
Abstract
Abstract
In order to answer the question “what research remains to be done?” we review the current state of the art in pharmaceutical aerosol deposition modeling and explore possible in vivo– in vitro correlations (IVIVC) linking drug deposition in the human lung to predictions made using in vitro physical airway models and in silico computer models. The use of physical replicas of portions of the respiratory tract is considered, alongside the advantages and disadvantages of the different imaging methods used to obtain their dimensions. The use of airway replicas to determine drug deposition in vitro is discussed and compared with the predictions from different empirical curve fits to long-standing in vivo deposition data for monodisperse aerosols. The use of improved computational models and three-dimensional computational fluid dynamics (CFD) to predict aerosol deposition within the respiratory tract is examined. CFD's ability to predict both drug deposition from pharmaceutical aerosol sprays and powder behavior in dry powder inhalers is examined; both were highlighted as important areas for future research. Although the authors note the abilities of current in vitro and in silico methods to predict in vivo data, a number of limitations remain. These include our present inability to either image or replicate all but the most proximal airways in sufficient spatial and temporal detail to allow full capture of the fluid and aerosol mechanics in these regions. In addition, the highly complex microscale behavior of aerosols within inhalers and the respiratory tract places extreme computational demands on in silico methods. When the complexity of variations in respiratory tract geometry is associated with additional factors such as breathing pattern, age, disease state, postural position, and patient-device interaction are all considered, it is clear that further research is required before the prediction of all aspects of inhaled pharmaceutical aerosol deposition is possible.
Introduction
In the present article we provide a summary of the material presented by the authors during this session. We begin with what remains to be done regarding the use of 3D physical models and imaging. This is followed by thoughts on the future of mathematical deposition models while we close with an in-depth look at what remains to be done with computational fluid dynamics to enhance its role in improving IVIVCs. Although we have attempted to capture in prose the oral presentations of the authors, it should be appreciated that some distillation and simplification has been necessary. Despite this fact, the statements below do approximate those made by the authors in their oral presentations.
3D Physical Models and Imaging
Several speakers addressed the advances in the sophistication of methods that were now available to build more realistic physical models of the RT (Fig. 1); these could then be used for in vitro deposition determinations.
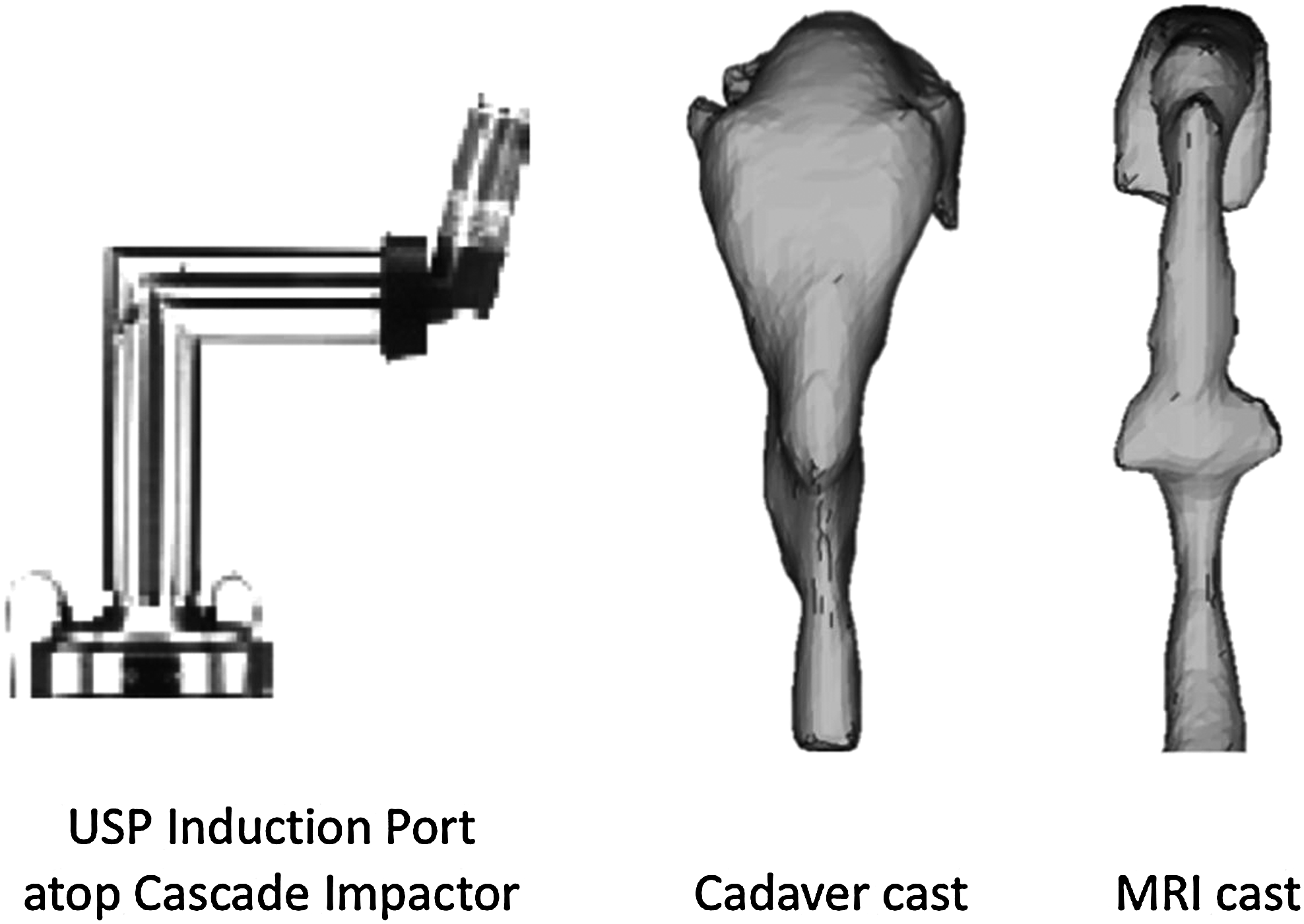
A comparison of the USP induction port and human throat models constructed from cadaver casts and MRI.(15)
The pharmacopeial induction port, often incorrectly called “a throat” and used for aerodynamic sizing of inhaler output was known to be an oversimplification that could only be used for product control purposes. Because throat deposition had been shown to be the major source of variability in lung deposition of inhaler-derived pharmaceutical aerosols,(4) improved physical models were essential if more accurate deposition predictions were to be sought from in vitro measurements. Cadaver casts of the oropharyngeal region suffered from distortions due to postmortem tissue shrinkage, as well as tissue distortions from the rubber injection process, and were generally considered inadequate today. As a result, these had given way to 3D computerized tomography (CT) based on X-ray images and magnetic resonance imaging (MRI) of the airways. The latter imaging techniques allowed models to more closely resolve the interface between the soft tissues of the upper airways and the airway itself. Overall, CT and MRI had enabled high resolution 3D images of the upper airways and lungs to be obtained(5) and models to be constructed from those images.
Imaging challenges that remain
Although multislice CT had greatly improved the 3D capabilities and resolution of CT, the required radiation dose in healthy volunteers was too high to justify. As a result, imaging artifacts could be minimized, successfully, only for individuals breathing tidally. Movement that occurred during the inhalation maneuvers used with many inhalers produced imaging artifacts at the radiation doses permitted for use in normal volunteers. The sophistication of the physical models that were available also depended on the region of interest in the RT and the desired age range of the subjects. Rapid prototype manufacturing methods had been used to create extrathoracic and upper tracheobronchial airway models almost exclusively based on adult CT scan data due to its comparative advantages.(6) As described above, however, radiation safety concerns had limited the usable CT scan data to the upper five or six tracheobronchial airway generations.(7) Thus, human lung cast morphometric data, as well as replicas of human lung casts, had to be used to derive in vitro airway models for generations 7 to 12.(8,9) Beyond generation 12, airway diameters were too small to produce in vitro models for aerosol deposition studies in the laboratory and idealized shapes had to be used to represent alveoli.(10–12)
Other uncertainties were noted such as changes in oral pharyngeal angles with head tilting and the fact that the shape of the laryngeal opening was a function of age and flow rate.(13,14) Dynamic imaging was an important technique that required further development because (a) tracheobronchial and pulmonary airway dimensions and carinal shape changed during each breath, (b) predicting and mimicking the ways in which a product was actually used by the patient was very difficult, and (c) forced breathing maneuvers were used with many pharmaceutical inhalers. Therefore, high temporal resolution via “dynamic MRI” was necessary. Presently, dynamic MRI was capable of achieving this, but only for single 2D slices. Echo planar imaging (EPI) could also be used with scan times per slice of less than 100 msec; unfortunately, this suffered from low spatial resolution (>2 mm) and image distortion at tissue–air interfaces. At present, the only feasible way of producing detailed 3D representations of the mouth and upper airway with MRI was to use triggered MRI.(15–18) This important technique had been used to produce images like those shown in Figure 2 for a single individual inhaling through low and high resistance devices; the changes seen in this figure were known to modify aerosol drug deposition patterns.(19)
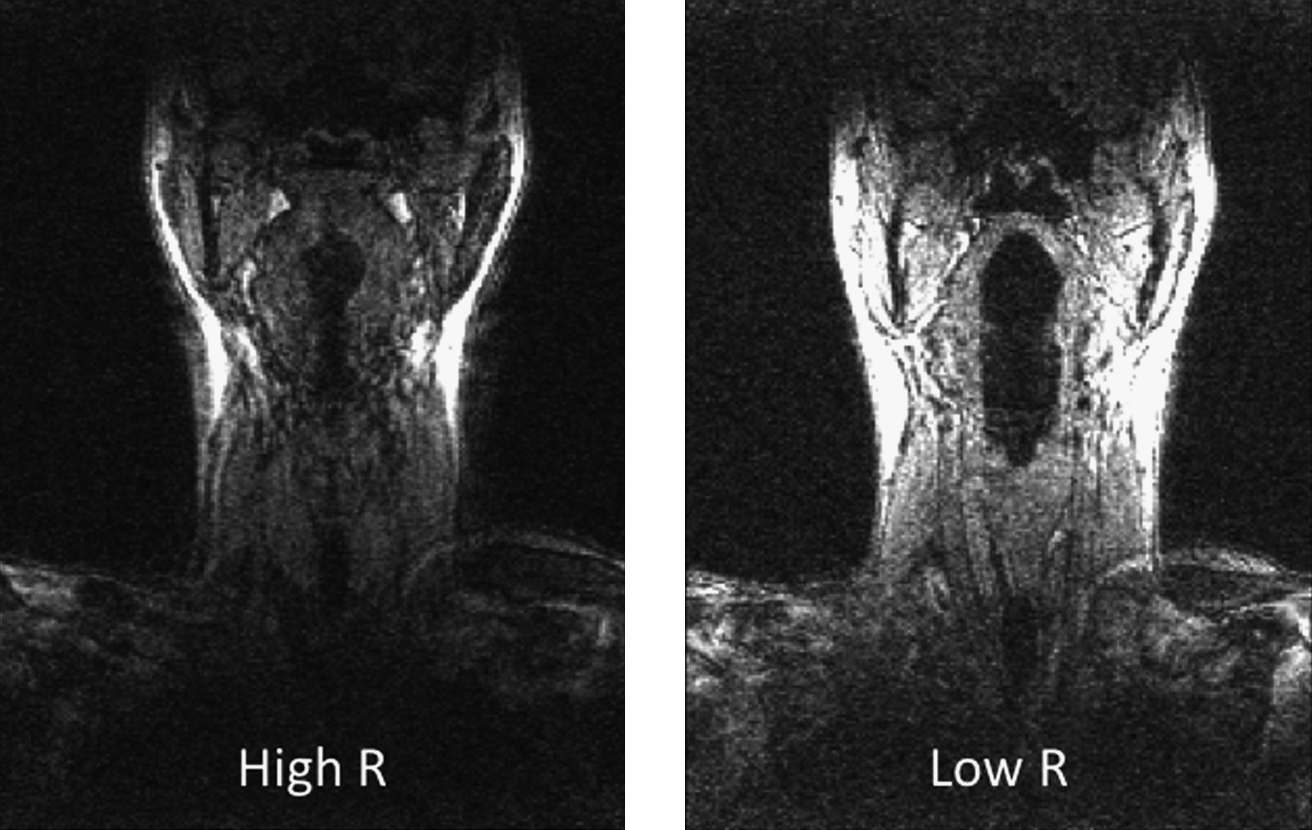
Triggered MRI images of a single individual inhaling through low and high resistance devices.(17)
Clearly, changes in oropharyngeal geometry like those shown in Figure 2 were most important when deposition from real inhalers with different airflow resistances had to be predicted. Unfortunately, studies like this, where significant alterations in airway volume were reported, were rare. Because MRI machines usually require subjects to be supine, the effects of posture were also poorly understood while the RT geometries for children and patients with different diseases were generally unavailable (one exception was noted where CT scans of infants had been used to develop physical models enabling in vitro studies of aerosol deposition.)(20,21)
Likewise, the variability of the RT geometries was not well characterized, especially with respect to the effects of the variables described above on the trachea and the upper airway generations. For example, lung volume was known to change depending on whether a subject was upright or prone. However, changes in airway diameter or morphology for the respiratory tract regions that were responsible for this change in lung volume were not well understood. It was also noted that potentially relevant anatomical structures may not be seen due to limitations of CT scanning techniques and that these had usually been omitted from images or simply ignored in the CT data that was reported in some studies. As a result, physical models that had been constructed based on such data contained geometric simplifications.
Imaging techniques in development
Several possibilities were discussed that were not widely available. The use of the hyperpolarized gases, 3He and 129Xe, had been used with either dynamic or static MRI in ventilation studies.(22) Although xenon was soluble in blood, helium was not absorbed by lung tissue. Therefore, in the future, the combination of hyperpolarized 3He and diffusion weighted imaging (DWI) may be useful when assessing the integrity and function of the alveolar spaces. Notably, the use of conventional and hyperpolarized MRI(23) to document the dimensions of the upper airways was in its infancy, whereas MRI had recently been used to quantitatively measure the regional deposition of aerosol with submillimeter spatial resolution in the RT of animals.(24) One further technique that may be useful was noted: pharyngometry involved noninvasive acoustic reflection techniques to yield information about the cross sectional areas of the upper airway; this had been described by Kamal.(25) However, pharyngometry does not provide 3D geometry and measurements require supine subjects breathing tidally.
Physical airway models for aerosol drug deposition studies
Casts that used to be created from wax impressions of cadaveric airways had been replaced in the last 10 years by plastic models created by rapid prototyping machines. Historically, the “lost wax technique”(26) involved the creation of a solid wax replica of those airspaces into which molten wax had been poured. Rigid (e.g., a polyester block) or flexible (e.g., a rubber film formed after evaporation of a volatile solvent) casts were prepared around the paraffin “negative” and the wax removed by melting and solvent rinsing. Although such models had been used to discern anatomical detail and surface features of the RT, they were laborious to construct, difficult to modify, and suffered from distortions due to cadaveric tissue shrinkage. More recently, physical airway models had been constructed from polymer resins in rapid prototyping machines. Based on a lung geometry surface model, these machines had been programmed to create a solid polymer airway replica for use in aerosol deposition studies.(27–30) Airway models made from laser-cured polymer resins were presently constructed by rapid prototyping in a “layer-by-layer” fashion over a period of hours. Thus, provided models were constructed with geometries that were representative of humans inhaling aerosols from pharmaceutical inhalers, there appeared to be no reason why aerosol drug deposition could not be studied in a range of physical models prepared by these techniques.
Presently however, there was a need to study and agree upon the most representative RT geometries; then to distill those geometries into a small number of easily manufactured physical airway models. Although there were a number of research groups studying aerosol deposition in realistic geometries of the human upper airways, three main approaches had been used. Groups were using (a) geometries taken from well-documented cadaveric casts in the literature, (b) “representative” geometries constructed after analysis of imaging data, (c) idealized geometries constructed with critical dimensions that were chosen to “merge medical imaging data and aerodynamic principles.” In many cases geometric simplifications were used to improve the ease with which the final physical models could be manufactured and used.(19,27,31–35) In most cases, the studied geometries were based on analysis of normal adult human airways, although intersubject variations in infant upper airways had also been studied recently.(20) Differences in aerosol deposition between the different models were presently unknown and the effects of age, disease, and the patient's interaction with a chosen inhaler all remained to be thoroughly examined. Notably however, the approaches in use showed a promising trend; one that was moving toward an agreed-upon, easily manufactured aerosol deposition simulator for the adult “mouth throat.” This should replace the USP induction port (Fig. 1), for aerosol deposition studies where an IVIVC was desirable.
Drug deposition studies in vitro
Typically, the internal airways of the physical models required coating with a viscous and adhesive liquid (e.g., silicone oil or glycerol). Suitable techniques for this were now part of the standard methods used for cascade impaction, to prevent particle reentrainment during analysis of the aerodynamic particle size distribution (APSD) of drugs emitted from inhalers (USP Chapter <601>).(36) Also, because the breathing maneuver used by a patient may well have a profound effect on both aerosol cloud formation and drug deposition behavior, testing deposition under the steady-state flow conditions most often used for quality control of inhalers after manufacture required, at a minimum, judicious choice of the steady flow rate to be use.(37) Unfortunately, although flow rate versus time profiles used by trained patients were known to be functions of inhaler air flow resistance,(38) the variance of the actual profiles employed by the general patient population during inhaler use were presently undocumented and likely to be poorly controlled by product instruction leaflets. In this context, a situation was described where drug deposition from a single powder inhaler, known for its reproducible dosing, had been tested in a realistic physical model of the mouth, throat and upper lung using two realistic inspiratory flow rate (FR) versus time profiles (Fig. 3).
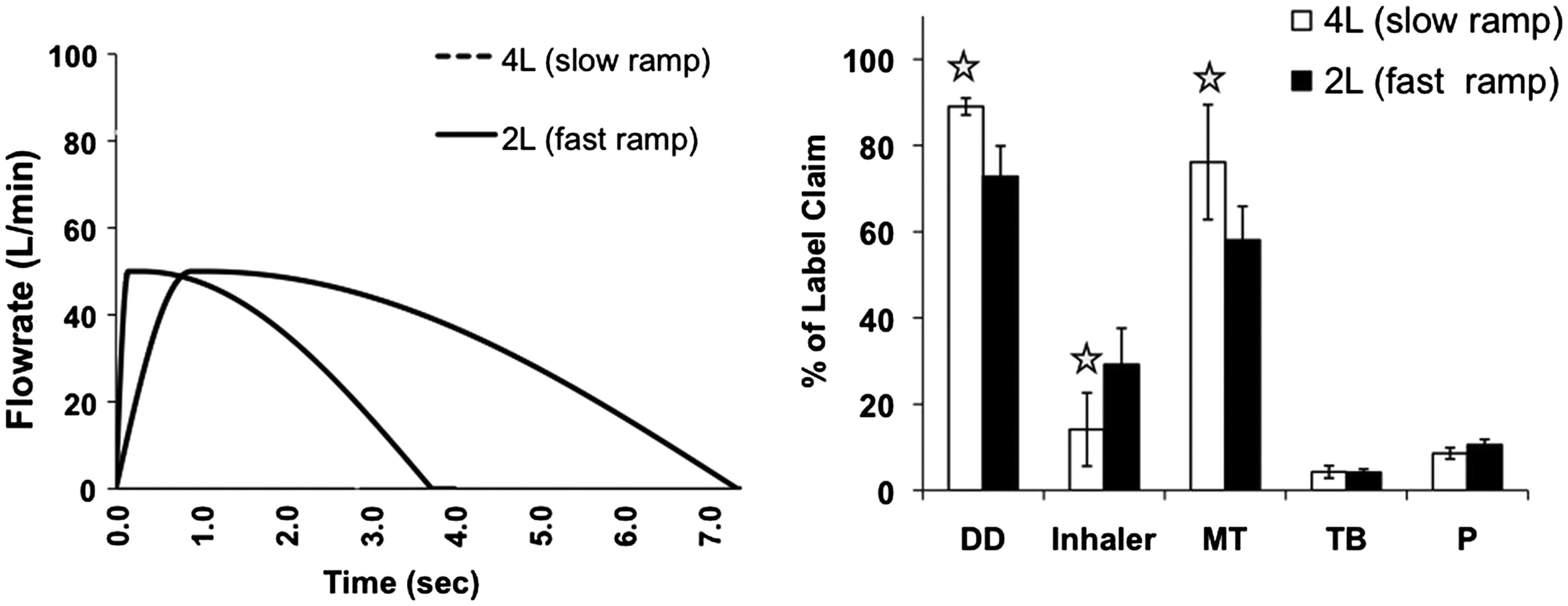
Albuterol deposition from NovolizerTM in a realistic mouth–throat geometry attached to a model of the trachea and first four lung generations [tracheobronchial (TB)]. Inspiratory flow rate versus time profiles (left-hand panel) were simulated to represent different individuals inhaling through the device.(40) Average drug retained in the inhaler is shown alongside deposition in the mouth–throat (MT), and “pulmonary region” (P), defined here as deposition beyond generation 4. DD shows the delivered dose for each scenario as a % of the 100-μg label claim. An asterisk indicates a significant difference by paired t-test (p < 0.05; n = 5).
The inhaler studied had moderate airflow resistance and different deposition profiles were apparent in the physical airway model when different inhalation maneuvers were employed (Fig. 3). Based on the work described by Finlay et al.(37,39) these differences were thought to be largely due to the effects of the different flow profiles on aerosol cloud production and inhaler emptying. It was clear, therefore, that patient inspiratory flow rate versus time curves needed to be studied, and likely variations agreed upon, if the effects of different maneuvers were to be incorporated within an IVIVC.
The approach described in Figure 3 was unusual; most often, physical replicas of the mouth–throat region alone had been used for in vitro testing. If the geometries of these were agreed, and “good” physical models of the mouth, throat, and larynx were used with known inhalation profiles, we could only expect to be able to predict total lung deposition (TLD). This was not as bad as it sounded because, to a first approximation, TLD was determined by mouth–throat deposition, exhalation of unit dose pharmaceutical aerosols was expected to be insignificant and TLD was probably what mattered most, clinically, as far as many topically active inhaled drugs were concerned. Thus, good physical models of the mouth–throat region were probably of the highest practical importance, especially because pharmacopeial inlet “throats” and some models based on cadaveric casts were known to underpredict throat deposition (Fig. 1). On the assumption that rigid physical mouth–throat models derived from 3D imaging of live, inhaling subjects could be used for IVIVC deposition modeling, an industry–academia collaboration had collected and analyzed a large data set from which a small number of physical mouth–throat models were selected statistically.(19) These models had been shown to provide accurate predictions, at least for two different powder inhalers(32) and another powder inhaler and dosimetric nebulizer, provided the model employed a sticky interior coating, realistic inhalation flow profiles and representative device handling. Under those conditions, the amount of drug escaping deposition in the mouth–throat model was equivalent to the total amount depositing in the lungs of healthy volunteers as assessed using a pharmacokinetic, charcoal block technique.(32) Significantly, if TLD was the desired outcome of such an experiment, there was no need to measure the particle size distribution of the aerosol; a filter at the exit of the mouth–throat model was all that was required for the in vitro measurement. However, with a cascade impactor in place, it may also be possible to estimate the APSD of aerosols exiting the mouth–throat model and to use this information as input to a numerical model to predict likely regional lung deposition downstream.(32) Alternatively, it was possible that a physical model of the upper RT generations may be added to that of a mouth throat(28,40) and upper tracheobronchial deposition measured to preclude the need for size determinations (Fig. 3); this approach avoids having to process size distribution data in accord with theoretically uncertain deposition behavior during a variable and dynamic breathing regime.
Validation of physical models
Oldham(41) reviewed the challenges involved with the validation process previously. These included (1) defining what was meant by validation, (2) defining appropriate experimental data for validation, and (3) determining when the agreement between model predictions and the chosen experiment was not fortuitous. For predictions of TLD it was easy to agree upon the first two of these criteria while fulfilling the third appeared to require a broader database with widened scope. This should include, for example, pMDIs with and without spacers as well as other inhalation platforms to fill the most obvious gaps and enable a comparison of in vitro and in vivo deposition across a range of pharmaceutical aerosols. Further validation was needed to cover populations other than healthy volunteers. With individuals suffering from lung diseases like chronic obstructive pulmonary disease (COPD), it was likely that the choice of representative flow profiles would become more important than a modified physical model of the mouth–throat and larynx, although the latter was likely to be of great importance when predicting aerosol deposition in children.
Prediction of regional deposition in the lung
For regional deposition within the lung itself Oldham's(41) first two criteria were also problematic because there were no direct methods to measure the regional deposition of pharmaceutical aerosol drugs in terms of in vivo anatomical space. Therefore, there were no solid data by which to judge any model's predictions. Unfortunately, the existing literature contained many in vivo claims based on unvalidated in vitro and in silico methods that were believed to confuse conversations with drug regulators. Like environmental aerosols, the safety and efficacy of drug clouds from inhalers were believed to relate to the doses depositing in three main regions of the RT as described by Stahlhofen et al.(42) Using Stahlhofen's terminology, the extrathoracic (mouth, throat, and larynx), tracheobronchial (ciliated airways), and alveolar regions (the remainder) represented the in vivo regions of interest for pharmaceutical systems. However, Stahlhofen's models were based on in vivo data for monodisperse stable aerosols with different sizes. Although they appeared to enable estimates of deposition in important regions of the RT, they failed to consider the effects of polydisperse aerosol distributions and aerosol size change due to evaporation and condensation.
Thiel described his “Stahlhofen predictions” for TLD based on analysis of APSD data collected for several inhalers (Table 1). He noted that a breath hold correction must be added to the aerosol residence time in the lung when predicting alveolar deposition, and that integration of equations over the log-normal curves for the APSD of pharmaceutical aerosols that were determined in vitro, from the nonballistic fraction of the discharge from each inhaler, provided evidence that the models were “sufficiently accurate” for pharmaceutical purposes.(43,44) Thiel also noted that the recently developed online “Aerosol Research Laboratory at Alberta (ARLA)” respiratory tract calculator,(3) that uses carefully chosen dimensionless parameters to capture intersubject variability in geometry, provided similarly accurate predictions.
Note: Steroid MDIs 1 and 2 used 10.17 sec and 1.5-sec breathholds, respectively.
The ICRP Model(45) was based upon “NYU” data(46,47) where subjects used tidal breathing at 14 breaths per minute, with approximately known inhalation rates and volumes. As shown in Table 1, albeit for a limited example, the ICRP version of the Stahlhofen equations(45) more accurately predicted total lung deposition than Stahlhofen's original equations.(42,48) In discussion, however, the present authors noted that the predicted subdivision of TLD into alveolar and tracheobronchial components using Stalhofen's algebraic approach was impossible to validate for pharmaceutical aerosols because the aerosol doses deposited in Stahlhofen's alveolar and tracheobronchial compartments were determined kinetically for insoluble, radiolabeled aerosols. That is, 24-h lung retention of well-characterized insoluble radiolabeled environmental aerosols was assigned to “alveolar” deposition while insoluble material cleared from the lung in the same period was considered to have been deposited in the tracheobronchial region where it was then cleared largely by mucociliary clearance.
Although Stahlhofen's equations(42) could be used with aerodynamic particle size distribution data to estimate the possible pulmonary and tracheobronchial deposition of pharmaceutical aerosols, those predictions were bound to be uncertain because pharmaceutical aerosols were often unstable and polydisperse, with inhaler platform-dependent momentum or “spray power.”(27,49) Pharmaceutical aerosols were also inhaled as boluses by humans with breathing and lung abnormalities; in short, pharmaceutical aerosols were not homogeneously distributed in inspired air like those used to create Stahlhofen's models. Furthermore, pharmaceutical aerosols were often of uncertain size because their aerodynamic size distributions reported in the literature were usually determined from unrealistic “steady-flow” cascade impaction estimates that were determined well downstream of the inhaler, often following unrealistic addition(s) of dilution air. Indeed, Figure 4 (50) was used as an illustration of the time dependency of the size distribution from a spray aerosol formed at the nozzle of an aerosol generator being developed as a prototype inhaler.(51) Despite these daunting issues, careful attention to detail had allowed validation of tracheobronchial and alveolar deposition predictions for unstable, hygroscopic aerosols using comparison to in vivo SPECT imaging data;(52) this included the prediction of variations in deposition across the population. However, the development and validation of similar models for subjects with disease remained a topic for future work.

Light-scattering data sampled with time from a Malvern SprayTechTM positioned at the nozzle of a heated capillary aerosol generator. Data is apparent median droplet diameter (micrometers) for an aqueous formulation exiting the generator during a 2-sec burst. Large droplets were formed at start up and close down with a lengthy steady-state period in between.(50,51)
The actual size of the aerosol from the capillary aerosol generator described in Figure 4 was a complex function of time and the interplay between aerosol droplets and their environment. Heat, mass, and momentum transfer (droplets to gas phase and vice versa) had to be accounted for in order to correctly predict (1) the deposition of this spray in the oropharynx and (2) the aerosol characteristics leaving the oropharynx and entering the trachea.(51)
Computational Fluid Dynamics
The time-consuming nature, expense, and large parameter space of experimental measurement made simulation using computational fluid dynamics (CFD) attractive. The dream of CFD was to (1) develop physicomathematical model(s) describing the probability that drug-containing particles or droplets would deposit in each region of the RT of patients, under a small set of well chosen circumstances (2) validate CFD routines in comparison with a finite experimental data set, and (3) use CFD to interpolate or extrapolate deposition data for situations that had not been studied experimentally. Unfortunately, existing commercially available CFD packages made it difficult to include the dynamic complexity of pharmaceutical aerosols; initial conditions for either droplet/particle size distributions or velocity in region(s) of cloud creation were difficult to determine experimentally and subroutines that had to be created to deal with issues like multicomponent droplet evaporation were neither intuitive nor transparent.(53,54) In practice, IVIVC's for both powder and spray systems demanded considerable experimental work in physical airway models to provide accurate initial conditions of the aerosol as a starting point for CFD. Nevertheless, once validated, CFD models could be predictive of aerosol drug deposition and, as such, the approach offered a convenient way of comparing and potentially optimizing inhaler performance.
Dry powder inhalers (DPIs)
One of the more challenging areas for CFD was the simulation of powder behavior in DPIs. The ultimate use of CFD during development of a DPI formulation should probably involve the simulation of the entire powder delivery process occurring during patient inhalation. This included simulation of (1) powder entrainment from the formulation inside the inhaler, (2) subsequent deagglomeration of the entrained powder, and (3) calculation of particle trajectories through the inhaler and respiratory tract, ending with deposition on the respiratory tract walls. The present state of the art and the way forward with each of these aspects were discussed.
Little research had yet been published using CFD to simulate even the first step of the process, powder entrainment.(55) Nevertheless, a large body of published research existed on the related topic of fluidized powder beds and it was likely that methods borrowed from the fluidized bed literature(56) were usable with CFD to calculate the gas–solid mixture flow that occurred as powders became airborne in DPIs. Particle motion could be simulated using an unresolved discrete particle analysis,(57) sometimes called discrete element methods (DEM), whereby the motion of particles was calculated from Newton's second law using lift and drag forces obtained from correlations specifically developed for micronized particles attached to larger carrier particles.(58) Countering these aerodynamic detachment forces were the forces of adhesion between particles. Complicating the analysis was the need to model particle collisions and possible triboelectric charging as well as the frictional forces that were confounded by the presence of surfaces with different degrees of “roughness.” It was also noted that in unresolved DEM, where correlations were used for the aerodynamic forces on particles, that local fluid flow in the neighborhood of the particle was unresolved. A more sophisticated, but computationally demanding approach, was instead to resolve the microscale fluid flow around each particle using direct numerical simulation, a topic that was ripe for future research using either lattice Boltzmann or Navier-Stokes approaches.(59)
Once particles were entrained, deagglomeration was needed if they were to avoid deposition in the mouth–throat. Deagglomeration could occur either through collision with the solid walls of the inhaler or by aerodynamic forces while the particles were airborne. For collisions, standard CFD methods could be used to predict agglomerate particle trajectories while qualitative indications of deagglomeration could be obtained by examining the number and velocity of wall impacts.(60) Quantitative predictions of deagglomeration had been made by Nichols and Wynn(61) by including models for collisional deceleration, assuming elastic deformation on impact; also by using JKR adhesion force models with incipient rolling motion combined with AFM data for adhesive forces. For deagglomeration induced by aerodynamic forces,(62) qualitative estimates of the effect of turbulent eddies on agglomerates had been made using integral strain rates.(63) Quantitative prediction of aerodynamic deagglomeration was also thought to be possible by resolving the energetic turbulent eddies using large eddy simulation (LES), although particle sizes in pharmaceutical systems were typically much smaller than the most energetic of eddy sizes; thus, correlations were needed to predict lift and drag forces due to flows at unresolved length scales.(58)
Spray aerosols
For pharmaceutical sprays, several challenges existed with the use of CFD. For example, the physics of spray aerosol formation and delivery included turbulent and often compressible flows, multiple phases, evaporation and condensation, heat transfer, and transient effects. Challenges in simulating sprays also included incomplete knowledge of inlet/initial conditions and the selection or development of adequate submodels to account for factors like turbulence, droplet evaporation, and droplet breakup. Still, CFD appeared to offer an effective tool when used in conjunction with in vitro experiments for the prediction of deposition in vivo. To date, the use of CFD for the analysis of pharmaceutical spray aerosols had focused primarily on modeling spray physics with comparisons to in vitro data for droplet velocity and deposition.
Successful comparisons of CFD spray simulations and in vitro data included the study of Dunbar,(64) which showed agreement between simulated and predicted droplet velocities for a pressurized metered dose inhaler (pMDI). Kleinstreuer(65) had simulated droplet transport and deposition from two pMDI systems in a spacer and upper airway geometry and found good agreement with existing in vitro and in vivo data. Longest et al.(49) also simulated spray transport and deposition for a pMDI, a capillary aerosol generator, and the Respimat inhaler. Deposition fractions in the inhaler mouthpieces and attached induction ports were in good agreement with concurrent in vitro experimental results for all three systems. Further details of the Respimat spray inhaler and evaluation in a more realistic mouth–throat geometry were also reported;(53) advantages of a concurrent CFD and in vitro approach for quantitative inhaler analysis and design had been described by the same authors.(54) Thus, current CFD studies of pharmaceutical spray aerosols had primarily compared numerical results with in vitro experiments in an attempt to model the spray physics of transport and deposition. Moving forward, what was also needed was the concurrent use of in vitro and CFD analyses to develop correlations with in vivo data. The idea was to use concurrent CFD and in vitro analyses together to address the issues of (1) spray physics and (2) geometric factors.(54) In this approach, in vitro experiments would be used to provide initial conditions, such as droplet distributions and inlet spray velocities, as well as validation data for the final CFD model. Insights gained from this concurrent approach could then be used to guide assessments of the remaining in vivo correlation issues that related to respiratory physiology and variability described above.
Deposition modeling with CFD
The application of CFD to model aerosol deposition in a 3D representation of the airways was relatively recent. Initially, the simulations had been constrained to specific stretches of the airway path, such as the trachea and a few generations of the lung, or the alveolar regions. Literature reports had offered some insight into the local effects of geometry on air and aerosol flow, such as the effects of tracheal rings, the shape of the carinal ridge,(66) or the size change of the alveoli.(67) However, those models were limited by the lack of upstream information about flow. Several of the present authors believed that a more comprehensive approach could start from well defined boundary conditions at the inhalation device and then progress through models of the oropharynx into the different lung generations, taking into account all upstream effects. Using this approach, reasonable predictions of deposition could likely be obtained, although it was noted that care was needed when including the effects of turbulence using a Reynolds-averaged approach, as shown by Figure 5. This figure shows a comparison between the in vitro experimental measurements of deposition in the main and lobar bronchi(29,68) versus those predicted using a commercial CFD program for the same geometries used to obtain the in vitro data.
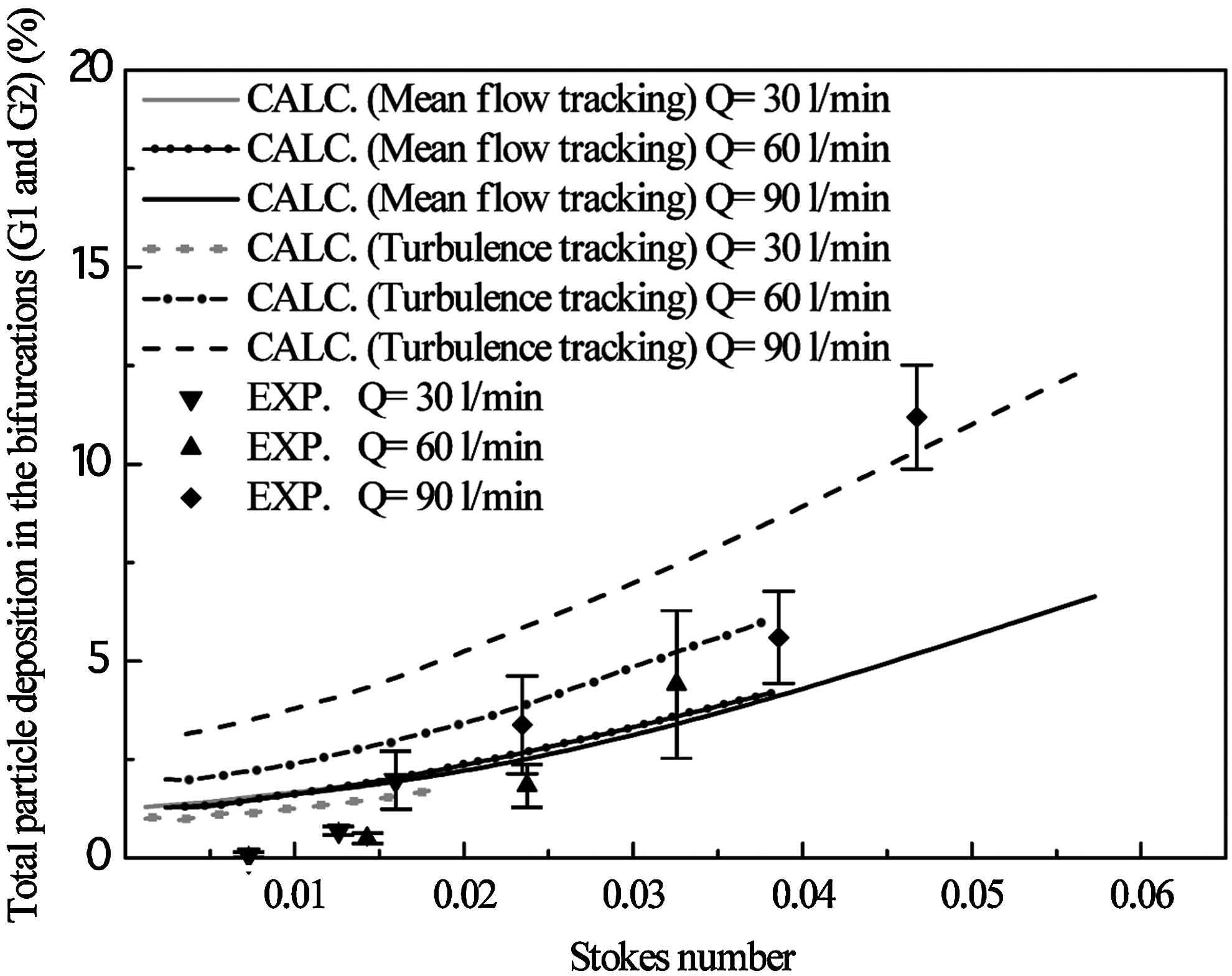
Deposition in the main and lobar bronchi (generations 1 and 2) is shown at three different inhalation flow rates, Q, as a function of the dimensionless Stoke's number for the in vitro measurements of Zhang et al.(28) (solid symbols) with their FB geometry. Also shown are lines indicating results obtained with a commercial CFD package (ANSYS CFX5.7) for the same FB geometry, with the Reynolds-averaged Navier-Stokes equations solved using a standard k-omega turbulence model, either with (“turbulence tracking”) or without (“mean flow tracking”) the standard eddy interaction model.(29)
This approach reached some level of completion, when the COPHIT [Computer Optimised Pulmonary delivery in Humans of Inhaled Therapies(69)] program, a project funded by the European Union using ANSYS/CFX, successfully simulated the entire airflow path from the device to the eighth generation. The program had modeled more distal airways that could not be resolved by CT scanning, by using a 1D approach. Other recent efforts, such as the collaboration between Materialise (Belgium) and Fluent, also built semicomplete respiratory tracts to obtain more realistic flows in the upper airways. However, these models had not been validated with experimental deposition data. In the mouth and throat, care was needed with Reynolds-averaged Navier-Stokes models to avoid the overestimation of deposition due to turbulent transport,(31,70) an issue that could be avoided by using large eddy simulation.(71) A potentially better approach for modeling flow and particle deposition in the tracheobronchial airways, allowing good accuracy control, was to break the airways down into parallel and serial sections and conduct an automated series of CFD simulations, as suggested by Zhang et al.(72) Notably, Vinchurkar and Longest(73) showed that rapidly applied tetrahedral and hybrid meshes, like those used with COPHIT, artificially influenced the flow field profiles leading to possibly inaccurate deposition results, especially for particle sizes less than 10 μm. They suggested that time intensive, but much more accurate, hexahedral meshes provided a better solution that matched the experimental data. This discussion highlighted the need to verify CFD predictions of aerosol deposition with experimental results to ensure that each CFD method was sound.
Deposition modeling in the future
Although current CFD simulations used static geometries obtained from medical imaging scans, future researchers may wish to include time dependent motion of the respiratory tract walls measured in vivo, although (as discussed earlier), such work awaited improvements in temporal and spatial imaging methods if the alveolar regions were to be resolved. Also, as noted above, geometric in vivo deposition data were as yet insufficiently detailed to enable validation of CFD simulations of respiratory tract deposition beyond the first few airway generations.
Whether CFD should supersede the simpler, 1D models of aerosol deposition in the lung discussed earlier (e.g., Stahlhofen et al.(42)) also depended on the purpose of the modeling. When properly applied (including realistic boundary conditions and appropriate turbulence model), CFD offered valuable insight into local deposition patterns. This was especially true in the upper airways, where the actual geometry could be well defined using CT scans. However, large-scale lung simulations, such as those performed by COPHIT,(69) still required several days or weeks of computing calculations in order to proceed from the CT scan of a patient to a completed deposition analysis. This approach seemed appropriate to analyze an individualized type of application, such as the design of a specific treatment for a localized lung tumor. However, those same characteristics made a full CFD approach less appealing for the study and design of aerosol drug delivery systems for use in a general population, largely because of its high price and the uncertainty concerning the representative nature of the selected geometry.
1D dynamic lung deposition models, although heavily simplified with respect to airway geometry assumptions, could incorporate all the fundamental physical processes that affected particle size and deposition at a small fraction of the computational effort of CFD. Naturally, these 1D models could not resolve localized deposition patterns, but they could likely be tuned to give accurate results for delivery of drugs to target an entire lung region. Most diseases treated with inhaled aerosols were believed to require targeting of either the tracheobronchial (beta agonist bronchodilators and mucolytics) or the alveolar region (large molecular weight systemic drugs) or both (anti-inflammatory and antibacterial drugs), and advanced 1D models could provide this information with high accuracy.(37) For these reasons, the 1D models discussed earlier(45) seem better suited for the development of nonindividualized aerosol drug delivery. However, because the range of physiologically relevant parameters was finite, 1D models could be used to incorporate the results of many CFD simulations within their parameter space, improving the quality of their predictions without incurring a large increase in computational cost. The low computational cost of 1D models, supported by CFD, may also allow such models to eventually be incorporated into smart delivery devices(74) whereby the deposition in the respiratory tract of a subject inhaling from a device could be predicted in real time and used as feedback to control dosing or delivery from the device. The translation of results between the two types of models (i.e., 1D vs. CFD) remained a topic of current and future research.
More validation of regional deposition data,(52) based on the physiological characteristics of each lung region, was needed(39) to improve our confidence in the deposition predictions for both 3D and 1D models with inhaled drugs in patients. Clear demonstration, by comparison with in vivo deposition data, that such models could accurately capture the variety of changes in lung geometry and regional deposition that occurred with various diseases(75,76)) or physical conditions(77) was an important area of ongoing research. Continued progress in imaging and modeling, combined with future increases in computing power, would certainly bring such modeling into routine use in preclinical device development. Although the pace at which numerical models were likely to be accepted as a part of regulatory standards would be slower, it was hoped that research on some of the topics presented in this article would allow progress to be made in that direction.
Conclusion
Methods of arriving at IVIVC are discussed that predict the spatial deposition of drugs in the airways following their presentation to humans from a variety of inhalation aerosol platforms. The advent of imaging and rapid prototyping has dramatically improved the ease of use of physical airway replicas that allow in vitro measurement of deposition. Mouth–throat replicas, for example, can be used to allow rapid estimation of total lung deposition in normal adults. However, questions remain regarding how best to incorporate variations between subjects, disease states, breathing patterns, and the effects of postural position (i.e., supine vs. sitting) as well as the variability induced by patient–device interactions. Methods that allow in vivo measurement and construction of models of airways with diameters <1 mm is currently beyond our reach, as are models of the alveolated regions that contract and expand with time. For droplets, additional issues arise associated with temporal size changes that may require correct mimicry of in vivo humidity and temperature conditions. Although simple algebraic and 1D deposition models appear to be able to predict respiratory tract deposition, including hygroscopic effects, further development and validation of these models for different diseases and subjects, especially children, are needed. CFD can be used to aid in the prediction of device performance, but much work remains to be done in this regard. In particular, simulation of powder entrainment and deaggregation within DPIs remains largely unexplored. For sprays, the complexity of spray production with pharmaceutical devices remains beyond the reach of typical commercial CFD routines; furthermore, initial and boundary conditions need to be obtained empirically. In summary, although considerable progress has been made in recent years with IVIVCs, as outlined here, further work remains to be done to allow these and future developments to be confidently incorporated throughout the processes of device development and regulatory approval.
Footnotes
Author Disclosure Statement
The authors of this review are employed by the companies and institutions disclosed on the title page of this manuscript. In some cases, the research referred to may be sponsored by those organizations and/or others, as disclosed in each of the cited references. No other conflicts of interest exist.