
Abstract
Abstract
The 1000 Years of Pharmaceutical Aerosols Conference convened posing the question; “what remains to be done?” When applying this question to the topic of inhaler devices, two hugely different perspectives could be taken. On the one hand, it could be argued that because there is an array of delivery systems available and the industry, prescribing physicians and patients alike have considerable choice, why would we believe it necessary to do anything further? On the other hand, as an industry, we are constantly reminded by our “customers” that the inhaler devices available are less than adequate, and in some cases woefully inadequate, that they are not “patient” friendly, not intuitive to use and importantly do nothing to encourage the patient to take the medication as intended and as prescribed. So, taking the second point of view as more reflective of reality—the Voice of the Customer—our starting point must be that there is still much to do in the field of inhaler devices. The purpose of this article is to outline some key basic requirements for inhaler design and perhaps to question some of the entrenched thinking that has pervaded inhaler product design for too many years.
The Inhaler Landscape in 2035—A Speculation
The inhaler landscape in 2010 has developed through a strong and sustained focus on the drug and it is interesting to observe that the recent “blockbuster” product, Spiriva, delivering the long acting anticholinergic tiotropium, uses a delivery technology that has been around for many decades—the capsule-based dry powder inhaler (DPI) device. In contrast, GSK's long-acting bronchodilator salmeterol and the corticosteroid fluticasone propionate use a bespoke delivery technology referred to as the Diskus® (Accuhaler®) developed specifically to deliver 1 month's therapy twice a day. It is also arguable that inhaler technology has become largely generic.(1) Of course, novel drugs are scarce and predictably market incumbents will fight fierce defensive actions(2) against generics as patents expire.
In order to speculate on progress to be expected over the next 25 years, it would be interesting to take a step back 25 years and look briefly at the landscape in 1985. This period was dominated by the metered dose inhaler (MDI), with capsule-based DPIs used when the MDI was unable to deliver large amounts of inhaled drug, to overcome the problem inhalation and discharge coordination, and of course, to provide a degree of patient choice. Inhaled short-acting bronchodilators and corticosteroids were beginning to dominate the market with some of the less effective drugs moving into decline. New inhaler devices were not yet seen, although clearly there were several in the latter stages of development; for example, the Turbuhaler® and the Diskhaler®. The Diskus® had not been “discovered” and the CFC challenge was invisible.
What progress has been made over the last 25 years? We still have the MDI, although some would say it is in decline (or maybe static), we have essentially met and overcome the challenge of developing and introducing non-CFC propellants, we have seen the emergence of true multidose DPIs with the Turbuhaler® being extraordinarily successful in Europe and the Diskus® successfully launched into the hitherto DPI naïve U.S. market. Several breath-actuated devices have been developed and introduced, but significant market penetration has not been achieved mainly because of the lack of convincing clinical evidence that coordination devices were worth prescribing and quite possibly cost—or rather company pricing strategies.
So, what can we expect in 2035? This is likely to be dependent upon the approach taken and the issues we as an industry will face; some of these are listed in Table 1.
When posing the question what remains to be done? this really provokes the question: is anything really needed and are current delivery systems adequate? If the latter question is answered in the affirmative, inhaled delivery devices would plateau and stagnate. If change is to occur then innovation is critical. But then the question becomes what, where, and how? Three classes of innovation have been identified by Christensen;(3) sustaining, disruptive, and revolutionary innovation; the concept is depicted schematically in Figure 1.

Schematic diagram illustrating Clayton Christensen's three classes of innovation.(4)
It is argued that sustaining innovation is driven largely by customers who do vary hugely in their demands. So, for only moderately demanding customers improved “performance” need only be marginal and each step of improvement is small based on a refinement of what the customer would regard as a traditional product. A good example of this would be the continued refinement of the car by manufacturers; new cars are only intended to sustain the existing market, sustain competitiveness, and perhaps gain a small additional market share—until, that is, the competition introduces its “refinement” and the status quo is maintained. There are more demanding customers who require product extensions with significant improved performance, and on shorter time scales. Perhaps the best example in this category is the mobile phone market where the Blackberry® and iPhone® have provided enhanced performance and capability for many demanding customers.
Disruptive innovation disrupts the marketplace and a single disruptor forces change on the whole market. The introduction of low-cost digital photography has changed the face of mass market photography. This has disrupted the traditional photographic film, developing and printing market to such an extent that major companies like Fujitsu have withdrawn from the production of mass market photographic film—does this mean the end is nigh for photography as we used to know it?
Revolutionary innovation changes everything. It changes the way we live, the way we do business, and touches everyone certainly in the developed world. Although landline telephony might not immediately seem like revolutionary innovation, it did touch everyone—until the introduction of telephony time could not be unified across a nation. The ability to communicate in real time across large distances did not exist, and so time could not be ascribed a given setting. For example, in the case of the UK, as time was measured according to the position of the sun, time in the East of England was different to time in the West of England simply because “Mr East” could not communicate with “Mr West” that it was 2.00 pm in the afternoon in real time. Clearly, the situation was much more pronounced in the United States, where the distances are far greater, and thus the “time differences” more pronounced. Telephony therefore changed our ability to standardize time and allowed everyone to operate from a reference base of a standard time and Greenwich Mean Time (GMT) was born.
The Internet is changing everything we do and the way we do it, and, the possibilities seem to be endless. This is revolutionary innovation that has opened the doors of the world—and long may it remain for peaceful purposes.
We can apply these concepts of innovation to inhalation drug delivery.
Sustaining innovations
A sustaining innovation improves known product performance and is incremental in character; for example, including dose counters on an MDI or DPI. Almost the total investment in respiratory device development over the last 25 years has been in this area of sustaining innovation; improving the three technologies DPI, MDI, and nebulizers. Even the non-CFC propellant challenge was a sustaining innovation as it simply maintained the industry's ability to remain in business with this delivery system.
Sustaining innovations over the next decade might include:
MDIs Dose counters More consistent metering valves Breath actuated devices Improved control over emitted particle size distribution Niche patient-friendly devices for the paediatric and growing geriatric populations DPIs The use of “airy” particulate powder formulations with NCEs or as branded generics Dose counters Inspiratory flow rate independence Moisture insensitive powder formulations Higher respirable dose efficiency Niche patient-friendly devices for the paediatric and growing geriatric populations Generic products in a broader range of delivery systems Nebulizers and aqueous-based delivery Better portability Delivery of suspensions of drug Systemic drug administration based on current technologies Modifications of the known systems to improve efficiency for biological molecules
Each sustaining innovation would not lead to a transformation of the market for delivering drug to the lung; they would enable each of the delivery systems to maintain and improve its position by small incremental steps maintaining the status quo with respect to the other delivery systems available. However, it is arguable that there are real advantages in such small and incremental steps in getting inhalation systems ahead, as witnessed in the very different but notable example of various “species” development through Darwinian evolution.
Disruptive innovations
A disruptive innovation introduces a new technology with the potential to displace existing products. Some respiratory examples might be:
Compliance: A universal and effective means of assuring compliance would be widely welcomed and disruptive for the sales of nonpossessors. In Figure 2 the drop-off in compliance is significant for all dosage forms but is most dramatic for inhaled products. Vapors: Within the last few years Alexza(4) has commenced the development of vapor-based inhaler medication for respiratory use and trials of more than five well-known compounds are underway, with claims of up to 200 drugs being suitable for this method of delivery.(5) Characteristically for a disruptive technology, initially the idea prompts many, many reasons why it cannot be realized; decomposition of the drug at the volatilization temperatures required, systemic versus local effects, ability to deliver the required mass, control over reproducible delivery, etc. Nanotechnology: Dautreband's “Microaerosols”(6) discusses work carried out on therapeutic aerosols in the submicron range. His apparatus was daunting and the data hard to interpret but it did appear he achieved significant responses with microaerosols of nanometre size as indicated by the methods available to him. By 2009 the arena of nanotechnology is “hot” across a wide spectrum of respiratory disease(7) and with increasing evidence(8,9) of pharmacological activity. Figure 3 shows the recent patent activity, which is indicative of interest. Controlled release: Both molecular and formulation means could be used to achieve more controlled and sustained pharmacological activity. Universal device: The availability of a generic DPI would be an interesting concept within the industry. With the ever-increasing health costs and escalating demand for low cost provision of healthcare, could healthcare providers resist actively sourcing a generic DPI with wide patient acceptability? Actives: “Silencing” RNA oligonucleotides stimulating new treatments and devices.
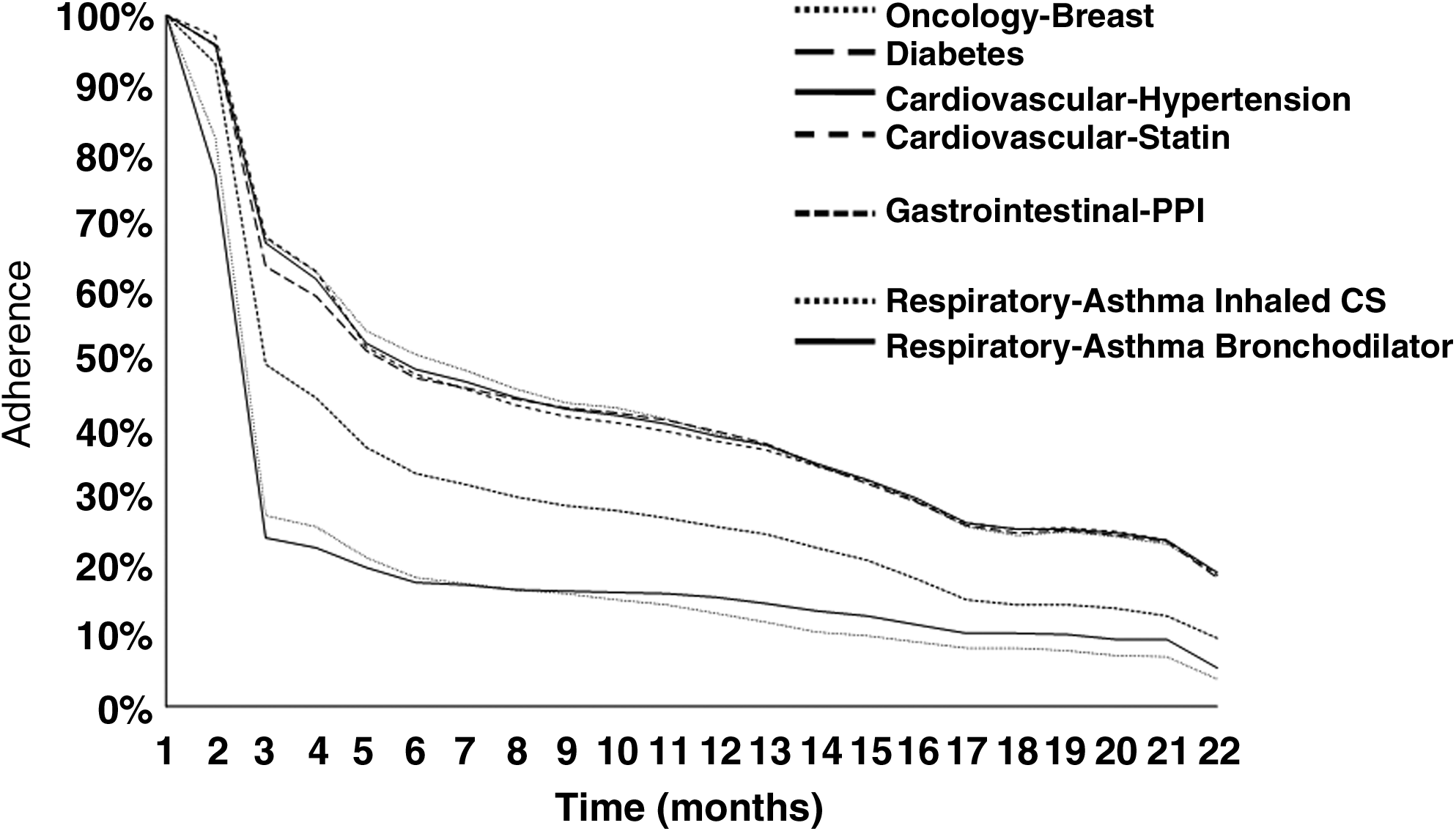
Patient adherence over time for various drug products (Source of data: NDC Health).
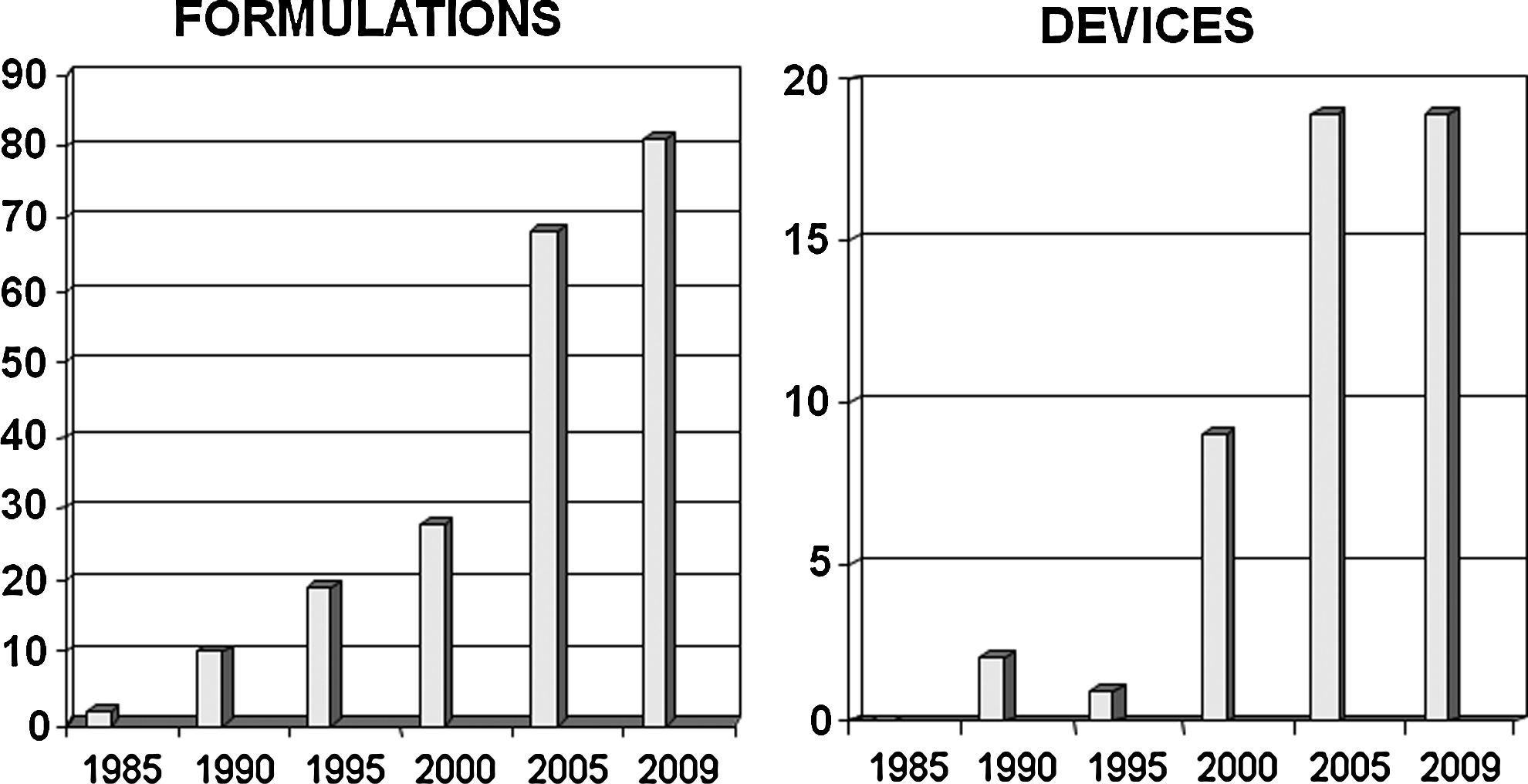
Number of first patents in a family published in 5 year steps between 1980 and 2010 (Source: search of Derwent World Patent Index).
Revolutionary innovations
Innovation that can be classed as revolutionary would introduce products into the market with fundamental new features that transform the lives of patients and their treatment approaches globally. Penicillin could be regarded as revolutionary in that it transformed the treatment of bacterial infection for mankind. It is perhaps ironic that this very treatment that can be regarded as revolutionary has been subject to much sustaining innovation over the years demanded by the resilience and progressive transformation of bacterial infection. Examples in the respiratory field might be:
The accurate and specific targeting of drug to the lung by the oral route; the replacement of inhalers by a tablet could be regarded as revolutionary. Gene technology could be used as a means to identify and supplement or replace gene complexes that give rise to a respiratory disease state. Infant “vaccination” against a predisposed genetic preponderance to respiratory diseases.
Revolutionary innovation in the respiratory field would eliminate inhalers; MDIs, DPIs, nebulizers and all our sustaining and disruptive efforts would count for nought. This is not, perhaps, a desired scenario given the human and capital investment the pharmaceutical industry has in respiratory research and inhaled product development. Equally, by the very nature of revolutionary innovation we cannot easily look forward and predict just when, if at all, a revolution step will be taken.
The ways and means of supporting a revolutionary innovative approach are not easily achieved, as sustained effort and commitment is required. Industry and academia research collaborations, an industry cooperative along the lines of IPAC for the development of non-CFCs, or entrepreneurial effort funded by the traditional route of venture capital with the formation of suitable legal structures are all means to execute work in disruptive and revolutionary innovations.
However, taking a somewhat realistic view, it is likely we will need to continue with the development of sustaining innovation and technologies that move us slowly forward down the “performance” improvement path with occasionally, a disruptive innovative step occurring; our challenge is to spot the winner in this latter category just as Charlie Thiel and his colleagues at Riker Laboratories did in 1956 when the MDI was first born.
Devices with Patient Compliance—A Need or a Nice to Have?
Delivering drug effectively and reproducibly to the lungs via the respiratory tract is a huge challenge. There are many reasons why the challenge is so huge, of which the technical challenge of generating particles/droplets of a size that are likely to deposit effectively in the lower respiratory tract is only a part. Conventionally, inhaled delivery systems have been designed and constructed to generate poly-dispersed aerosols where the majority of particles/droplets are in the so-called respirable range; the respirable range has been defined over the years as 1–5 micron.
Devices such as MDIs, DPIs, and jet nebulizers utilize technologies that are in many cases at least 50 years old and consequently were developed at a time when “usability” by the patients was not a major consideration; indeed, in some cases not a consideration at all.
Moreover, many devices are frequently being used for purposes for which they were never intended. The MDI was a disruptive solution (and quite possibly in the minds of some, a revolutionary solution) to the problem of developing a multidose portable inhaler for the delivery of short-acting β-agonists. The potency of these agents combined with the ability to take an extra dose(s) if a positive response was not achieved quickly meant that poor inhalation technique was rarely a problem when an MDI was used to relieve acute symptoms. However, MDIs were never really intended to be used for drugs such as inhaled corticosteroids where the patient does not receive rapid feedback on the effectiveness of the inhalation and MDI discharge manoeuvre; inhaled corticosteroids require reliable and reproducible delivery on each occasion the drug is inhaled to achieve control of symptoms over the long term and poor inhalation technique by the patient can seriously jeopardize this requirement.
A combination of increased regulatory scrutiny on inhalation products and a collective almost single focus by those in the industry in the late 1980s when the industry was faced with the phasing out of CFC propellants meant that patients and physicians were left, and still are left, with the choosing between devices that are capable of delivering drug to the lungs only when used strictly as according to the instructions. However, intrasubject variability is very high and the devices now available are very difficult to use effectively. Indeed, many studies indicate that the majority of patients are not able to use their devices effectively, MDIs and DPIs, and hence, the benefits of potent therapies such as inhaled corticosteroids for the treatment of asthma are often not fully realized.
There are several terms that are used, sometimes interchangeably, which need some definition:
The competence of a patient is essentially the ability to use a given device correctly. It is arguable that the “simpler” a device is to use then the greater proportion of patients who will have the competence to use that device correctly. For those familiar with the wide range of devices available it will be clear that there is also a wide range device complexities and many devices require multiple and complex steps for it to be used correctly. Perhaps the classic example of complexity is the MDI, which not only requires the patient to follow a number of steps in the use of the MDI but also requires them to undertake the particularly difficult manoeuvre of actuating the MDI just as they are inhaling through the mouthpiece.
Contrivance is the conscious, or unconscious, decision to do something different even when having the knowledge of what should be done. A good example of contrivance is for a patient demonstrating a good technique with a spacer and an MDI in the clinic but in the home environment choosing not to use the spacer.
The concept of compliance requires the conscious engagement of the patient to understand the rationale behind the medication, the consequences of not taking the medication as intended or of incorrect or improper use of the device, and the long-term benefits of taking the medication as intended along with improved quality of life.
The problems in achieving the intended outcomes can be summarized as follows:
Lack of a coordinated focus on the management of asthma and COPD: specialist training in device usage and the importance of compliance. Patient-to-patient variability in the use of DPIs: inspiratory flow rates, respiratory volumes and respiratory “work.” Slow onset of action for inhaled corticosteroids in asthma: no clear relationship between taking the drug and the therapeutic benefit in minds of patients
In countries such as Finland with a coordinated focus on the management of asthma and where asthmatics are seen by specialists who can address issues of competence and contrivance, the improvements in all outcomes for asthmatics have been very impressive. However, in many other countries the same dramatic benefits have not been seem because many, if not most, patients do not receive adequate instruction and, importantly, re-instruction on the use of the medication and the device.
Although the need to ensure that patients use current devices effectively—device compliance—is one challenge for clinicians,(10,11) an equally great challenge is to persuade the patients to take medications such as inhaled corticosteroids regularly. Regimen compliance—taking medication according to the recommended regimen—is poor in almost all therapeutic areas, including oral therapy and does not appear to be significantly worse for inhaled therapies. Regimen compliance is not a key issue for short-acting β-agonists that provide rapid relief within a few minutes but is certainly a major issue to the much more important classes of drugs, inhaled corticosteroids, long-acting β-agonists and long-acting anticholinergics, which substantially reduce the day-to-day hindrance of asthma, and decreased exacerbations, hospitalizations, and missed work or school; they also provide improved quality of life for both COPD and asthmatic patients, provided, of course, they are taken regularly.
The slow onset of action of inhaled corticosteroids in asthma means that there is not a clear relationship between talking the drug and the therapeutic outcome in the minds of the patients. Moreover the effect of missing doses or poor device competence, contrivance, or compliance can lead to a rapid loss of control so that patients probably do not achieve maximal benefit, and this can often be interpreted by the physician as increasing severity of the disease.
The evidence available at present suggests that device compliance can be addressed reasonably effectively by the physician or nurse, although education and contact with medical services seems to have little positive impact on regimen compliance.(12) More recently, two studies have indicated that feedback regarding the adherence to a regimen together with reminders such as a built in alarm can have a positive impact on regimen compliance.(13) Crucially, these small pilot studies were not designed or powered to show improvements in clinically relevant outcomes and further work is required.
Those developing some of the newer devices have started to address the issues of compliance and have developed devices that are easier to use effectively and that include options for providing feedback, reminders, and/or monitoring of compliance.(14) In part, this has been out of necessity in the case of systemic drug delivery of potent peptides such as insulin as variable drug delivery can have unfortunate and serious consequences.
There appears to be some barriers within the pharmaceutical industry to develop more innovative delivery systems that can address the issue of device competence and compliance:
“Necessity” seems to be the only driver. Insulin required low variability of delivery and this was effectively achieved, although, in the case of Exubera, it was not a commercial success. Competitive advantage can serve as a driver. New devices for asthma and COPD may be prohibitively expensive. This then begs the all-important question of who pays—health providers, the pharmaceutical industry, or the patient. The pharmaceutical industry is regarded by many as conservative with “precedent” ruling the decision-making process and a “sustaining” attitude of if it's good enough for the past, it's good enough for the future.
However, some pharmaceutical companies have recognized a commercial and competitive advantage by providing device and delivery system enhancements such as inhaled antibiotics for cystic fibrosis; this was in direct response to feedback from clinicians on the therapeutic benefits that could be achieved by delivering this drug directly into the lung.
The development of completely new devices for conditions such asthma and COPD is usually considered to be prohibitively expensive, and investment is generally focused on new molecules to obtain a commercial advantage, protected by patents, or “me too” generic devices, which generally have similar weaknesses as the reference device.
In summary, clinicians and patients do not need more efficient devices but simply need devices that are:
Intuitive to use so patients will and can use them effectively Provide feedback and/or information regarding compliance
It would not be necessary to build features such as feedback and compliance monitors into a device that would inevitably significantly increase the cost, the same benefits could be achieved with an add-on device that would not compromise the basic device, and this would obviate many of the potential hurdles that would inevitably be raised by regulators if they were an intrinsic part of the device. Such devices would not be needed for all patients but could be invaluable in the management of many patients who require added assistance in the use of a fairly complex drug delivery system. However appropriate, well-designed studies are required to show whether such approaches do indeed impact on clinical outcomes.
The Future of the MDI
Current state of art
Since its introduction in 1956, the pressurized metered dose inhaler (MDI) has been the most widely used delivery system for the treatment of asthma and COPD, but over the last half century there have been many sustaining developments of the MDI. For example, although the basic subsystems of modern HFA formulated MDIs are the same as their earlier CFC counterparts, each subsystem has been substantially improved in terms of both basic component design and in the enhanced quality of manufacture of subsystems and the product itself.
Increased regulatory requirements, particularly during the late 1980s and 1990s, and the transition to HFA propellants have been primary drivers of these innovations, although much of that innovation can only be described as sustaining—there has been no innovation in the MDI field that could be described as disruptive or indeed revolutionary.
Some examples of these sustaining innovations are:
Metering valves have been improved to function with HFA propellants to meet more stringent regulatory requirements on dosing uniformity and to reduce the levels of extractables/leachables that can potentially contaminate the product. Canister technologies, for example, novel fluorinated coatings, have been developed to reduce drug degradation and physical deposition of the drug on the internal surfaces of the canister. The transition to HFA propellants led to the development of MDIs with increased lung deposition, technologies to help control residual particle size and to the development of MDI actuators with improved delivery efficiency. Dose counters have been incorporated into the basic MDI to enhance patient compliance through a clearer indication of the quantity of remaining medication.
Although there are additional improvements in development, it is likely that the future of MDIs will be driven more by market factors than by unmet technical requirements, and in this context it is also likely that any innovation in the basic MDI will be of a sustaining nature rather than disruptive.
So, what will determine the future of the MDI and how will these factors shape the next 25 years of MDI use?
Factors influencing the future of MDIs
Market developments
It is most likely that market forces will play a key role in determining the future technical development of the MDI. For example, there are significant cost pressures in developed countries and the desire for Western style medication in developing countries, and these should secure the future of MDIs as they are inherently of lower cost to manufacture of any of the current-day alternatives delivery systems with multidose capability—particularly on a cost-per-dose basis. Thus, this largely generic market is expected to be a major driver of growth.
World Health Report (1998)(15) estimates there are 300 million asthma and 230 million COPD sufferers worldwide, of which many are in developing countries, and it is estimated that up to 50% of smokers will develop COPD to some extent.(16) Given the price-sensitive nature of these markets, they should provide significant opportunities for future MDI growth. It is expected, therefore, that many NCE developers will choose to utilize cost effective technologies, such as the MDI, in order to develop products that will be commercially viable in both developed and emerging markets.
It is also expected that there will be expansion into new therapeutic areas where the MDI may be better suited than other alternatives, for example:
Moving back to the delivery of drugs for allergic rhinitis; MDIs offer several benefits over aqueous sprays The use of the MDI for the delivery of drugs by inhalation for systemic activity; migraine is a likely therapeutic target for this technology Local delivery of protein and peptides to the lung
It could be argued that the future of MDIs is to some extent dependent on the use of this delivery system for the treatment of diseases other than asthma and COPD. MDIs were once a mainstay in the treatment of allergic rhinitis but were replaced with aqueous pump sprays as the Montreal Protocol did not provide a ”medical use exemption” for allergic rhinitis because it was believed there was an alternative and equally effective delivery system through pump spray products. Now that the industry has developed alternative non-CFC propellants, HFA 134a and HFA 227, and has gained considerable experience in the formulation of the MDI using these propellants with a wide range of drugs, the barriers to adoption of the MDI for the treatment of allergic rhinitis have been largely removed.
There are also several benefits for the use of the MDI; preservatives are unnecessary as the HFA formulation itself is nonsupportive of microbial growth, the ability to extend developed MDI formulations for new indications and greater patient acceptability of MDIs over aqueous pump sprays. It is noted that there are several products that are currently under development for allergic rhinitis using the MDI system.
The use of the inhaled route of administration for rapid onset of action for migraine treatment and the localized delivery of proteins/peptides for lung diseases will also provide additional niche markets for the MDI.
Many of these therapeutic areas will require significant technical innovation not only to develop a stable and robust product but also products that are manufacturable and marketable.
Political dynamics
Any future technical development of MDIs must be viewed against the political dynamics that exist with respect to the global warming potential of HFA propellants (HFA 134a and HFA 227) for inhalation, and these could influence the future of MDIs. It should be noted that the environmental impact of HFA propellants is much less established than for CFC propellants. Although MDIs constituted only a small percentage of the total CFC use, CFCs were the overwhelming anthropogenic contributor to stratospheric ozone depletion, and as such, it was imperative that CFCs were eliminated.
However, there is a much weaker link between the HFA propellant use and global warming. HFA propellant use is only a small contributor to greenhouse gas emissions and amounts to approximately 3% of total emissions of CO2 equivalents in 2007.(17) Additionally, of this total HFA propellant use, MDIs constitute a very small percentage of HFA use (<2%). Thus, the contribution of HFA MDIs to global warming may be considered negligible. There are wildly varying estimates of future HFA emissions,(17) but these estimates are highly speculative. Furthermore, it has not yet been demonstrated that HFA MDIs have any higher global warming potential than DPIs because the full array of processes involved in device manufacturing—the so-called cradle to grave of manufacturing plastic and metal components—has not been analyzed, quantified, and balanced against alternative delivery systems; such an analysis should be included in a thorough assessment and decisions should not simply focus on the contribution of the HFA propellant to global warming.
Despite the clear scientific justification for eliminating CFC propellants, their elimination from MDIs was only achieved some 21 years after the signing of the Montreal Protocol. Because there is a far weaker scientific rationale for the elimination of HFA propellants from MDIs, it is highly unlikely that any form of restriction in the use of HFA propellants for MDIs will occur for a very long time—if at all.
Technical opportunities
There are a number of technical considerations that will influence the future of MDIs. These can be considered in the following categories of development:
General MDI performance Improved suspension stability Enhanced metering valve performance Expansion of the “performance” space
MDIs will continue to be refined with an emphasis on expanding the range of drugs that can be delivered using MDIs and improving dosing consistency.
Fine particle fraction is viewed as the principal determinant of the “clinical” performance of inhalation systems. MDIs have been recognized as providing a high fine-particle fraction, and there will be a drive to achieving fine particle fractions well in excess of 50%. Dose-by-dose counting needs to be universally introduced, allowing better patient compliance through a clear knowledge of the number of doses remaining and already taken.
Future MDIs may also use fast fill/fast empty (FFFE) valves or other designs to overcome priming effects, to optimize further elastomers to reduce leachables and extractables, and valve and canister coatings to reduce drug deposition for suspension MDIs and drug degradation for solution MDIs.
There has been limited market interest in novel actuator technologies because delivery efficiency from current HFA MDIs has been regarded as adequate. However, simple cosmetic improvements to MDI actuators are likely in order to gain and maintain market differentiation. High efficiency actuators, for example, Map Therapeutics' Tempo® inhaler may be used on products for applications where cost is less critical or where it is important to minimize oropharyngeal deposition. Although the incorporation of dose counters may be delayed in some developing markets where cost is a critical determinant, ultimately dose counters will be widely used even in markets where they are not currently required from a regulatory perspective.
Breath-actuated MDI systems have been available since the 1970s, but have not been widely commercialized due to increased overall product cost. However, the prevalence of breath-actuated MDIs may increase as companies seek market differentiation, as managed care providers require improvements in pharmacoeconomics gained through improved patient compliance, and as simpler breath actuation technologies are developed.
There are huge opportunities in formulation technologies and although many of these were developed a decade or so ago, their emergence into MDIs is certainly on the horizons of this article. Some of the technical opportunities are listed below:
Novel excipients: HFA soluble excipients for example, oligolactic acid (OLA);(18) submicron bulking excipients; PulmoSphere®.(19) API particle engineering: SAXS; SCF approaches. “Hardware” improvements: improved metering valves through surface coatings and minimizing silicone content; particulate semipermeable matrix.
An example of the significant improvement that can be made in suspension HFA formulations through the use of HFA soluble excipient stabilizers is shown in Figure 4 with reference to the use of OLA.

Impact of addition of oligolactic acid (OLA) on suspension stability of dispersions in HFA-134a (3M, St. Paul, MN). The left vial is the drug suspension in the absence of OLA, while the right vial contains OLA excipient.
Such approaches offer the opportunity to make step changes in the physical stability of suspension formulations and thereby offering a substantial improvement in delivered dose consistency and, potentially, fine-particle fraction.
The porous particles offer an equally impressive improvement in the physical stability of suspension formulations, but clearly require additional formulation excipients to create the porous structure (see Fig. 5, courtesy of Novartis Pharmaceutical Corp., San Carlos, CA).

Dispersion of porous particles, such as those prepared using the PulmoSphere™ technology (Novartis Pharmaceutical Corp.), enable stable suspensions of drugs in HFA propellants.
Future MDI formulation technologies are likely to incorporate new formulation technologies that allow for increased fine particle dose and increased dosing consistency. Numerous formulation technologies have been developed to an enabling stage for suspension formulations, using porous particles, HFA soluble excipients, and suspended excipient particles. Solution formulations with dissolved excipients to manipulate the particle size distribution of the emitted dose and sustained release drug delivery have also been developed but none to date have reached the market.
There are also major opportunities for enhanced MDI performance through developments in the metering valve and canister systems. It is well known that drug deposition on the internal surfaces of the metering valve and canister can reduce the amount of drug in suspension and thereby impact negatively on dose content uniformity and dose through life consistency; MDI to MDI variability can also be impacted negatively.
Coating the internal surface of the canister with a highly hydrophobic polymer can significantly reduces drug “loss” by adsorption onto these internal surfaces. This is shown dramatically in Figure 6 for budesonide where there is a reduction of around 75% of drug deposited initially and after storage.
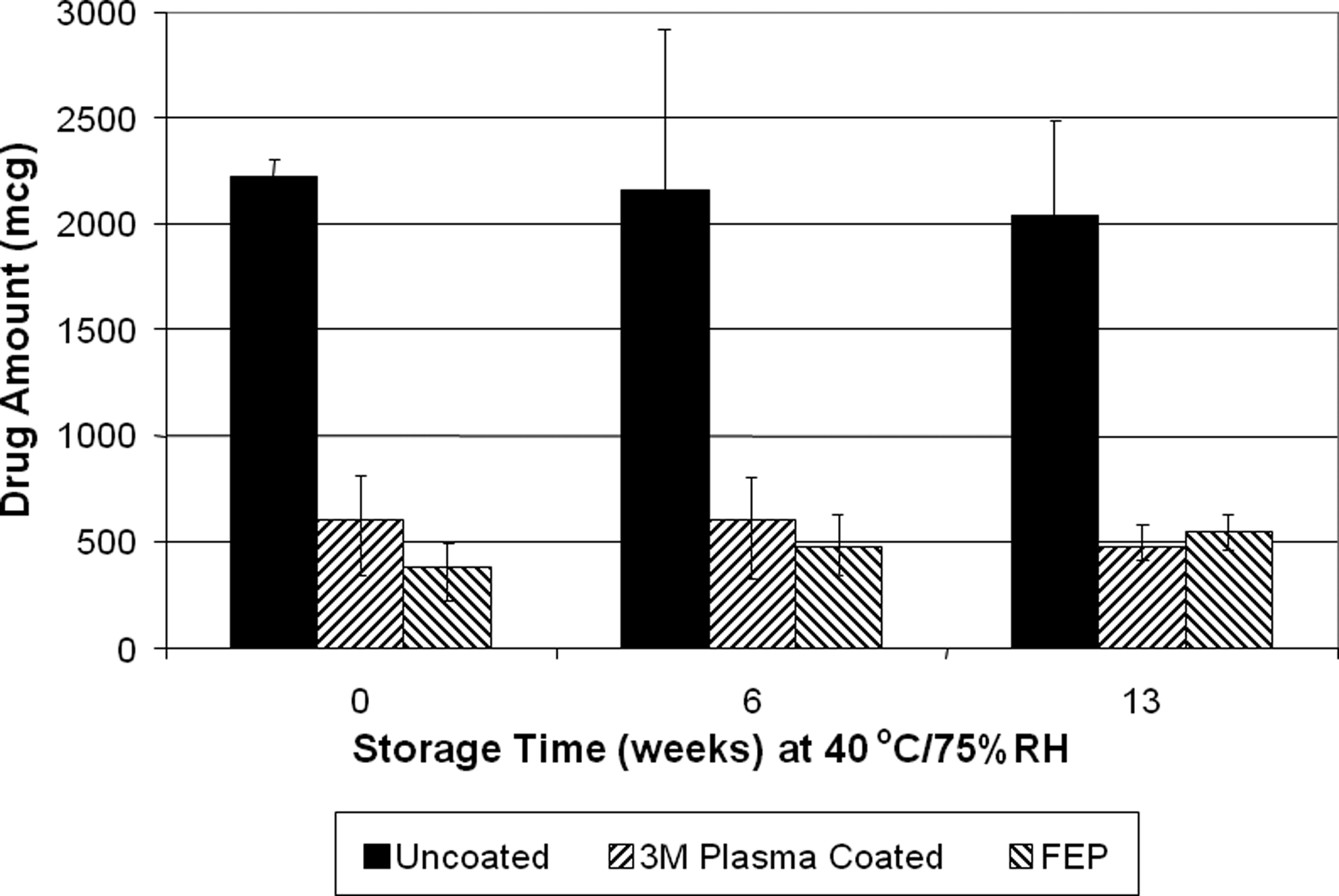
Impact of coating of pMDI canisters with a hydrophobic polymer on reducing adsorption of drug on canister surfaces.
The concept of FFFE metering valves has been around for several decades without market success. The FFFE approach, however, does offer a number of key benefits—the main benefits being resistance to loss of prime (the loss of propellant and drug contents from the metering chamber of the valve between dosing episodes thereby reducing the contents of the “next” dose delivered), a reduction in the dosing through life trend that is often seen with standard metering valves and reduced dose content uniformity through the in-use life of the MDI.
The FFFE metering valve concept still requires a relatively stable suspension formulation, although it is less sensitive to the physical stability of the formulation than are standard metering valves. Although the patient is instructed to shake the canister before use, any pause prior to actuation of the metering valve could lead to some flocculation with sedimentation or creaming as shown for the latter in Figure 4 above.
There has been huge progress over the last 2 decades in reducing the amounts and nature of extractables and leachables from the elastomers used in metering valves. The move to the so-called “white” elastomers provided the first step through the removal of carbon black as a reinforcing agent in the compounding of the rubber formulation that served to eliminate the parts per million and parts per billion of polynucleararomatic extractables—some of which were highly carcinogenic. Bespoke synthetic elastomers have provided yet another incremental but significant step in the reduction in extractables and leachables.
These sustaining improvements in the quality and integrity of the elastomers used in metering valves have been stimulated by regulatory pressure, the need to provide effective sealing performance in the presence of the new HFA propellants, and to provide good metering valve performance under circumstances where there is little natural lubrication of the moving components of the metering valve due to lack of HFA soluble excipients/stabilizers.
Other more significant changes to the MDI such as unit dose MDIs and adjustable dose MDIs are technically feasible but would require specific drug and product delivery rationale to drive the developments forward, but these may be eventually commercialized for niche opportunities.
Some of these are certain to reach the market in the future. However, future MDI formulation and hardware innovations will be balanced with the desire to maintain two primary benefits of the MDI system—low cost and regulatory familiarity with this delivery system. Thus, as a result, it is likely that future MDIs will not be radically different from existing MDIs and any of the innovations made in this area will only be of a sustaining nature.
In terms of a prioritized “technical wish list,” the two key areas would be first to provide a universal metering valve, which is formulation independent and can be used irrespective of the propellant (HFA 134a and HFA227), the drug content, and chemical structure, and any excipient that may be required to stabilize the formulation. The second key area would be the ability to make more drugs into solution aerosol formulations and thereby eliminate any consequences of flocculation, creaming or sedimentation found in suspension formulations. These technical innovations could not be regarded as anything other than of a sustaining nature, although the introduction of a universal metering valve from one manufacturer may be regarded by other manufacturers as somewhat disruptive.
There are, of course, some “technical solutions” that are available but have yet to gain mainstream market acceptance; of these it is worth highlighting the following:
Breath actuation to increase substantially patient coordination FFFE valves to reduce the impact of flocculation, creaming, and sedimentation Lower number of doses for MDIs (e.g., 30 doses or less) Delivery of proteins and peptides (along with breath actuation to reduce concerns about patient coordination) Particle engineering technologies (e.g., PulmoSphere™) Sustained release (e.g., the use of OLAs) Improved efficiency actuators to increase fine particle fraction, provide enhanced lung delivery, and potentially to target specific parts of the lung
Any one of these technical opportunities would not in itself transform the MDI in a disruptive sense, but combining some key technical solutions into an MDI could achieve a substantial improvement, which although sustaining in nature, could feed new life into the MDI and set it apart for another very successful 25 years.
The Ideal Set of Attributes for a Pulmonary Device
By way of background, it could be argued that the value of the attributes of a pulmonary device should be judged by how successfully the patient can use the device to control their symptoms and, perhaps controversially, it could also be argued that the “in patient success” is always the final arbiter.
However, a significant part of the patient's “normal” behavior is often omitted when considering device usage from a patient perspective. An idealized view is taken where it is presumed that the patient will always follow the Instructions for Use (IFU) implicitly no matter how far from “normal” practice this may be.
The potential for incorrect dosing due to the differences between the patient's “normal behavior” and that which is required by the IFU is where more attention should be focused by inhaler device developers. It is possible to use this approach to distinguish between device attributes, and to define a best set of attributes to meet the final goal of successfully controlling the patient's symptoms in a compliant manner without inducing any degree of contriving behavior through poor design or through the ignoring of patient needs.
Present state of art
The goal of an inhalation device to control patients' symptoms must include the broader goal of ensuring a supply of the product—the cost of goods must be in line with clinical benefit and competition, providing a safe and efficacious dose at a reasonable cost. This is concordant with the FDA, which speaks of safety, efficacy, and cost as primary drivers. All other project drivers in designing and developing a pulmonary delivery device are subsets of these three; for example, the ease of manufacture can be viewed as a subset of cost.
Setting safety aside as an underpinning criterion of all medical/drug product developments, we can concentrate on efficacy. Efficacy can be broken down into pharmaceutical effect and patient behavior. Pharmaceutically, the patient expects the drug to deliver a net benefit; the control of symptoms must provide an improvement in lifestyle above the unwanted side effects. There is little drive to control asthma symptoms if the therapy causes other unfortunate and significant side effects.
The concept of the effect of patient behavior on efficacy is now discussed in terms of this being the main driver for device attributes. Patient behavior referred to here is both the immediate short-term behavior (when the patient is actually taking the dose) and also its impact on long-term compliance; does the patient persist with the therapy over the long term?
In order for a device to provide an efficacious dose the patient must use the device within the constraints of a set of conditions. These can be defined as:
Having an inspiratory flow profile within an acceptable range, and, the device used within the limitations set by the IFU—the term “IFU normal” will be used to define the limitations defined by the IFU.
Beyond “IFU normal” there are variations in behavior that may well be described as typical human behavior. This typical human behavior would include how the inhaler is orientated, how the inhalation sequence is timed, how or if the device is shaken, plus a number of other actions that the patient would be expected to do when using an inhaler.
During device development, the developer is obliged to ensure efficacy within the limitations of the “IFU normal” but can disclaim the effect of typical human behavior with the IFU. Almost perversely, any behavior outside the “IFU normal” is considered accidental misuse, and although the effects are often characterized, there are many modes of accidental misuse that are well within the range of typical human behavior that will result in a critical error—one that would result in an incorrect dose being delivered.
It has been shown that patients, when presented with respiratory devices and the IFU, will make critical errors in usage (Fig. 7). Following one-to-one training the number of critical errors reduces but still remains relatively high; for example, approximately 10% of subjects when using GSK's Diskus® device still made critical errors even after training.(20) It has also been shown that DPIs cannot be used interchangeably without specific training.(21)

Critical errors observed using various dry powder inhalers in a patient handling study, before and after specific training.
It is possible to review pulmonary devices by group assessing the possible differences between IFU normal and typical human behavior, and to consider how many opportunities exist for critical errors to be made by the patient during use. The opportunities for critical errors are analogous to a “minefield”; the more opportunities that exist then the more likely patients are to encounter one. If there are no opportunities for critical errors then the likelihood of short term compliance will increase and the physician can have greater confidence that the patient will be able to get an efficacious dose during their normal use, which will include typical human behavior.
A number of device groups have been considered using this approach:
MDI Breath actuated MDI Reservoir DPI Premetered DPI Breath-actuated premetered DPI. (Breath actuation in this example refers to the opening of a dose in response to a breath trigger and not simply that breathing is required to entrain the dose. In this definition GSK's Diskus® would not be breath actuated as the dose opening is a manual operation.)
The review involves identifying the steps called up in the IFU and evaluating the effect of varying these steps (assuming the patient did not follow them exactly). In addition, a number of standard misuse conditions have been included:
Storage: storage can affect dose consistency, an example being loss of prime in an MDI, requiring repriming and thus more IFU steps Double dosing: making a dose ready and then not taking it should not have any effect on subsequent dose accuracy Random actuation: the possibility of misuse by completely misunderstanding the requirement to breathe through the device, anecdotally applied to MDIs, or similar failures Incorrect sequence: a simple reordering of IFU steps
Table 2 shows an interpretation of the critical IFU steps for a generic MDI, along with the standard misuse conditions. Alongside each is an opinion of the potential effect of varying each of these critical steps. Opportunities for critical errors include timing with respect to breathing, shaking, orientation, relative timing of sequence, poststorage use and incorrect sequence, and random discharge of the dose.
It is interesting to note that introducing breath actuation into the MDI (Table 3) removes only one opportunity for a patient to perform a critical error, and this is with respect to the inspiratory cycle and the actuation of the canister (breath timing).
The IFU sequence is simplified in the case of a reservoir DPI, as exemplified by AstraZeneca's Turbuhaler®. A typical IFU sequence would include: open, orient, actuate (twist base), breathe out, breathe in correctly, and close. The simplified IFU allows less opportunity for the user to create critical errors as shown in Table 4.
In the case of premetered DPIs, for example GSK's Diskus®, there is a further simplification of the IFU. A typical sequence would include: open, push lever, breathe out, breathe in correctly, and close. Table 5 shows that there are a number of opportunities for critical errors to be made; these include orientation, shaking, breathing, and double dosing and, potentially, the timing between stages.
It is notable that the majority of the potential critical errors in the premetered DPI occur in the time between the dose being opened, and the patient breathing in. It is possible to minimize the time between opening the dose and breathing if a breath actuated mechanism is used. This type of device would potentially eliminate patient errors resulting from orientation, shaking, breathing, double dosing, and the timing between stages by organizing the dose containment system in a manner whereby it is only opened in response to the correct inspiratory flow; thus, the operating sequence would be Open–Breathe–Close. Such a system is depicted in Table 6.
The above creates a DPI device with attributes that enable an Open–Breathe–Close sequence and reduced sensitivity to the usual human errors. Although no proof is offered, it is considered likely that this would provide a step change in short-term compliance compared to existing marketed devices. It could also be construed that such a device, in combination with clear additional feedback features, would be an improvement in securing longer term compliance. The patient's acceptance of any given device has been shown to have a strong correlation to long-term compliance,(20) and hence, the need to understand further the complexity of patient acceptance of a device beyond the belief of its safety, reliability, and ease of use. It is entirely possible that a device that eliminates opportunities for user error could improve acceptance, thus improving the likelihood of long-term compliance.
What Needs to be Done?
Although there has been huge progress over the last 25 years in introducing HFA propellants in place of the ozone-depleting CFCs, and all the attendant subcomponent refinements, the introduction of true multidose DPIs, a better understanding of the formulation factors affecting DPI performance, the development of a raft of alternative small-particle formation technologies and a much better clinical perspective and understanding of the key patient interaction with devices, it is clear there are still many opportunities for innovation and the creation of a so-called “ideal” inhaler device. All of the progress made during this period has been of a sustaining nature; none, it is argued, can be regarded as disruptive, and as for revolutionary innovation in the field of inhaler devices, it is fair to say that it has not been seen yet.
There are a multitude of opportunities for innovation in inhalation devices but for this innovation to be driven there needs to be appropriate drivers to innovation; introducing innovation for innovation sake is not a sustainable driver. Often the best drivers of innovation are specific technical and scientific needs and the resolution of problems. This field in particular is littered with the remains of technology and innovation for technology and innovation sake, where the technology and innovation is not aligned to a need or solution of a problem—the so-called technology looking for an application. Take the patent literature for DPIs; there are literally hundreds of patents for DPI devices ranging from the interesting to the bizarre, and then look at how many discrete DPIs are currently marketed and how many are likely to be introduced over the next 5 years, 10 years, and 25 years; the answer is a handful with very few digits.
In answering the question “what needs to be done?” this can be approached at a number of levels. First, we can take the traditional approach and consider what the weaknesses and failings are in the current delivery systems of MDIs, DPIs, and portable “nebulizers.”
MDIs
As we have seen in the foregoing, an overriding requirement for an MDI is to deliver a consistent dose of drug on each and every occasion the dose is discharged irrespective of patient peculiarities during use of the MDI. Few MDIs meet this requirement in real terms. There are a multitude of contributing factors to achieving the consistency required ranging from the metering valve and associated components to formulation science of particle stability and particle/droplet formation.
It is well known and understood by all who have worked in the development of an MDI that the delivery of drug to the lung is critically dependent upon the patient actuating the MDI during the inspiratory cycle; that is, discharging the dose from the MDI while breathing in, and this is not an easy manoeuvre to coordinate for many. The opportunity for a patient to deliver a “zero” dose is real and does exist, the opportunity for delivering only a partial dose (whatever that may be) is huge, whereas the opportunity for delivering the intended dose is regarded by many as only slight. In the case of a patient taking an oral product, say a tablet, the process is binary—the tablet is either in the palm of the hand of the patient or is traveling down the digestive tract of the patient to be absorbed; the opportunity for receiving only a partial dose under these circumstances is nonexistent. So, given the life-preserving nature of medication for the treatment of asthma and COPD, why is it acceptable to continue to use a drug delivery system with such significant opportunities for patients to receive less than the intended medication?
One solution is the use of a breath-actuated mechanism whereby the dose is only discharged while the patient is inhaling. Breath-actuated devices have been developed and marketed for at least 2 decades but the barrier to broader adoption has been cost. For breath actuation to become a reality, the cost of adding this important dose controller must be either low in real terms or any additional cost absorbed by the manufacturer. Clearly, there is the opportunity for add-on cost sharing by the manufacturer and the payer.
What needs to be done for MDIs? (1) Provide an MDI that can perform consistently during the most exacting conditions of actuation by a patient; (2) provide cost-effective breath actuation to eliminate the need for patients to coordinate actuation of the MDI with breathing in.
DPIs
Although DPIs are widely regarded as breath actuated, this does not mean that a consistent dose is delivered to the lung on each and every occasion. Many factors come into play to determine exactly how much drug is inhaled and deposited within the lung. The more important of these patient related factors include peak inspiratory flow, initial inspiratory acceleration, volume of air inhaled, lung size, lung condition, oropharyngeal architecture, and degree of mouth-opening during inhalation. There are other factors that may also come into play.
From the DPI formulation perspective, there are also many contributing factors determining how much drug is delivered to the lung and these include the ease/efficiency of drug particle release from a carrier-based system, the nature of the carrier, the efficiency of break up for those formulations based on drug particle pelletization, particle/particle interaction, the inherent cohesive nature of the drug substance, and others. In reality, it is not possible to detach device-related factors from formulation-based factors as the two are inextricably linked. However, as discussed in the preceding section, there some key design features for DPIs that can help reduce patient error and aid compliance.
What needs to be done for DPIs? (1) Provide a DPI with a simple three-step operation: open–inhale–close, which can take into account typical human behavior; (2) provide a formulation and device combination that is wholly independent of patient inspiratory flow conditions over the widest possible range.
Portable nebulizers
Although portable nebulizers have not been discussed in this article, they may have a key role for some molecules and therapies of the future. What is vital is that the portable nebulizer must meet all the patient-important characteristics presented for MDIs and DPIs; they must eliminate as far as possible the various typical human behavior encountered and must provide a consistent and reproducible dose on each and every occasion.
In summary, what needs to be done for inhaler devices of the future is the provision of delivery systems that facilitate compliance of medication delivery, and this should take into account both typical human behavior and the performance of the inhaler system in delivering a consistent and reproducible dose to the lung when used over the widest range of patient processes.
Footnotes
Author Disclosure Statement
No conflicts of interest exist for any of the authors with respect to the content of this review.