
Abstract
Abstract
Background:
Droplet evaporation has been known to bias cascade impactor measurement of aerosols generated by jet nebulizers. Previous work suggests that vibrating mesh nebulizers behave differently from jet nebulizers. Unlike jet nebulizers, vibrating mesh nebulizers do not rely on compressed air to generate droplets. However, entrained air is still required to transport the generated droplets through the cascade impactor during measurement. The mixing of the droplet and entrained air streams, and heat and mass transfer occurring downstream determines the final aerosol size distribution actually measured by the cascade impactor. This study is aimed at quantifying the effect of these factors on droplet size measurements for the case of vibrating mesh nebulizers.
Methods:
A simple droplet evaporation model has been applied to investigate aerodynamic size measurement of drug aerosol droplets produced by a proprietary vibrating mesh nebulizer. The droplet size measurement system used in this study is the Next Generation Impactor (NGI) cascade impactor. Comparison of modeling results with experiment indicates that droplet evaporation remains a significant effect when sizing aerosol generated by a vibrating mesh nebulizer.
Results and Conclusions:
Results from the droplet evaporation model shows that the mass median aerodynamic diameter (MMAD) measured by the NGI is strongly influenced not only by the initial droplet size, but also by factors such as the temperature and humidity of entrained air, the nebulizer output rate, and the entrained air flow rate. The modeling and experimental results indicate that the influence of these variables on size measurements may be reduced significantly by refrigerating the impactor down to 5°C prior to measurement. The same data also support the conclusion that for the case of nebulized drug solutions, laser diffraction spectrometry provides a meaningful droplet sizing approach, that is simpler and less susceptible to such droplet evaporation artifacts.
Introduction
The droplet evaporation phenomena and the effect on size determination has been widely studied for the case of jet nebulizers.(1–3) Approaches proposed to mitigate this effect have focused on suppressing droplet evaporation through temperature control, for example, cooling of the impactor,(3–5) or by humidifying the entrained air.(6) The picture is not so clear for the case of vibrating mesh nebulizers, which do not rely on compressed air atomization for aerosol generation. A recent study by Hardaker et al.(7) suggests that mesh nebulizers behave differently from jet nebulizers, when their respective size distributions are measured with a Next Generation Impactor (NGI) in the cooled and ambient state. In comparison to the jet nebulizer, a smaller size difference between the cooled and uncooled state measurements was observed for the case of vibrating mesh nebulizers. Hardaker et al. hypothesized that droplet evaporation does not entirely explain this difference in nebulizer behavior, and suggested that other phenomena such as droplet coalescence may be responsible for these observations.
The goal of the present study is to gain a better understanding of droplet evaporation effects during measurement for the case of vibrating mesh nebulizers. Specifically, a theoretical model of droplet evaporation has been used to estimate measurement bias during NGI cascade impactor characterization of liquid aerosols generated using a vibrating mesh nebulizer. The theoretical model provides a basis for explaining the previously observed differences in behavior between jet and vibrating mesh nebulizers. The theoretical model has been evaluated by comparing modeling results with available experimental data for the case of antibiotic aerosols generated using a prototype nebulizer. The droplet evaporation model has then been used in a predictive manner to assess the significance of various factors in biasing impactor size measurements. Approaches for minimizing the impact of extraneous factors on size measurement have been evaluated. It is shown that the cooled NGI approach is effective in reducing impactor measurement bias even for the case of aerosols produced by a vibrating mesh nebulizer. Alternative approaches such as humidifying the entrained air are also predicted to work.
Experimental: Description of Nebulizer Test Setup
The vibrating mesh nebulizer used in this study is a development prototype of the Novartis liquid pulmonary drug delivery system (PDDS). Earlier design variants of this system, and its mode of operation have been described by Dhand.(8) The PDDS has a drug reservoir that communicates with a piezo-electric driven vibrating mesh assembly. When activated by an electronic controller, the vibrating mesh generates a continuous droplet stream.
The performance of the PDDS is characterized by the droplet size distribution of the generated aerosol, and the corresponding liquid output rate Ql. The output rate Ql is typically measured by timing the duration needed to aerosolize a given metered volume of drug. For the case of nebulized drug solutions, laser diffraction provides a rapid and precise method to characterize the aerosol size distribution at the point of generation, essentially free from evaporation or condensation effects.(9,10) In this study, the laser diffraction size distributions have been reported in terms of the volume weighted median droplet diameter (VMD) di, measured at the exit of the PDDS nebulizer. The laser diffraction system used in this study is the Malvern Spraytec (Malvern Instruments, Inc., Westborough, MA, USA).
For the case of nebulizers as for other inhaled drugs, regulatory bodies expect characterization of the aerodynamic particle size distribution by a cascade impactor. For unit density spheres (e.g., droplets of dilute aqueous drug solutions), the droplet geometric size measured by laser diffraction is expected to correlate well with the aerodynamic size measured by cascade impaction. However, because cascade impactor measurements are more susceptible to droplet evaporation in the sampling train, such correlations may not be readily apparent unless care is taken to minimize droplet evaporation.
In this study, the NGI (MSP Corp, Minneapolis, MN, USA) has been used to characterize nebulized aerosols from the PDDS. A schematic diagram of the cascade impactor test system is shown in Figure 1. The nebulizer is coupled to a “T-piece” which is mounted at the entrance of the USP induction port connected to the NGI impactor. Ambient entrained air (at temperature Ta, relative humidity, Ha) is used to convey the droplet stream generated by the PDDS into the NGI cascade. The flow rate of entrained ambient air, Qa, is set using an adjustable metering valve, and is monitored using a flow meter (Model 4040, TSI Inc., Shoreview, MN, USA). The aerosol drug deposited in the collection cups is assayed using a drug-specific HPLC method. For convenience, the size distribution obtained from the cascade impactor is reported in terms of the mass median aerodynamic diameter (MMAD).
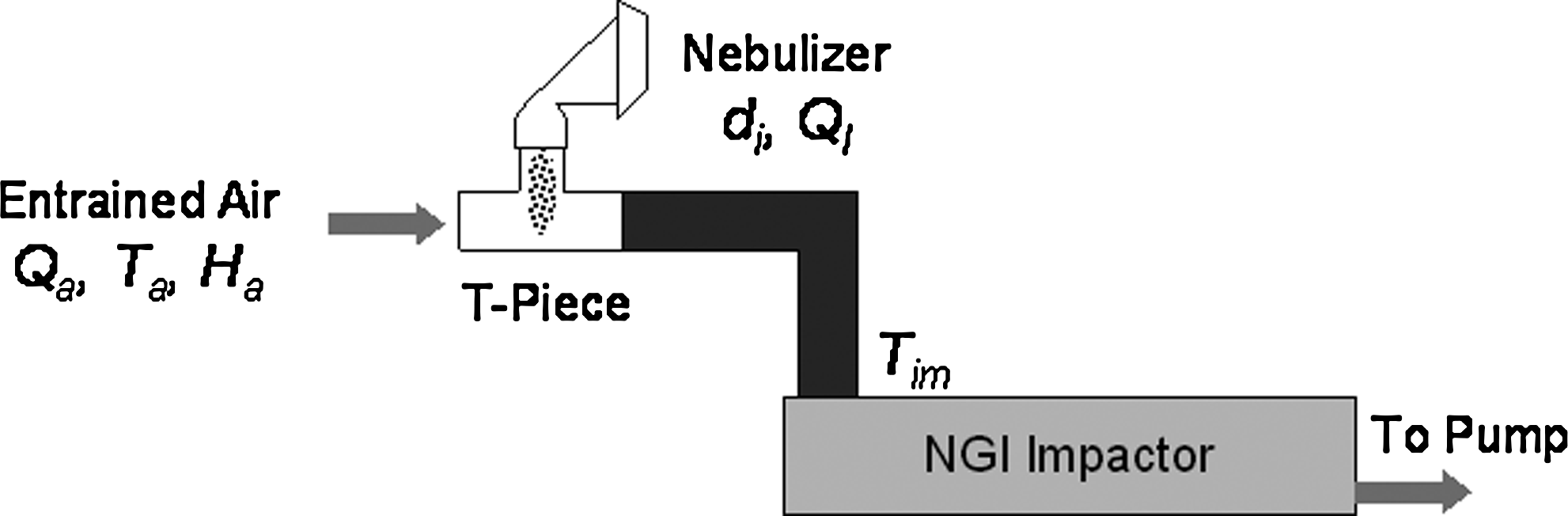
Schematic diagram of NGI test setup.
The MMAD determined using the NGI test setup in Figure 1 is expected to track the droplet size di generated at the nebulizer exit (as measured by laser diffraction). The MMAD for the case of vibrating mesh nebulizers is also strongly influenced by additional factors, such as the entrained air flow rate, temperature, and humidity (Qa, Ta, Ha), the nebulizer output rate Ql, and the impactor temperature Tim. For example, droplet evaporation, and thus a bias towards smaller size is favored if the entrained air is not saturated (Ha <100%), and/or if the aerosol concentration is low (i.e., ratio of liquid flow to entrained air flow, Ql/Qa, is small).
The droplet evaporation model, presented in the next section, has been used to assess the influence of these various factors; to help in correct interpretation of the test results; and to improve the correlation between laser diffraction and cascade impactor data by reducing the influence of extraneous variables.
Theory: Droplet Evaporation Model
The droplet evaporation model is similar to previously published models,(11–13) but has been adapted and applied to the specific situation of the nebulizer characterization setup described in Figure 1. The model assumes the following:
The drug solution in the PDDS is equilibrated to ambient temperature prior to aerosolization. The droplet generation mechanism does not affect the temperature of the drug in the reservoir or in the emitted droplets. The droplets generated from the PDDS are monodisperse with initial size di. The droplets do not undergo coalescence or deposition in the USP induction port. Changes in droplet number concentration due to Ostwald ripening are neglected. The mixing of droplet and entrained air streams is instantaneous and uniform. The mass and heat transfer between droplets and surrounding air is diffusion dominated. Heat transfer between entrained air and flow channel walls is efficient and rapid. For the case where the impactor temperature is different from ambient (e.g., for a refrigerated impactor), the free stream temperature of the entrained air rapidly reaches the impactor temperature Tim. The drug being nebulized is a dilute solution having a bulk density and specific heat close to that of water. The depression of water vapor pressure due to the presence of solute is assumed to follow Raoult's law, while for small droplets, the Kelvin surface curvature effect is assumed to apply.
The model is then described by a coupled set of three ordinary differential equations (ODE), for the time-dependent droplet size dp, droplet temperature Td, and water vapor partial pressure P∞ [Equations (1–3) below]. Based on assumption (5) above, a separate governing equation for free stream temperature T∞ of the entrained air has not been included, as T∞ is assumed to rapidly attain the impactor temperature Tim. The above approximation is expected to affect the droplet evaporation kinetics to some degree, but not as much the final equilibrium droplet size.
In the equations above, t is time, R is the universal gas constant, Dw is the diffusivity of water vapor in air, and ka is the thermal conductivity of air; Mw, ρw, hw, and Cpw are, respectively, the molecular weight, density, latent heat of vaporization, and specific heat of water; Pd and P∞ are, respectively, the partial pressure of water vapor at the droplet surface and free stream; Td and T∞ are, respectively, the droplet and the free stream temperature; Cs and CT are the Knudsen correction factors for mass and heat transfer; and Nd is the droplet number concentration.
The above equations are solved numerically using an ODE solver in the Mathcad engineering calculation software, subject to the following initial conditions:
where di is the initial droplet size at the nebulizer exit, and Ps is the equilibrium saturation water vapor pressure at temperature Ta. The droplet number concentration in Equation (3) is given by the following,
Equation (7) assumes the aerosol generated by the nebulizer is monodisperse with initial droplet size di. In treating a polydisperse aerosol as monodisperse, a logical choice for di would be the “diameter of average surface area” of the emitted aerosol, based on the theoretical expectation that the evaporation rate is proportional to the exposed droplet surface area. As a practical matter, di is set here to a size metric that is more readily available, that is, the volume median diameter at the nebulizer exit, as measured by laser diffraction. This, and other departures from ideality as represented in the assumptions stated above are accounted for by introducing an empirical correction factor ϕ of order unity in Equation (7). The factor ϕ is determined by comparing theory with experiment for a representative data set.
The model described in Equations (1)–(7) above accounts for all of the variables previously described in Section 3 as influencing the measured MMAD. These variables (i.e., T a , H a , Q a , D i , Ql, Tim) are inputs to the calculation above, and the evolution of droplet diameter with time is obtained as the desired output. It should be noted that treating the droplet size distribution as monodisperse permits the droplet evaporation dynamics to be described by a reasonably simple set of mathematical equations that are straightforward to solve. However, this simplification implies that the model cannot be used to predict “second-order” effects such as the evolution in the spread of the droplet size distribution, for which more complex and computationally intensive numerical modeling approaches are necessary.(14,15)
Model Setup: Comparison of Modeling Results with Experiment
To set up the model, it is first necessary to determine the conversion factor ϕ. This has been done by comparing a single example set of experimental results with modeling results and adjusting ϕ to obtain good agreement between theory and experiment. The value of ϕ so obtained is then fixed for all future model computations.
The dataset selected for this exercise was one where the feasibility of sizing an nebulized antibiotic (120 mg/mL solution) using the NGI was examined. In this experiment, drug aerosol was sampled by the NGI at entrained air flow rates of 15 LPM and 30 LPM, respectively (see Table 1), and the aerosol size distribution determined using a drug-specific assay. The aerosol for both treatments was generated using a single PDDS unit with a measured drug output rate Ql of 0.296 mL/min and a median droplet size di of 4.3 μm (as measured by laser diffraction). The ambient conditions as represented by columns 4–6 in Table 1 were identical for the two treatments. The final column in Table 1 represents the MMAD obtained using the NGI. Comparing the MMAD with the di values clearly indicates that the droplets have undergone significant evaporation, with greater shrinkage occurring at the higher entrained air flow (condition B, 30 LPM).
As the droplet stream from the PDDS mixes with unsaturated entrained air, droplet evaporation causes the background water vapor concentration to increase. The extent of evaporation depends on the concentration of the resulting aerosol, which is related to the ratio Ql/Qa [see Equation (7)]. If the aerosol concentration is sufficiently high, droplet evaporation can cause the water vapor concentration to reach saturation levels, quenching further evaporation. A higher entrained air flow rate would lead to a more dilute aerosol, thus allowing for more evaporative shrinkage of droplets. The numerical model when applied to the above experiment is able to capture the observed dependence of MMAD on entrained flow. Figure 2 is a plot of calculated time traces of dp and P∞ for treatments A and B, and predicts that the evaporative reduction of droplet size and corresponding increase in water vapor concentration occurs rapidly (i.e., within 10s of milliseconds), until equilibrium is reached. The equilibrium size predicted by the model compares well with the experimentally measured MMAD for ϕ = 1.35, and this value has been used for all other calculations reported here.

Predicted trace of dp and P∞ for treatments A and B in Table 1.
Because the droplets are predicted to reach equilibrium, the final droplet size can also be estimated using a simple vapor mass balance expression, obtained by equating the water vapor mass evaporated from droplets to the mass required to saturate the entrained air. The expression may be written as follows:
where df is the equilibrium droplet size, and Ps(T) represents the equilibrium vapor pressure at the droplet surface at temperature T.
Model Predictions: Factors Affecting Impactor Measurement of Droplet Size for the Case of Vibrating Mesh Nebulizers
Having fixed the empirical correction factor ϕ, the droplet evaporation model has been used to predict the influence of different variables on the droplet size measured by cascade impaction. The effect of ambient temperature and pressure on MMAD is shown in Figure 3a and b, which are plots of predicted equilibrium droplet size as a function of Ta and P∞, for Qa = 30 and 15 LPM, respectively. The PDDS device of Figure 2 has been modeled here. Figure 3 suggests that for the case of vibrating mesh nebulizers, droplet evaporation remains a significant issue, and the measurement of MMAD is strongly influenced by the temperature and humidity of entrained ambient air. Note that the range of Ta and Ha in Figure 3 reflects that in an actively controlled laboratory environment—greater variation could be expected in uncontrolled environments. Although the sensitivity to environmental conditions is predicted to be smaller at Qa = 15 LPM, comparison of the MMAD against the initial droplet size di of 4.3 μm indicates that that a significant bias toward smaller size remains. The situation for vibrating mesh nebulizers is therefore not too different from that for jet nebulizers in this regard.
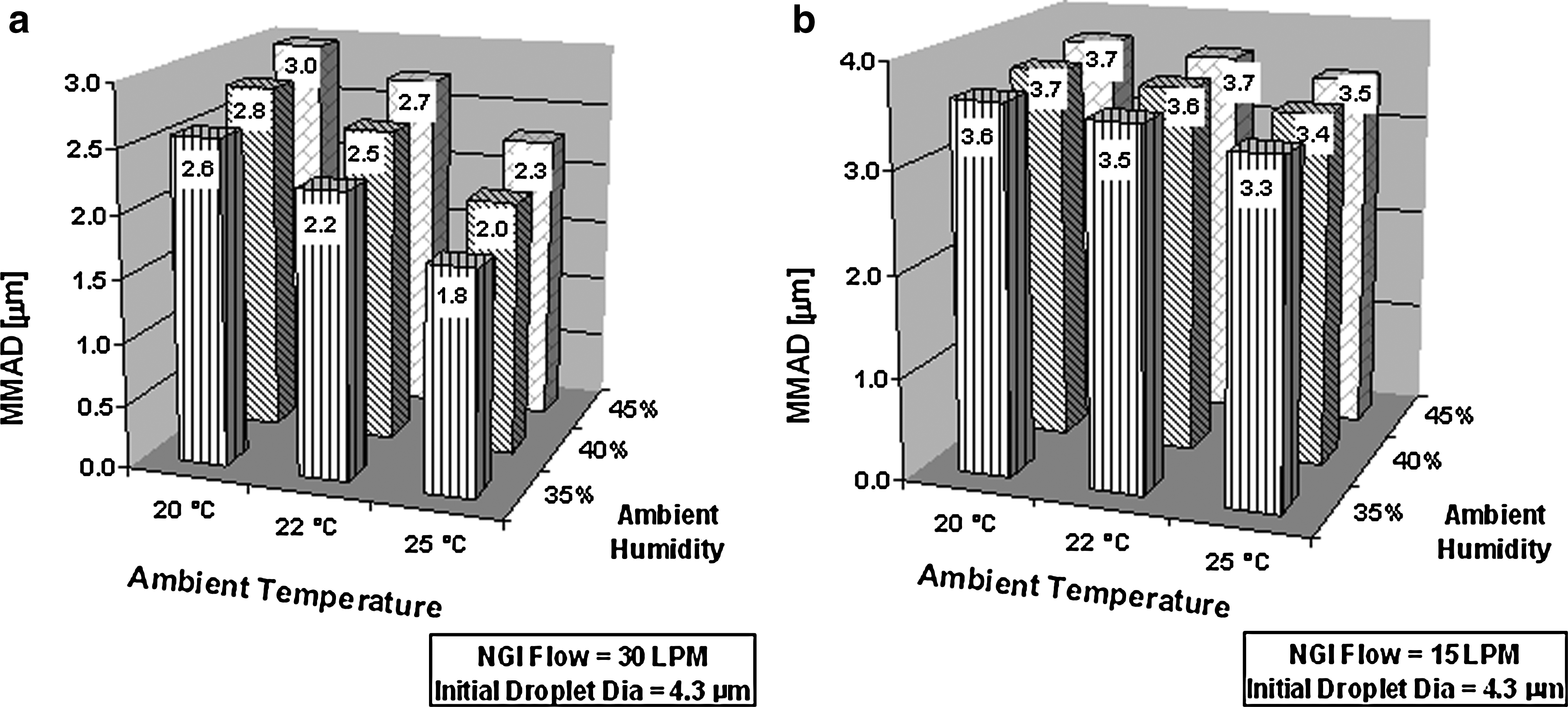
Predicted MMAD as a function of ambient temperature and humidity for the case of (
Application of the droplet evaporation model to the case of vibrating mesh nebulizers indicates that variance in the measured MMAD may arise from seemingly unexpected sources, for example, variability in the nebulizer output rate Ql. At constant Qa, as the liquid output rate Ql decreases, the aerosol concentration is lowered, evaporation is increased, and the MMAD is reduced. This trend is shown in Figure 4, for the case of di = 4.3 μm, Qa = 15 LPM, and Ql ranging from 0.1–0.5 mL/min. Figures 3 and 4 taken together suggest that correlation between droplet size measured by laser diffraction and cascade impactor may not be achieved unless the factors infleuncing droplet evaporation are accounted for.
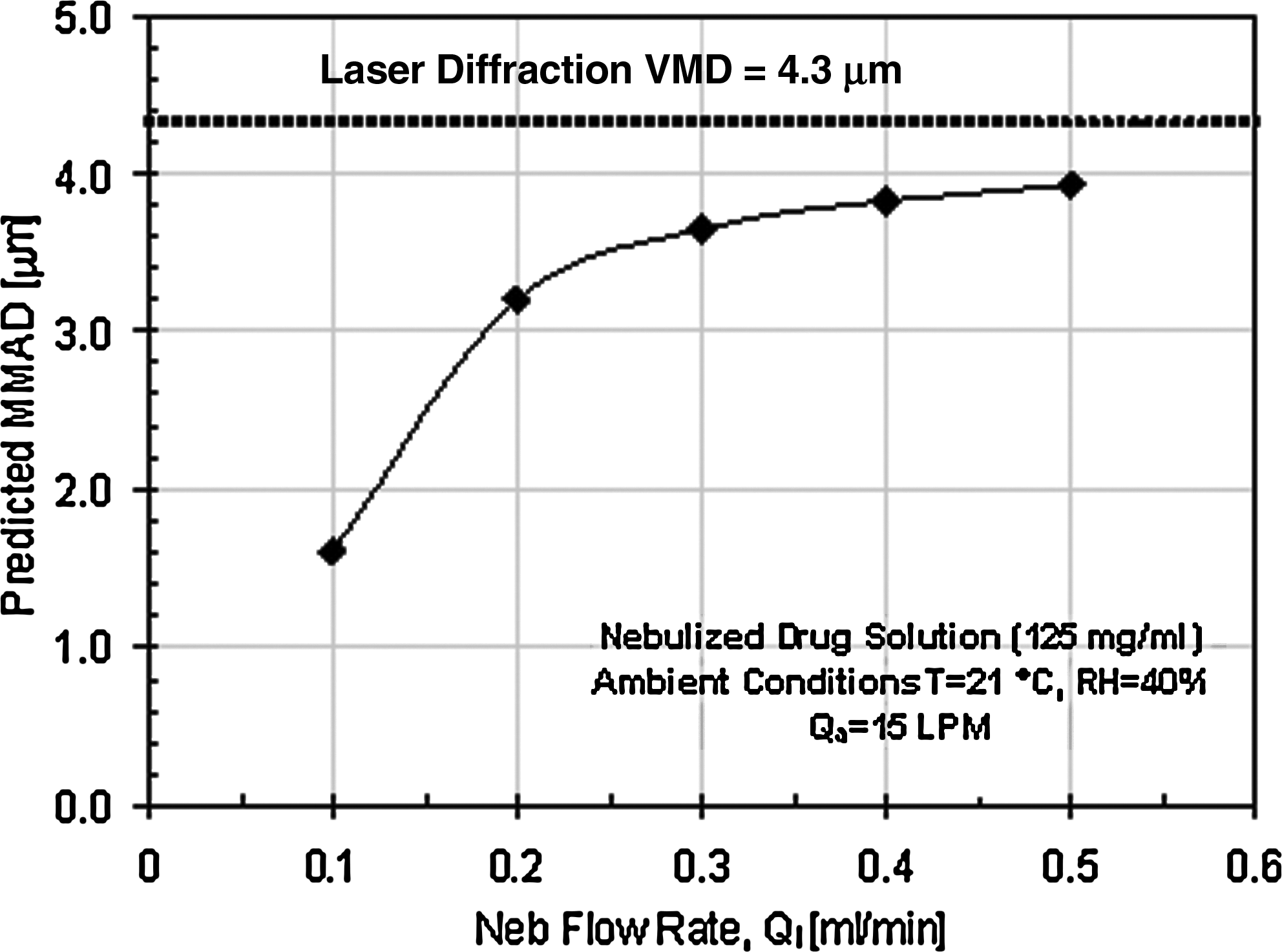
Predicted MMAD as a function of liquid output rate Ql.
This is clearly demonstrated by applying the droplet evaporation model to an experiment where laser diffraction and cascade impactor measurements were obtained for a well-defined set of experimental conditions. Table 2 represents a test matrix where drug aerosol from eight PDDS nebulizers covering a range of droplet size di and output rate Ql were measured using an NGI operating at an entrained air flow rate of 15 LPM. Ambient air temperature and humidity for these experiments were targeted at 70 F and 40%, and the actual values recorded during the run. The drug in this case is a nebulized antibiotic (125 mg/mL) solution in water.
Comparing the droplet size di measured by laser diffraction against the MMAD measured by the NGI indicates that significant droplet evaporation has occurred. Furthermore, correlation between the MMAD and di is poor (see Fig. 5, open squares) indicating that droplet evaporation is not uniform over the eight runs. However, when the numerical model is applied to this experiment using the values in Table 2 used as input, the predicted equilibrium droplet sizes correlate well with the experimentally measured MMAD (Fig. 5, solid diamonds). This suggests that the apparent poor correlation between laser diffraction and cascade impactor data is due to variance in droplet evaporation caused by external factors (i.e., Ta, Ha, Ql), and that better correlation may be obtained by accounting for these effects, or better still, entirely eliminating them.
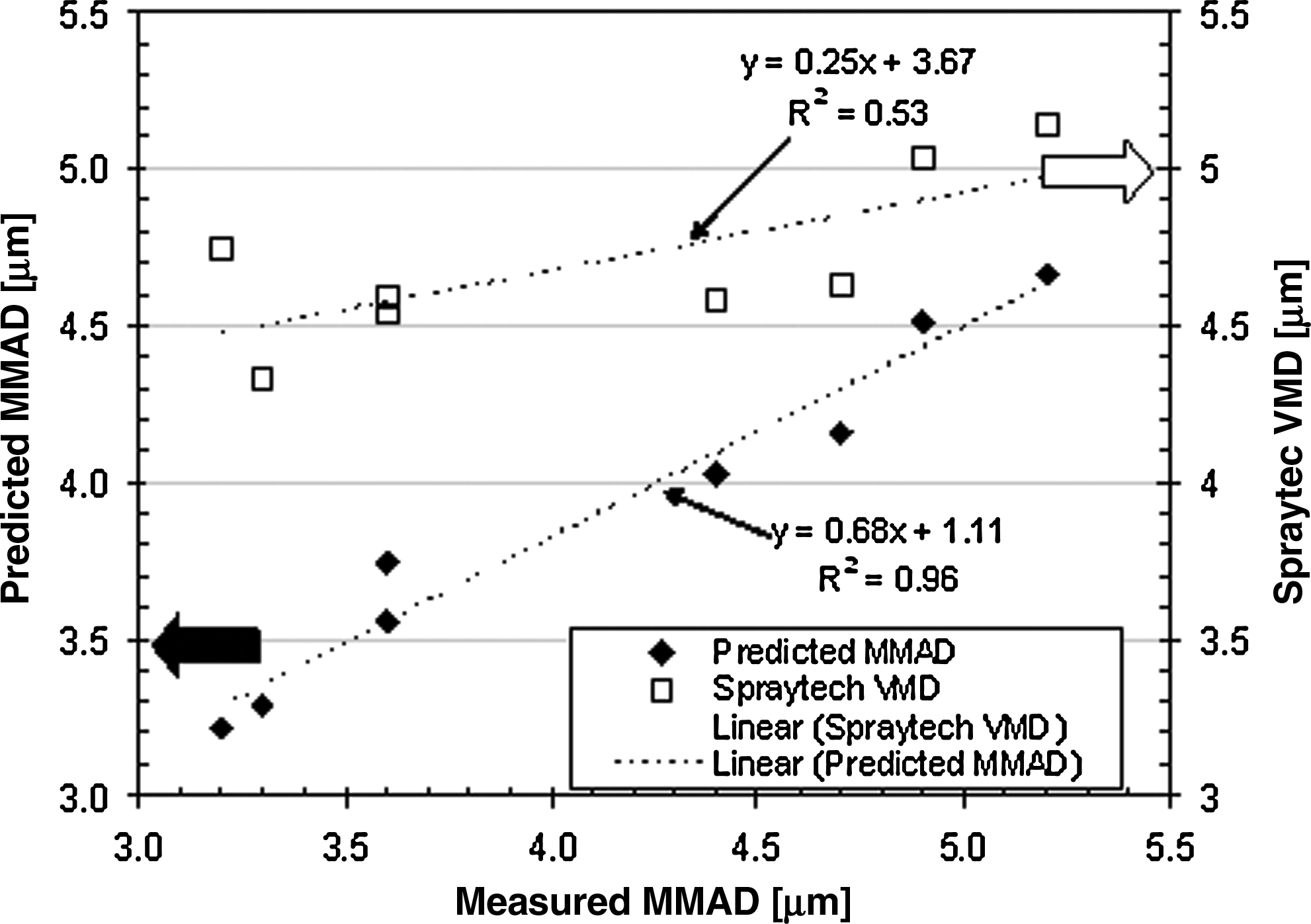
Correlation between (1) median droplet size measured by laser diffraction versus MMAD measured by NGI (open squares); and (2) equilibrium droplet size predicted by model versus MMAD measured by NGI (filled diamonds). Linear best fit lines to the data are also plotted.
Approaches to eliminating droplet evaporation during cascade impactor measurement include cooling or humidifying the entrained air.(3–6) Cooling of the impactor has been demonstrated to be an effective technique in minimizing droplet evaporation for the case of jet nebulizers.(5) Previous work suggested that the picture may not be as clear cut for the case of vibrating mesh nebulizers.(7) Applying the model to simulate the above approaches indicates that either of the approaches should work. Figure 6 shows plots of predicted droplet size as a function liquid flow rate for the two scenarios mentioned above. The drug modeled is a nebulized antibiotic solution (120 mg/mL), and the initial droplet size di is assumed to be 4.3 μm. The temperature and relative humidity of the entrained air are assumed to be 21°C and 40%, respectively. Figure 6a considers the case of humidifying the entrained air—the model predicts that humidifying the air from 40 to 95% relative humidity will essentially stop droplet evaporation, and thus eliminate the dependence of equilibrium droplet size on Ql. Figure 6b considers the case of cooling the entrained air—and again, it is seen that cooling the air from 21°C to 5°C eliminates the dependence of equilibrium size on Ql. Cooling causes the initially unsaturated entrained air to reach saturation, thus quenching droplet evaporation.
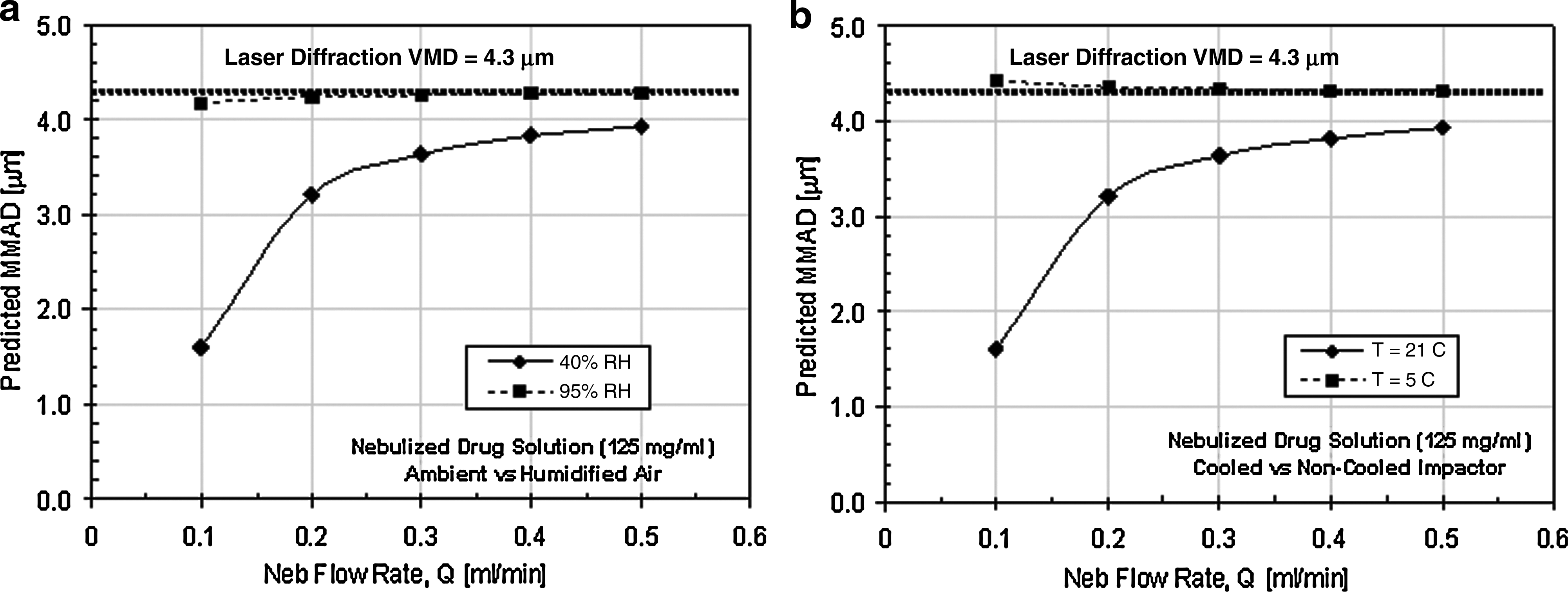
Predicted MMAD as a function of output rate, Ql: (
The model has also been used to assess whether cooling entrained air reduces sensitivity to ambient temperature and humidity. Figure 7 plots the final equilibrium droplet size as a function of initial temperature and humidity of entrained air. Comparing Figure 7 with Figure 3b, it is clear that cooling the entrained air to 5°C during impactor measurement greatly reduces sensitivity to ambient environmental conditions.
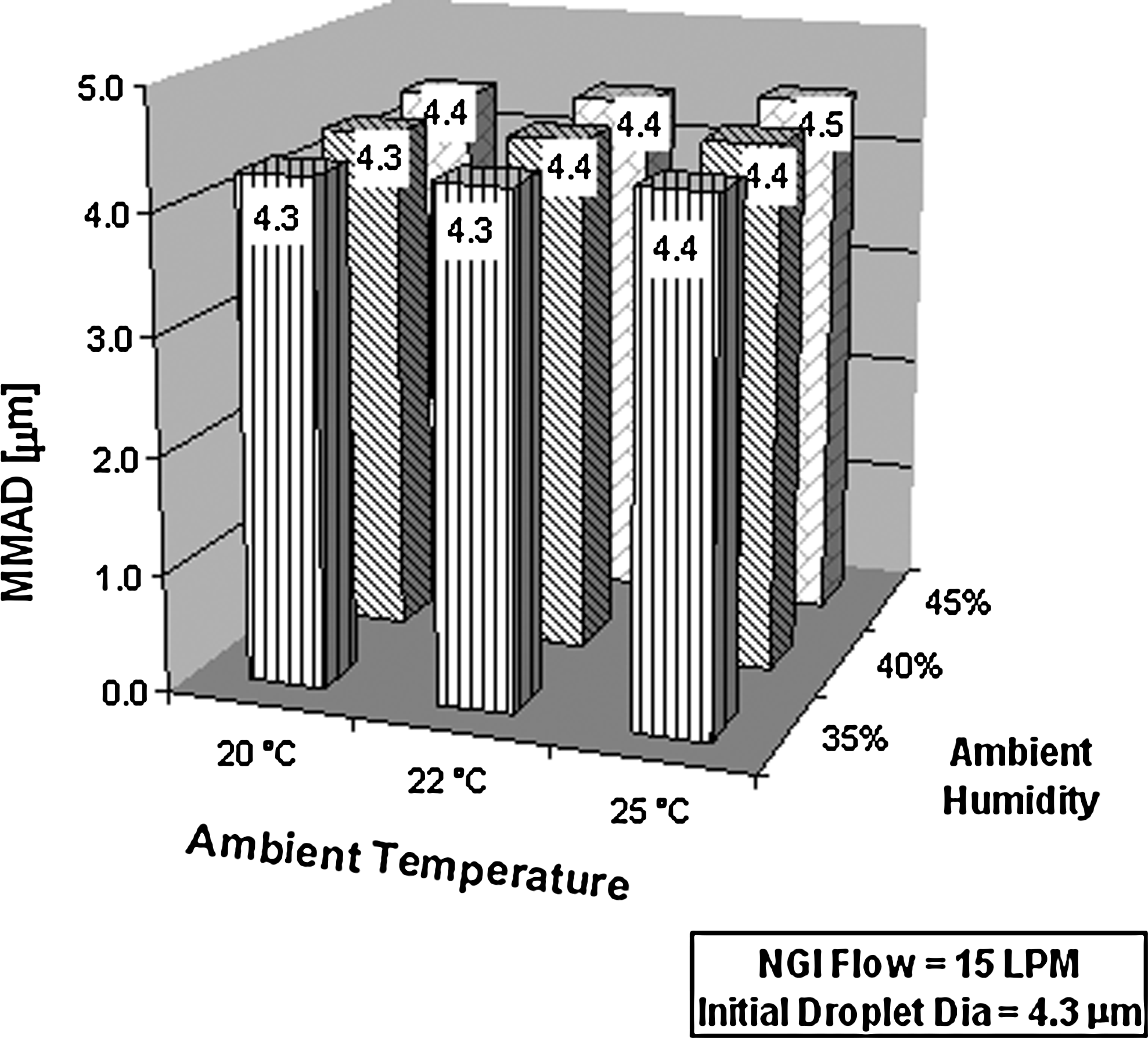
Predicted MMAD as a function of ambient air temperature and humidity for the case of cooled entrained air.
A simple experimental technique to cool entrained air during cascade impactor measurement is to refrigerate the impactor prior to measurement.(5) This approach has been experimentally tested here for the case of a vibrating mesh nebulizer. Table 3 presents the test matrix for this experiment, along with results obtained.
Nebulized drug aerosols were generated using two PDDS nebulizers with known di and Ql, and sized using the NGI in a cooled and ambient state. In addition, the effect of variation in entrained air flow Qa was also studied, by operating the NGI at flow rates from 14–16 LPM. The measured MMAD results indicate good agreement between laser diffraction and NGI data for the case of cooled impactor, but significant differences remain for the case of uncooled impactor. The same runs were also simulated using the droplet evaporation model, and the predicted MMAD compared against the actual MMAD measured by the NGI (see Fig. 8). The correlation between theory and experiment is quite good, indicating that the droplet evaporation model is able to capture the essential dynamics of the situation.
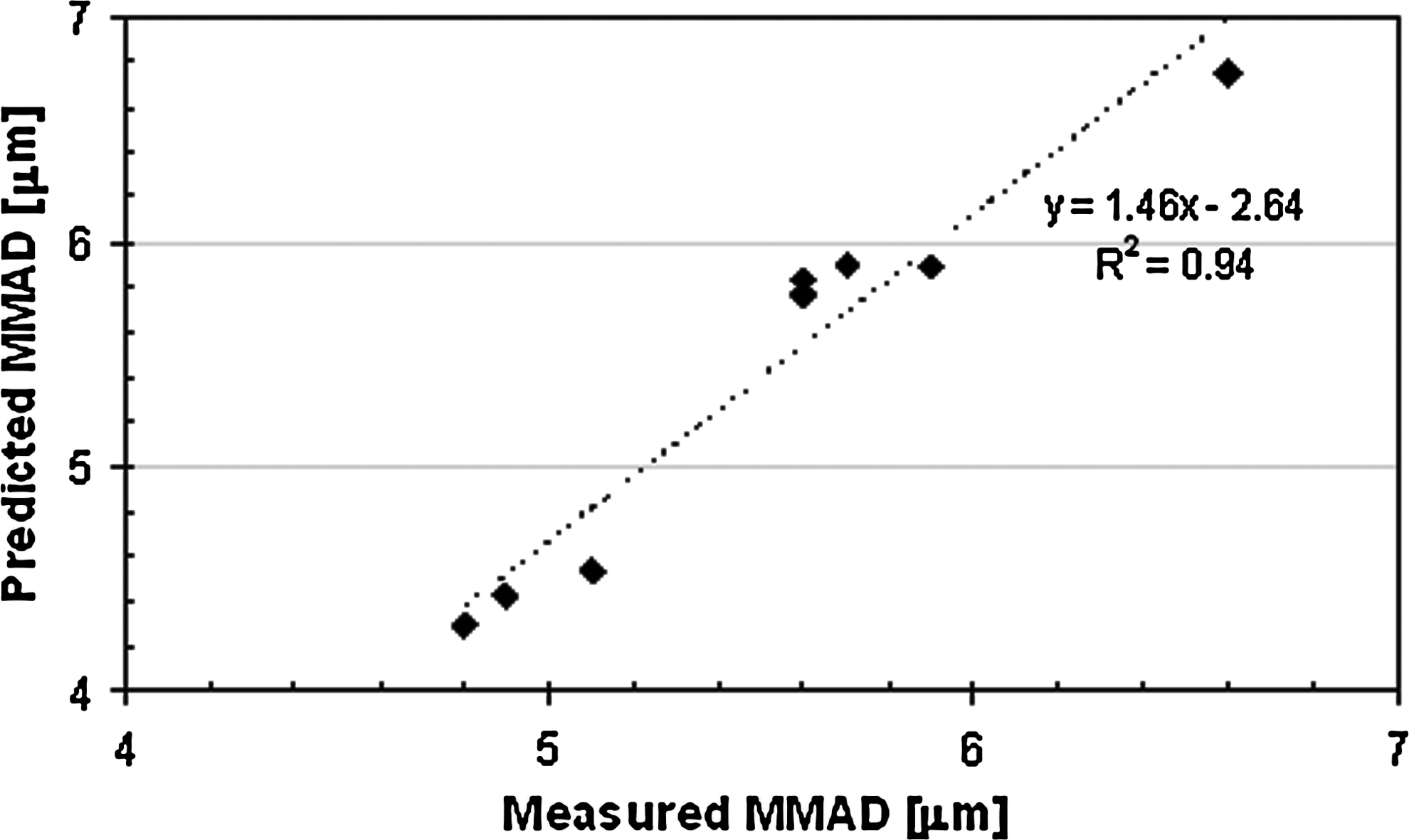
Correlation between theory and experiment for the test matrix presented in Table 3.
The robustness of the cooled impactor method has been assessed by using the model to predict the sensitivity of equilibrium droplet size to the temperature to which the entrained air is cooled. Figure 9 presents modeling results for the case of the two PDDS nebulizers used in the test matrix of Table 3. The dotted lines represent the volume median diameter measured by the laser diffraction system. It is seen that the MMAD measured by the NGI correlates well with the laser diffraction results as long as the entrained air is cooled below 9°C.
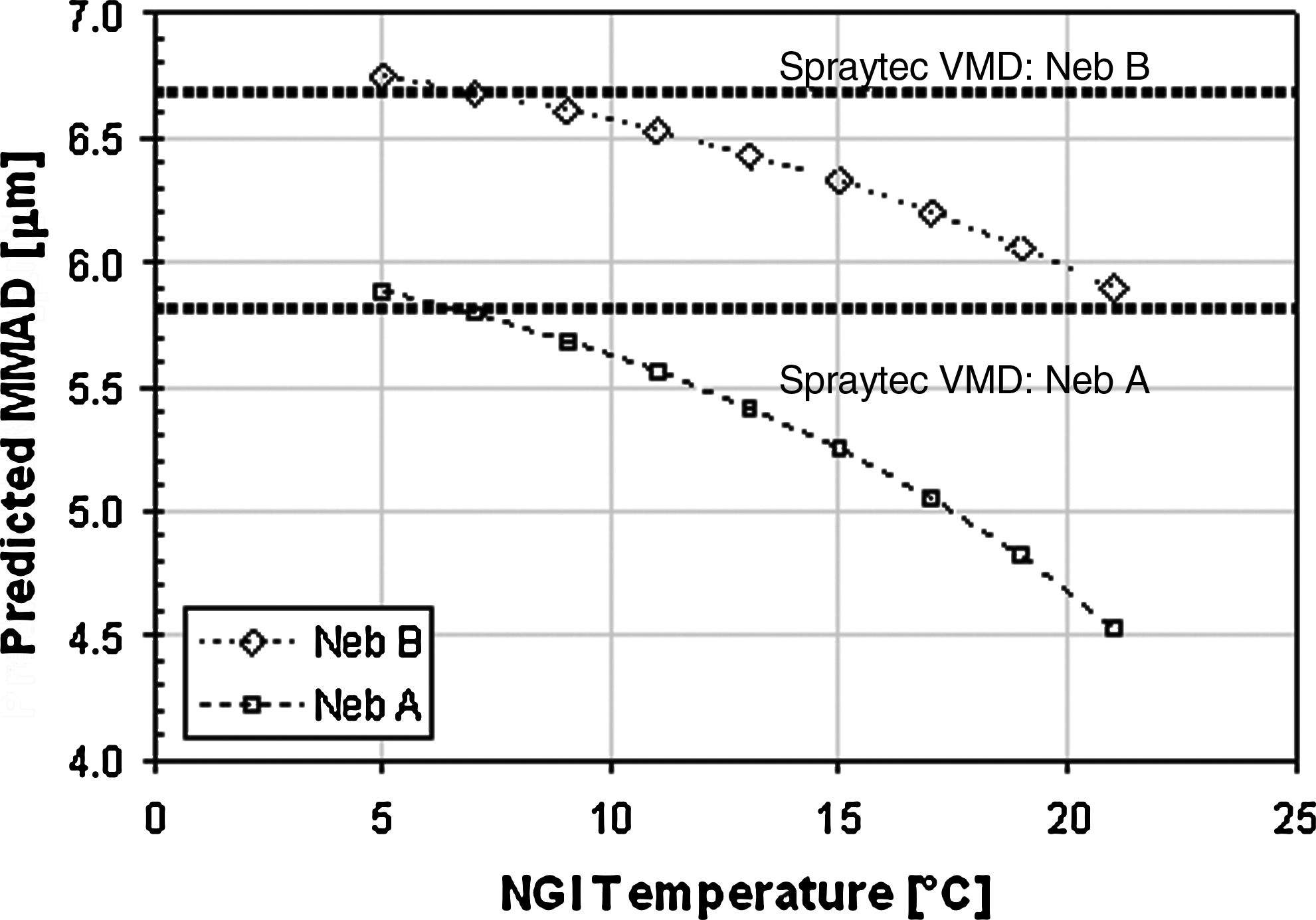
Predicted MMAD as a function of temperature to which entrained air is cooled.
For the specific case of the PDDS vibrating mesh nebulizer, the data and discussion above suggests that the cooled impactor approach is reasonably effective in controlling droplet evaporation during measurement. The droplet evaporation model used here indicates that in addition to environmental conditions, droplet evaporation is also influenced by nebulizer characteristics such as drug output rate, and factors such as impactor flow rate. These additional factors need to be taken into account before deciding on the suitability of any approach taken to mitigate the problem of droplet evaporation during measurement of nebulized aerosols. For the case of nebulized aerosols, the present study also reinforces previous work(9,10) in presenting laser diffraction spectrometry as an alternative droplet size measurement approach that is reliable, simple to implement, and less susceptible to measurement artifacts such as droplet evaporation.
Conclusion
A simple droplet evaporation model has been applied to NGI cascade impactor measurement of droplet size distributions produced by a proprietary vibrating mesh nebulizer. The model has been used to estimate the sensitivity of the measured MMAD to factors such as the temperature Ta and humidity Ha of entrained ambient air, the nebulizer output rate Ql, the entrained air flow rate Qa, and the initial droplet size di. The modeling and experimental results indicate that the influence of these variables on measurements may be reduced significantly by refrigerating the impactor down to 5°C before measurement. The modeling results also suggest that for the case of dilute drug solutions generated by a vibrating mesh nebulizer, it is feasible to achieve good correlation between laser diffraction and cascade impactor data by minimizing droplet evaporation in this manner. For the case of nebulized solutions, this study provides further support for choosing the laser diffraction as a more desirable method in comparison to cascade impaction.
Footnotes
Acknowledgments
The authors are indebted to Truong Dang for his assistance in generating experimental data used in this article.
Author Disclosure Statement
No conflicts of interest exist.