
Abstract
Abstract
Background:
Changes in fractional exhaled nitric oxide (FeNO) occurring after bronchial allergen challenges (BAC) are still not understood, neither are any possible associations between FeNO and forced expiratory volume in 1 sec (FEV1). The aim of the study was to compare the fluctuations of FeNO and FEV1, which occur within 72 h of BAC in children sensitive to grass pollen.
Methods:
Seventy-four children were divided into two groups based on their medical histories and the results of skin prick tests with 10 common allergens. Individuals in whom the test yielded a positive result to at least grass pollen (Group A, n = 57), and those with negative test results against all of the allergens applied (Group B, n = 17) were subjected to BAC. FeNO was measured at a baseline and at 1, 8, 21, and 72 h after the last dose of the allergen inhalation, whereas FEV1 was measured at a baseline, hourly for 8 h after the challenge and at 21 and 72 h thereafter.
Results:
Baseline FeNO in sensitive subjects (Group A) was significantly higher than in controls of Group B. In all grass pollen-sensitive subjects, even those that were free of a bronchial response, FeNO was markedly elevated compared to its baseline values, starting from the eighth hour onward, and still increased 72 h post-BAC, whereas FEV1 returned to a baseline at the 72nd h post-BAC. The highest increase in FeNO was registered in individuals with a dual asthmatic response.
Conclusions:
An increase in FeNO in sensitive subjects starts a few hours later than the decrease in FEV1. Consequently, measurements of FeNO seem to be useful in long-term monitoring of the allergic reaction triggered by a specific allergen.
Introduction
Moreover, FeNO is known to be elevated in bronchial allergen challenges (BAC), increasing a few hours after the allergen is inhaled.(7–10) However, the dynamics of post-BAC FeNO changes are still not understood, especially in terms of peak values and the duration of the effect. Furthermore, little is known about any possible associations between FeNO and forced expiratory volume in 1 sec(FEV1), which is measured routinely as an outcome of BAC, or between FeNO and nonspecific bronchial hyperreactivity (BHR).
Consequently, the aim of the study was to compare the fluctuations of FeNO and FEV1, which occur within 72 h of BAC in children sensitive to grass pollen. We also determined if the time course of FEV1 and FeNO was affected by sensitivity to allergens other than grass pollen, previous history of antiasthmatic treatment, BHR, or the type of reaction to BAC.
Materials and Methods
The experiments were carried out between October 2006 and January 2007, that is, at a time not affected by the pollen season. All the procedures were approved by the Ethics Committee of the Medical University of Bialystok; the subjects and/or the parents of any of the underaged subjects gave their informed consent before the start of any procedure.
Subjects
Seventy-four children were qualified for the experiment. They were divided into two groups based on their medical histories and the results of the skin prick tests (SPTs) with 10 common allergens (pollens of hazel, alder, birch, grass and mugwort, Dermatophagoides pteronyssinus, Dermatophagoides farinae, cat dander, dog hair, Alternaria tenuis; Allergopharma, Germany). Group A consisted of 57 children with a history of seasonal allergic rhinitis in whom the test yielded a positive result to at least grass pollen (wheals of at least 3 mm in diameter), whereas Group B included 17 healthy children with negative test results against all of the allergens applied. Detailed histories were collected from all subjects with special attention paid to any past occurrences of allergic symptoms and the use of antiasthmatic medications. Either current or past active and passive tobacco smokers were excluded from further analyses based upon their histories. Characteristics of both the groups are summarized in Table 1. Besides clinical parameters, both the groups differed in terms of age and gender structures.
Of predicted value.
Study design
Baseline values of the following parameters were measured prior to the experiment: forced expiratory volume in 1 sec (FEV1), nitric oxide concentration in exhaled air (FeNO), serum concentration of eosinophil derived neurotoxin (EDN), and serum concentrations of total IgE (tIgE) and specific IgE (sIgE) against grass pollen. Moreover, a bronchial provocation test with histamine was performed.
Forced expiratory volume (FEV1). FEV1 was measured by means of Koko Digidoser dosimeter/spirometer (Ferraris, Englewood Ciffs, NJ, USA) according to ERS/ATS guidelines.(11)
Nitric oxide in exhaled air (FeNO). FeNO was measured using a NioxMino® analyzer (Aerocrine, Sweden) at a mouth flow rate of 50 mL/sec and a pressure of 10 cm H2O. At least two measurements were performed, so as to achieve two technically adequate results, not differing from each other by more than 10% with a sustained plateau of at least 8 sec. The lower result of the two tests was considered as appropriate. The measurement range of the device ranged from 5 to 300 pbb, and accuracy amounted to ± 5 ppb for values <50 ppb.
Eosinophil-derived neurotoxin (EDN)
Blood samples were centrifuged 30 min after their collection. Serum was stored at −70°C until the day of evaluation. Commercial ELISA kits (Medical & Biological Laboratories Co. Ltd, Japan) were used to determine serum EDN concentrations.
Bronchial provocation test with histamine
The bronchial provocation test with histamine was performed by the five-breath method according to Rosenthal,(12) using a DeVilbiss 646 jet nebulizer connected to a Koko Digidoser dosimeter/spirometer (Ferraris), powered by compressed air. Histamine was used at concentrations of 0.025, 0.25, 2.5, 10.0, and 25.0 mg/mL. FEV1 was measured 3 min after each concentration inhalation. The test was stopped when two sequential FEV1 values were registered to decrease at least 20% compared to baseline values. Computer software calculated PC20FEV1, that is, the provocative concentration of histamine which caused a 20% decrease from baseline value of FEV1. The result of the test was considered positive when the PC20FEV1 value was lower than or equal to 25 mg/mL of histamine.
Bronchial allergen challenge (BAC)
BAC was carried out with a standardized extract of a grass pollen mixture (catalog No. 006, 5000 SBU/mL, Allergopharma, Germany). The extract was always prepared directly before the challenge test at concentrations of 8, 40, 200, 1000, and 5000 SBU/mL. BAC was performed according to Ryan's method,(13) with our own modification,(14) using the same devices as described above for the histamine challenge. The modification consisted of enlarging the number of inspirations from 5 to 10 and extending the time of aerosol production from 0.6 to 3.0 sec.(14) BAC was always started at the lowest concentration of the allergen. FEV1 was measured 15 min after each allergen inhalation. A 20% or more decline from its baseline value was considered as a positive result of the test. Computer software calculated PC20FEV1; that is, the provocative concentration of allergen which caused a 20% decrease from baseline value of FEV1.
Follow-up measurements of FeNO were taken at 1, 8, 21, and 72 h after the last dose of the allergen inhalation, whereas FEV1 was measured hourly for 8 h after the challenge and at 21 and 72 h thereafter.
Baseline and post-BAC values of FEV1 and FeNO were compared between Groups A and B. Moreover, separate analyses were performed to compare FEV1 and FeNO between the following subgroups of Group A subjects: (1) those sensitive solely to grass pollen allergens versus those who besides grass pollen, had positive results of SPTs to at least one of the other allergens, (2) those with a history of seasonal allergic rhinitis (SAR) and allergic conjunctivitis (AC) versus those who at least once had been prescribed antiasthmatic treatment besides possessing the aforementioned conditions, (3) those with different PC20FEV1 values obtained during the bronchial provocation test with histamine (≤8 mg/mL vs. >8 ≤25 mg/mL vs. >25 mg/mL), and (4) subjects with isolated early asthmatic reaction (EAR+ /LAR−) after BAC versus those with dual asthmatic reaction (EAR+/LAR+) versus those with isolated late asthmatic reaction (EAR−/LAR+) versus those with a negative result of BAC (EAR−/LAR−). Both the early and late asthmatic reactions (EAR and LAR) were defined as a ≥20% decrease from the baseline value of FEV1.
Statistical analysis
Normal distribution of continuous variables was tested by the Kolmogorow-Smirnov test. Logarithmic transformation was used for PC20FEV1 values obtained during the bronchial provocation test with histamine. Mean values between Groups A and B or between dichotomous subgroups of Group A were compared using the Mann-Whitney U-test, whereas the means among multiple subgroups of Group A were compared with the Krauskal-Wallis' test. The significance of time course differences among FEV1 or FeNO values was tested by the Friedman ANOVA test. Associations between continuous variables were analyzed with Spearman's coefficient of linear correlation (r). All calculations were performed using Statistica 8 (StatSoft®, Poland) software, and statistical significance was defined as p ≤ 0.05.
Results
Subjects with positive SPTs versus controls
Histamine and allergen challenges were well tolerated by all the study participants. Baseline characteristics of Groups A and B are shown in Table 1. Subjects of Group B had a higher FEV1, and lower FeNO compared to Group A participants. At baseline, 29 of the 57 Group A subjects had positive results of the bronchial provocation test with histamine (PC20FEV1 <25 mg/mL), including 12 subjects with hyperreactivity characteristic for asthma (PC20FEV1 <8 mg/mL). Baseline FeNO was found to be significantly correlated with PC20FEV1 for histamine (Table 2).
Time changes in FEV1 that were observed due to BAC in Group A patients resembled those occurring in a dual asthmatic reaction. FEV1 in Group A was significantly lower compared to its baseline at any time point analyzed, other than at 72 h post-BAC. FEV1 was also at all times lower than in Group B throughout the study. In the latter group, no significant fluctuations of FEV1 were noted compared to its baseline (Fig. 1), and none of the subjects demonstrated bronchoconstriction during the allergen challenge.
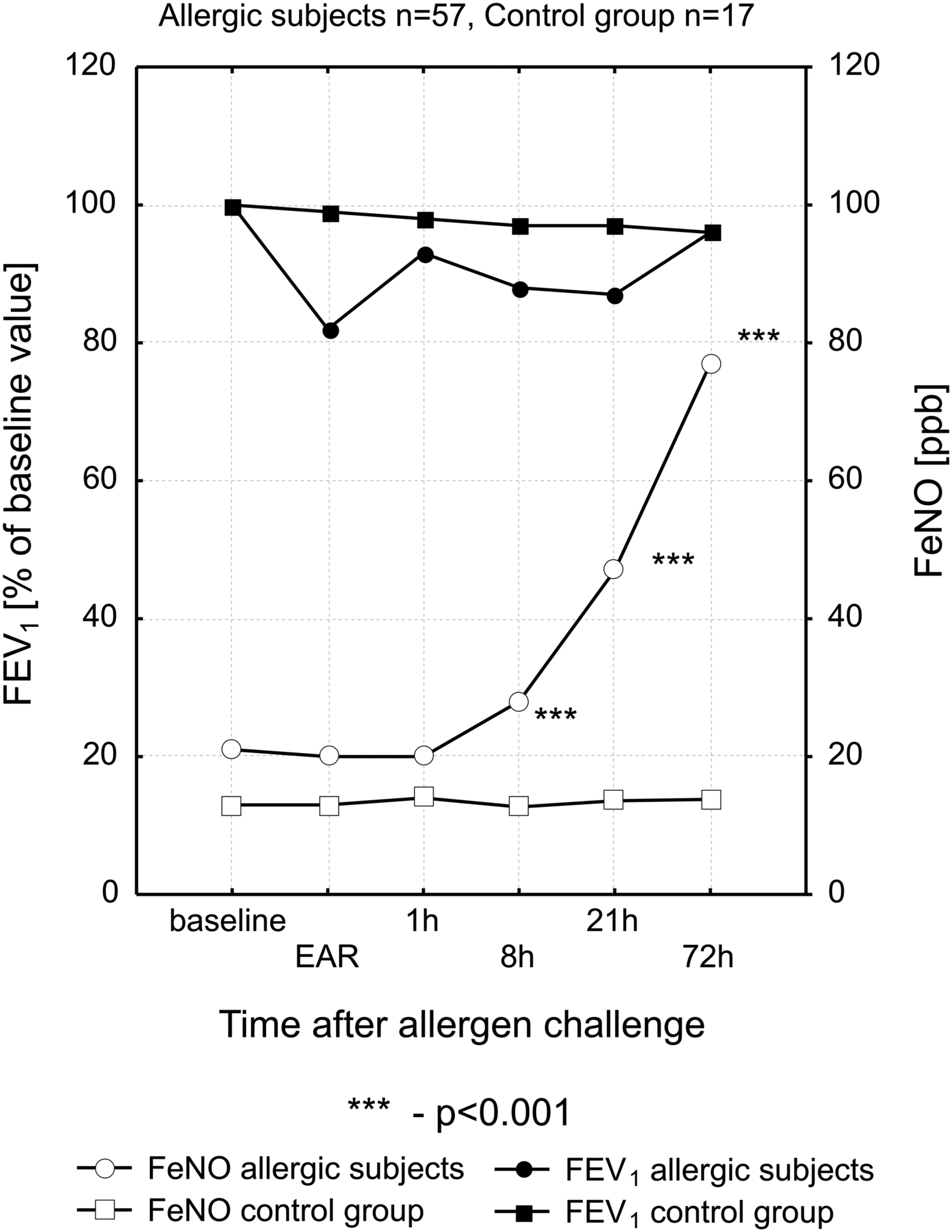
Time course of BAC-induced changes in FEV1 and FeNO in subjects with a history of seasonal allergic rhinitis (Group A, n = 57) and healthy controls (Group B, n = 17).
Post-BAC values of FeNO in Group A were significantly higher compared to the controls at every time point studied. Significant increases in this parameter were observed after 8 h post-BAC and continued for up to 72 h. No significant BAC-related changes in FeNO were in turn observed among Group B subjects (Fig. 1). However, there was a significant correlation between baseline FeNO and the values of that variable 72 h post-BAC (Table 2).
Sensitivity solely to grass pollen versus multiple sensitivity
Initial prick tests revealed that Group A was inhomogenous and comprised of 18 subjects who were sensitive solely to grass pollen allergens, and 39 subjects who had positive SPTs to at least one of the other allergens: tree pollen, mites, cat dander, or molds.
Both subgroups differed in terms of baseline FeNO, which was significantly higher among subjects who besides grass pollen were also sensitive to other common allergens (P < 0.05). Significant correlations between baseline FeNO and PC20FEV1 for histamine or between baseline FeNO and the values of that parameter 72 h post-BAC were noted in the latter group (Table 2). Further time course of post-BAC changes in FeNO did not differ significantly between the groups. Moreover, no significant differences between subgroups described were found in terms of FEV1 at any time point studied (Fig. 2).
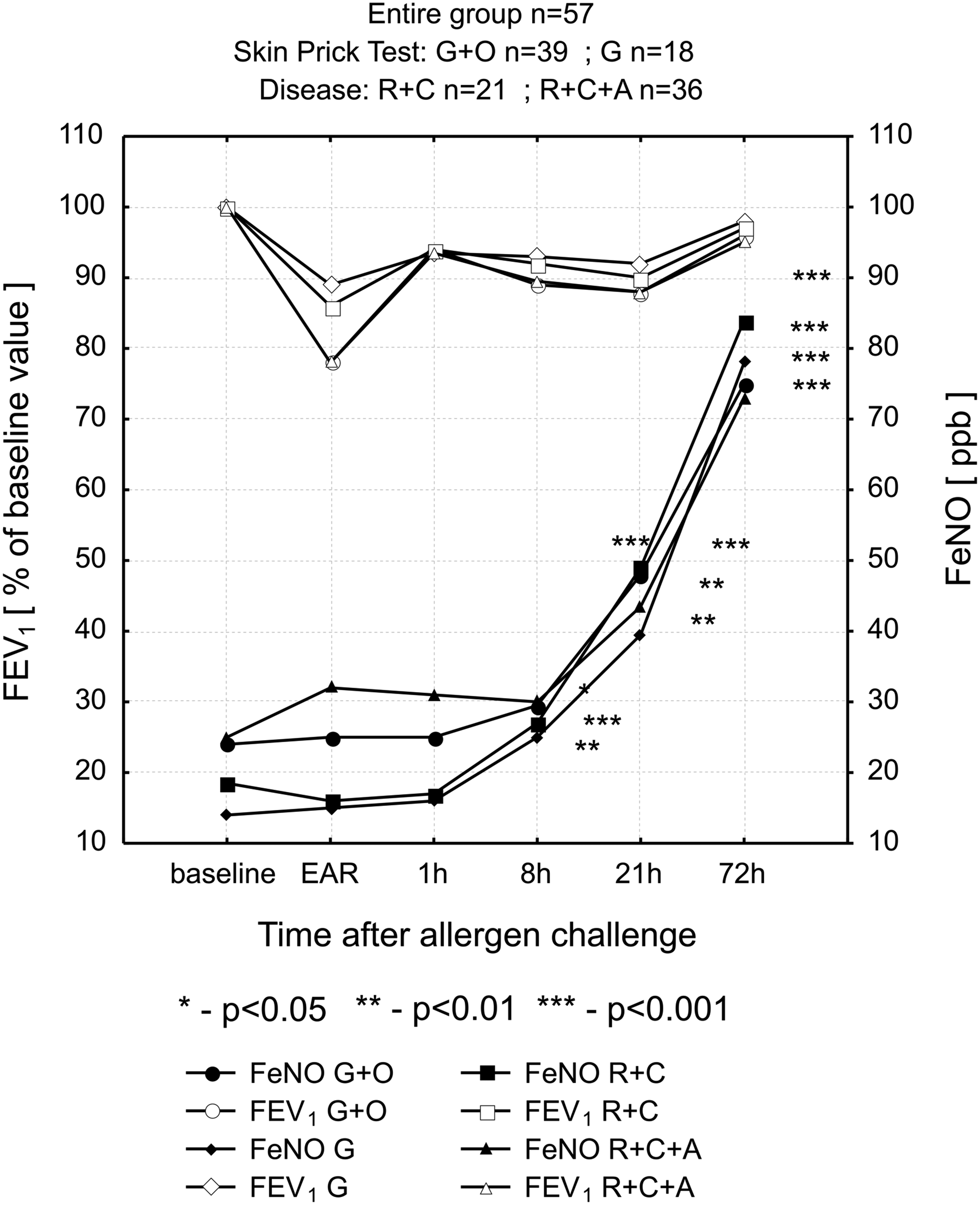
Time course of BAC-induced changes in FEV1 and FeNO in subjects with a history of seasonal allergic rhinitis (Group A, n = 57) stratified based on the results of skin prick tests or medical histories. G = positive solely to grass pollen allergens, n = 18; G+O = positive to grass pollen allergens and at least one of the other allergens, n = 39; R+C = seasonal allergic rhinitis and allergic conjunctivitis, n = 21; R+C+A = seasonal allergic rhinitis and allergic conjunctivitis and antiasthmatic treatment prescribed at least once, n = 36.
Medical history and BAC results
Based on medical history, two subgroups were distinguished among Group A subjects: (1) those with a history of seasonal allergic rhinitis and allergic conjunctivitis (n = 21), and (2) those who at least once had been prescribed antiasthmatic treatment besides the aforementioned conditions (n = 36). The only significant differences between these subgroups pertained to baseline FeNO, which proved to be higher in patients who were previously subjected to antiasthmatic treatment (Fig. 2). Moreover, a significant correlation between baseline FeNO and PC20FEV1 for histamine was noted in the group without antiasthmatic treatment (Table 2).
Histamine challenge and BAC
Based on histamine challenge, subjects of Group A were divided into the following subgroups: (A1) subjects with hyperreactivity characteristic of asthma (PC20FEV1 <8 mg/mL, n = 12), (A2) subjects with positive results (PC20FEV1 ≤25 mg/mL but over 8 mg/mL, n = 17), and (A3) subjects with negative results (PC20FEV1 >25 mg/mL, n = 28). Detailed characteristics of these subgroups are summarized in Table 3. Patients of subgroup A1 had significantly higher serum EDN concentrations and baseline FeNO compared to other subgroups.
of predicted value; binterquartile range.
Also, FeNO measured 72 h post-BAC was the highest in subgroup A1 subjects (Fig. 3). However, the relative increase in FeNO in that group during the 72-h experiment (2.7-fold) was significantly lower compared to other subgroups (4.92-fold and 4.49-fold increase in subgroups A2 and A3, respectively).
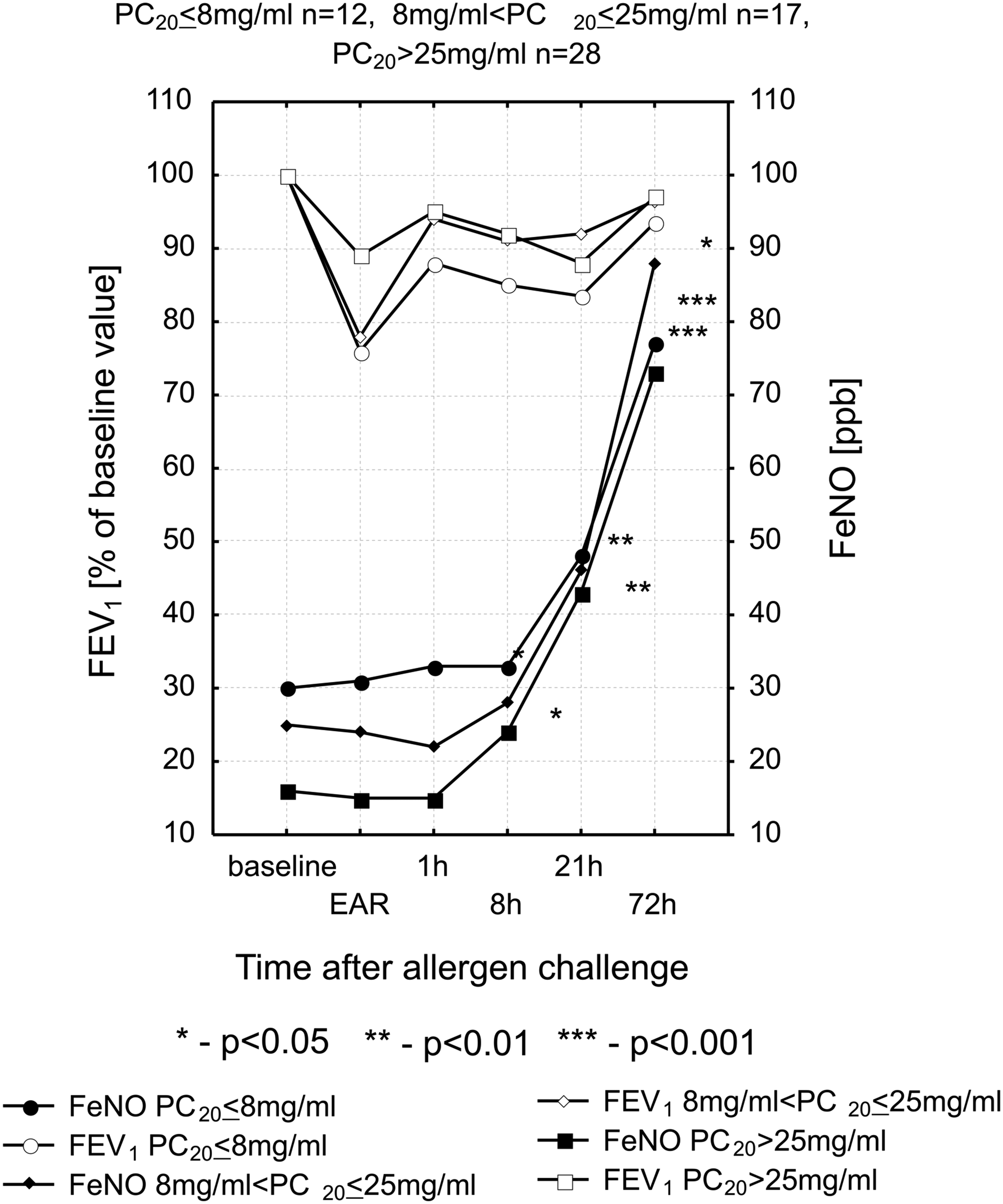
Time course of BAC-induced changes in FEV1 and FeNO in subjects with a history of seasonal allergic rhinitis (Group A, n = 57) stratified based on histamine challenge results.
Type of BAC-induced asthmatic reaction and FeNO
Four groups of patients were distinguished among subjects of Group A based on BAC results: with isolated early asthmatic reaction (EAR+ /LAR−, n = 19), with dual asthmatic reaction (EAR+/LAR+, n = 13), with isolated late asthmatic reaction (EAR−/LAR+, n = 3), and with a negative test result (EAR−/LAR−, n = 22). Their detailed characteristics are presented in Table 4.
of predicted value, binterquartile range.
The relative increase in FeNO during the 72-h experiment was the highest (5.28-fold) in the EAR+/LAR+subgroup, and significantly the lowest in those with isolated LAR or negative test results (3.2-fold and 2.73-fold, respectively) (Fig. 4).
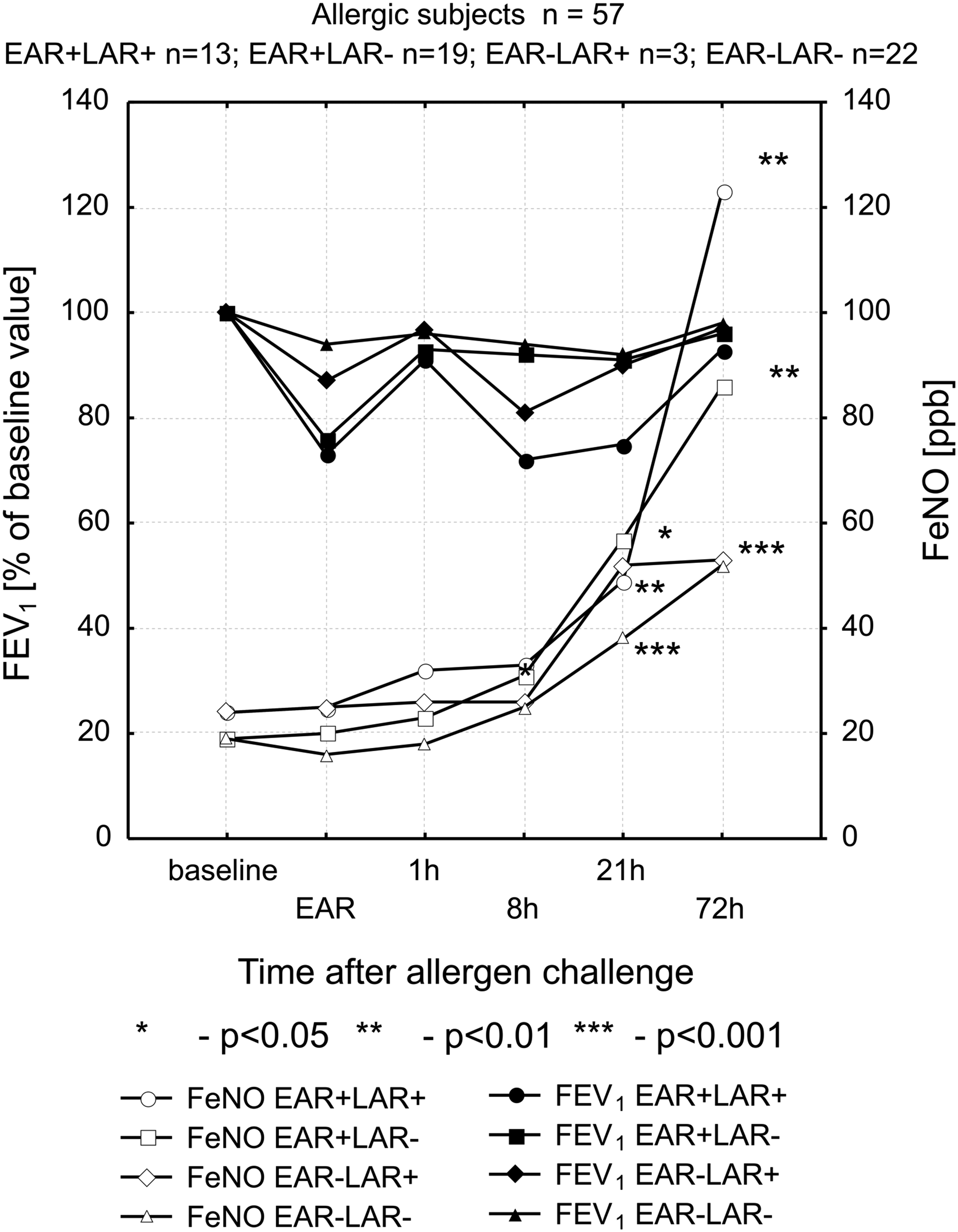
Time course of BAC-induced changes in FEV1 and FeNO in subjects with a history of seasonal allergic rhinitis (Group A, n = 57) stratified based on BAC results.
FeNO and allergen dose
Because 10 out of the 28 individuals with positive reactions to the BAC had negative results to the histamine challenge, correlations between the dose of the allergen that was inhaled and FeNO at baseline or post-72-h challenge were analyzed. An increase in baseline FeNO was revealed to be associated with the lower concentrations of allergen needed to develop bronchoconstriction (r = −0.16, p = 0.420). An increase in the dose of allergen inhaled during BAC was in turn related to increased FeNO after 72 h of the challenge (r = 0.28, p = 0.149). However, the aforementioned correlations were not significant.
Discussion
Our study revealed that FeNO in all grass pollen-sensitive subjects, even those that were free of a bronchial response, was significantly higher compared to its baseline values starting from the eighth hour onward after BAC. However, baseline FeNO in individuals with significant bronchial hyperreactivity, and hence considered to be asthmatics, was two times higher compared to other sensitive subjects. Moreover, patients with bronchial hyperreactivity had twofold higher serum EDN levels than other subgroups analyzed.
Early or late bronchoconstriction was observed in 35 sensitive participants (61.4%) subjected to bronchial provocation. The highest increase in FeNO was registered in individuals with a dual asthmatic response. In all subjects studied, the levels of FeNO were the highest at the 72nd hour after BAC, that is, at a time when FEV1 was already returning to its baseline values.
Several articles on FeNO concentration after an allergen challenge in adults have been published thus far.(7,8,15–17)
Paredi et al.(8) compared changes in exhaled nitric oxide and carbon monoxide resulting from an allergen challenge performed in asthmatics sensitive to different aeroallergens (cat dander, house dust mite, and grass pollen). They found that exhaled nitric oxide was increased in patients with dual asthmatic response only. At the end of the 20-h observation the level of NO in exhaled air still remained elevated in that subgroup.(8) In our study in turn, elevated FeNO was observed in all subjects sensitive to grass pollen following the eighth hour after BAC. Although the follow-up period was considerably longer compared to Paredi et al.,(8) it was also too short to reveal the duration of post-BAC FeNO effect.
Pipari et al.(17) measured FeNO before and 24 h after a specific challenge test performed to assess occupational asthma. The authors concluded that FeNO can be used in monitoring the course of airway inflammation, because it accompanies late asthmatic reactions after a bronchial challenge either in patients with normal or in those with slightly increased basal nitric oxide concentrations. However, in contrast to our observations, they observed no elevation in the exhaled NO in sensitive patients without BAC-related bronchoconstriction.(17) In our study, subjects who were sensitive to grass pollen demonstrated a marked increase in FeNO concentrations in comparison to the baseline value even if no bronchoconstriction occurred during BAC. Consequently, it is very likely that patients who showed no bronchoconstriction after BAC in Pipari et al.(17) study were not in fact sensitive to the allergen evaluated, similar to Group B subjects in our study.
Bodini et al.(18) analyzed the effects of long-term allergen exposure on FeNO and PEF in asthmatic children. They found significant increase in FeNO after moving the subjects from a mite-free environment to a site with natural mite exposure for a period of 19 days. An increase in FeNO was observed for the first 5 days, and then reached a plateau until the end of the exposure. A fall in FeNO concentration accompanied the next allergen avoidance. Fluctuations in PEF values in that group were not significant for the whole period of the study.(18) Consequently, both our study and the experiments of Bodini et al.(18) revealed that FeNO is a more sensitive indicator of long-term airway reaction after allergen exposition than PEF or FEV1.
Lopuhaa et al.(10) analyzed the BAC-related changes in eNO in patients suffering from allergic asthma or allergic rhinitis. Both groups tested being sensitive to Dermatophagoides pteronyssinus. Nitric oxide levels in exhaled air of subjects was measured four times: at baseline, 1 h, 24 h, and 1 week after the allergen challenge. The inhalation of the allergen triggered an increase in eNO which started from 1 h, reached a peak at 24 h and was still elevated 1 week later. Our study revealed that following BAC, FeNO concentrations were significantly higher after 72 h than at 21 h post-BAC. These discrepancies in terms of the FeNO time course post-BAC may have resulted from the different study protocol used by Lopuhaa et al.(10) Thus, both studies confirm the effects of asthma on baseline levels of FeNO. In our study, subjects who were previously treated with antiasthmatic medications had a significantly higher baseline FeNO than subjects with a history of allergic rhinitis only.
The study of Pedroletti et al.(19) did not reveal any changes in FeNO after nasal allergen provocation. The authors concluded that a single nasal allergen challenge does not augment bronchial inflammation.
Tsuburai et al.(20) claimed an increase in exhaled nitric oxide in some patients during the early post-BAC response (1.5 h after allergen inhalation). An early increase in exhaled nitric oxide during EAR was also previously observed by Deykin et al.,(21) but their experiment included only 10 patients.
Thus, it appears that only one of the studies performed thus far claims to show a continuous increase of FeNO after 24 h post-BAC. Another innovative aspect of our experiment is related to fact that it is the first one in which participants were not adults but mostly subjects aged 10 to 16 years.
EDN is a marker of eosinophil activation. According to several recently published studies, it is more accurate biomarker of the asthma severity in children than other molecules, that were previously considered diagnostic standards.(22,23) In our study baseline values of EDN were elevated in subjects with hyperreactivity characteristic of asthma (PC20FEV1 <8 mg/mL) and dual asthmatic reaction to BAC. Also, the relative increase in FeNO following allergen inhalation was the highest in these subjects suggesting indirectly that higher baseline levels of EDN are associated more intense allergic process.
Our study of post-BAC FeNO and FEV1 changes over time significantly contributes to several aspects of current knowledge on bronchial provocation with an allergen. First, it shows that an increase in FeNO after allergen inhalation occurs in all subjects sensitive to grass pollen, whereas bronchoconstriction was noted only in some of them. It is plausible that individuals sensitive to grass pollen who did not demonstrate bronchoconstriction during BAC did so because there was less histamine or/and leukotriene release from mast cells than in those individuals who presented with bronchoconstriction. However, the stimulation of inducible nitric oxide synthase (iNOS) in their airways was probably similar in both groups.
Second, we have shown that in patients demonstrating bronchoconstriction during BAC, an increase in FeNO starts a few hours later than the decrease in FEV1, which may be connected with the time-delayed induction of iNOS responsible for the nitric oxide synthesis.
Finally, we have concluded that measurements of FeNO seem to be useful in long-term monitoring of the allergic reaction triggered by a specific allergen.
Footnotes
Author Disclosure Statement
No conflicts of interest exist.