
Abstract
Abstract
Background:
We investigated whether combination chemotherapy, targeted with the AeroProbe® Intracorporeal Nebulizing Catheter (INC), could be safely administered, and developed a radiologic grading scheme to monitor subclinical effects on the lungs.
Methods:
In anesthetized and mechanically ventilated healthy dogs (n = 3), we introduced the INC via a flexible bronchoscope into the right caudal lung lobe and administered escalating dosages of gemcitabine (1, 2, 3, or 6 mg/kg) followed by cisplatin (10 mg/m2). Treatments were performed every 2 weeks for 4 treatments and dogs were monitored weekly with physical examination, biochemical tests, and thoracic radiographs. Dogs were sacrificed 2 weeks after the final treatment and tissues examined histologically. A radiologic grading scheme was developed to monitor subclinical pulmonary toxicity.
Results:
No significant side effects occurred in any dog. All dogs developed focal pneumonitis radiographically, and chronic, severe pneumonia with fibrosis histologically limited to the treated portion of the lung. Radiologic scores increased over time following increasing doses of chemotherapy.
Conclusions:
Targeted aerosol delivery of gemcitabine and cisplatin by INC was clinically well tolerated. This minimally invasive method is promising for lung cancer treatment, especially given the lack of clinical toxicity. The proposed radiologic grading scheme provides a method to monitor subclinical local drug toxicity.
Introduction
Lung cancer in people has the highest mortality rate among cancers. In 2010, it is estimated that 222,520 men and women (116,750 men, 105,770 women) will be diagnosed with lung cancer, and 157,300 men and women will die of this disease. For patients with lung cancer, 5-year survival rates with chemotherapy or combinations of surgery, chemotherapy, and radiation therapy rarely exceed 15%.(2,3) Novel therapies are direly needed for lung cancer because of its devastating impact on quality of life and high fatality rate.
The standard of care for lung cancer chemotherapy in people involves platinum-based, double-agent protocols, and chemotherapy improves survival time and quality of life, as well as decreases disease-related symptoms.(4) However, with systemic chemotherapy, less than 6% of the administered dose is distributed to the lung tissue.(5) Inhalant chemotherapy has been attempted in both people and dogs for the treatment of primary and metastatic lung cancer in limited reports. Treatment has been effective for approximately 25–60% of people and dogs treated in this manner.(6–10) Previous investigators primarily employed jet nebulizers for aerosolization,(6–10) whereas newer aerosol technologies such as vibrating mesh nebulizers and microsprayers are more efficient for aerosol delivery.
We have shown that by delivering chemotherapy directly to the lung or targeting to a selected lung lobe, higher drug concentrations are achieved in tissue using lower doses and with less systemic drug effects.(11) In our previous study we delivered escalating doses of cisplatin (CDDP) to a selected lung lobe in normal dogs, resulting in superior tissue drug concentrations compared to intravenous administration.(11) Lung damage (pneumonitis and fibrosis) was confined to a small portion of the treated lung lobe. Increased drug concentrations in the affected lung tissue could improve efficacy of chemotherapy for lung cancer. Physical characteristics of the delivery device used in that study, the Aeroprobe Intracorporeal Nebulization Catheter® (INC), and the spray it generates have been described.(11) Briefly, the INC is a catheter designed to feed through the biopsy channel of a bronchoscope. It consists of a central channel for fluid passage that is surrounded by channels for air passage under pressure. The jets of pressurized air generate a plume of aerosol droplets from the fluid stream.
Because inhalant chemotherapy has very low systemic toxicity,(6–11) it is likely that local toxicity will be dose-limiting long before systemic toxicity.(9) However, with the exception of radiological scoring systems to monitor lungs of coal mine workers (1980 International Labour Office (ILO) International Classification of Radiographs of Pneumoconioses),(12) no guidelines exist to quantify pulmonary changes secondary to targeted aerosolized chemotherapy. Pneumonitis has been assigned grades of toxicity according to the National Cancer Institute Common Toxicity Criteria for Adverse Events.(13) However, these designations are strictly based on clinical performance and not on imaging. A radiologic grading scheme could help to monitor subclinical pulmonary toxicity following inhalation of chemotherapy.
Most regimens for lung cancer treatment employ combinations of chemotherapeutic agents. Multidrug chemotherapy is typically more efficacious than single agent therapy, and synergism has been reported when combining antimetabolites with platinum chemotherapy agents, such as CDDP. The purpose of the current study was to evaluate tolerance and safety of intrapulmonary targeted combination chemotherapy via the INC. Accordingly, we administered escalating dosages of gemcitabine sequentially with a set background dose of CDDP to the right caudal lung lobe in normal dogs. Additionally, we developed a grading scheme to assess the severity of radiographic changes in the lungs of treated dogs that could be applied to future studies and clinical trials.
Materials and Methods
Subjects
The protocol was approved by the Institutional Animal Care and Use Committee and dogs were used and housed at the University of Missouri College of Veterinary Medicine, which is AAALAC accredited. Healthy dogs (n = 3) were obtained from a certified distributor and evaluated by physical examination, baseline thoracic radiographs, as well as hematologic and biochemical screening. Dogs were observed twice daily by kennel staff, and at least once daily by investigators. Any abnormalities in health status such as vomiting, inappetance, diarrhea, or cough were reported by kennel staff.
Procedures
Dogs were anesthetized and mechanically ventilated. Dogs were first premedicated with intramuscular injections of butorphanol (0.5 mg/kg), xylazine (0.5 mg/kg), and glycopyrrolate (0.01 mg/kg) to achieve analgesia, sedation, and antitussive effects. Anesthesia was induced by mask and maintained using isoflurane gas (0.5–2.0%) by inhalation. All dogs were placed on positive pressure ventilation to provide consistency. Anesthesia was maintained at the depth needed to allow bronchoscopy. Cardiopulmonary monitoring was accomplished by electrocardiographic and pulse oximetry measurements as well as physical examination.
Procedures were identical to those employed in our previous study. Briefly, normal saline was administered intravenously at a rate of 5 mL/kg/h throughout the procedure. Each dog was placed in sternal recumbency and bronchoscopy was performed with Olympus BF1T20D endoscope (Olympus America, Center Valley, PA). The Aeroprobe INC® was then inserted through the biopsy channel of the bronchoscope and positioned at the bronchus for the right caudal lung lobe (RCLL). Once positioned, gemcitabine (escalating dosages at sequential treatments of 1, 2, 3, or 6 mg/kg of a 40 mg/mL solution reconstituted according to manufacturer's instructions, Eli Lilly, Indianapolis, IN) followed immediately by CDDP (10 mg/m2 of 1 mg/mL solution, APP Pharmaceuticals, LLC, Schaumburg, IL) was aerosolized into the RCLL through the INC. Dogs were recovered and monitored with weekly radiographs, complete blood counts (CBCs), serum, or plasma chemistry profiles and urinalysis. CBCs were collected twice weekly to determine myelosuppression. Treatments were repeated every 2 weeks for 4 treatments (10 weeks total protocol duration). The total cumulative dose of each drug was thus 40 mg/m2 for CDDP, and 12 mg/kg gemcitabine. Two weeks after the last treatment, dogs were euthanized and tissues harvested immediately postmortem for gross and histologic examination, as per our prior study.(11) A 2-week interval was chosen to allow some tissue recovery between doses, and to allow systemic effects, if any, to abate.
Additionally, our previous study included 3 dogs with similar origin and husbandry to which we administered four escalating doses of CDDP (10, 15, 20, and 30 mg/m2) at 2-week intervals.(11) Dogs were sacrificed on week 10. A fourth dog was treated with a single high dose (30 mg/m2) of CDDP and sacrificed 2 weeks later. Radiographic images of the lungs of these dogs were also used for the development of a radiologic grading scheme for the study presented here. The only difference between that study and the study presented here was the change in drugs and the fact that in the present study we did not perform intravenous dosing or pharmacokinetics. Identical procedures were employed for administration of inhalant chemotherapy and monitoring in the two studies.
Radiologic grading scheme
Because it became evident that local toxicity to the lungs following inhaled chemotherapy could be dose-limiting well in advance of systemic toxicity, a grading scheme was developed to document radiographic changes occurring in the lungs of treated dogs. Thoracic radiographs were reviewed from dogs in this (n = 3) and the previous study (n = 4), which had radiologic and histologic findings similar to those in the present study.(11) Interstitial, bronchiolar, and alveolar changes were each scored as mild, moderate, or severe, and the distribution of abnormalities was classified as focal versus multifocal. All radiologic scores were assigned by one board-certified veterinary radiologist (S.E.) who was blinded to the treatment scheme. In order to create the grading scheme (Table 1) final histologic findings were considered and correlated to radiographic findings immediately prior to sacrifice. Thus, radiographic findings immediately prior to euthanasia were considered to be the most severe, and radiographic appearance at baseline was considered to be unaffected (score of 0). Scores were then extrapolated to account for the progression of radiographic changes seen between baseline and final radiographic evaluation. A radiologic score was assigned to weekly radiographs from all seven dogs.
Results
Clinically, dogs did not show any signs of overt toxicity (cough, vomiting, diarrhea). Hematologic parameters were normal throughout the study except for mild neutropenia in one dog seen 1 week after the final treatment. Additionally, plasma chemistry evaluations were all normal except for an occasional mild decrease in sodium and chloride levels. Urinalyses were normal in all dogs. All deviations from normal in hematologic and biochemical evaluation were clinically insignificant.
Radiographic evaluation revealed focal, mild to moderate peribronchiolar infiltrates progressing to an interstitial–alveolar pattern in the right middle and caudal lung lobes. Changes improved slightly in between treatments, with gradual progression over time. This pattern was similar among dogs treated, regardless of treatment group. The composite scores were assigned as the sum of the individual scores using the proposed grading system, resulting in semiquantified toxicity as shown in Figure 1.
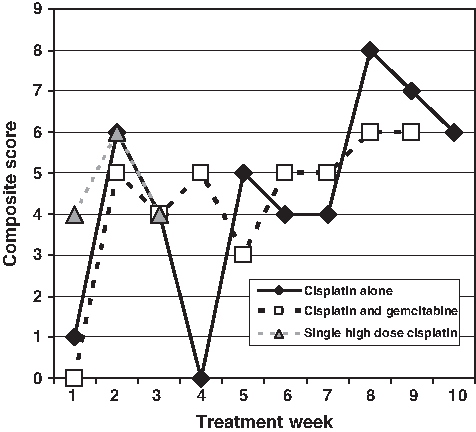
Radiographic composite scores (sum of scores for interstitial, peribronchial, alveolar, and location as described in Table 1) for dogs treated with inhalant CDDP alone (n = 3) or inhalant gemcitabine combined with CDDP (n = 3) or single high-dose CDDP (n = 1). Data are expressed as a mean and graphed by treatment group. Treatments were administered on odd-numbered weeks. Evaluation by median and interquartile range gave similar results (data not shown), and evaluation of all groups combined showed a gradually increasing score (data not shown).
Considering toxicity of chemotherapy as graded 0–5 according to the Veterinary Cooperative Oncology Group modification of the human system of Common Terminology Criteria for Adverse Events (as well as the human classification scheme),(13) we interpreted the composite scores and combined them with subjective clinical assessment to propose a classification of grading toxicity due to inhalant therapy. Grade 0 (no toxicity) would be assigned if there is no change from baseline in appearance of pulmonary structures. Likewise, Grade 1 (mild) would be assigned for composite scores 1–3, Grade 2 (moderate) for scores 4–5, Grade 3 (severe) for scores 6–7, Grade 4 (life-threatening) for scores greater than 7, and Grade 5 for death due to respiratory failure following inhalant therapy. For application in future studies, if more than one lung lobe is treated, then each lobe or hemithorax should be graded separately and the highest grade assigned will dictate the severity of toxicity (Table 1).
Following treatment, the various patterns of radiographic pulmonary infiltrates included alveolar flooding with lobar margination, unstructured interstitial patterns of varying severities, and mild to severe peribronchial thickening. Radiographic changes progressed in severity throughout treatment, leading to increased score and higher final grade (Fig. 1). Peribronchial radiographic findings appeared after the second treatment and then worsened over the course of the study. Presence of radiographic peribronchial changes resulted in higher toxicity score and grade.
Results of postmortem examination demonstrated macroscopic and microscopic changes that were confined to portions of the right caudal and middle lung lobe (Fig. 2, arrow). Histologically, all dogs developed similar changes consisting of severe pneumonitis with moderate to severe peribronchial fibrosis, localized to a portion of the treated lobe (Fig. 3A and B). Involved areas showed collapsed alveoli containing some lymphocytes and hemosiderin-laden macrophages. Additionally, type II pneumocyte hyperplasia was seen. Although the bronchial mucosa was normal, bronchiolar mucosa was denuded with reepithelialization by hypertrophic and dysplastic epithelial cells. Untreated lung lobes showed normal gross and histologic appearance.
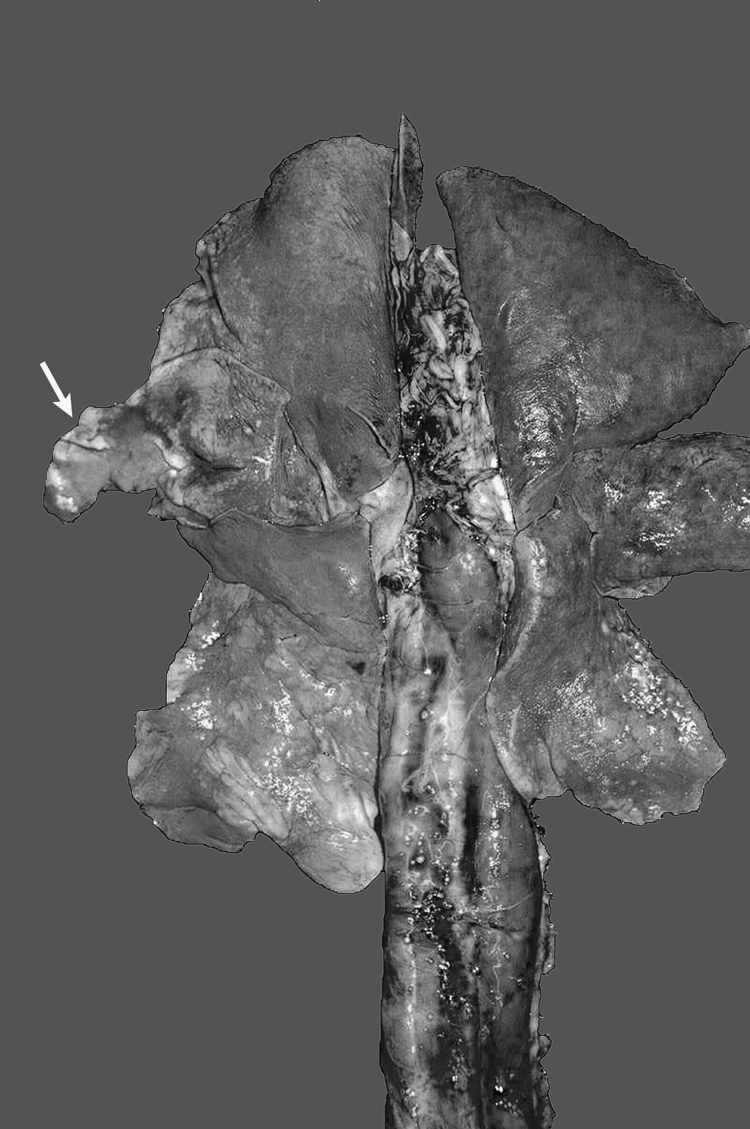
Lungs, esophagus, and trachea showing area of consolidation in right caudal and middle (arrow) lung lobes corresponding to treated area.

Discussion
The present study showed that combining chemotherapy drugs for aerosolized inhalant delivery to the lungs of dogs was clinically well tolerated with acceptable local effects. A combination of CDDP and gemcitabine chemotherapy can be targeted to a selected lung lobe by INC. The administration of a combination of chemotherapy drugs by inhalation for cancer therapy has not been previously reported in dogs or humans. In this study there were adverse effects noted in the adjacent lobe, most likely a result of some variability in placement of the INC. Although severe pneumonitis and fibrosis was observed in a portion of the treated lung lobe, dogs appeared clinically unaffected and these histologic changes may be acceptable in light of the potential benefit. These histologic changes were similar to those seen following single-agent CDDP inhalant therapy as seen in our previous study.(11) In most cancers, combination chemotherapy is more effective than single-agent therapy, and so our findings are critical in order to establish the relative safety of dual-agent cancer therapy by the inhalant route. Our goal was to confirm the feasibility of this approach, as demonstrated in our previous investigation.(11) Clinical trials evaluating efficacy are now indicated. Although drug activity following nebulization was not an objective of this study, previous investigations support preservation of cytotoxic activity following nebulization of CDDP and gemcitabine with the INC and other nebulizers.(14,15)
The choice of chemotherapy drugs for combination in this study was rational given their proposed synergism. This combination is likely to be among the most promising in the inhalational treatment of lung cancer, as both drugs have already shown efficacy when administered systemically and are often used in combination therapy for lung cancer as first-line therapy.(16) CDDP creates large DNA adducts and causes strand breaks. When combined with antimetabolites, this DNA damage is potentiated and attempts at DNA repair are hindered by inclusion of false bases from the gemcitabine. It follows, therefore, that combination inhaled chemotherapy could be more effective than treatment with a single agent. Only one report has described inhalation of CDDP aerosol in people,(17) and only our previous work describes its use in dogs.(11) Gemcitabine aerosol therapy has been reported in rodent and baboon models,(14,18) and in a recent report in dogs with metastatic osteosarcoma.(19) Gemcitabine has no reported irritant effects. However, no reports have combined the two drugs given by the inhalant route. Moreover, previous investigators did not selectively target a lung lobe for administration of inhaled chemotherapy. This is important because primary lung cancer is often localized to a portion of the lung or lung lobe; and by targeting inhaled chemotherapy, exposure of normal lung to potentially toxic agents can be minimized.
Because inhaled chemotherapy achieves high concentrations of chemotherapy in the lungs with low systemic concentrations, local toxicity is likely to be dose-limiting long before systemic toxicity.(11) This issue has not been formally addressed in previous reports of inhalant chemotherapy. Because dogs are often initially asymptomatic despite radiographic evidence of worsening pulmonary insult, it is important to develop a noninvasive method by which maximally tolerated dose to the pulmonary parenchyma can be assessed. Although advanced imaging modalities such as computed tomography, positron emission tomography, and magnetic resonance imaging are more sensitive than plain radiography, routine radiographs are more accessible and much less expensive for serial monitoring, especially in animal studies. We found that the radiographic changes worsened with sequential administration of chemotherapy (Fig. 1), eventually progressing to severe grade after administration of four treatments over 8 weeks. Therefore, the radiologic grading scheme and toxicity scoring that is proposed here should be applied to future dog studies in a prospective manner. It is interesting to note that the scores differ at week 4 with a low score attributed to cisplatin alone (0) and higher score with combination chemotherapy (5). Although it is possible that adding gemcitabine also adds toxicity, the fact that scores are similar at earlier and later assessments suggests that either any benefit to single agent therapy is transient, or that the low score for dogs treated with cisplatin alone underestimates the lung changes. Despite the insensitivity of plain radiographs relative to advanced imaging techniques, we were able to document progressive lung changes in asymptomatic dogs, and the cost and convenience of radiography justifies it as a rational tool in monitoring the effects of inhalant chemotherapy. Using dogs as models for translational research, our findings also provide a starting point for similar evaluation in people.
We also considered the fact that adverse events associated with delivery of inhalant chemotherapy could cause lung injury that does not immediately lead to oxygen dependence or other clinical measures of lung function, but could result in delayed fibrosis as is observed following radiation therapy, and as was the case in the present study. Additionally, unpredicted adverse effects, such as the changes seen in the adjacent lung lobe in this study, are important to characterize when evaluating inhalant therapy. Without a method of noninvasively quantifying asymptomatic lung injury, it is not possible to determine a maximally tolerated dose. Because cytotoxic chemotherapy is administered with the goal of achieving a maximally tolerated dose, this is a major limitation of other studies evaluating inhalant chemotherapy. When minimally invasive treatments have to be administered repeatedly, it is also not reasonable to perform serial lung biopsies to assess toxicity histologically. By performing serial radiographs and applying the proposed grading scheme, it should be possible to monitor subclinical pulmonary toxicity following inhalation chemotherapy, and to determine a maximal tolerated dose.
Although the dogs reported here received radiographs weekly, there likely was little or no contribution of radiation injury to the findings reported here. The total dose of radiation to the lungs of the dogs in this study is predicted to be approximately 1–2 cGy, whereas the minimum dose required for acute or chronic pneumonitis is estimated to be 1750 cGy.(20)
Radiologic and histologic changes associated with the treatment were detected; however, it is not known whether these would have ameliorated with time. In fact, radiographic changes did improve between treatments. It is possible that much of the pneumonitis would have subsided in time. Although the function of the affected lobe is unknown, animals and people typically can tolerate decreased function or lack of a single lung lobe, and our study showed that other lung lobes were unaffected clinically, radiographically, and histologically.
We chose the INC for drug delivery because the catheter allows delivery to an isolated lobe. Additionally, aerosolized sprays (defined as fine liquid droplets in a gas) have been shown to be superior to mask or even endotracheal tube delivery of jet nebulized solutions with more than 60% of solution reaching the lung with an aerosol spray device similar to the INC, and less than 2% of solution reaching the lung with other methods.(21) In our previous study, we found uniformly high concentrations of CDDP in the targeted lung lobe.(11) Thus, drug delivery with the INC achieves high peripheral pulmonary lung deposition in the specified lung lobe. Despite these advantages, use of the INC does entail repeated anesthetic events and intubation. Although the use of a bronchoscope is not necessary, it helps to visualize positioning of the INC at the airway opening leading to the targeted lung lobe.
Future studies will examine efficacy of inhalation chemotherapy in tumor-bearing patients, reversibility of toxicity induced in the lung, application of the radiologic grading scheme, and correlation of the grading scheme to other methods of monitoring lung injury (such as advanced imaging and biologic testing). The feasibility and safety of administering chemotherapy noninvasively by the INC suggests this mode of administration could be a viable treatment option for lung cancer.
Footnotes
Acknowledgments
The authors appreciate the intellectual support of George Baran and Bryan Finlay of Trudell Medical, Inc. This article was supported by Joan's Legacy Foundation. The authors also thank Trudell Medical, Inc., for the generous gift of the INCs employed in this study.
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.