
Abstract
Abstract
Background:
Noninvasive monitoring of airway inflammation is important for diagnosis and treatment intervention of lung disease. Mediators of interest are often nonvolatile molecules that are exhaled as aerosols and captured by breath condensation. Because analysis of exhaled breath condensate has been troublesome in the past, partly due to poor standardization and unknown dilution, we investigated in detail the influence of respiratory variables on exhaled particle number and size distribution during tidal breathing in healthy volunteers.
Methods:
Particle number was detected by a condensation nuclei counter, and size distribution was determined by a laser spectrometer online with high time resolution while subjects underwent a defined protocol of normal and deep tidal breathing. Intra- and intersubject variability of particle emission was analyzed and physical properties of exhaled aerosols were correlated to pulmonary function variables obtained by bodyplethysmography.
Results:
The particle size distribution was in the submicron range and stable during tidal breathing. Increasing tidal volumes dominantly influenced particle number emission while flow rates had only little effect. Reproducibility within subjects was high, but there was a large variation of particle emission between subjects. The ratio of functional residual capacity to total lung capacity was found to correlate with exhaled particle numbers. This indicates that particle generation is caused by reopening of terminal airways and is dependent on functional residual capacity.
Conclusion:
We conclude that online determination of exhaled aerosols from the human lungs is a prerequisite to standardize the assessment of nonvolatile mediators by normalization to the aerosol emission rate.
Introduction
Several studies are found in the literature dealing with the characterization of number and size of exhaled particles.(7,8) Recently, Morawska et al.(9) provide a broad overview of possible particle sources resulting from normal breathing, speaking, and coughing. A common finding in the different studies was that the exhaled particle number varied for the individual subject depending on his or her activity and showed a high intersubject variability.
Possible mechanisms of aerosol generation are, on the one hand, entrainment of particles from airway lining fluid at high shear velocities, and on the other hand, breakup of fluid films resulting from reopening of closed terminal airway capillaries. For normal/quiet tidal breathing, as performed for breath condensate sampling, the first mechanism can be excluded due to absence of sufficient shear forces. Recent results of Johnson and Morawska(10) and earlier investigations of Gebhart et al.(11) confirm these theoretical considerations, clearly identifying the reopening of collapsed terminal airways as the mechanism of aerosol generation. It has been suggested that the surface tension between the lung lining fluid and the air in the lumen is the primary mechanical effect responsible for airway closure.(12,13) At end expiration, surface tension driven instabilities can lead to the formation of liquid bridges or to structural collapse of small peripheral airways. The increasing transpulmonary pressure during the next inspiration results in the reopening of closed terminal airways associated with audible crackles(14–16) and the generation of small droplets.
Particle number as well as particle size distribution in exhaled air is the result of the particle generation rate on the one hand and the rate of redeposition in the lung structures during the exhalation process on the other hand. Considerations taking into account the dimensions of the peripheral airway structures (<500 μm) and typical residence times of several seconds following particle generation clearly demonstrate that most particles in the supermicron range will be redeposited due to gravitational settling. Consistently, exhaled particles from the human lung have been measured and reported in the submicron range with a mean diameter between 0.3–0.8 μm.(7,8,10)
Although the physical mechanism of aerosol generation in the human lung seems to be basically understood, systematic investigations of the physical properties of the exhaled aerosol and their dependency on the individual lung status and pulmonary function variables are missing. Importantly, knowledge of the total particulate number emission rates and particle size distribution might allow for the normalization of biomarker concentrations measured in the breath condensate. This is essential for the correct interpretation of results from biochemical analysis of the breath condensate, and might thus help to reduce variability.(17)
Therefore, we investigated in detail the influence of respiratory variables on the exhaled particle number and size distribution during tidal breathing in healthy volunteers. The aim was to identify the respiratory parameters that determine the particle emission rate. Moreover, the intra- and intersubject variability of particle emission was analyzed and physical properties of exhaled aerosols were correlated to pulmonary function variables obtained by bodyplethysmography. In addition, the data were analyzed to provide experimental evidence for the mechanism of droplet generation. Finally, this analysis was complemented by calculating the effect of redeposition using the semiempirical ICRP-model (particle deposition model of human respiratory tract developed by the International Commission on Radiological Protection).(18)
Materials and Methods
Particle measurement
The particle concentration and the size distribution of the exhaled breath as well as the respiratory flow rate were measured using an experimental setup shown in Figure 1. The setup was designed to allow for the analysis of individual breath events. This required the online measurement of the particle number and the size distribution with high time resolution (1-sec interval). Moreover, precautions were taken to avoid modifications of the exhaled aerosol properties caused, for example, by large dead volumes or by water vapor condensation. The subject breathes via a mouthpiece connected to a tube (Tygon S-50-HL, ID 19 mm, LIQUID-scan, Überlingen, Germany) into a thermostated box containing the necessary tubing and the measuring instruments. Particle free air is inhaled through a HEPA-filter to avoid interference with background aerosol. To avoid unintended inhalation of ambient air through the nose the volunteer wears a nose clip. The exhaled breath is lead into a second branch (length 0.5 m, i.d. 19 mm) strictly separated from the inhalation branch (length of 0.65 m, i.d. 19 mm) by directional valves (model 1954, Intersurgical, Sankt Augustin, Germany). Each branch contains a laminar flow element (Fleisch laminar flow element Type 1, Dr. Fenyves und Gut, Hechingen, Germany). The inspiration and expiration flow rates are determined from the respective flow signals taking into account the stationary flows of the measuring instruments. The breathing curves (flow rates) are displayed in real time on a computer screen to assist the volunteer to perform the breathing manoeuvres.
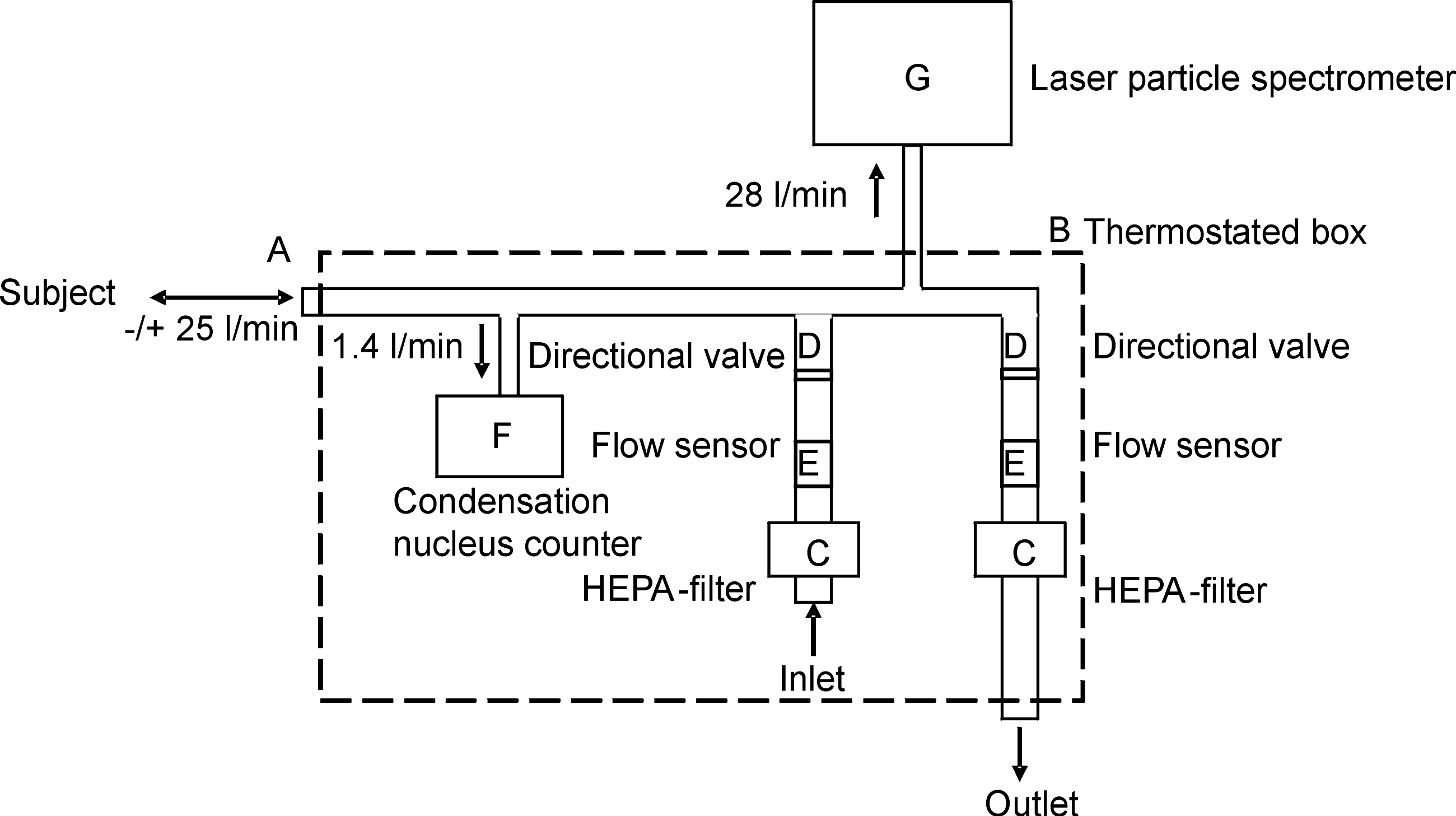
Experimental setup for time-resolved measurement of the exhaled particle concentration, particle size distribution, and airflow. The subject breathes via a mouthpiece connected to a tube (
The particle concentration is measured by a condensation nuclei counter (CNC - TSI 3760, TSI GmbH, Aachen, Germany), by taking a side sample stream of 1.4 L/min from the exhaled breath. The size distribution is analyzed by leading the entire breath flow through a laser spectrometer with a sample stream of 28 L/min (PMT Lasair II-110, Heimsheim, Germany). This instrument sizes the particles in six channels in the range between 0.1 and 5 μm: 0.1–0.2, 0.2–0.3, 0.3–0.5, 0.5–1.0, 1.0–5.0, and >5.0 μm. A high-flow CNC and a high-flow clean room particle spectrometer are used to allow for sufficient time resolution in the measurements because the concentration of the particles generated in the lung is expected to be low. For synchronization of the flow signals and the concentration signals we chose a CNC delay time of 2 sec (0.5 sec related to the tubing and 1.5 sec response time of the CNC). To prevent water vapor condensation from the saturated exhaled air in the measuring system the flow sensors and the condensation nuclei counter are placed inside a box thermostated to 37°C and the side sample stream of the particle spectrometer is sufficiently diluted to prevent condensational growth of the particles due to the pressure drop in the focussing nozzle of the LASAIR.
Before the endogenously generated particles can be characterized in the exhaled breath a breathing period of about 2 min is necessary to remove all the particles from the lung that originated from the inhaled ambient air.
Study subjects
Human investigations were approved by the Ethics Committee of the Hannover Medical School. All subjects gave written informed consent after being fully informed about the procedures and the study. Twenty-one healthy volunteers (12 male, 9 female) aged between 21 and 63 years with normal pulmonary function and no history of pulmonary disease participated in the study (Table 1). Participants were included if they were nonsmokers, or smokers with a history of less than 10 pack years with no smoking in the past 12 months. They had no respiratory tract infection in the past 4 weeks, and did not take any regular medication.
Demographics and pulmonary function variables of study subjects. Forced expiratory volume in 1 sec (FEV1) and forced vital capacity (FVC) are given as % predicted normal (%pred). Total vital capacity (TLC), residual volume (RV), and functional residual capacity (FRC) are given in liters.
Study design
All subjects underwent spirometry according to ERS/ATS standards(19) and bodyplethysmography to determine pulmonary function variables (Table 1).
In a pilot study with five volunteers, respiratory variables were identified that fundamentally influenced the emitted particle number and size distribution. Therefore, subjects performed a series of breathing manoeuvres with variation of inspiratory flow rate, expiratory flow rate, and tidal volume to assess the effect on exhaled particle number and size distribution. In this pilot study, only one respiratory variable at a time was varied during several consecutive breathing cycles while the others were kept constant. The results of this pilot study were used to develop the protocol for the breath aerosol analysis in the main study.
In the main study, 16 volunteers (aged 20–63 years) underwent a standard protocol with predefined breathing manoeuvres while the properties of the exhaled aerosol were recorded. For each subject the tidal volume was varied from about 20 to 80% of the individual vital capacity. Tidal volumes less than 0.7 liter were disregarded because the exhalation periods were too short compared to the response times of the measuring devices.
To determine the reproducibility of the results (intrasubject variability) each subject had to repeat the breathing manoeuvres after 2 h the same day, and once again during a second visit within 2 months. The subjects wore a nose clip and were seated upright for all experimental measurements.
Modeling
Modeling of particle redeposition was carried out using the ICRP model. This model calculates regional deposition efficiencies in different lung regions, that is, extrathoracic, upper bronchial, lower bronchial, and the alveolar region as a function of respiratory flow rate and various physiological parameters. Each lung region is represented by a filter with a characteristic volume and deposition efficiencies specific for inhalation and exhalation. Because the subjects inhaled particle-free air and particle generation is assumed to take place in the peripheral lung areas, the lung filter deposition efficiencies were set to zero for the calculations during the inhalation path. For the exhalation, the regional particle deposition efficiency was calculated using the filter efficiencies as specified in the ICRP model for exhalation. This allowed for the calculation of the total penetration probability of particles generated in the lung periphery on their way up to the mouth.
Results
Pulmonary function determinants for breath particle concentration
Pilot study
The results of a simultaneous measurement of exhaled particle concentration and airflows for three breathing patterns are shown in Figure 2. The upper curve shows the respiratory flow rate recorded during the breathing manoeuvre: positive (negative) values represent inhalation (exhalation). A delay time of 2 sec for the TSI number counter has been taken into account to synchronize the concentration displayed in the lower curve with the breath flow rate. The high time resolution of the measurements allowed for the analysis of individual breaths. This enabled to measure not only the integral number of particles per breath but also to determine the temporal emission pattern of each individual manoeuvre to a certain extent. For example, a steady increase in the particle concentration can be observed towards the end of expiration (Fig. 2).
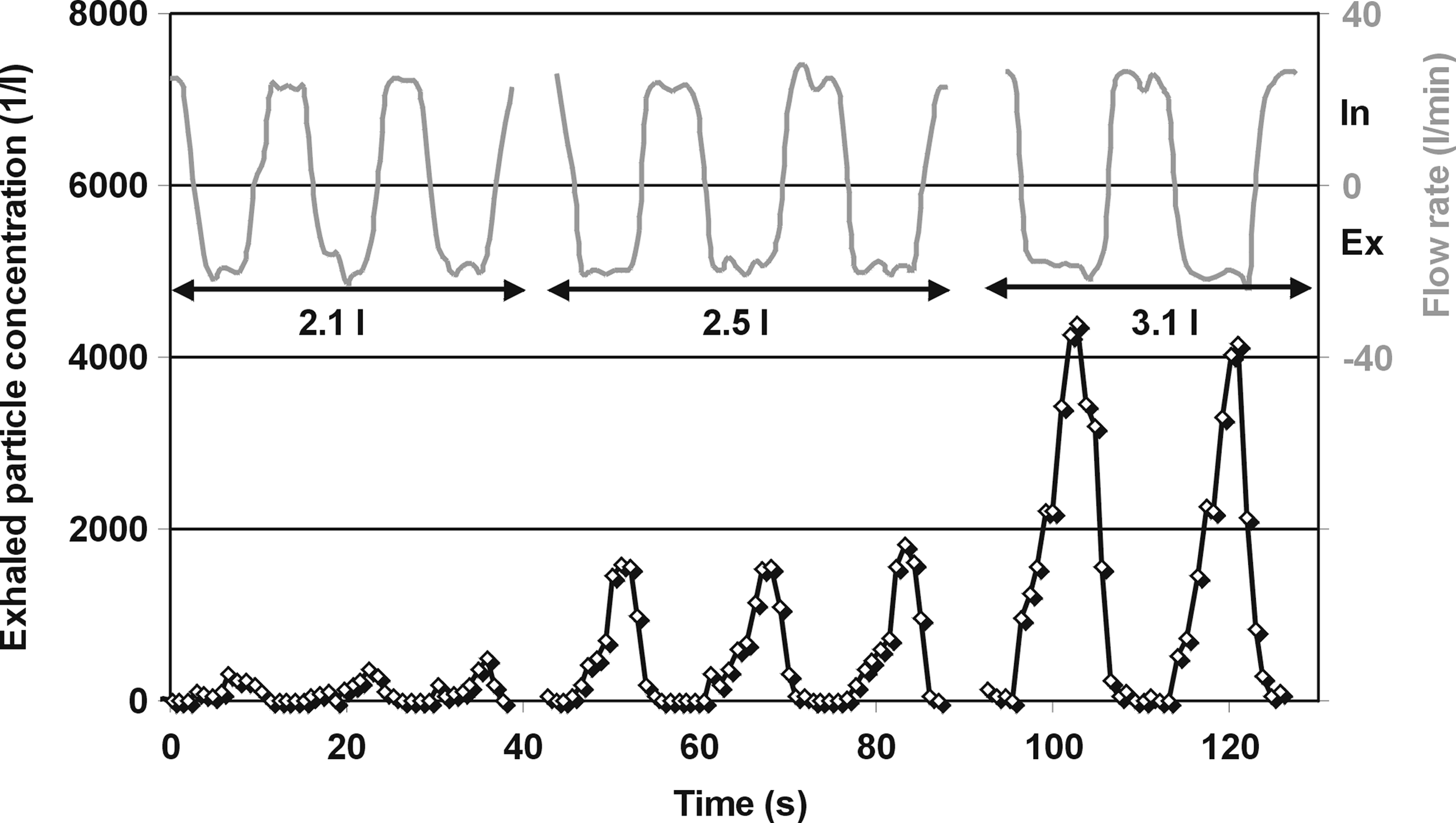
Exhaled particle concentration (lower curve) and flow rates (upper curve) for several consecutive breathing cycles in a healthy volunteer at three different tidal volumes of 2.1 L (left), 2.5 L (middle), and 3.1 L (right).
Relevant respiratory variables determining the emission rate of the exhaled particles were identified. When a deep expiration manoeuvre was performed after a period of normal tidal breathing a strong increase in particle concentration with the following exhalation step was observed. In contrast, a deep inhalation did not change the exhaled particle concentration significantly with the next exhalation.
For all subjects, a strong rise in exhaled particle number concentration was measured with increasing tidal volumes performed at moderate airflow rates between 25 and 30 L/min. The difference in particle emission observed at the smallest and largest tidal volume could be more than two orders of magnitude. In contrast, the influence of inspiratory flow rate and expiratory flow rate on exhaled particle emission was comparatively small: variation of expiratory flow rate between 10 and 50 L/min resulted in an increase in exhaled droplet number by a factor of 3. When inspiratory flow rate was modified by a factor of 5 (range: 20–100 L/min) there was only a trend (not significant) of increasing number emission.
For all volunteers, the particle size was mainly in the submicron range with a count median diameter of 0.3 μm. This distribution was virtually independent from any variation of the different respiratory variables.
Main study
To compare the influence of ventilation between subjects, a ventilation ratio was used and defined as the ratio of tidal volume VT to vital capacity VC. For all subjects, particle number per breath strongly increased with increasing ventilation ratio. For each subject, exhaled particle number per breath (N) could be well approximated by the following exponential function:
Figure 3 shows the particle emission per breath in relation to increasing ventilation ratio for three volunteers. Exhaled particles per breath at a defined ventilation ratio were obtained by averaging three to eight consecutive breathing cycles with constant respiratory parameters. Importantly, the number of emitted particles rises by more than a factor of 100 when increasing the tidal volume from its smallest to its largest value. The average exhaled particle concentration varied between five particles per liter for tidal breathing up to about 5000 droplets per liter for deep breathing with large tidal volumes. This exponential function was present in each subject and it was highly reproducible: there was no significant difference in this characteristic particle emission pattern when the test was repeated either on the same day or on a separate day (Fig. 3).
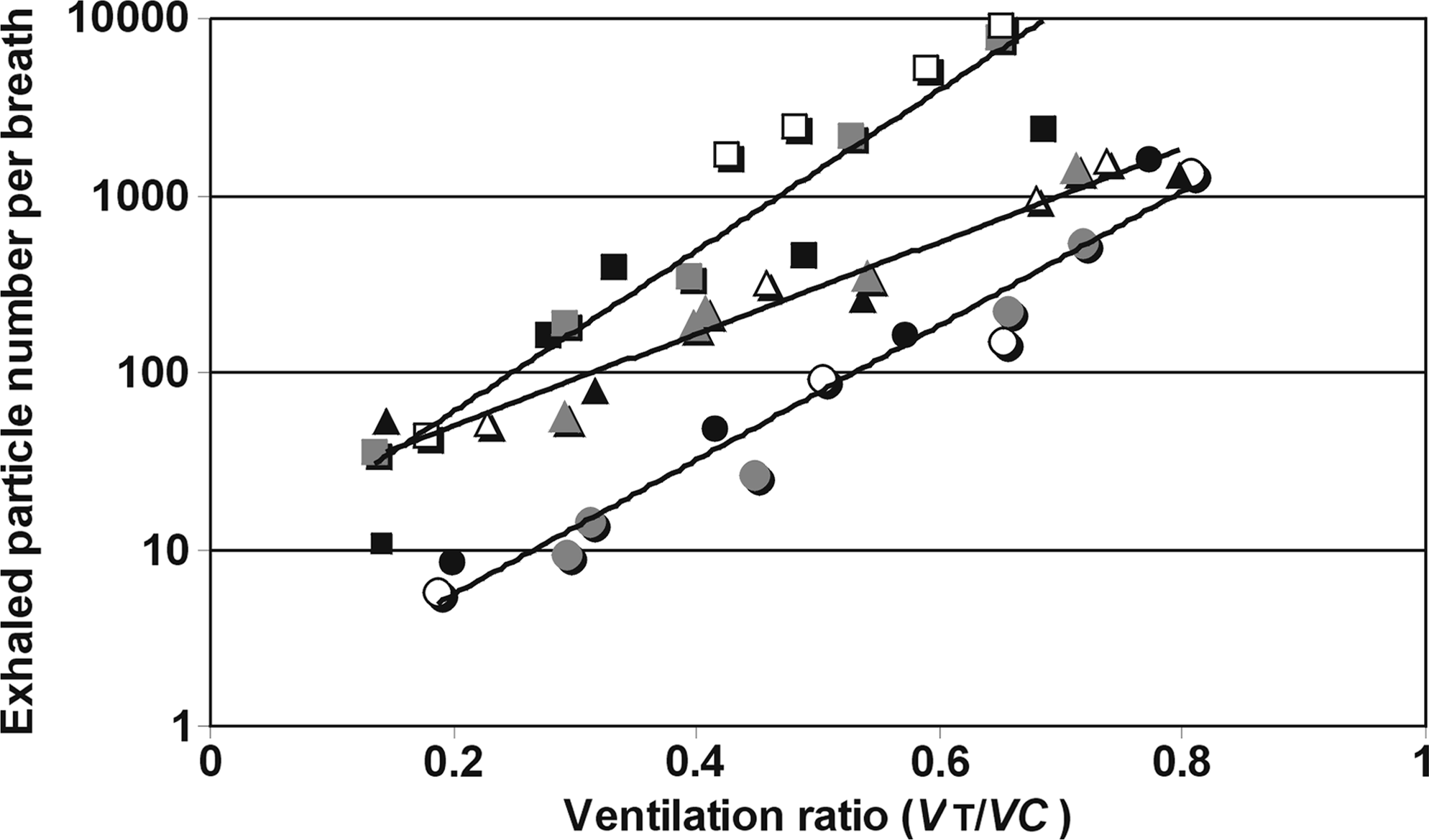
Exhaled particle number per breath as a function of the ventilation ratio tidal volume (VT)/vital capacity (VC) for three volunteers. Different symbols (circle, square, triangle) are used per subject and the different shadings (white, gray, black) indicate the three repeated measurements.
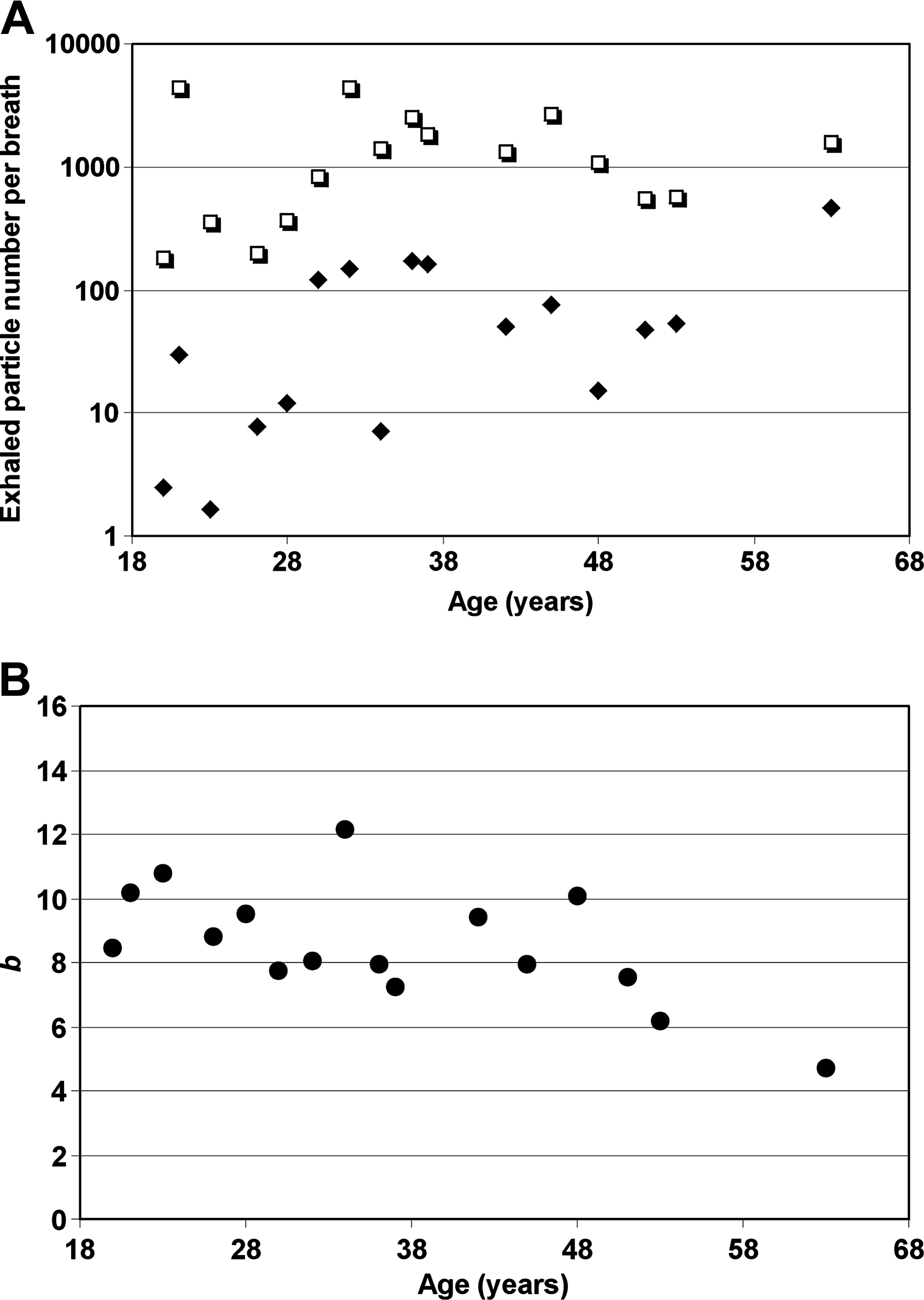
Although the exponent, b, varied between 5 and 12 (minimum to maximum) among subjects, there was a much larger range of values of the prefactor, A, covering almost two orders of magnitude. In Figure 4A, the emission rates for all subjects according to age are displayed using an emission index, defined as the number of particles emitted per breath at a ventilation ratio VT/VC of 0.6 (open symbols). The large intersubject variability in the number of exhaled particles is evident, resulting in a coefficient of variation of 87% for the applied emission index. There was no correlation of the emission index with age (r = 0.250, p = 0.350) at VT/VC = 0.6. At a ventilation ratio of 0.2, which is close to normal tidal breathing, a trend toward higher particle emission rates with age was observed (r = 0.497, p = 0.0501). Interestingly, when exhaled particles per breath were measured at normal tidal breathing without standardization and plotted against age (Fig. 4B, closed symbols), we found a significant correlation between particle emission and age (r = 0.568, p = 0.022). However, the variation was considerable (e.g., in the two youngest subjects >10-fold).
(
In Figure 4B, the slope b of the exponential function, describing the relationship between the particle emission and the ventilation ratio, is plotted against the age for all subjects. The slope significantly decreased with increasing subject age (r = −0.58, p = 0.02). Only a small intersubject variability was observed for b, with values mainly in the range between 8 and 10 (coefficient of variation of 21%).
For each volunteer one exponential curve was fitted to all particle concentration data obtained from the measurements of the three sessions. A high interday and intraday reproducibility was found for the exhaled droplet number with an average correlation coefficient of 0.92.
Particle emission at a ventilation ratio VT/VC of 0.6 was also correlated to the individual pulmonary function variables obtained by bodyplethysmography such as total lung capacity, functional residual capacity, and residual volume. Using this emission index, a decrease in the number of particles emitted per breath was observed with the ratio of functional residual capacity to total lung capacity (FRC/TLC; Fig. 5) with a correlation coefficient r = −0.51 (p = 0.04). The relation of decreasing particle emission rates with increasing FRC/TLC was only found for ventilation ratios above 0.45. FRC, which was determined by bodyplethysmography for each subject, is defined as the lung volume at end expiration during normal tidal breathing. The vertical error bars on the data points in Figure 5 indicate the standard deviation of the data taken at the three different sessions, clearly showing that the intrasubject variability was much smaller than the intersubject variability. When ventilation ratio was related to exhaled particle concentration instead of exhaled particle number per breath, similar trends and relationships were observed.
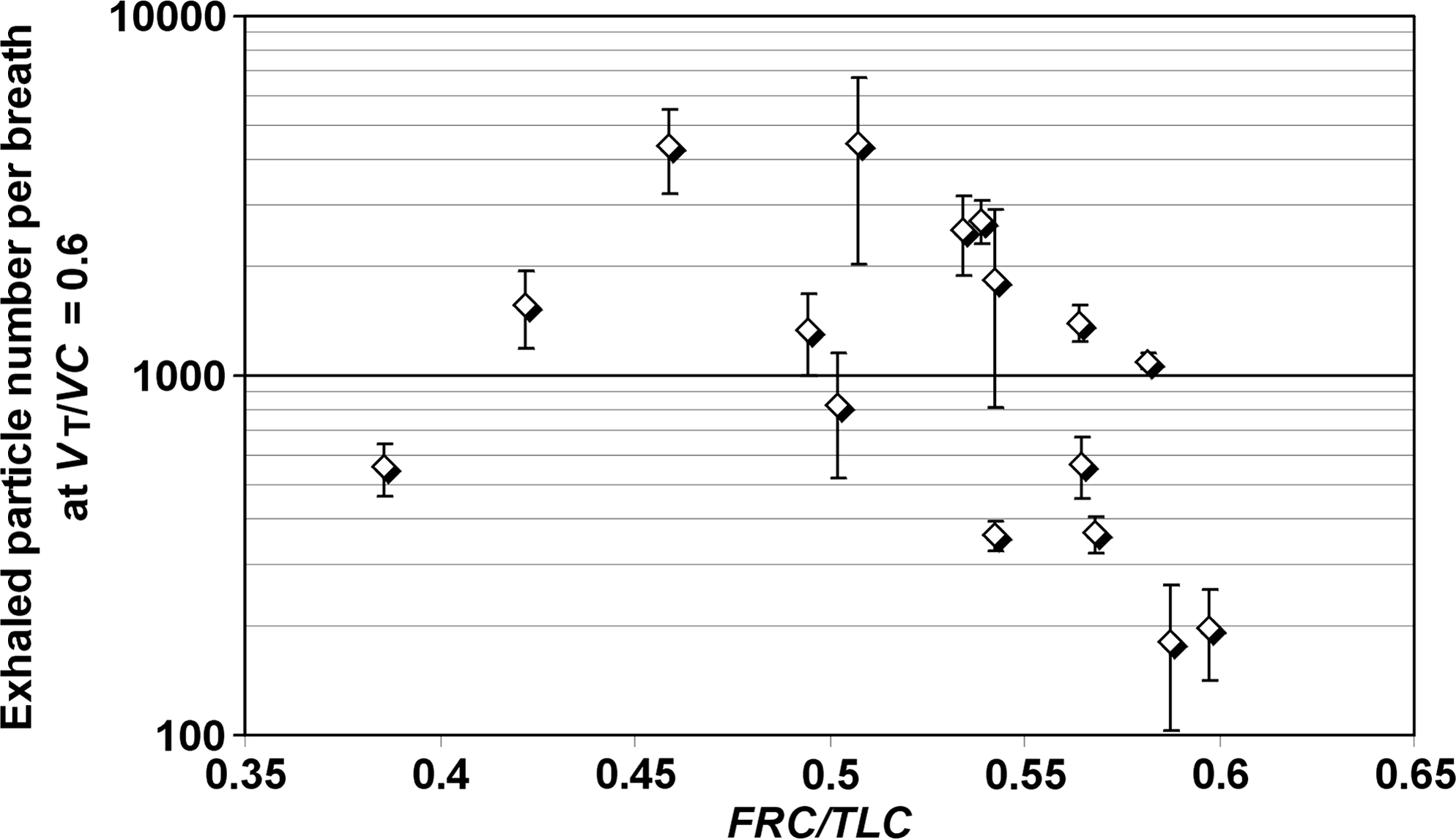
Particle emission index at a ratio of tidal volume (VT)/vital capacity (VC) = 0.6 as a function of the corresponding ratio of functional residual capacity (FRC)/total lung capacity (TLC). Each symbol displays the mean of three measurements ± standard deviation. The Spearman correlation coefficient and p value is given (r = −0.512, p = 0.04).
Figure 6 shows a typical number size density distribution as measured with the optical particle spectrometer. The curve is the best fit to a lognormal function resulting in a count median diameter of 0.3 μm, with a geometric standard deviation of 1.64. For all subjects, the number size distribution averaged per breathing cycle was predominantly in the submicron range, with a count median diameter of 0.28 μm. Only a small droplet fraction of about 2% was in the supermicron range, with no particles larger than 5 μm. For normal tidal breathing, as performed for breath condensate sampling, the count median diameter was 278 nm, with only a small intersubject variability (coefficient of variation of 9%). This size distribution was only slightly dependent of the tidal volume. With increasing tidal volume and therefore increasing residual times in the lungs, a slight shift toward smaller particle sizes was observed. Generally, the size distribution was averaged over the entire exhalation process. However, a time resolved scanning of a single exhalation process showed a shift of the normalized size distribution toward smaller particles with increasing exhalation time (Fig. 7), which is evidence for losses by gravitational settling.
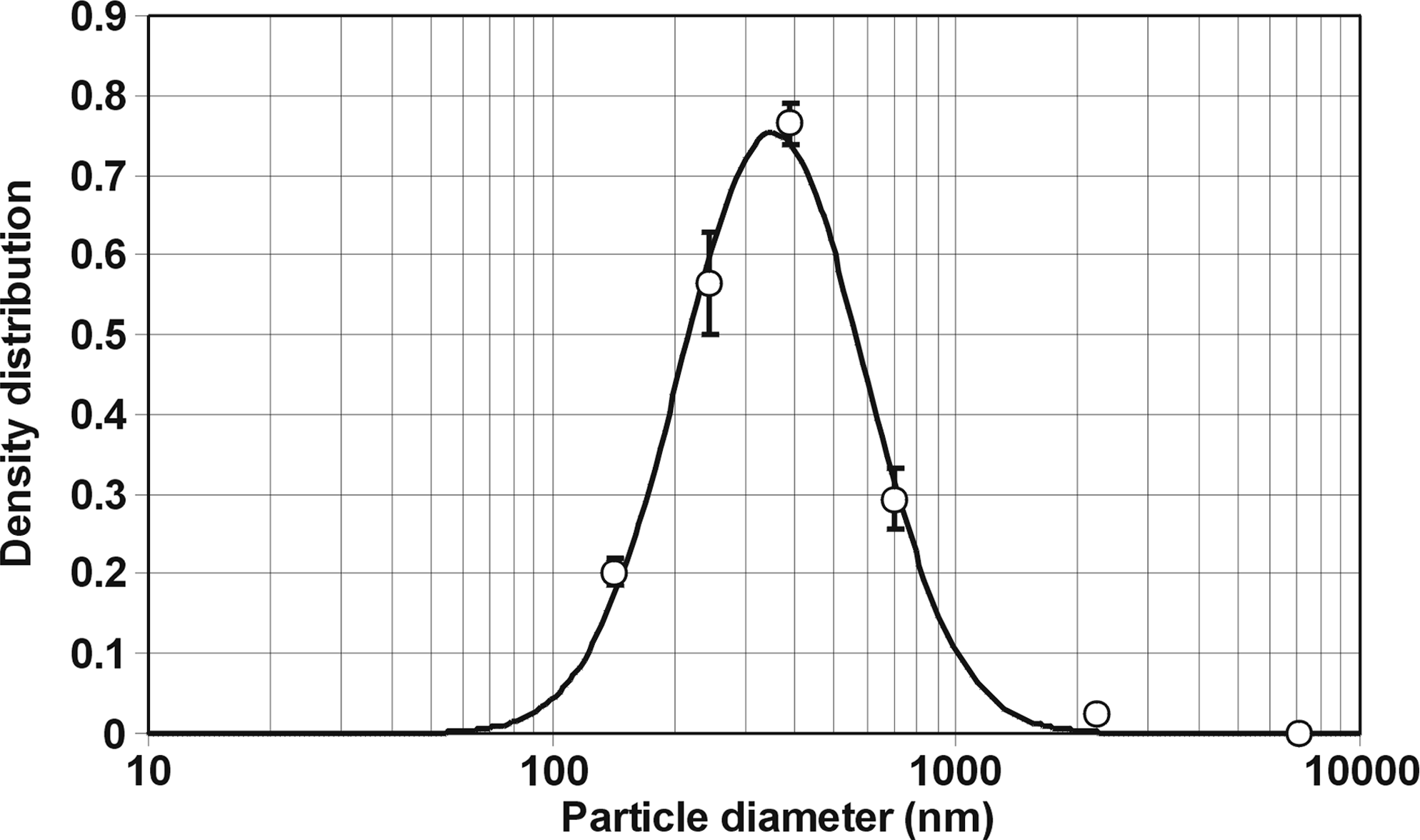
Number size distribution of exhaled particles from all subjects at a ratio of tidal volume (VT)/vital capacity (VC) = 0.5. Vertical error bars indicate the standard deviation for the density values at the different particle diameters.

Number size distribution of exhaled particles from a healthy subject breathing at a tidal volume of 2.5 L measured during an entire exhalation process at an expiration time of 2, 6, and 10 sec.
Modeling
Figure 8 shows penetration curves from model calculations using the ICRP model. The calculations were performed for the standard male (functional residual capacity of 3.30 L) breathing with a tidal volume of 1 L, 2.5 L, and 4 liter at flow rates of 0.4 L/sec.
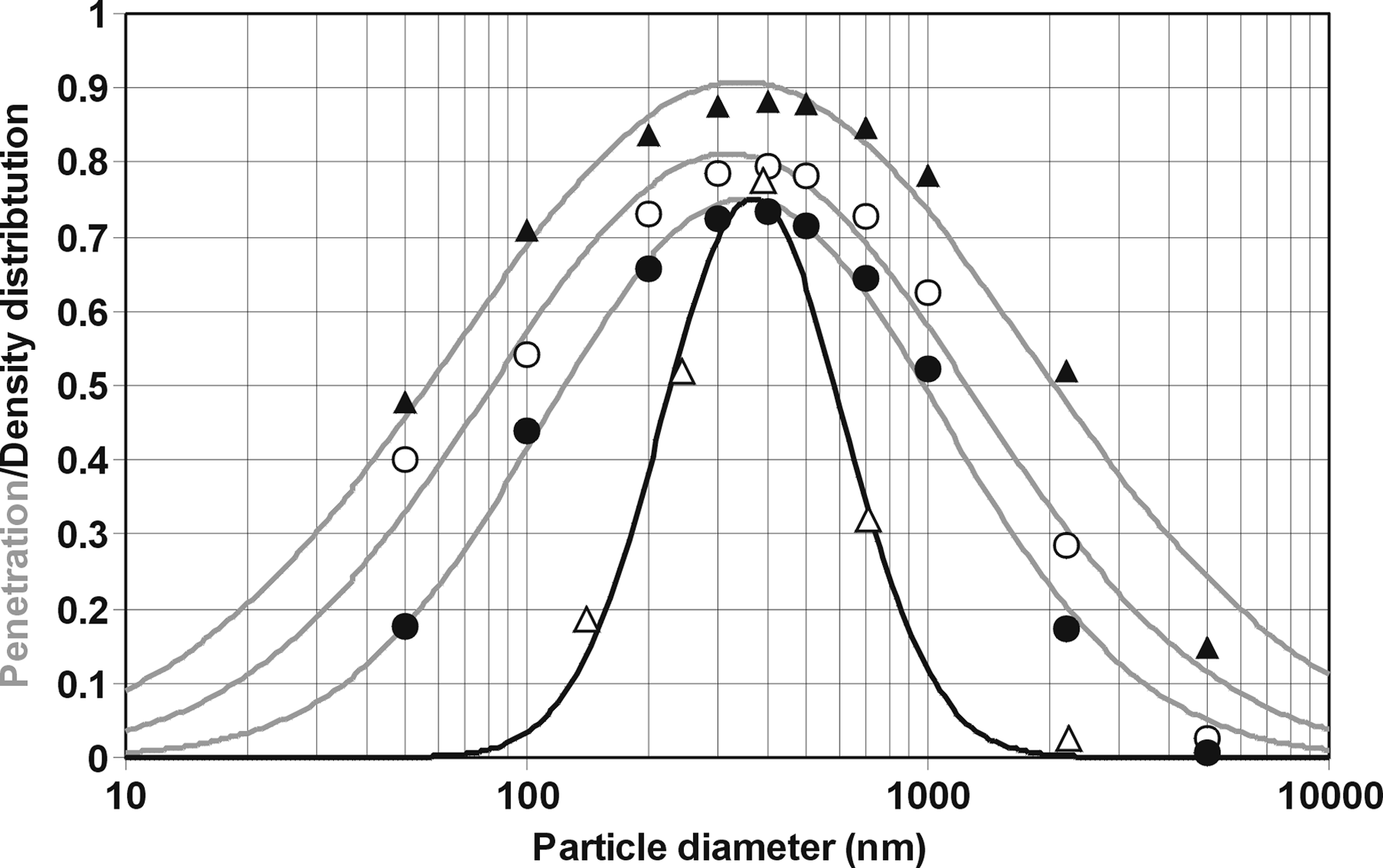
Penetration curves calculated from ICRP model at tidal volumes of 1 L (closed triangles), 2.5 L (open circles), and 4 L (closed circles) compared to the experimentally determined number size distribution for a volunteer at a tidal volume of 2.5 L (open triangles).
In all cases the fraction of particles not deposited in the respiratory tract reaches its maximum at 0.4 μm, which matches well with the experimentally determined droplet size distribution. Because large particles are always efficiently removed, only a small fraction of potentially generated supermicron droplets can be exhaled during normal tidal breathing. Taking into account the small airway dimensions in the lung periphery together with typical residence times of several seconds, it is obvious that redeposition of these particles occurs mainly due to gravitational settling in the deep lung. Particles smaller than about 0.1 μm are deposited in the alveolar region due to diffusion processes, and according to this, were not detected in exhaled breath from subjects in the clinical study.
Discussion
This study measured online and with high time resolution the number and the complete size distribution of exhaled particles in every single human breath. This allowed to investigate essential determinants of particle emission from the human lung in relation to different respiratory variables. The tidal volume was the most important variable that determined the particle emission of an individual. Importantly, there was a large variation between subjects in the exhaled particle number per breath covering about two orders of magnitude. For all subjects the particle size was predominantly in the submicron range, with a count median diameter of 0.3 μm. These results were highly reproducible, indicating that exhaled aerosols can serve as a fingerprint, possibly representing the individual lung status.
We found that variation of the inspiratory flow rate only had a small effect on exhaled particle numbers while increase in expiratory flow rate caused a modest increase in particle emission by a factor of 3, which was far below the influence that changes in tidal volume provoked (>100-fold). The increased particle emission with higher expiratory flows can well be explained with reduced losses by gravitational settling. Therefore, we conclude that particle generation does not occur due to shear forces, but rather due to reopening of collapsed or occluded terminal airways. This is in agreement with recent published results(10) that suggested reopening of terminal airways as the main source for exhaled particles. In detail, with decreasing transpulmonary pressure at the end of each expiration, surface tension-driven instabilities result in the formation of liquid bridges occluding the lumen or causing structural airway collapse. The reopening of these structures during the next inspiration process due to increasing transpulmonary pressure linked with a sudden breakup of the surfactant film generates droplets in the deep lung. These particles are emitted with the next exhalation. Our time-resolved analysis of the exhaled particle concentration during every individual breath clearly confirms this generation mechanism because the particle concentration is steadily increasing toward end expiration, which depicts the deep lung areas. Interestingly, an increase in tidal volume by shifting toward expiration results in higher particle concentrations than the same increase in tidal volume by shifting the inspiration. This also suggests that breathing below the functional residual capacity is related to airway closure with increased particle emission. Finally, the exponential behavior of the particle emission flux as a function of tidal volume as observed in all subjects clearly confirms the peripheral lung areas as the dominant particle source.
Particle generation from the human lung is a very reproducible phenomenon. This is of utmost importance when planning to use particle characteristics for a normalization procedure in exhaled breath condensate assessments. Clearly, repeat analysis of particle emission either the same day or several days apart gave good repeatability of the particle emission (Fig. 3) allowing for the calculation of an individual particle generation factor at a given tidal volume (Fig. 4A). From this high reproducibility it can be concluded that the individual particle number is very characteristic for the actual individual lung status. As depicted in Figure 4A, the high intersubject variation in particle emission rates addresses the need to measure the physical aerosol properties simultaneously during breath condensate sampling to correctly interpret biochemical results in exhaled breath condensate. Because the size of emitted particles does not vary substantially between subjects it becomes clear that the amount of sampled lung lining fluid is closely related to the number of exhaled particles or to the particle emission index, respectively. This highlights that the ratio of the mass of condensed water vapor and the mass of the collected lining fluid, often called the dilution factor, can vary considerably by two orders of magnitude between subjects.
The reason for the large intersubject variation of particle emission by two orders of magnitude is unknown and difficult to explain. Therefore, we compared the particle emission to individual lung parameters. We found higher exhaled particle number in those subjects who had a lower ratio of functional residual capacity to total lung capacity (Fig. 5). FRC represents a measure of the individual expiration level because it reflects the lung volume at the end of a normal expiration. Assuming that breathing at residual volume has the greatest probability of airways to collapse, it is interesting to find a correlation of FRC/TLC with particle emission. Admittedly, FRC was only measured once during bodyplethysmography and not prior to every particle measurement in each subject, but it has been shown that FRC is fairly reproducible.(20) Therefore, we conclude that breathing at a level that is closer to the residual volume is correlated to higher particle generation because airways are more likely to collapse. This might at least partly explain the huge intersubject variation seen for the particle emission.
It has been reported that there is an age-related increase in closing volume, presumably caused by increased tendency to collapse of the peripheral airways due to loss of elastic recoil of the tissue.(21) From that, one would expect higher particle numbers with age. As depicted in Figure 4A, exhaled particle numbers per breath were positively correlated with age when subjects were breathing normally at tidal volumes around 1 liter. This finding is in agreement with recent results of Johnson and Morawska.(10) At higher ventilation ratios this correlation is lost. The huge variation of particle emission between subjects of similar age questions the biological significance of this correlation anyway and highlights the importance to individually determine particle emission characteristics.
The particle number size distribution experimentally found has a maximum at 0.4 μm, which is in good agreement with theoretical curves obtained from the ICRP model. These curves describe the penetration of particles generated in the distal airways on their way up to the mouth where they are measured. In line with our findings, exhaled particles from the human lung have been measured and reported in the submicron range with a diameter between 0.3 and 0.8 μm.(7,8,10) Taking into account typical residence times of several seconds in the small airways, particles greater than 0.5 μm will be deposited in this region, so that potential inertial deposition processes in the upper lung areas are not relevant. Particles smaller than 0.1 μm will be deposited due to diffusion processes. The effect of particle removal is clearly visible in the shift of the droplet size distribution during an individual exhalation, caused by increasing gravitational deposition of the larger particles in the size range above 0.5 μm. Consistently, a time-resolved scanning of a single exhalation shows a shift of the normalized size distribution toward smaller particles with increasing exhalation time (Fig. 7), clearly demonstrating the effect of losses due to gravitational settling. It must be stated, however, that this analysis does not allow to draw firm conclusions on the size of the droplets at the origin of their generation. This subject is addressed in a separate article.(22)
There is, of course, an error margin related to the measurement technique. Because the exhalation flow rate was always kept around 25 L/min, the exhaled air was partially diluted resulting in a relative humidity in the range between 90 and 100% at the sensing zone of the size spectrometer. This could lead to a shrinking of droplets generated in the lung at conditions of 100% relative humidity. However, because the droplets generated are basically isotonic, that is, they contain 0.9% sodium chloride, they do not evaporate completely due to the stabilizing effect of the electrolytes. Therefore, the range of a possible size reduction could be in the range of a factor of about 2 for a relative humidity larger than 90%. A second source of uncertainty is related to sizing errors occurring with optical sizing instruments. Their sizing characteristic is sensitive to the optical properties of the aerosol, especially in the size range close to the instruments' wave length (810 nm for Lasair II-110). Because composition and structure of the ambient aerosol are usually different from the characteristics of the standard polystyrene latex particles used for calibration, there is potential for underestimating the particle diameter up to a factor of nearly 2. Taking into account these considerations the diameter of the exhaled particles could be underestimated up to a factor of more than 3. Therefore, this analysis does not allow for the calculation of reliable exhaled aerosol mass emission rates and dilution factors for exhaled breath condensate assessments. However, simultaneous measurement of the physical aerosol properties during breath condensate sampling enables a normalization procedure of the concentrations of nonvolatile biomarkers measured in breath condensate.
Taken together, this study contributes significantly toward a better understanding of the process of aerosol generation from the human lung and establishes a sound basis for further development of exhaled breath analysis as a potential tool for detection and monitoring of lung disease. Because a number of lung diseases have been described to be caused by or associated with airway closure(12) it is tempting to suggest that these alterations could result in a change of the exhaled particle number and size distribution. Thus, simple breath-particle monitoring (primarily number flux) might serve as a convenient noninvasive method for detection and especially monitoring of lung disease. Furthermore, breath-particle monitoring (number flux and size distribution) enables a normalization procedure for improved validity of the biochemical analysis of exhaled breath condensate.
Footnotes
Acknowledgments
This work was supported by a grant of the Deutsche Forschungsgemeinschaft (Ho2158/1-1). The authors are grateful to the subjects for their participation in the study.
Author Disclosure Statement
The authors declare that they have jointly filed a patent application on the use of particle monitoring for detection and monitoring of lung disease.