
Abstract
Abstract
Significant advances have been made in the last 50 years in developing safe and efficacious aerosol formulations for pulmonary delivery. The key to future innovation may lie at the interface between biology and particle engineering. Improved understanding of biological processes including particle clearance, cellular targeting, intracellular trafficking, and drug absorption are needed to better design formulations that deliver to the “target” with the optimal balance of pharmacodynamic, pharmacokinetic, and safety profiles. More specifically, continued advances are needed in the development of: (1) controlled release formulations; (2) formulations with improved regional targeting within the lungs (e.g., airway versus alveoli and vice versa); (3) formulations containing active targeting moieties; (4) formulation strategies for improving the systemic bioavailability of inhaled macromolecules; (5) formulation strategies for delivering macromolecules, including siRNA and DNA into cells; and (f ) formulations with improved dose consistency. It is likely that such innovation will require the development of novel excipients and particle engineering strategies. Future innovation must also take into the account the changing marketplace and the diverse set of customers (patient, healthcare professional, heath authorities, payers, and politicians) who must be satisfied. The pharmacoeconomics of new delivery systems will be closely scrutinized, so it is imperative that cost factors be taken into account. Otherwise, the new technology option may overshoot the evolving inhalation marketplace.
Introduction
A A A
To put these definitions in context for inhaled drug products, consider a brief history of innovation in pressurized metered dose inhalers (pMDI). The first pMDIs for delivery of epinephrine and isoproterenol were marketed in 1956 by Riker Laboratories.(2) This innovation revolutionized the delivery of asthma therapeutics, providing a portable, simple to use delivery system, which effectively targeted the drug directly to the site of action.(3) The first pMDI formulations were comprised of drug dissolved in mixtures of ethanol and chlorofluorocarbon propellants. In subsequent years, a large number of sustaining innovations were advanced. These included the development of suspension-based formulations to deliver drugs with poor solubility in propellant/ethanol mixtures, the development of spacers and valved-holding chambers to improve delivery to the lungs, the development of breath-actuated pMDIs to eliminate issues associated with coordination of the inhalation maneuver with the firing of the device, and many more.(3) The finding that chlorofluorocarbons catalyzed destruction of stratospheric ozone precipitated additional innovation in pMDI products, driving replacement of CFC products with more environmentally friendly hydrofluoroalkane (e.g., HFA-134a and HFA-227)-based products. Although the changes were largely transparent to the patient, incremental advances in formulation, valve design, and materials were required to enable the CFC to HFA transition.(3,4)
The pharmaceutical industry (Pharma) is conservative and risk averse. Owing to the high costs and long development times associated with drug development, Pharma will generally not risk concurrently developing a new drug with a new delivery technology. As a result, the pace of innovation can be slow and disruptive and revolutionary innovations rarely occur. Innovation is also complicated by the multiple customers who must be satisfied. This includes not only the patient, but also healthcare professionals (e.g., doctors, nurses, respiratory therapists), Health Authorities (e.g., FDA, EMEA), and last but not least, the payers and politicians. Unfortunately, the four are not always in alignment.
The balance of this article will focus on innovation in formulation design and its potential impact on the future of pulmonary aerosol products. The Formulation Session revolved around four topics: (1) the role that particle engineering will play in pulmonary drug delivery, (2) the potential advantages that particle engineering may bring to the design of fixed dose combination products, (3) the potential for controlled and targeted delivery of drugs to the lungs, and (4) the future of macromolecule delivery post-Exubera. Additional discussion regarding what remains to be done with respect to formulation design in pMDIs is captured in the companion manuscript in this issue (Smith et al: Inhaler devices: what remains to be done?).
Particle Engineering: Overcoming Interparticle Cohesive Forces to Improve Powder Fluidization and Dispersibility
Dry powder inhalers were first introduced in the early 1970s as alternatives to the aforementioned pMDIs. The early devices (e.g., Spinhaler®, Fisons; Rotahaler®, Glaxo) contained micronized drug packaged in hard gelatin capsules.(5) Powder dispersion was accomplished passively via the patient's inspiratory effort. The typical density of the micronized drug particles was between 1.0 and 1.5 g/cm3, necessitating that the geometric diameter of the particles be less than about 5 μm for effective delivery to the lungs. Unfortunately, micronized particles of this size exhibit strong interparticle cohesive forces, resulting in poor powder flow and dispersibility.(6–9) To overcome this phenomenon, the fine particles are generally blended with coarse lactose carrier particles to form ordered mixtures, or formulated as stabilized agglomerates.(10–12) Low drug loading and lung delivery efficiencies of ca. 10–30% limits the maximum dose that can be delivered in a single inhalation to just a few milligrams, restricting the delivery of some therapeutics as dry powders.(13) An additional consequence of the classical passive device/blend formulation technology is the marked dependence of aerosol performance on the patient's peak inspiratory flow rate (PIF), where increases in powder dispersion at high PIF leads to greater lung deposition. Another perceived disadvantage of the early dry powder inhalers (DPIs) was their dependence on the capsule. Gelatin capsules had to be maintained in a narrow range of humidity to avoid becoming brittle or distorted. As a result, many powders exhibited irreversible coarsening on storage. In addition, capsules were often difficult to handle during an acute asthma attack, especially for the youngest and oldest of patients.
DPI development focused on solving these problems through advances in device engineering. To improve the ease of use, two different types of multidose DPIs were developed: reservoir devices in which bulk powder is metered by the device (e.g., Turbuhaler, Astra-Zeneca), and multidose devices in which the individual doses are premetered and packaged in moisture-proof foil–foil blisters. These devices have been well accepted by patients, but because they still use blends of micronized drug, their modest delivery efficiency remained.(5)
In the last 20 years, advances have been made in understanding interparticle cohesive forces in bulk powders and their impact on powder fluidization and dispersibility.(6–20) For ordered mixtures, analytical techniques including atomic force microscopy, inverse gas chromatography, Raman spectroscopy, and X-ray photoelectron spectroscopy have provided guidance in the development of new blending technologies (e.g., the use of fine lactose and hydrophobic force control agents such as magnesium stearate, leucine, or phospholipids).(10–12) Innovations have also been made in specifically engineering particles to improve bulk powder properties.(13–20)
Particle engineering is characterized by advances in formulation and/or the particle manufacturing process. The goal is to design critical features into the particles, including: improved stability of macromolecules,(21–26) improved powder dispersibility,(13–20) controlled release,(27–33) or increased drug permeability and bioavailability.(34–42) These attributes are introduced through the use of novel excipients into the particles, or alternatively, by insightful control of particle characteristics such as particle density, morphology, microviscosity, or surface energy. In order to achieve these features new process technologies including spray-drying,(13–21,25–26,42–54) foam-drying,(55) supercritical fluid precipitation,(53,54,56,57) solution atomization xrystallization (SAX),(58) high gravity controlled crystallization,(59) and confined impinging jet precipitation(60) have been advanced.
Particle engineering technologies have demonstrated significant improvements in the efficiency of pulmonary delivery compared to standard micronized drugs. Lung delivery efficiencies approaching 70% of the delivered dose have been reported for porous particles prepared by spray-drying processes.(18–20,61–63) The increases in delivery efficiency are the result of reductions in interparticle cohesive forces due to increases in the geometric size of the particles,(16–19) increases in particle porosity or rugosity,(14–20,25–26,48,50,51) and reductions in surface energy achieved with hydrophobic excipients.(25,45,48,61–63) The improved lung targeting may enable reductions in the nominal dose, decreases in local side effects (e.g., reduced throat hoarseness, throat ulceration, and candidiasis for inhaled corticosteroids), and decreases in systemic side effects for orally bioavailable drugs. It may also allow drugs with a fine balance between efficacy and systemic side effects to become patient valuable medicines.
Despite their improved lung targeting, porous particles have yet to penetrate into the asthma/chronic obstructive pulmonary disease (COPD) market. Asthma/COPD pharmacological agents are low cost, potent molecules with a high therapeutic index. They are often administered at the plateau of the dose–response curve, where differences in lung function are not easily discernable. As such, the improvements in delivery efficiencies noted for porous particles have provided little impetus for Pharma to reformulate. Engineered particles have achieved greater success in the delivery of protein therapeutics, where they provide room temperature stable formulations with high delivery efficiencies,(21–26,48,49,55) and in the delivery of anti-infectives, where the high drug loading and high delivery efficiencies enable therapeutic doses up to 25 mg to be delivered in a single inhalation.(32,33,47,50,61,63–67) Being able to deliver anti-Pseudomonal therapeutics with a portable inhaler in a fraction of the time required to deliver the same drug via nebulization is expected to improve quality of life and compliance for cystic fibrosis patients.(64–66)
What remains to be done?
The Entrenched Player's Dilemma is the choice faced by existing businesses in a changing marketplace. According to Tapscott:(68) “The commercial success of their products in the marketplace increases their dependency on them. Making radical changes in the product's capabilities could cannibalize sales or lead to costly realignments of strategy and business infrastructure. The result is that entrenched players are generally not motivated to develop or deploy disruptive technologies.” This in part helps to explain why engineered particles have yet to be commercialized in the asthma/COPD space. Many have questioned whether the improvements in delivery efficiency noted will result in a measurable clinical benefit. To put it another way, is the change really needed?
As such, penetration into the asthma/COPD market may require that engineered particles help to drive improvements in patient compliance, in addition to their demonstrated improvements in lung targeting. Recent marketing studies(69) have categorized the drivers for poor patient compliance with inhaled asthma therapeutics into three buckets: (1) complex treatment regimes, (2) treatment costs, and (3) poor inhaler technique. The burden associated with complex treatment regimes can be decreased by molecule engineering (development of once daily therapeutics) and formulation engineering (formulation of fixed dose combinations of multiple therapeutics). Poor inhaler technique can be improved through advances in device engineering. What may not be fully appreciated is the impact that particle engineering can have on improving compliance resulting from poor inhaler technique.
Improvements in dose consistency can be achieved with porous particles in three principal areas: (1) reductions in the variability associated with oropharyngeal filtering; (2) lung deposition, which is largely independent of the patients breathing profile; (3) reductions in the variability associated with coformulation of two or more therapeutics as ordered mixtures.
As intimated, porous particles enable lung doses of 40–70% of the nominal dose to be readily achieved. Recent retrospective analysis of lung deposition studies by Taylor(69a) and Börgstrom and Olsson(70) have demonstrated that effectively “bypassing” deposition in the oropharynx leads to significant reductions in interpatient variability (Fig. 1). Increases in lung deposition from the 10–30% typically observed with micronized drug blends, to 40–70% for porous particles, decreases the mean RSD from 30–50% to 10–20%.(70) Similar reductions in interpatient variability with increasing lung delivery can be achieved with other delivery platforms including solution inhalers or “soft mist inhalers.”(70a)
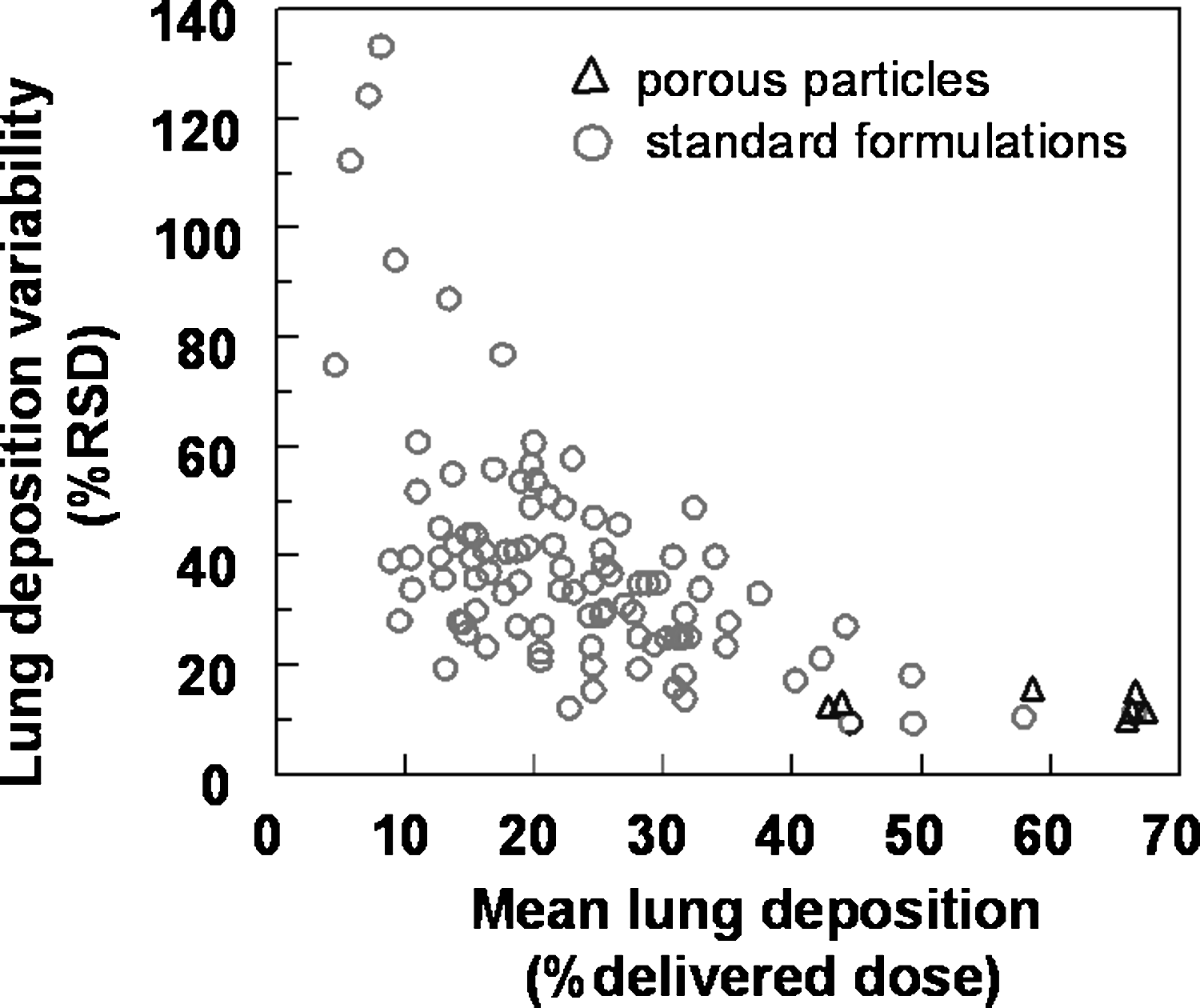
Plot of the interpatient variability in lung deposition, expressed as the relative standard deviation in lung deposition data versus mean lung deposition, expressed as the percentage of the delivered dose. Data for porous particles are pictured as open triangles. Adapted from Börgstrom et al.(70)
The ability of porous particles to fluidize and disperse at low dispersion energies in passive DPIs enables lung deposition which is independent of PIF. Figure 2 presents a summary of multiple pharmacoscintigraphy for porous particles delivered with passive, capsule-based inhalers.(18–20) Plotted is the deviation from mean lung deposition versus the pressure drop in the inhaler. This encompasses pressure drops ranging from around 1 to 10 kPa. To put the range of pressure drops in perspective, Figure 2 also displays the ranges of pressure drops (mean to minimum values) achieved by COPD patients with multiple devices, across a range of age and severity of disease.(71–73) Interpatient variability, expressed as the relative standard deviation from the mean total lung deposition value in each study was just 12%. The clinical data is so tight that it nearly passes USP guidelines for in vitro delivered dose uniformity. The results suggest that unless there is gross misuse of the device, COPD patients will achieve a consistent dose of drug in the lungs, independent of their PIF through the device.

Plot of the % deviation from mean lung deposition versus inhaler pressure drop for porous particles in various gamma scintigraphy studies. Due to differences in device resistance across the multiple studies, we have chosen to express the differences in peak inspiratory flow rate as a pressure drop. Flow rate independence is observed across a range of pressure drops encountered for a number of devices in COPD patients.(71–73) The range of pressure drops are presented as the mean and lower end of the range. The dashed lines represent ±35% of the mean values.
One perceived need for asthma/COPD therapeutics is to more effectively target the airways (i.e., the region with the highest receptor and smooth muscle concentration), while limiting deposition at the alveolar level. Alveolar deposition does not lead to effective bronchodilation or anti-inflammatory action, but does potentially contribute to systemic absorption and unwanted side effects. Achieving regional targeting in the lungs to enhance airway deposition has proven challenging, as differences in lung morphology and extent of lung disease between patients may have a greater influence on regional deposition than do formulation factors.(74)
Porous particles may enable a novel strategy for selectively targeting the conducting airways, challenging our preconceptions of what an ideal particle size distribution for treating asthma/COPD should be. The majority of lung deposition models have been developed to predict deposition from continuous aerosols, that is, respiration from the environment, rather than the bolus aerosols typically delivered from therapeutic inhalers during a single inhalation followed by a breathhold. Modification of the ICRP model(75) to account for these factors indicates that maximum lung deposition should occur for an aerodynamic diameter, da, of approximately 1 μm (Fig. 3a). At this size, nearly 90% of the aerosol is expected to be deposited in the alveoli. As discussed, fine particles approaching 1 μm have strong interparticle cohesive forces, leading to incomplete powder dispersion, and variations in aerosol performance with a patient's inhalation profile. In contrast, for da = 5 μm, the ICRP-Bolus model predicts that approximately 30% of the aerosol will be deposited in the conducting airways, and about 50% in the alveoli. A similar deposition of 30% in the conducting airways can be achieved for a particle with da = 10 μm, but with just 10% alveolar deposition.

Predicted aerosol deposition patterns for bolus aerosols. (
Interparticle cohesive forces depend critically on the geometric size of the particles. Van der Waals forces tend to scale with the diameter of the particles, whereas drag and lift forces responsible for powder fluidization and dispersion scale with the square of the particle diameter. A preferred strategy for achieving da = 10-μm particles may be to manufacture large porous particles with a geometric diameter, dg, of 40 μm and a particle density, ρ p , of about 0.1 g/cm3. At these geometric sizes, the drag and lift forces are expected to exceed the interparticle cohesive forces resulting in powders that effectively fluidize and disperse to primary particles with a simple, passive dry powder inhaler. In this limit, da = dg (ρ p )1/2. The predictions of the ICRP-Bolus model for a 40-μm particle as a function of particle density are captured in Figure 3b. At ρ p = 0.1 g/cm3, the model predicts ca. 20% total lung deposition, most of which is anticipated to occur in the conducting airways. The potential downside of the large porous particle approach is that a large fraction of the particles will be deposited in the oropharynx, with its potential to cause local side effects. This would be expected to be comparable to current marketed products. As well, the high variability in oropharyngeal and lung morphology from patient to patient noted above may lead to variability in the total lung dose and regional targeting.
In summary, porous particles enable improvements in lung targeting and dosing consistency. It remains to be seen whether the improvements in aerosol delivery will translate into corresponding improvements in clinical outcomes. In essence, it is the clinical work to establish this link which remains to be done. To realize the potential of porous particles in asthma/COPD, it is likely that an Entrenched Player will have to take the risk and make this investment.
Engineering Particles for Fixed Dose Combinations
The resounding success achieved with Advair®/Seretide® (GlaxoSmithKline, United Kingdom) has sparked significant activity in the development of combination products for asthma/COPD.(76–84) Combination therapies are here to stay. Some are even talking about triple therapies, and we are sure they will come.(76–77) The benefit to patients is clear—one inhaler containing all their respiratory medicines. This has translated into measurable improvements in patient compliance. Patients utilizing Advair refill prescriptions more often than do patients using separate inhalers, suggesting improved compliance.(78) They also use less short-acting beta-agonists,(78) suggesting better control of their disease. Beyond the compliance benefit afforded by a single inhaler, the combination therapy also shows reductions in mortality in COPD patients compared with monotherapies.(81) It has been proposed that there may be a benefit related to administering both therapeutic agents simultaneously to the lungs, because they have complementary modes of action and target different aspects of the underlying disease pathophysiology.(83) In vitro studies suggest that there may be synergistic interactions between the two classes of compounds at the receptor, molecular, and cellular level.(79–83) For Advair, the synergistic action of fluticasone and salmeterol is believed to occur only when both drugs reach the target cells simultaneously at their required concentrations. There may also be an added safety benefit to delivering combinations of fluticasone and salmeterol versus salmeterol alone in asthma patients.
Given the tight, and ever tightening regulatory standards that we need to meet, we need to find innovative solutions for formulating a mixture of drugs other than simply blending them together with the attendant issues around homogeneous and reproducible delivery of each drug—and this is particularly acute when the drugs have vastly different potencies. Achieving dose content uniformity in a blend of two actives and carrier particles can be challenging.(84–88) Observed issues include: segregation, poor stability, variable dosing, and under- and overdosing.(84)
Similarly, in suspension pMDIs differences in the particle properties may cause differential suspension characteristics of the APIs and wall losses to the canister, resulting in more variable product performance.(89–93) Wall losses can be potentially minimized by coating of the canister wall. Although disparities in the formulations have been dealt with by separating them in two canisters in the patent literature,(94,95) this would make the pMDI more bulky and potentially require more effort to actuate. It is possible to have a solution formulation if all the APIs are soluble and chemically stable in the propellant, or to have one drug dissolved while another drug is suspended in the propellant.
Particle engineering may be able to provide alternative options for designing combination products, where colocalization of the two therapeutic agents at the target cells is guaranteed by engineering particles where both actives are present in the same particle.(58,96–107)
Early returns on this approach are promising, although significant work remains. Particle engineering approaches can be subdivided into three classes: formulation of cocrystals,(96,97) particles prepared from controlled crystallization techniques,(58,98–100) and coprecipitates prepared by techniques such as spray drying.(101–107) Results of some recently reported studies are summarized in Table 1. Scanning electron microscopic images of some of the engineered particles are presented in Figure 4.
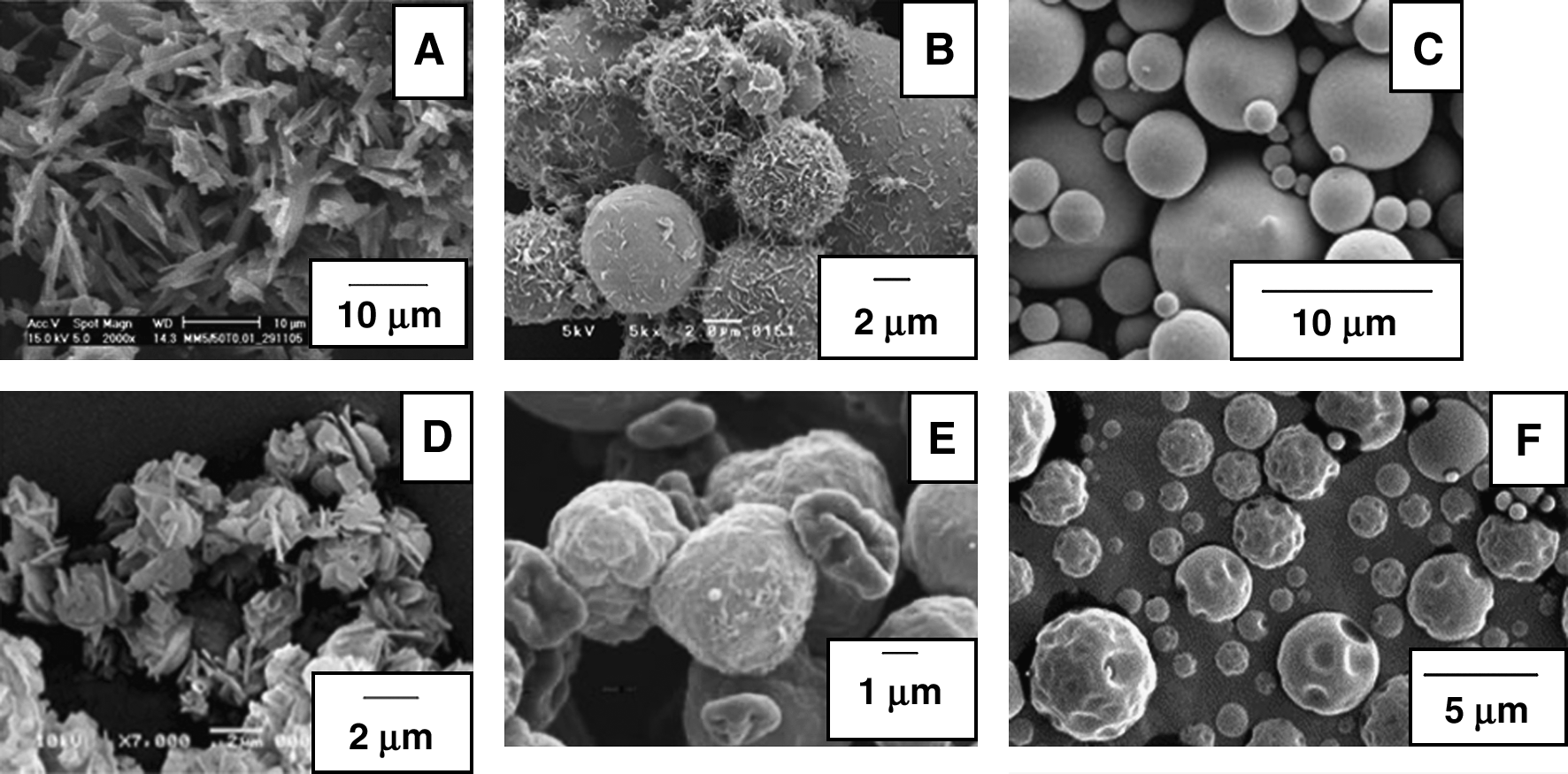
Scanning electron microscopic images of engineered particles comprising fixed dose combinations of therapeutics. (
SS, salbutamol sulfate; IB, ipratropium bromide; TS, terbutaline sulfate; BDP, beclomethasone dipropionate; FP, fluticasone propionate; SX, salmeterol xinafoate; CIP, ciprofloxacin hydrochloride; DOX, doxycycline hydrochloride; CEF, ceftazidime; BUD, budesonide; FF, formoterol fumarate; DNase, Dornase alfa; SAX, solution atomization xrystallization; AFR, aerosol flow reactor; SD, spray drying; C, crystal; A, amorphous; FPD, fine particle dose; FD, freeze drying; PAC, paclitaxel; CISP, cisplatin.
Cocrystals comprising both APIs in a single-crystal lattice would be ideal but difficult to obtain, as intermolecular forces dictate crystal packing and the formation of cocrystals. Cocrystal formulations comprising salbutamol sulfate and iprotropium bromide were studied by Jin et al.(96) Evidence for cocrystal formation included: a single columnar crystal habit, a unique X-ray powder diffraction pattern compared to the two pure drugs and their physical mixture, and unique thermal transitions in hot-stage microscopy and differential scanning microscopy. The cocrystals were subsequently micronized and blended with coarse lactose carrier particles and delivered using the active Spiros dry powder inhaler at a flow rate of 60 L/min. The mean MMAD values for salbutamol and ipratropium were 3.5 and 3.7 μm, respectively. As would be expected, no significant differences in the FPD<5μm (43 vs. 38% of the delivered dose) was noted for the two drugs. It is not certain that a cocrystal was in fact achieved, as definitive X-ray diffraction characterization of the crystal was not reported. Although differences in the X-ray powder diffraction pattern were observed for the drug combination, this could simply be the result of the formation of an alternative polymorph during the coprocessing.
Alternative controlled crystallization processes studied include Solution Atomization and Xrystallization, SAX™,(58) crystallization in an aerosol flow reactor,(98) and conventional freeze drying.(99) Drugs crystallized using the SAX technique in the absence of excipients exhibit poor aerosol delivery with an emitted dose of just 46% and a FPD<3.6μm of 5 %.(58) It is likely that aerosol performance could be significantly improved by inclusion of an excipient to reduce interparticle cohesive forces. In this regard, freeze-dried particles comprising combinations of chemotherapeutics and leucine exhibit significantly improved aerosol performance.(99) Westmeier et al.(100) also delivered modest performance for their formulations comprising crystals of fluticasone and salmeterol, comparable to that achieved in Advair (FPD5.0μm = 22%). What was clearly demonstrated in each case, however, was that the aerosol performance was comparable for the two drugs in the formulation (i.e., the FPD was within 15% for the two drugs).
Coprecipitation may be an alternative if the APIs distribute uniformly in the precipitate. Coprecipitation and drying can be achieved in a single step by cospray drying the APIs (in solution, suspension, or combination).(101–107,107a) A bulking agent can be used in the coprecipitation process to avoid the use of blend technologies for low dose drugs. A prerequisite for coprecipitates is no segregation or other physical changes of the drugs in the formulation, but these data are missing in the public domain. The aerosol performance for several spray-dried formulations is captured in Table 1. When APIs are dissolved and then precipitated in a single particle they are typically present as an amorphous solid. Consistent with the data on crystal mixtures above, aerosol performance is comparable to current lactose blends, unless a suitable excipient (e.g., leucine, crystalline mannitol) is included in the formulation. As would be expected, the engineered particles exhibited effective incorporation of the two actives into a single particle, with comparable aerosol performance for the two actives.
What remains to be done?
The use of separate formulations and dose containers is a possible strategy to simplify the future development process of combination products.(108) However, a particle engineering solution that provides a single engineered particle comprising both drugs, with the required physical and chemical stability is desirable.
Most of the engineered particles comprising fixed dose combinations described herein exhibit aerosol performance similar to current micronized drug blends. In order to realize the full potential of these formulations it is desirable to improve lung targeting and dose consistency (as intimated in the previous section), by judicious control of the particle morphology and/or surface composition. The different actives to be formulated in a single particle may have vastly different physicochemical properties (e.g., solubilities, pH requirements, etc.). The formulation conditions that maximize stability for one drug may adversely impact stability of the other. The studies reported to date have not addressed the potentially significant physical and chemical stability issues, which may result from incorporating both actives in the same particle. In addition, issues such as scale-up and regulatory acceptance of the new particle engineering technologies remain to be addressed. Combination products also present significant challenges from an analytical perspective.(84) Analytical methods previously developed for the monotherapies may not be suitable for the combination products. More complex methods [e.g., liquid chromatography/mass spectrometry (LC-MS)] may be required. The ability to selectively target the different actives in a fixed-dose combination to different regional sites within the lungs based on their receptor locations represents another challenge requiring attention.
Controlled and Targeted Delivery of Drugs to the Lungs
There have been no controlled release formulations approved for pulmonary delivery. Providing controlled release could allow twice daily drugs to be delivered once daily, and this could contribute to better patient compliance, better control over asthma and COPD, and a step change in exacerbations and morbidity—a real benefit to the patient. Development of controlled release formulations for the lungs is complicated by the multiple clearance pathways (e.g., mucociliary clearance, macrophages clearance, systemic absorption, cough clearance), and the safety and slow clearance of retentive excipients (e.g., polymers).
Schanker and colleagues(109,110) studied the pulmonary absorption properties of a large number of therapeutics. Hydrophilic small molecules with an octanol/water partition coefficient, Pow, less than 0 had a mean lung residence time of about 1 h, whereas lipophilic small molecules (Pow > 0) had a mean lung residence time of about 1 min (Fig. 5). The differences in lung residence time with log Pow reflect differences in the pathway of absorption: whereas lipophilic therapeutics are absorbed via transcellular pathways, hydrophilic therapeutics are absorbed paracellularly. Only when the molecular weight rises above ca. 1000 g/mol are significant increases in lung residence time noted.

Plot of the absorption half-life as a function of the octanol–water partition coefficient for small molecules (mol wt <1000 g/mol). Plot is a compilation of data collected by Schanker and coworkers.(109) Adapted from Patton et al.(110)
In the asthma/COPD space, formulations comprising the short-acting β-agonist salbutamol were originally administered four times daily. Pharma companies chose to go the route of molecule engineering, developing long-acting β2-adrenergic agonists (LABA) to reduce dosing frequency and improve patient compliance. If one follows the evolution of β2-adrenergic agonists, there has been a steady progression toward once daily therapeutics, from albuterol to twice daily formoterol and salmeterol, to once daily indacaterol. The benefit of molecule engineering is clear. Molecule-based patents provide the best form of intellectual property and long-term exclusivity. It is much more difficult to circumvent a molecule patent than it is to work around a formulation or process patent.
It is far more likely that controlled release formulations will be developed for marketed therapeutics with a longstanding history of safety and efficacy, which are being repurposed for pulmonary indications. This is the case for anti-infectives and chemotherapeutics. The case is particularly compelling for treating lung infections, as strong links between the pharmacokinetics of the drug and the resulting pharmacodynamic response have been noted.(111,112)
Inhaled ciprofloxacin hydrochloride (log Pow = 0.28) is rapidly absorbed into the systemic circulation with peak serum levels observed within a few minutes postinhalation.(113) Two controlled release formulations are currently in clinical development for the treatment of chronic Pseudomonas aeruginosa (Pa) infections in cystic fibrosis patients.(114–116) The most advanced formulation strategies for pulmonary controlled release have involved excipients that are endogenous to the lungs such as phospholipids in the form of liposomes,(117) or salts that are naturally occurring in the lungs, which offer favorably slow dissolution rates.(118) Other excipients have frequently been employed, such as a variety of polymers, but these have yet to appear in products in clinical development.(119) Formulation of ciprofloxacin as the insoluble betaine salt at neutral pH dramatically increases the lung residence time, with resultant decreases in colony forming unit (CFU) counts in vivo.(114) Ciprofloxacin betaine has been formulated as a micronized drug coated with a porous layer of phospholipid using an emulsion-based spray-drying process.(115) The dry powder is administered to patients with a portable, passive inhaler. Alternatively, the hydrochloride salt of ciprofloxacin has been encapsulated in liposomes and administered with a jet nebulizer.(116) Studies have demonstrated the maintenance of liposome integrity following nebulization, a reduction in Pa colony forming units in cystic fibrosis and bronchiectasis patients, and extended systemic absorption profiles consistent with once-daily administration.(119a,119b) Liposomes may also be able to penetrate into Pa biofilms, with virulence factors in the biofilm (e.g., rhamnolipids) facilitating targeted release of drug within the biofilm.(119c) In addition to potential improvements in efficacy, the controlled release formulations of ciprofloxacin may help to improve patient compliance, by reducing the burden of treatment. Liposomal formulations of the aminoglycoside, amikacin,(120) and the chemotherapeutics cisplatin,(121) and 9-nitrocamptothecin,(122) are also in clinical development. The development of formulation strategies for liposomal dry powders continues to be advanced.(123)
A variety of formulation strategies have been explored for the controlled delivery of rifampicin and capreomycin in the treatment of tuberculosis infections.(32,33,124,125) Perhaps the most intriguing are polylactide-co-glycolide (PLGA) nanoparticles.(124) Formulations comprising nanoparticles have many potential benefits, including enhanced dissolution properties for poorly soluble drugs, and the potential for intracellular targeting, translocation of drug-loaded particles into the systemic circulation, and pulmonary controlled release.(126–128) Owing to their small size and strong interparticle cohesive forces, nanoparticles pose significant formulation and delivery challenges. One approach to circumventing these issues has been to spray dry the dispersed PLGA nanoparticles to form a larger microparticle (Fig. 6).(124) The low-density porous particle may be effectively delivered to the pulmonary epithelium without significant losses via exhalation. The nanoparticles are subsequently released in lung lining fluid. For the rifampicin nanoparticles, significant increases in lung residence time were observed.(124) In a recent review, Muttil et al.(129) suggest that: “Aerosol delivery (of controlled release TB therapeutics) to the lungs as an adjunct to conventional therapy has the potential to decrease the dosing frequency and duration of therapy. This may ultimately lead to less severe side effects, improved patient compliance, and reduced emergence of drug-resistant strains of tuberculosis.”(129)

Scanning electron micrographs of spray-dried porous particles comprising rifampicin nanoparticles. A magnification of the surface of the PNAP indicates a shell of aggregated nanoparticles with structure intact. Photomicrographs courtesy of Jean Sung and David Edwards.
What remains to be done?
The limitations on progress with respect to controlled or targeted delivery are not related to the physicochemical properties of the particles or to the ability to deliver these particles to the pulmonary epithelium. More importantly, information is required on the nature of lung disease and biology to allow appropriate drug delivery systems to be developed. In this regard, regional differences in lung transport rates (absorption, mucociliary, cell mediated) and mechanism (phagocytosis, receptor-mediated endocytosis, transcytosis, paracellular) for specific agents is required.(130) Clear objectives should be adopted to address specific questions, such as, what is the: (1) site for absorption to the systemic circulation? (2) rationale for duration of action of locally acting agents? (3) defined location of target (receptor, cell, tumor?).
In preclinical testing, we are limited to a variety of healthy (pharmacokinetic), and diseased (pharmacodynamic, efficacy) animal models.(131–135) The value of these models lies not in their physiological or anatomical similarity to humans, but in their ability to predict the behavior of therapeutic agents in humans. In this respect, much has been done to develop allometric scaling of dose, for example, from one species to another in addition to establishing the relevance of the pathogenesis of disease in humans.(134,135) Improved methods of following the disposition of drugs are required at the scale of scrutiny that would allow the questions in the foregoing paragraph to be answered clearly. Of note in this regard is the use of cell culture models.(136–138) However, a balance will be required between considering the limitations of: (1) animal models based on specific differences in anatomy and physiology, and; (2) cell and tissue culture models based on biophysical and biochemical differences with respect to the functional cells in a whole organism (Fig. 7).

In vitro and in vivo methods for following the disposition of drugs in the lungs are critical for the development of formulations for controlled and targeted delivery.
In addition to the standard clearance pathways found in the lungs, some therapeutics (e.g., nucleic acids) must also overcome cellular barriers, including cellular uptake, endosomal release, nuclear localization, nuclear uptake, and gene transcription.(139,140) Effective delivery of nucleic acids remains a significant challenge, and it is likely that revolutionary innovation will be required to eventually achieve success. Perhaps targeted nanoparticles will drive this innovation.
Delivery of Macromolecules via Inhalation
The development of Exubera® (recombinant human insulin for inhalation, Pfizer, New York, NY) has played a large role in shaping our perceptions with respect to inhaled macromolecule delivery. Exubera also presents an interesting case study in market dynamics. The lack of market success cannot be traced to a single cause; in fact, there were a number of diverse issues that contributed to its poor market showing. What is clear is that the needs of the diverse and complicated set of customers (i.e., patients, healthcare professionals, Health Authorities, and payers) were not fully satisfied. To better understand some of the reasons why Exubera failed and “what needs to be done” to move forward with future development of inhaled macromolecules, it is instructive to trace the history of insulin delivery.(141)
In his pioneering studies, Banting extracted insulin from the pancreas of animals and injected it to patients suffering from diabetes with miraculous results.(142) In need of help in commercializing his discovery, he turned to Eli Lilly and Company, who immediately began production of bovine and porcine insulins. The early forms of the drug had high levels of proinsulin, leading to side effects. As well, a small fraction of patients developed neutralizing antibodies to the foreign protein. Lilly focused on reducing levels of proinsulin, decreasing it from 5% in 1921 to 1% in 1970 to 0.01% in 1980.(141) Lilly's continued desire to improve protein purity led them to collaborate with Genentech on a revolutionary innovation, that is, the development of recombinant human insulin (Humulin). Humulin was marketed at a premium to animal-derived insulins. Despite the fact that Lilly's market research with endocrinologists suggested that Humulin would be disruptive, the actual market response was tepid at best.(141) Lilly researcher Bruce Frank conceded that: “In retrospect, the market was not all that dissatisfied with highly purified pork insulin.”(141)
Although recombinant human insulin eventually replaced animal-derived insulin, it had little impact in shaping the insulin market. Once Novo-Nordisk and Hoechst developed their own forms of recombinant human insulin of comparable efficacy and purity, the drug was viewed as a commodity.(141)
Disruptive innovation in insulin therapy was driven by improvements in the “convenience” of delivery. The need for injections with all their pain, discomfort, and social stigma was central to the advancement. Whereas Lilly struggled to achieve premium pricing with Humulin, Novo had no problem with achieving a 30% premium for their novel pen injectors.(141) The needles in the pens were shorter, sharper, and silicone tipped. Dosing was less cumbersome, obtrusive, and painful. Patients utilizing the pens were more inclined to take multiple shots daily, thereby enabling Novo to increase their share of insulin sales.(141)
Sustaining technologies tend to maintain a rate of performance improvement. That is, they give customers improvements in the attributes they already value. For example, Lilly's steady move to increase insulin purity was incremental in nature. Eventually, their attempts to sell highly purified recombinant human insulin at a premium price “overshot” the market. In contrast, disruptive technologies, such as the pen injectors, introduced a new set of features into the marketplace than what customers had traditionally valued. The pen injectors were initially introduced in Europe in 1985. It is worth noting that when the pens were introduced, many endocrinologists referred to them as “expensive toys.”(143) It would be more than a decade before they would make a serious splash in the U.S. market.
Although pens were moving toward market acceptance, there came a significant push to find noninvasive routes for delivery of macromolecules. The pulmonary route of administration was considered the best alternative, as proteins are naturally absorbed into the systemic circulation without the need for penetration enhancers.(144,145) Exubera completed Phase 2b clinical trials in 1998. Due to concerns regarding the long-term safety of inhaled insulin, Exubera would not be approved until 2006. Over that time, pen injectors became more entrenched, the types of injectable insulins continued to evolve (e.g., short-acting for meal-time and long-acting for overnight control of blood glucose), and the role that payers (both public and private) play also changed. Did Exubera simply miss its window to be disruptive, or did the product overshoot the market needs? Disruptive technologies often take several years to achieve significant market success, and market penetration in the diabetes space is often slow. Lantus (insulin glargine) languished for several years with modest sales before blossoming into a multibillion dollar blockbuster. Did Pfizer pull the plug on Exubera too quickly?
Advocates of Exubera were hopeful that the drug would help to improve patient compliance with insulin therapy and encourage them to begin insulin treatment earlier in the life cycle of their disease. Indeed, multiple studies explored the barriers to insulin injections, with the following published statistics: more than 70% of patients are reluctant to start injectable insulin, with 21–56% of Type 2 patients refusing to start.(142–144) At least 10% of patients are “needle-phobic.”(146–148) The fear of needles is likely under reported, as the medical profession self-selects for patients who are needle “fearless.” Pfizer conducted two additional studies evaluating nearly 7000 patient records, and found that patients often delay initiating insulin injections (by up to 4 years) due to fear of, and/or discomfort caused by multiple injections.(149) These delays may result in an increased risk of developing severe and costly health complications. Consistent with these published studies was a controlled marketing trial which studied the preference of Type 2 patients for various insulin therapies. The patients in the study were failing to achieve target glycemic control through diet and/or oral therapy with hypoglycemic agents. A synopsis of the results of the study was provided by Zenios et al.(150)
“In this study, one group of patients was given written information about existing treatment options (oral hypoglycaemic agents and subcutaneous insulin), whereas the second received the same information plus details of the risks and benefits of inhaled insulin. Individuals in both groups were then asked to make choices about their future diabetes therapy. When the choices of therapy included inhaled insulin, 43% chose to start insulin (with 35% electing to take inhaled insulin). In the group where inhaled insulin was not given as an option, however, only 15.5% opted to begin taking subcutaneous insulin.
These results, coupled with positive quality of life data for inhaled insulin during clinical development, led many to believe that there was a significant potential market. Some physicians countered that: “the imagined horrors of insulin injection greatly outstrip the reality, and most patients will make a smooth transition to insulin with the help of sympathetic counseling and support.”(151) Heinemann pointed out that the psychological barrier is not just the result of needle phobia, but a fear of the other aspects of insulin therapy, including weight gain and risk of hypoglycemic events.(143) If patients were so positive about the prospects of inhaled insulin, why did it do so poorly in the marketplace?
The answer to this question likely hinges on three key points. First, clinical trials conducted with Exubera did not demonstrate a clear medical need for inhaled insulin. Second, the product was priced at a premium to other forms of insulin, including pens. Third, the long-term safety of inhaled insulin was unknown. These issues led to a clear dilemma: why should physicians prescribe and payers reimburse at a premium for a drug product that has failed to demonstrate a clear medical benefit, and where there is an increased risk of long-term adverse events?
In addition to these issues there was the matter that Exubera was less convenient to use relative to current injectable insulins. Hence, by the time Exubera received approval in 2006, the product had clearly overshot the evolving marketplace, and some even questioned whether the product was “innovative” at all.(143) We will return to this question later, but let's first examine the “product-based” barriers to adoption of Exubera in more detail.
The safety concerns were primarily associated with decreases in lung function, increases in antibody formation, and the potential for the development or potentiation of lung cancer.
Exubera produced a small but statistically significant drop in lung function (FEV1 and DLCO).(152) The effects were fully reversible and nonprogressive. In fact, patients inhaling Exubera for 7–8 years actually had smaller drops in FEV1 (47 mL/year, n = 54), than did control patients with Type 2 diabetes (71 mL/year, n = 125).(153,154) A vehicle-controlled Phase 4 study with Exubera, demonstrated that the decrease in lung function also occurred with the vehicle.(155) Hence, the effect is likely due to the excipients and not the drug substance. A similar decrease in lung function was noted by Lilly/Alkermes.(156) With that said, most physicians would agree that the small initial drop in lung function (ca. 40 mL in FEV1) observed is of no clinical significance.(143) Nonetheless, patients taking Exubera were required to receive biannual lung function tests, a test that many endocrinologists were not equipped to perform.
Exubera also promotes greater antibody formation than injectable insulin. The type of antibodies formed (i.e., IgG) are the same for both injectable and inhaled insulin. The antibodies are not neutralizing, and have no impact on dose, glycemic control, or rates of hypoglycemia over time.(157)
A higher percentage of patients taking Exubera (6 cases in 4740 patients, 0.13%) were diagnosed with lung cancer, compared to the control group taking subcutaneous insulin (1 case in 4292 patients, 0.02%).(158) All of the patients in whom malignancies were observed in the Exubera group had a history of smoking. Two of the six cases were preexisting. In a large retrospective study, Govindararajan et al.(159) studied the incidence of lung cancer in patients with diabetes. Data for 87,678 individuals in the Veteran's Integrated Services Network 16 database were assessed. A total of 1371 individuals or 1.6% developed lung cancer.(159) The level of malignancies observed in both the Exubera control and treated groups alike and were significantly lower than that reported by Govindararajan et al.(159) The risk of developing lung cancer as a result of inhaling insulin may be small or nonexistent, but because insulin has trophic effects, it cannot be fully excluded. Additional Phase 4 studies exploring inflammation in the lungs following inhalation of Exubera over a 3-month period, found no evidence of cellular or protein infiltration compared to injectable insulin.(160) In a related study, Papagianni et al.(161) demonstrated that inhaled insulin does not trigger lung inflammation and airway remodeling.
Overall, data for Exubera (including Phase 4 safety studies), and additional data generated on other inhaled insulin products in development continue to suggest that delivering insulin via the pulmonary route is safe.(162) With that said, unless a clear medical benefit for inhaled insulin can be established clinically, physicians and payers will likely continue to believe that even a small safety risk is unwarranted.
Concerns regarding convenience of Exubera center around: (1) the bulky, cumbersome inhaler, which is not intuitive to use, and far from discrete to use in a public place; (2) the confusing use of milligrams to define the dose versus conventional units; (3) the lack of dose proportionality (3 × 1 mg ≠ 1 × 3 mg); (4) difficulties associated with dose titration, and (5) the long administration time required (i.e., several blisters to be inhaled) when a large number of units are needed. All of these product-based issues are likely solvable in future generation products. Many were, in fact, addressed in other inhaled insulin products in development.
The high cost of Exubera was driven to a large extent by the low systemic bioavailability of the drug substance. The delivery efficiency for insulin to the systemic circulation accounting for manufacturing losses, losses in the device, losses in the oropharynx, and enzymatic degradation was just 6–7%. In addition, manufacturing costs for the powder, device, and packaging all contributed to the need for a high price for the product.
The good news is that Exubera and other inhaled insulin products helped to drive significant innovation in the inhalation field. These innovations are fueling new applications, in the delivery of alternative peptides and anti-infectives.(61,67)
Innovations achieved with Exubera included: (1) the first marketed room-temperature stable formulation of insulin; (2) the first inhaled drug product comprising an amorphous solid; (3) the first inhaled drug product prepared by a spray-drying process; (4) the development of novel drum-filling equipment designed to fill 1 mg of a poorly flowable engineered powder with a relative standard deviation of <3%; (5) foil–foil blister and heat-sealing technologies that protect the amorphous solid from the deleterious effects of moisture; (6) the first active dry powder inhaler, which decouples the aerosolization event from the patient's inspiratory effort.(26) Significant innovations in insulin delivery also occurred outside of Exubera.
For example, Alkermes advanced low density, porous particles with larger geometric sizes. (16,163,164) Due to decreased interparticle cohesive forces, these powders enabled simpler, less expensive, portable dry powder inhalers to be utilized. A new class of solution inhalation systems was developed, including the AERx® System (Aradigm), with its nearly monodisperse particle size distribution and breath control features practically eliminating deposition in the oropharyngeal region, and thus resulting in intrasubject variability equivalent or superior to subcutaneous insulin.(165,166) The AERx device has the capability of delivering up to 10 units of insulin per puff, with the added benefit of being able to dial in any dose between 2 and 10 units. Kos(167) developed a pressurized metered dose inhaler platform comprising semicrystalline insulin dispersed in HFA-134a. They were able to deliver >1 mg to the lungs in a single inhalation with their proprietary slow-spray actuator.
To be frank, the failure of Exubera represents a significant blow to the field of inhaled macromolecules, but it is by no means a death knell. The industry must learn from its mistakes, take stock of the changing marketplace, and develop new drug products that more effectively match patient need with economic reality. Exubera was priced at a slight premium over injectable insulins (11.8% over 5 × 3 mL Lantus®, 8.6% over 5 × 3 mL Novolog®). Hence, the improvements needed to make inhaled insulin price competitive are within reach.
Although about 40% of the insulin loaded into the Exubera device was delivered into the deep lung, only one out of every four protein molecules reached the systemic circulation. It is presumed that much of the protein is lost to enzymatic degradation in the lungs. Hence, it is desirable to find innovations that increase the efficiency of protein delivery to the deep lung, and perhaps more importantly, safely increase its bioavailability. After all of these years, the mechanism of systemic uptake of proteins remains unclear. The fact that significant questions remain regarding the biology of macromolecule absorption, suggests that significant opportunity also remains for dramatically improving the uptake of proteins into the systemic circulation.
Several strategies have been explored to increase the bioavailability of inhaled proteins. These include: (1) the addition of protease inhibitors which slow degradation of proteins in the lungs;(38) (2) the inclusion of excipients that “enhance” the systemic absorption of insulin;(34–37) (3) the use of active transporters, and(39–41) (4) PEGylation.(42)
The most advanced of these options is the use of excipients to enhance absorption. Many excipients can increase the bioavailability of peptides by up to sevenfold, and some appear to have no acute toxicity at low concentrations, but their safety and tolerability need to be verified in longer term studies. To this end, MannKind filed a new drug application in 2009 for approval of their Technosphere® insulin, which is comprised of monomeric insulin adsorbed onto crystals of fumaryldiketopiperazine (FDKP).(34–36) Technosphere insulin is rapidly absorbed into the systemic circulation (tmax = 15–20 min), with significant improvements in bioavailability (30–50%) relative to other forms of inhaled insulin.(34–36) Technosphere insulin may afford clinical improvements in weight gain, fasting, and postprandial glucose levels. It is hoped that the MannKind product will provide better coverage of prandial insulin requirements than current injectable insulins. Approval of Technosphere insulin would help to rejuvenate the pipeline of inhaled macromolecules, ushering in new formulations comprising novel excipients to facilitate systemic delivery. Improvements in bioavailability should enable Technosphere insulin to be priced competitively with current marketed injectable insulins.
Formulations are being developed which utilize immunoglobulin receptors in the airways to facilitate transcytosis of proteins. For example, Sacaan et al.(39) have developed a chimeric fusion protein consisting of a ligand that binds to the polymeric immunoglobulin receptor (pIgR) and a therapeutic protein. The high-capacity pIgR efficiently delivers IgA dimers (MW = 450,000 Daltons) and IgM pentamers (MW = 900,000 Daltons) from the basolateral to the apical surface of the lung epithelium. Bitonti et al.(40,41) have explored Fc fusion molecules that bind to, and are transported by, an antibody receptor, FcRn (the neonatal Fc receptor). Bioavailabilities of 20–50% have been achieved in preclinical models for erythropoietin, interferon-α, interferon-β, and follicle stimulating hormone with serum half-lives of >1 day. Proof-of-concept has been demonstrated in nonhuman primates with EPO–Fc conjugates.(41)
PEGylation of proteins provides a depot for controlled release in the lungs, while also protecting the protein from enzymatic degradation.(42) PEGylation results in nearly 100% bioavailability for the protein, albeit at a significant loss in activity.
It is clear that the Exubera device did not meet the market needs. For future products, the delivery system must be as convenient to use as the injectable insulin pens. The ideal device would be portable, inexpensive, and capable of delivering a dose in a matter of seconds. The device would enable discrete dosing, even in a crowded restaurant, and be intuitive to use with minimal teaching required. Dose titration is a plus, depending on the indication.
All of the first-generation inhaled insulin products utilized regular insulin and targeted the entire insulin market (i.e., broad indications in both Type 1 and Type 2 patients). As Heinemann points out,(143) inhaled insulin may benefit by focusing on segments of the insulin market where there is a clear unmet need. He provided two examples: (1) obese patients who have a slow onset of action due to slow systemic absorption of insulin following subcutaneous injection; (2) elderly Type 2 patients who require only a small fixed dose of insulin. In this regard, it is worth noting that AIR insulin demonstrated a significant improvement in HbA1c relative to intensive insulin glargine in Type 2 diabetics.(164) Due to the large number of diabetic patients, even a niche product can be a significant opportunity.
Pushing insulin therapy earlier in the treatment regimen should be a goal. Currently injectable insulin is fourth or fifth line, and it takes 11–12 years before treatment with insulin is initialized. Earlier treatment with inhaled insulin may help to preserve pancreatic function, while also providing improved glycemic control for Type 2 patients.(168) Of course, development of meal-time insulin products does not completely eliminate the need for injections. Basal insulin via the pulmonary route would eliminate the needle entirely.
Obviously, the development of inhaled insulin represents the highest bar in terms of safety for an inhaled product (i.e., using an otherwise healthy lung as a portal to deliver insulin multiple times daily for the rest of a person's life). The benefit/risk ratio for other inhaled proteins may be more advantageous. In this regard, pulmonary delivery of many other approved biologics has progressed into human clinical trials.
Despite the advances in injection technology, 13% of diagnosed growth hormone deficient children in a 2005 study missed more than half of their prescribed doses over a 2-year period.(168a) Inhaled growth hormone powder was found to be safe in a 6-month toxicology study in primates, and in human clinical testing for up to 28 days.(168b) In a pediatric trial, while inhaled insulin was well tolerated and produced comparable PK profiles to subcutaneous injection, the 3.5% bioavailability was half that reported in adults and is attributed to differences in deposition pattern.(168c) The low bioavailability and resulting higher COGs and large inhaled dose (up to tens of mg) for this product, together with the difficulty in providing dose titration in a convenient single inhalation, reduced the market attractiveness and led to the shelving of this product. An inhaled growth hormone product could fill a market need if the bioavailability can be increased and convenience issues addressed.
If development of inhaled insulin were not delayed and had led to rapid marketing success, systemic delivery via the pulmonary route of other biologic products would likely have gained support. Because this scenario did not occur, what may have been more appropriate inhaled protein/peptide products than insulin; that is, those with higher potency or bioavailability, wider therapeutic windows, or other advantages, were not developed. For example, although inhaled interferon alpha is only ∼10% bioavailable via inhalation, pharmacodynamic responses comparable to subcutaneous injection were observed.(168d) The potential lack of significant side effects for a once-daily inhaled IFN-α product could have provided a competitive safety and tolerability advantage over the marketed thrice weekly injections of IFN-α or once weekly injections of the pegylated IFN-α products.
Rat inhalation studies of oxyntomodulin and PYY, molecules with the potential to curb obesity, both show an improved pharmacodynamic response compared to i.v. infusion, while providing lower systemic exposure. It is not known if these results are due to the differing PK profiles, or some other novel attributes associated with the formulation or the pulmonary route.
Local delivery of proteins (e.g., antibodies, vaccines, proteins) to treat lung diseases acutely is seemingly a simpler target. The use of Pulmozyme® (inhaled DNase) to improve lung function in CF patients has been a market success story.(169)
Despite the fact that a large number of pathogens enter the body via the respiratory tract, there are no approved pulmonary vaccines. The inability of parenteral vaccines to induce mucosal immunity is considered by some to be a significant limitation. The efficacy and safety of inhaled measles vaccine has been established in more than four million children in Mexico.(170) These studies clearly demonstrated that inhaled administration of measles vaccine results in a more robust immune response, and improved protection relative to parenteral vaccine. Advances in our understanding of the “drying process” are facilitating the stabilization of live vaccines (e.g., measles) as dry powders.(171) Preclinical studies with nonreplicative influenza vaccines have also demonstrated the utility of inhaled vaccines to improve the immune response relative to parenteral or intranasal administration.(172–174) The bar for regulatory approval of new vaccine delivery systems is very high, and it remains difficult to get traction for inhaled vaccine delivery within Pharma and Health Authorities.
A number of other proteins for local effect are currently in clinical development including cyclosporine for prophylaxis against rejection in lung transplant patients,(175) and α1-antitrypsin in genetic emphysema.(176)
Unconventional strategies such as utilizing alveolar macrophages to take up nanopartticles and deliver proteins systemically are in their infancy. Improving our understanding of lung biology may also hold the key to effective delivery of oligonucleotides, including siRNA.(177,178) It is likely that revolutionary advances will be required to achieve success in this regard, as current delivery strategies do not effectively meet the requirements.
What remains to be done?
The clinical development of protein therapeutics (e.g., peptides, antibodies) continues to be a significant proportion of Pharma pipelines. We continue to believe that development of a noninvasive delivery system for macromolecules fills an unmet need. We further believe that the pulmonary route of delivery remains the method of administration with the highest likelihood of success. Making this a reality will require the development of products that meet all customer needs, including healthcare professionals, payers, and organizations like the National Institute for Health and Clinical Excellence (NICE). In particular, advances are needed in our understanding of the lung biology in order to facilitate: (1) improvements in systemic bioavailability of inhaled macromolecules, in order to make these products more cost competitive. This includes both passive and active forms of transport across the pulmonary epithelium; (2) the ability to effectively deliver the macromolecule into cells and control their delivery once inside the cell; (3) the ability to provide controlled release formulations of macromolecules. Beyond these formulation challenges, it is critical that the safety of the inhaled route for systemic delivery of macromolecules continue to be established, and that more convenient delivery systems be developed.
Conclusions
Once upon a time (and it was not that long ago), Pharma companies would design clinical programs to establish the safety and efficacy of their drug. Once approval was achieved with Health Authorities, the market success of the product was more or less guaranteed, especially if the drug was marketed by a company with significant marketing muscle.
At the level of the consumer, a patient with lung disease such as asthma would go to their physician, who would have a range of drugs to prescribe. Independent of the drug, the patient typically would pay a single defined prescription copay. Hence, there was no need for the physician or the patient to trade-off features in a product for reduced cost. As such, the market was not disruptible.(179) With the current focus on reducing healthcare costs, patients and payers must increasingly make trade-offs. Independent institutes now perform a critical review of the benefits of a product. Only if the outcome of the review is positive will reimbursement be granted. Even if approved, reimbursement may be on a tiered system, with significantly higher copays for higher priced products that are not well differentiated. Exubera is a prime example of a drug product that overshot the market needs. Payers, and ultimately patients, were not willing to pay the increased cost of Exubera to avoid the needle.
Pharma companies must now increasingly take into account these independent “consumer watchdogs” if they are to effectively market a new drug.(150) They may even need to run additional clinical trials to specifically meet their needs. At a minimum, the nature of clinical trials will be scrutinized to a higher degree with pharmacoeconomics in mind.
As we move forward with new formulation technologies we must be cognizant of whether the added features that we are incorporating in our inhaled drug products are truly needed from a patient point of view. Innovations which significantly improve the efficacy and safety of the drug product are clear, especially if they can be achieved at an acceptable cost. What about innovations that drive improvements in convenience, or difficult to measure benefits like compliance? Are these features going to overshoot the market? These questions are central to whether engineered particles will truly be impactful in respiratory products.
Advances in particle engineering are enabling more complex formulations with multiple functions to be designed. For example, controlling the drying rates and solubilities of excipients in a spray-drying process enables formation of core-shell particles.(25,45,46,69a) In this regard, it is possible to create a shell comprising a hydrophobic excipient (e.g., leucine or trileucine), encapsulating a core of an amorphous drug and glass stabilizing excipient.(25) If the amorphous drug is a protein, removing contact with the air/water interface is important in achieving the desired long-term stability.(25,171,69a) The hydrophobic shell provides good powder fluidization and dispersibility, enabling high delivery efficiencies to the deep lung. It is also possible to include “targeting” agents in the shell. For example, coformulation of an immune modifying agent with IgG enables effective targeting to pulmonary macrophages via the Fc-γ receptor.(180)
Feasibility has been demonstrated for engineering an ensemble of nanoparticles in a microparticle for effective delivery to the lungs.(52,124) By judicious choice of the size, charge, and excipient coating on the nanoparticle it may be possible to effectively target these particles into cells and facilitate trafficking to the appropriate organelle. Alternatively, coating nanoparticles with a layer of polyethylene glycol may enable penetration of the nanopaticle below airway mucus, thereby avoiding mucociliary clearance and providing a means of achieving controlled release in the airways.
Hence, one can envision, single particles comprising multiple actives that are delivered to the lungs with high efficiency, with the potential to effectively “target” specific cells, while also providing effective stabilization for labile drugs. As improvements in our understanding of lung biology continues, particle engineering will play a key role in marrying this knowledge with effective delivery system, and ultimately in providing highly differentiated drug products.
Footnotes
Author Disclosure Statement
No conflicts of interest exist for any of the authors with respect to the content of the review.