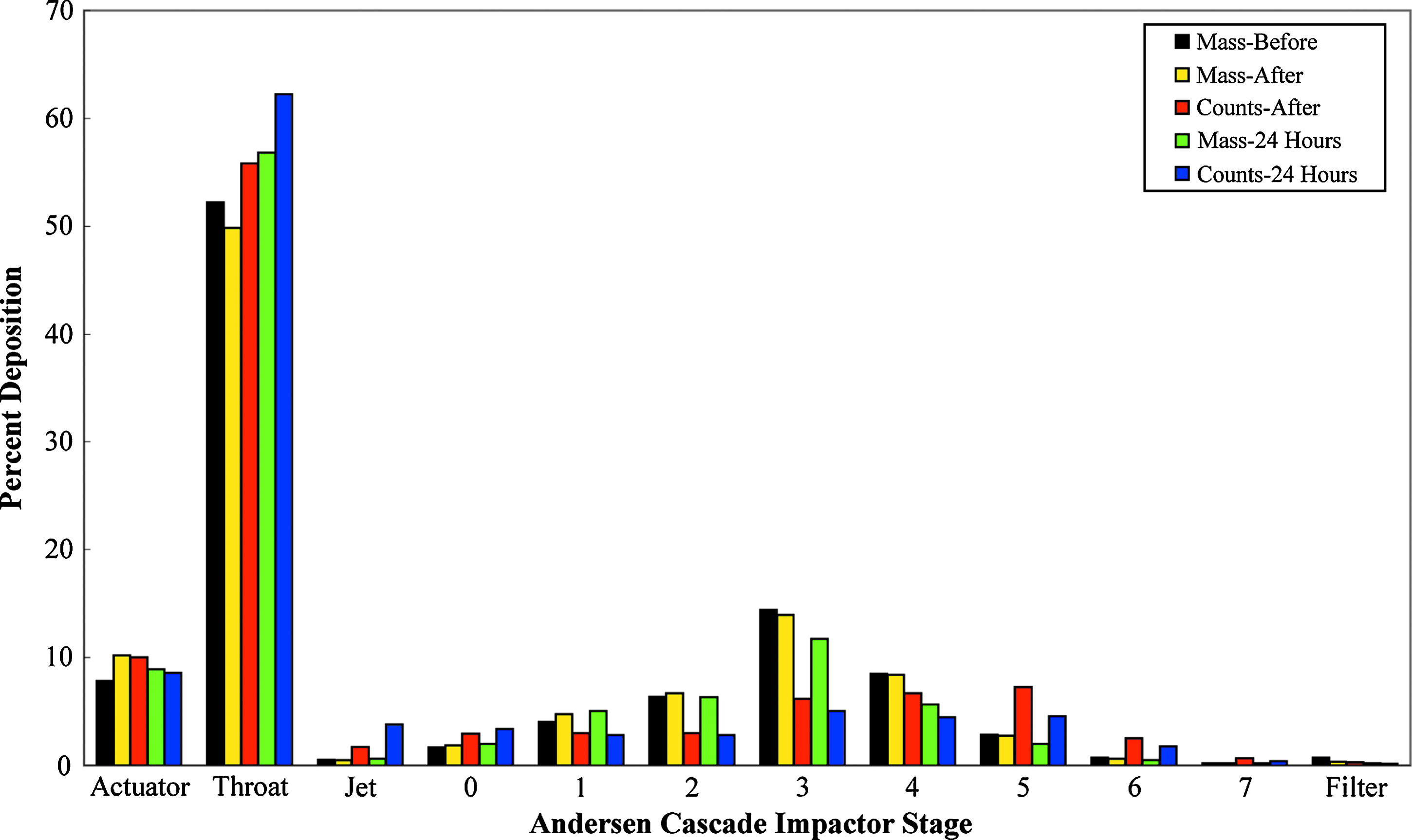
The procedure used to validate the radiolabel has been previously described.(9) Briefly, it was necessary to ensure that the mass of the drug and radioactivity per actuation were within original specifications. It was also necessary to ensure that the particle size distribution [e.g., MMAD and geometric standard deviation (GSD)] and medication delivery (i.e., total mass of drug delivered ex-actuator) did not change after radiolabeling. The mass of the drug was determined by HPLC specific for BDP. An Andersen 1 Particle Sizing Sampler (Mark II) fitted with a USP glass throat was used to determine particle size distributions by BDP specific HPLC. The Quartz Crystal Microbalance (QCM) Cascade Impactor System was used immediately after radiolabeling as a preliminary quality check before proceeding to subject use. The data from the Andersen Impactor was used as the primary data for validation purposes and is depicted in Figures 1 and 2. Before the labeling procedure was begun, the canister containing the formulation was actuated into an Andersen Sampler (i.e., “BEFORE”). After the mass of the drug and activity per actuation were determined, the labeled canister was actuated into a second Andersen Sampler (i.e., “AFTER”). The “BEFORE” and “AFTER” mass distributions for each MDI were compared with each other and with the radiolabel distribution. During validation, the radiolabel and mass of the drug were also compared 24 h after the preparation of the inhaler. The subjects used the radiolabeled inhalers within 6 h of preparation. The amount of radiolabeled drug in the actuator and USP throat was also measured. If the particle size distributions agreed (i.e., original manufacturing specifications were met), the formulation was considered properly labeled for the clinical study. Medication delivery as determined by HPLC was also tested to ensure that the values were within original specifications.

Andersen Cascade Impactor data showing the distribution of HFA-BDP mass before and immediately after radiolabeling, radioactivity counts after radiolabeling, and mass and counts after patient use, measured 24 h later.
Andersen Cascade Impactor data showing the distribution of CFC-BDP mass before and immediately after radiolabeling, radioactivity counts after radiolabeling, and mass and counts after patient use, measured 24 h later.
Gamma camera imaging technique
After the inhalation of the 99mTc-labeled drug by the subjects, the following 90-sec image regions were obtained: posterior thorax, anterior thorax, anterior upper abdomen, posterior upper abdomen, left lateral oropharynx, actuator, spacer, and exhalation filter. Final results were not multiplied by tissue attenuation factors. Such use of attenuation factors is debatable and in this case less important because of the relative homogeneity of the subject population. The subjects were instructed not to speak or swallow until the scans were completed, thus minimizing the amount of drug in the stomach. Each subject received a Xenon-133 lung ventilation imaging procedure performed using standard clinical imaging techniques. These images provided an outline of the lungs to which the labeled drug scintigraphs were compared.
The total counts obtained from the anterior and posterior views of the thorax and abdomen were averaged and then summed with the oropharynx activity to give total counts within the subject.
Example:
Clinical study design
The study was performed in accordance with Good Clinical Practices, Good Laboratory Practices, and the ethical principles enunciated in the revised Declaration of Helsinki. The study was approved by the University of Minnesota institutional review board, and written informed consent was obtained from each subject.
This was an open-label, nonrandomized study utilizing 12 healthy male subjects assigned to different exposure regimes (described in Tables 2 and 3) to determine the drug deposition and distribution of radiolabeled HFA-BDP and CFC-BDP from two common spacer devices: Aerochamber and Volumatic.
When comparing spacer delay effects, the studies were performed with a single radiolabeled canister to reduce radiolabeling variability effects; however, this required two different subject groups. In most cases the identical set of subjects was not used in a crossover fashion when comparing spacer versus no spacer effects.
The essential aspect of this study was to assure standardization of inhaler techniques. Standardization of inhalation technique was achieved through the use of a custom Breath Pattern Monitor previously described.(9) The Breath Pattern Monitor allowed subjects to observe a visual display of their breath pattern on a computer screen in real time. Subjects were trained to reproduce the desired breath pattern, ensuring standardization of inhaled doses. The subjects were instructed to target a 10-sec breathhold in every case except where stated in the results.
Radiolabeled BDP canisters were prepared on the morning of each study day. One inhalation consisting of no more than 400 microcuries was administered per subject on each study day. Following inhalation, deposition of the drug in the lungs, upper abdomen, oropharynx, the inhaler mouthpiece, spacer, and the amount the subject expired into an exhalation filtertrap were measured by gamma scintigraphy.
Healthy male subjects between 25 and 50 years of age (inclusive) were screened for the study. All subjects were nonsmokers for at least 1 year and have a <10 pack-year smoking history. Subjects had a screening FEV1>85% of predicted normal. All subjects demonstrated acceptable technique in the use of an MDI and reproducibility of their inspiratory flow patterns (i.e., inspiratory times of 2.8–3.5 sec and breath holds of 9–11 sec) using the Breath Pattern Monitor. Safety was assessed by collection of adverse events, vital signs, and physical examination.
Statistical analysis
There were three subjects per testing condition (described in Tables 2, 3, and 4). Therefore, the study was not powered to enable formal hypothesis testing to be conducted. Thus, summary statistics alone are expressed, specifically, means and standard deviations.
Results
Demographic and baseline lung function values are presented in Table 1. Representative radiolabeling validation graphs for HFA-BDP and CFC-BDP are presented in Figures 1 and 2. Two impactor runs were performed for each radiolabeled MDI: one prior to the radiolabeling process, and one immediately after the radiolabeling process. After radiolabeling, each plate was counted for radioactivity and then assayed chemically. The radioactivity versus mass per Andersen stage was again checked after subject use. These measurements of before and after radiolabeling chemical analyses and after radiolabeling radioactivity analysis are shown graphically in Figures 1 and 2. Results of the radiolabeling validations showed that: (1) the radiolabeling process did not alter the particle size distribution of the original products. That is, the chemical specific mass of the drug at each stage did not change after the radiolabeling process, and (2) the radioactivity count distribution closely matched the mass distribution of the drug after radiolabeling.
Breathing pattern data collected in real-time during the actual inhalation dosing showed that the subjects achieved the target of an on-time actuation, an inspiratory time of 3 sec and a breathhold of 1 or 10 sec. The subjects received less than 10 min of training on the Breath Pattern Monitor on each study day.
The results depicted in Table 2 show that the use of Aerochamber with HFA-BDP does not substantially alter lung deposition with or without a 2-sec spacer delay. There was, however, a decrease in oropharyngeal deposition with values going from approximately 28% to 3–5%. The amount of drug held in the Aerochamber accounted for the reduction in oropharygeal drug deposition. The results in Table 2 demonstrate that lung deposition with CFC-BDP is low (approximately 3–7%) with and without Aerochamber and/or spacer delays. Similar to HFA-BDP, CFC-BDP also demonstrated less oropharyngeal deposition with the spacer.
Mean percent of ex-actuator dose ± standard deviation.
n = 3/formulation.
Abdominal deposition was <2% in all cases.
The results depicted in Table 3 with the Volumatic spacer generally paralleled those obtained with the Aerochamber. However, a 2-sec spacer delay with the Volumatic spacer caused a decrease in lung deposition with HFA-BDP accounted for by an increase in spacer deposition. This did not appear to be the case using CFC-BDP with a spacer delay where there was no difference in deposition distribution.
Abdominal deposition was <2% in all cases except CFC-BDP-250 where it was equal to a mean of 6%.
n = 3/formulation.
Mean percent of ex-actuator dose ± standard deviation.
Not conducted.
The results depicted in Table 4 show that the small particle HFA-BDP requires the normal, recommended 10-sec breathhold to optimize lung deposition. A 1-sec breathhold reduced lung deposition by 16%. The difference was accounted for in the exhaled deposition fraction. Lung deposition for the large particle CFC-BDP was not affected by breathhold.
Mean percent of ex-actuator dose.
n = 3/group.
Discussion
This study was considered to be preliminary in nature in the sense that it was not powered to draw valid statistical conclusions. Rather, the series of comparisons described in this study was designed to demonstrate qualitative differences in inhalers, spacers, and circumstances of clinical use. This report demonstrated that as previously described, Aerochamber and Volumatic spacers reduce steroid deposition in the oropharynx and do so over a wide range of particle sizes. However the smaller particle sized products (HFA-BDP-40 and HFA-BDP-80) showed less decrease in lung deposition when subjects exhibited a delay in inspiration after MDI actuation compared with the larger particle sized CFC-BDP.
Clinicians often consider spacers as accomplishing three things. First, their use is presumed to reduce or eliminate discoordination issues. The results of the study cited here as well as in other publications(20) show that with a small particle drug aerosol (i.e., 1.0–1.5 microns MMAD), discoordination issues are reduced with or without a spacer. Second, spacers are generally perceived to reduce oropharyngeal deposition. This assumption appears to be true when using large or small particle MDIs. However, small particle MDIs have less oropharyngeal deposition without a spacer. Third, it is believed that spacers increase lung deposition. However, the results of this study show that lung deposition is relatively unaffected when using small particle aerosols (i.e., HFA-BDP) and either the same or perhaps slightly less when using large particle MDIs (i.e., CFC-BDP) with spacers. It is conceivable that large particle aerosols that are agglomerates of smaller particles may benefit from some deagglomeration in spacers and thus produce a higher fine particle fraction, but this was not observed in this study.
Spacers are primarily designed to reduce oropharyngeal deposition and reduce the need for coordination of actuation with inspiration when used with an MDI. Spacers accomplish this by reducing the ballistic component of the aerosol plume. Spacers are presumed to take the initial impaction of the aerosol, which can be as high as 30 meters per second of velocity, and reduce it considerably. Deposition of aerosols can be thought of as the product of force behind the particle as well as the size (or mass) of the particle. Thus, a large particle with a high velocity will tend to deposit very quickly in the line of fire area of either a spacer or the oropharynx. Alternatively, a small particle with less velocity can follow a curved path and stay suspended for a longer period of time. The hypothesis in this study was that smaller particle drugs (i.e., HFA-BDP) would have a positive effect on lung deposition when used with spacers. The results of this study support this hypothesis.
There have been several reported studies using MDIs and spacer delays in the literature. Clark and Lipworth(13) showed in a clinical study that delayed inhalation of salbutamol from a Volumatic™ spacer resulted in a twofold reduction in lung bioavailability of salbutamol. Barry and O'Callaghan(14) examined the use of budesonide MDI with the Nebuhaler™ spacer and a 10-sec delay in an in vitro experiment. They reported a decrease of fine particle mass from 31 to 23 μg of the 200-μg dose label claim with a spacer when using a 10-sec delay. Despite the shortcomings of spacers, the British Thoracic Society guidelines recommended the use of spacers with beta-agonists as an alternative to nebulizers.(15)
An additional consideration in the use of spacers in the pediatric population is that the lung surface area in very young children is smaller than adults and thus the fixed delivered dose of an inhaled steroid, per square centimeter of lung surface area, may be higher with children as opposed to adults. In this regard, Devadason et al.(16) conducted a radiolabeled deposition study of HFA-BDP without a spacer in children ages 5–15 years old. They reported lung deposition values greater than 37% in children 5–7 years old and 54% in 11–17 year olds. Another study reported by Roller et al.(17) was conducted in mild asthmatic children ages 5–7 with HFA-BDP and the Aerochamber Plus™. Lung deposition was approximately 35% during tidal breathing through the spacer. However, lung deposition rose to 58% with a normal 10-sec breathhold. Lung deposition in children 8–17 years of age also showed a similar effect of increased lung deposition with a spacer when using a 10-sec breathhold versus spacer tidal breathing.
HFA-BDP has a particle size of approximately 1.1 microns with a geometric standard deviation of approximately 2. CFC-BDP has a particle size of approximately 3.5 microns with a geometric standard deviation of 1.9. Additionally, the valve size of HFA-BDP is 50 μL with approximately 45 μL of propellant supplying the velocity to the plume. CFC-BDP uses a 63-μL valve with nearly 63 μL of propellant supplying the velocity of the plume. Thus, the larger particle size drugs with more force propelling them should have greater drug impaction and retention within a spacer. Because the larger particles are deposited very quickly, fewer drug particles remain suspended within the spacer, thereby potentially providing less benefit to a patient when there is a delay before the patient breathes. By contrast, a smaller particle that stays suspended longer has the potential to provide greater advantage to a patient when there is a delay in emptying the spacer. Although drug particle size is not taken into consideration in asthma treatment guidelines, the use of spacers in the pediatric population continues to be recommended in guidelines issued by GINA, NAEPP, and the British Thoracic Society for both steroids and beta-agonists (Dolovich et al.(18)).
The data described in this study showed that spacers used with HFA-BDP can deliver meaningful drug quantities to patients. Incorporating spacer delays with any product is not recommended. However, it is recognized that with certain patient populations (e.g., pediatric patients), some delay between actuating and breathing may occur, thus resulting in a spacer delay. A 2-sec delay is actually a long delay in time, but it appears to be a common clinical occurrence. Delays up to 10-sec appear far less clinically relevant and are not recommended for use with any inhaled product. MDI aerosols with smaller particle size can clearly stay suspended in air more than formulations with larger particle sizes. Thus, HFA-BDP with its small particle size of 1.1 microns delivered more drug when spacer delays occurred compared with the larger particle steroid, CFC-BDP.
The results of this study confirmed the high lung deposition of HFA-BDP compared with CFC-BDP previously reported.(6,7.,9,19,20). An additional study also showed that HFA-BDP delivered 53% lung deposition compared with 4% lung deposition for CFC-BDP and 13% for CFC-fluticasone.(21) The mass median aerodynamic diameter was 0.9, 2.0, and 3.5 microns for HFA-BDP, CFC-fluticasone, and CFC-BDP, respectively.(19) This finding is consistent with the notion that particle size heavily influences lung deposition, either with or without spacers. Studies with other small particle steroids such as HFA-ciclesonide have confirmed high lung deposition (i.e., 52%) in healthy adults.(21)
Smaller drug particles in the HFA-BDP spray remain suspended longer in the air and allow the patient more time after actuation to inhale. This was exemplified in a previous study whereby results without spacers showed that in asthmatics, lung deposition of HFA-BDP was only decreased from approximately 59 to 37% under severe patient breathing discoordination conditions, using a press and breather inhaler.(20) This high lung deposition value of 37% under extreme discoordination circumstances was higher than the best lung deposition value of CFC-BPD of less than 10% under obtained under coordinated patient use.
In summary, the spacer study described here supports the value of having small particles able to remain suspended in inspiratory air. All of the factors cited previously including particle size, spray force, spray temperature, spray duration, and the use of spacers support the “forgiving” aspect of small particle aerosols such as HFA-BDP in that high lung deposition values can be shown to occur in both patients with and without the ability to coordinate actuation with inspiration and irrespective of spacer use.
Footnotes
Acknowledgments
The studies described in this manuscript were funded by 3M Pharmaceuticals, the commercial developer of the QVAR™ press & breathe metered dose inhaler. The manuscript preparation was funded by Teva Specialty Pharmaceuticals. The authors thank Patricia Davidson, M.S., Robert Boudreau, M.D., Bruce Hasselquist, Ph.D., Jim Tennison, B.S., Tim Bredow, Ph.D., Jennie VandenBurgt, B.S., and Christopher Lyle, M.S., for their expert technical assistance.
Author Disclosure Statement
The authors declare no conflicts of interest exist.