
Abstract
Abstract
Background:
Jet nebulizers coupled to spacers are frequently used to promote drug lung deposition, but their clinical efficacy has not been established. Few in vivo studies have been performed with mesh nebulizers, commonly used to nebulize antibiotics. Our study compared inhaled mass and urinary drug concentration of amikacin by using three different nebulizer delivery configuration systems: a standard unvented jet nebulizer (Sidestream®) used alone or coupled to a 110-mL corrugated piece of tubing and a vibrating mesh nebulizer (e-Flow rapid®).
Method:
The inhaled mass of amikacin was assessed using the residual gravimetric method. Delivery efficacy was evaluated by assessing amikacin urinary drug concentration in six healthy spontaneously breathing volunteers. Urinary amikacin was monitored by fluorescent polarization immunoassay then cumulative excreted amount and antibiotic elimination rate were calculated.
Results and Conclusions:
The total daily amount of amikacin urinary excretion (Cu) was almost twice as high with eFlow rapid® compared to Sidestream® used alone; intermediate values being observed when the device was coupled to a corrugated piece of tubing. The latter configuration was also associated with a higher total daily amount of amikacin urinary excretion. In vivo drug output rate was around threefold higher with the eFlow Rapid® than with the Sidestream® used in any configuration. These results were concordant to those obtained with in vitro analysis comparing inhaled mass of amikacin for the three nebulizers. The elimination constant (Ke) and the mass median aerodynamic diameter (MMAD) did not differ between the three devices. In conclusion, the vibrating mesh nebulizer is more efficient, promoting larger urinary drug concentration and drug output. Coupling a corrugated piece of tubing to the standard jet nebulizer favors delivery efficacy.
Introduction
Traditional constant-output nebulizers deliver the aerosol at a constant rate during inhalation, exhalation, and breathhold,(9) which is poorly efficient.(10) A large fraction of drug output is wasted during the expiratory phase. Several developments have been made to reduce these drawbacks. The open vent system integrating an inlet that allows air to be drawn into the nebulizer during inhalation represents an alternative method. This early development has promoted increasing nebulizer output during inspiration compared to that generated during expiration. This would lead to lower drug wastage and shorter nebulization time. If the extra vent is blocked, a similar amount of drug would leave the nebulizer and be inhaled, but over a much longer time.(11) A further development comprises the adjunction of a valve system opening during inspiration only. Upon exhalation the valve closes and exhaled air passes out of the device through a separate expiratory pathway. The amount of inhaled drug may be doubled.(12) Adding either a reservoir(13) or a corrugated tube(14,15) on the expiratory way can limit drug losses during exhalation and increase the inhaled amount. Indeed, studies on inhaled drug mass and lung deposition have shown an increase in fine droplet dose delivered to the lung for nebulizers coupled with a reservoir compared to jet nebulizers used alone.(13,16) Combining a corrugated tube represents a simple and low-cost procedure to favor antibiotic lung deposition in hospitalized patients. However, comprehensive comparative studies on the efficacy of jet nebulizer devices coupled or not to a corrugated tube behind the T-pieces are still lacking.
Over the past 10 years, innovative, vibrating, or static inhalation devices based on mesh technology have been developed. This new technology provides several practical advantages such as increased fine particle fraction due to standardized microperforations, higher output rate of inhaled medication, better portability, and easier handling.(17) In vitro studies(18,19) have contributed to establish functional properties of mesh nebulizers, particularly for commercially available devices. However, validation clinical studies with these devices are still missing. Nebulization with mesh devices under controlled inhalation has shown greater efficacy than nebulization with conventional devices.(20) Nebulizers equipped with a microperforated vibrating membrane have been poorly studied for nebulizing aminoglycosides(21) even though they have been regularly used in CF patients,(22) notably to administer inhaled aminoglycosides, the treatment of choice for chronic Pseudomonas aeruginosa (Pa) infections in those patients.(23,24)
This study was designed to evaluate in vitro and in vivo characteristics of the combination of a 110-mL corrugated tube to a standard unvented jet nebulizer, the same nebulizer used alone and using a mesh nebulizer. Finally we analyzed the concordance between our in vitro and in vivo results.
Material and Methods
Nebulizers
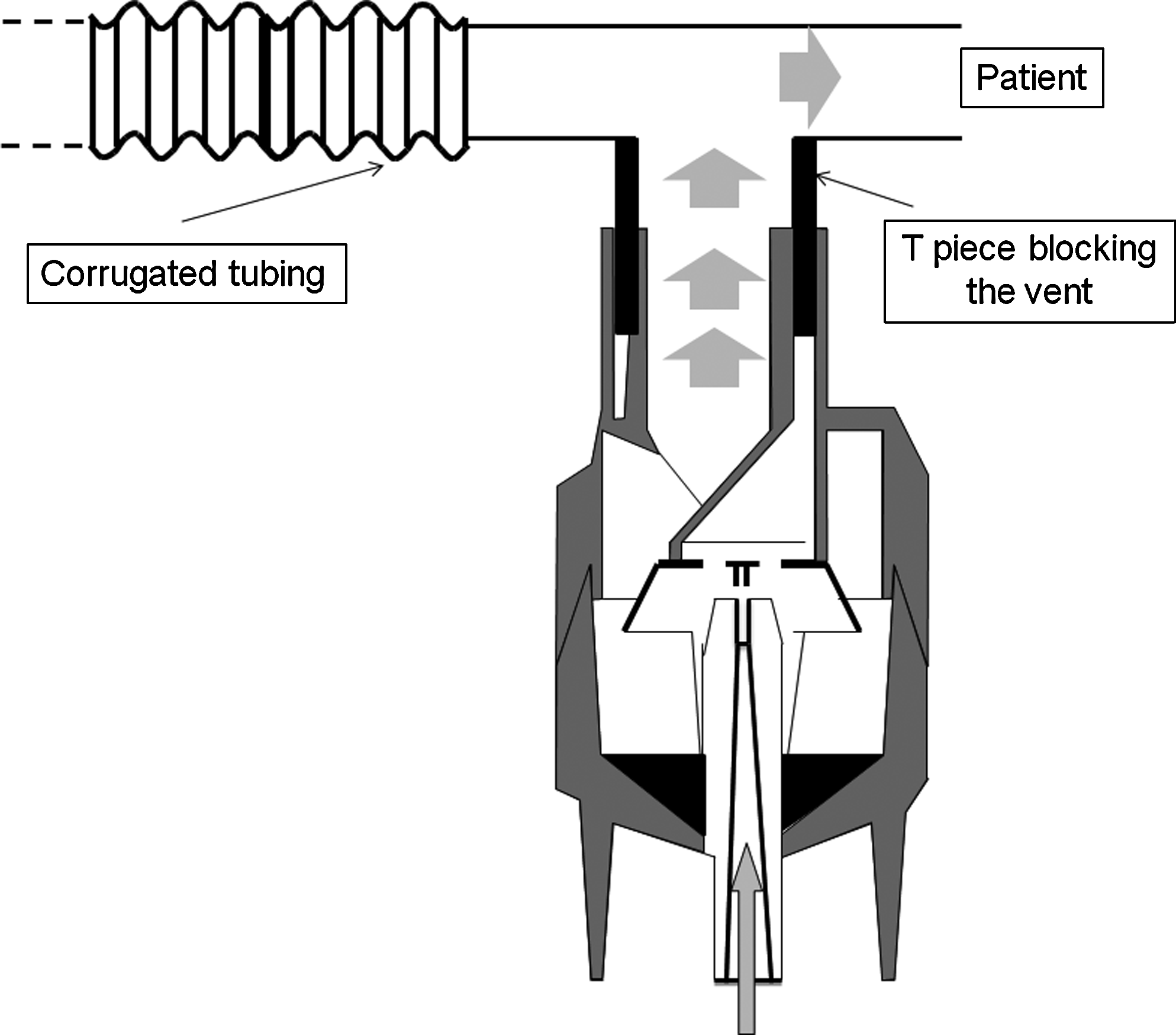
Two types of nebulizers under different configurations were used. A well-known and validated jet nebulizer (Sidestream®, Philips-Respironics. Pittsburgh, PA, USA), used in a modified configuration with a T-piece blocking the extra vent, was used in two configurations: with the T-piece alone (N1) (Fig. 1) or with a 110-mL corrugated tubing connected on the expiratory way (N2) (Fig. 2). The nebulizer was driven by a well-adapted compressor (Portaneb, driving gas flow 6 L/min, Medic-Aid, Pagham, UK). The eFlow rapid® (PARI Pharma GmbH, Munich, Germany) (N3), a nebulizer of new generation using the microperforated vibrating membrane technology, was used as the vibrating mesh reference nebulizer.

Jet nebulizer (Sidestream®, Philips-Respironics, Pittsburgh, PA, USA), used in a modified configuration with a T-piece blocking the extra vent.
Jet nebulizer (Sidestream®, Philips-Respironics), used in a modified configuration with a T-piece blocking the extra vent and a 110-mL corrugated tubing connected on the expiratory way.
Particle size measurement
Particle size distribution from each nebulizer device was assessed using a Malvern Mastersizer-X laser particle sizer (Malvern Instruments Ltd, Malvern, Worcestershire, UK) following the protocol as described by Majoral and colleagues.(25) Nebulizing reservoirs were filled with 4 mL of 125 mg/mL amikacin solution. All measurements were performed in duplicates with three samples of each nebulizer configuration being tested.
Particle size measurements were performed in standing cloud during 1 min of nebulization time. The dispersion code used was “polydisperse” and the optic presentation “2 QAA.” Results, expressed as median mass aerodynamic diameter (MMAD), were carried out using the Mastersizer-X software (Malvern Instruments Ltd). The fraction of the drug mass contained in particles of a diameter between 1 and 5 μm was considered as aerosol respirable mass fraction (RF%)(26) reflecting particle deposition in the bronchial tree.(27)
In vitro assessment of inhaled mass
In vitro experiments were performed to quantify the inhaled mass, the emitted dose as well the dose remaining in the nebulizer at the end of the experiments. The inhaled mass was assessed by the residual gravimetric method.(28)
Each nebulizer was filled with 4 mL of amikacin (125 mg/mL) (Amukin, Bristol-Myers Squibb, Braine l'Alleud, Belgium) and was weighted empty, after filling, and at the end of the nebulization. The nebulizers were connected to a lung model (5600i Dual Adult Training/Test Lung, Michigan Instrument Inc., Grand Rapids, MI, USA) set at 20/min frequency, 440-mL tidal volume, 10% inspiratory pause, and 33% inspiration/expiration ratio.
A filter holder containing a dry filter (Air Safety Ltd, Lancashire, UK), weighted before nebulization, was placed between the lung model and the nebulizer. The solution was nebulized until the end of nebulization for the eFlow rapid® and until 1 min after sputtering point for the two Sidestream® configurations. At the end of the nebulization the filter was dried for 24 h. Drug mass was measured by subtracting the weight of the filter before and 24 h after the nebulization. Before output measurement, relative mass of the drug in total solute mass (drug and excipients) collected on the filters was measured in triplicate. A total of 500 μL of amikacin solution (250 mg/mL) was placed on a dried filter. After 24 h of drying, the filter was weighted. The initial amount of amikacin placed on the filter was expressed proportionally to the difference between both weights, which represents the relative mass of drug. Inhaled mass was calculated by multiplying the drug mass with the relative mass of active compounds. Inhaled mass was measured in triplicate for each nebulizer configuration. All measurements were performed under the same hygrometry conditions. Weights were measured by using a high precision scale (Mettler AE166, Mettler Instruments, Zurich, Switzerland; 0.0001 g precision).
The rate of inhaled mass was expressed as the fraction between the inhaled mass and the duration of the nebulization.
In vitro measurement of pulmonary deposition
Subjects
After approval by our Institutional Ethics Committee, six nonsmoking healthy male volunteers (mean age = 28.5 ± 4.4 years) were recruited. A written informed consent was obtained. Each volunteer performed a spirometry according to the ATS/ERS guidelines,(29) and data were expressed as percentage of predicted value.(30) The subjects did not receive any aminoglycoside during the month prior to the experiments. All subjects declared to be free of allergy to aminoglycosides.
Nebulization
The solution was nebulized until 1 min after the appearance of the sputtering point for Sidestream® configurations and until the end of nebulization for the eFlow rapid®. A 300-μL aliquot was collected from both the initial and the final solutions to monitor amikacin concentrations. The nominal mass of amikacin was defined as the mass of drug filled in the reservoir before nebulization. It was calculated by multiplying the initial volume with the initial amikacin concentration. The residual mass of amikacin was defined as the mass trapped in the reservoir at the end of nebulization. It was calculated by multiplying the residual volume with the final amikacin concentration. Nebulizer drug mass output is defined as the amount of drug leaving the nebulizer and is calculated by subtracting the residual mass of amikacin from the nominal mass of amikacin.
Subjects were randomly assigned to the three nebulizer configurations. Each subject received a single treatment from each device. A washout period of 48 h was observed between each nebulization was performed at the same place at room temperature. Bladder emptying was requested before nebulization. The subjects inhaled the aerosol under spontaneous breathing in a sitting position while wearing a noseclip. During nebulization, tidal volume (Vt; mL), respiratory rate (RR; min−1) and minute ventilation (VE; mL min−1) were continuously monitored by inductance plethysmography (Medical Electronic Construction, MEC, Brussels, Belgium).
Drug monitoring
Urine was collected immediately before and for 24 h following nebulization. Each micturition time and volume were recorded. Urine aliquots were stored at 4°C until further analysis. Urinary amikacin concentration was assessed by fluorescent polarization immunoassay (FPIA, Abbott, IL, USA). The total amount of amikacin excreted in the urine after nebulization (Cu max) was calculated by the sum of cumulative concentrations of amikacin at each collection (Cu) and extrapolated to infinity. The elimination constant (Ke) was calculated from the maximal cumulative urinary amikacin concentrations plotted versus time. The equation used was: Cu = Cu max (1 − e−Ke.t).(31) Data interpretation was performed using JMP software (SAS Institute, Cary, NC, USA) according to the Michaelis-Menten kinetic model.
Statistical analysis
Results are presented as mean ± SD and the coefficient of variation (SD/mean × 100) was used to express data variability. For in vitro data, one-way analysis of variance (ANOVA) was used to assess the differences between devices. For in vivo data, the significance of the differences between devices was assessed by ANOVA for repeated measures. When appropriate, comparisons between groups were made using a post hoc test using the Holm-Sidak correction with 0.05 as a threshold p-value. Subsequently, a p-value obtained with comparison between nebulizer using in vitro and in vivo settings were compared to assess the concordance between the two approaches.
Results
In vitro data
In vitro data are summarized in Figure 3. Inhaled mass was at least twice as high for the eFlow compared to the Sidestream (Fig. 3A). Addition of a corrugated tubing increased the percentage of the nominal dose of amikacin by almost two-thirds compared to the device without tubing (Fig. 3A). The duration of the nebulization was dramatically reduced with the eFlow rapid® and was statistically significantly different from the two Sidestream® configurations (Fig. 3B).

Comparison of in vitro data obtained during nebulization with eFlow rapid® (N1), with Sidestream® alone (N2), or with a spacer (N3). Results are expressed as mean ± SD., mass median aerodynamic diameter. RF, respiratory fraction; NS, not significant; *p < 0.05; **p < 0.01; ***p < 0.001.
Rate of inhaled mass was also different for the three configurations with larger values being observed for the eFlow device and lower values for the jet nebulizer alone (Fig. 3C). The MMAD (Fig. 3D) and the respiratory fraction (Fig. 3E) were not significantly different between the nebulizers.
In vitro data
Anthropometric and spirometric data of subjects are summarized in Table 1. Respiratory parameters are summarized in Table 2. Respiratory rate was significantly lower with eFlow compared to that obtained with Sidestream coupled with an extension (9.2 ± 2.9 min−1 vs. 12.5 ± 2.1 min−1; p = 0.009). Tidal volume and minute ventilation were similar for all three devices.
Results are expressed as mean ± SD.
FVC, forced vital capacity; FEV1, forced expiratory volume in 1 sec.
Results are expressed as mean ± SD, with the coefficient of variation in brackets. Vt, tidal volume; RR, respiratory rate; VE, minute ventilation.
Nebulizer drug mass output was significantly higher with the eFlow rapid® in comparison with the two Sidestream® devices (365.4 ± 27.5 mg for N3 vs. 293.4 ± 102.1 mg for N1 and 289.7 ± 27.5 mg for N2; p < 0.05). Initial amount of amikacin was equal for the three nebulizers. Before starting nebulization, the concentration of amikacin (in the reservoir) was not different among nebulizers (131.2 ± 3.9 mg/mL for N1, 133.3 ± 3.4 mg/mL for N2, 133.7 ± 7.0 mg/mL for N3; P = 0.673). However, at the end of nebulization, the concentration of amikacin (in the reservoir) was significantly higher with the two Sidestream® nebulizers in comparison with the eFlow rapid® (186.5 ± 9.5 mg/mL for N1 and 192.7 ±11.1 mg/mL for N2 vs. 138.3 ± 5.4 mg/mL for N3; p < 0.001). Coupling of an extension to the nebulizer did not modify final drug concentrations. Indeed, no difference was observed between final amikacin concentrations obtained from the two Sidestream® nebulizers (p = 0.494). The residual mass of amikacin at the end of nebulization was higher with the two Sidestream configurations than with the eFlow rapid (260.4 ± 39 mg for N1 and 260.5 ± 13 mg for N2 vs. 181.7 ± 20 for N3; p = 0.01).
Urinary levels of amikacin were monitored in the absence of any nebulization treatment. Amikacin concentration obtained from six urine samples during the pretreatment period before the second and the third nebulization averaged 1.4 ± 0.4 μg/mL and 1.6 ± 0.7 μg/mL, respectively. As these values felt below the limit of quantification of the analytical method they were considered as a “zero” level.
Pharmacokinetic data are summarized in Figure 4. The total daily amount of urinary amikacin excretion (Cu) was significantly higher with the vibrating mesh nebulizer than with the two jet nebulizer devices. Intermediate values of urinary amikacin excretion were found for the jet nebulizer coupled with a spacer (Fig. 4A). The variation coefficient was different for the three nebulizers (26% for N1, 15% for N2, and 22% for N3). Nebulization time was shortest with the vibrating mesh nebulizer and longest with the jet nebulizer that was not coupled to the extension (Fig. 4B). Drug output rate was much higher for the vibrating mesh nebulizer with intermediate values being obtained for the jet nebulizer coupled with a spacer (Fig. 4C). The elimination constant (Ke) was not significantly different between the three devices (p = 0.71) (Fig. 4D).

Descriptive plot of comparison of pharmacological data obtained after nebulization with eFlow rapid® (N1), with Sidestream® alone (N2), or with a spacer (N3) in six healthy subjects. Results are plotted for each subject, the horizontal lines represent the mean values. Cu Max, total daily amount of urinary amikacin excretion. NS, not significant; *p < 0.05; **p < 0.01; ***p < 0.001.
As illustrated in Figure 5, even though similar profiles were observed for each individual subject, intersubject variability for Cu max was found to be lower with the Sidestream alone and higher for the e-Flow rapid. The daily excreted amount of amikacin was 6.15% of the initial dose for N1, 8.2% for N2 and 11.6% for N3.

Total daily urinary amikacin excretion for the six subjects. Results are expressed as mean (mg). N1, Sidestream®; N2 Sidesteam® + spacer; N3, eFlow rapid®.
The in vitro data concerning the inhaled mass were in good agreement with the in vivo data on urinary excretion. Indeed, significant differences were found between the three nebulizers when comparing in vitro data as well as when comparing in vivo data.
Discussion
Our work showed that coupling a spacer to an unvented Sidestream® jet nebulizer increased efficacy of drug delivery to the lung. Our data also showed that eFlow rapid® delivered more drug over a shorter period of time in comparison to the two Sidestream® configurations. Finally, we showed that the amount of amikacin excreted in the urine in healthy subjects is in concordance with the in vitro measurements of lung inhaled mass for the three device configurations studied.
Our results are in agreement with other findings showing that only a small fraction of the nebulized drug is finally deposited in the lung with jet nebulizers.(31,32) We found that only 6.2% of the nominal dose was deposited in the lung with the Sidestream®. Corcoran and colleagues have previously reported that a reservoir bag associated with a standard jet nebulizer increases the delivery rate of nebulized medication.(16) This finding supports our data, which show that coupling a corrugated tube to the Sidestream® promotes increased amikacin urinary excretion of 33% compared with the Sidestream® alone. This higher amount of amikacin excreted in the urine can be explained by the bolus of the aerosol trapped in the corrugated tube during the expiratory phase allowing generation of a higher quantity of aerosol during the inspiratory phase. These results are in accordance with to those of Corcoran and colleagues,(13) who reported a 31.8% increase in the fine droplet dose delivered to the lung when using a reservoir coupled to a jet nebulizer, compared to the same jet nebulizer alone.
Some factors could contribute to explaining the striking increase in urinary amikacin excretion when using the eFlow rapid®. This could be related, at least partly, to the higher inhaled mass as evidenced by our in vitro results. The higher drug mass output observed in our in vivo experiments with the eFlow rapid® could also partly explain the increased urinary drug excretion. Another feature possibly contributing to this issue is the higher aerosol concentration, particularly at the beginning of inhalation.(33) The higher drug concentration at the beginning of the inhalation is probably due to the 30-mL aerosol holding chamber. During exhalation, the patient breathes through an expiratory valve allowing aerosol to fill the chamber where it is held for the next inspiration.(21) Moreover, the eFlow rapid® has a higher nebulizer output in comparison with a standard jet nebulizer.(21) The higher deposition with eFlow rapid®, even though nebulizer output and MMAD were similar, could also be explained by the higher residual mass of drug found in the residual volume with Sidestream®, which could explain the lower amount of drug administrated to the lungs as the residual volume is the same.
Our results show a significant reduction of the nebulization time with eFlow rapid® compared to the unvented Sidestream®, which improves nebulizer output rate and could be associated with enhanced patient compliance.(34) Comparable decrease in duration of nebulization with eFlow rapid® compared to a breath enhanced jet nebulizer has recently been reported.(35)
The amount of amikacin excreted in the urine was fairly inhomogeneous with the eFlow rapid® and the Sidestream® with spacer. The variability of the Sidestream® is equal to that measured in a previous study.(31) By contrast, data from another group(36) showed that the variation coefficient was more homogenous for the measurement of lung deposition within 15% of the mean for the PARI LC PLUS® and 10% for the eFlow. Hubert and colleagues,(35) in a recent blood pharmacokinetic study, have shown a greater variability of the Cu Max measured at 86 and 56%, respectively, for eFlow rapid® and the Pari LC Plus®. Moreover, this larger variability could be explained by the fact that the population studied was composed by CF patients and not by healthy subjects.(10,37)
However there was a significant difference in aerosol delivery to the lung between the three nebulizers, although the drug kinetics were identical for the three devices, confirming that the difference in urinary elimination was due to the difference in aerosol efficacy. The total amount of amikacin excreted is linked to the effect of the devices on the subjects. As the nebulizations were paired, the influence of the subject was then eliminated. The elimination constant reflects the penetration depth of nebulized drug into the lung.(38) A more peripheral deposition would be associated with a higher elimination constant due to the greater absorption in lung periphery. In other words, material deposited in the alveoli would be absorbed rapidly, whereas that deposited higher in the airways would be absorbed more slowly. Particle size and respirable mass fractions did not differ between the three devices. As particle size and respiratory fraction determine a preferential localization of lung deposition,(39) our results suggest that lung deposition distribution was identical and not related to the device or the configuration used.
The respiratory rate was significantly lower with the eFlow rapid® in comparison with the Sidestream® with a spacer. These results could be explained by a possible lung irritant effect of aminoglycosides, more important with a greater output rate, that is, a higher aerosol concentration.
O'Riordan(40) showed that the use of a valved holding chamber resulted in an almost twofold reduction in MMAD compared with the same jet nebulizer with a T-piece. Our results show that coupling a corrugated tube did not affect particle size or respiratory fraction.
Our results are also in accordance with the well-known increase in concentration of the drug solution into the reservoir during the nebulization period due to evaporation of the solvent(41) with the jet nebulizers. Moreover, we also demonstrated a higher drug concentration with eFlow rapid® at the end of the nebulization compared to the drug concentration in the nominal dose. This finding could be explained by solvent evaporation during nebulization due to an increased temperature of the drug solution during the experiment (data not shown).
This study focused on healthy subjects. This may certainly contribute to a better homogeneity of aerosol distribution and ease the comparison between devices. As large difference in lung properties and breathing pattern can be observed in pathological conditions, further investigations in relation to specific disease groups should be performed.
In conclusion, the present study clearly showed that the unvented Sidestream® coupled with an extension was associated to an increased dose deposition. Coupling with a spacer could be easily adopted in daily practice in order to administer large antibiotic doses to hospitalized patients. We also showed that eFlow rapid® was more efficient in terms of lung deposition and drug output for amikacin nebulization in comparison with an unvented Sidestream® jet nebulizer, although it displayed larger intersubject variability. The eFlow rapid® seems to be favorable to the nebulization of aminoglycosides due to its high dose delivery to the lung. Further studies are required to verify our results in specific lung diseases.
Footnotes
Acknowledgments
This work was supported by the Belgian Fonds National de la Recherche Scientifique (grant no. 3.4529.10). The authors further thank Mrs Stéphanie Asta for dosing urinary amikacin, Prof. Claire de Burbure for revising the manuscript, and Dr. Flora Mususamba for statistical advice.
Author Disclosure Statement
Aerodrug is a department of La Diffusion Technique Francaise (Saint Etienne, France). L. Vecellio is an employee of la Diffusion Technique Française.