
Abstract
Abstract
Background:
Inhaled corticosteroid (ICS) therapy has improved the quality of life (QOL) for many asthmatics and reduced mortality rates associated with asthma. However, some patients do not obtain therapeutic benefit despite satisfactory adherence.
Objectives:
To determine whether asthmatic patients were using ICS devices appropriately, and to clarify relationships between these results and QOL.
Subjects and Methods:
We studied 100 adult asthmatics, divided into two groups: 50 patients consecutively registered as using DiskusR (fluticasone; D-group) and 50 consecutively registered as using TurbuhalerR (budesonide; T-group). We measured peak inspiratory flows (PIFs) using the In-Check DialR device. Subjects also completed the Asthma Control Test for evaluation of QOL.
Results:
In the D-group, no patients showed PIF below the optimal range (30–90 L/min), whereas 52% of patients had PIF ≥91 L/min. In the T-group, 6% of patients showed PIF over the optimal range (60–90 L/min), and 44% had PIF ≤59 L/min. When patients in the T-group were required to deliberately make a maximal inhalation, 14% still had PIF ≤59 L/min. The proportion of patients with poor control was significantly greater in the T-group than in the D-group. According to univariate logistic regression analyses, low PIF tended to be associated with poor asthma control in the T-group. No significant correlation was found between PIF and age in the D-group, but PIF decreased significantly with age in the T-group.
Conclusions:
Appropriate measures for patients in whom PIF has been judged as lower than optimal include adequate education for inhalation and/or changing to a different inhalation device. These measures should be kept in mind for elderly asthma patients in particular, where appropriate selection of a corticosteroid inhalation device in the early stages of therapy would also be important.
Introduction
Two types of inhaler are currently used to deliver ICS: dry powder inhalers (DPIs); and pressurized metered-dose aerosols. DiskusR (GlaxoSmithKline, London, UK) and TurbuhalerR (AstraZeneca, Lund, Sweden) are representative DPIs. With a DPI, the rate of drug delivery to the lungs depends on appropriate peak inspiratory flow (PIF) and correlates with the quantity of microparticles given off by the charge powder. To evaluate PIF, some reports have suggested that the In-Check DialR device, which can recreate the resistance encountered when inhaling with different DPI inhalers, offers the advantage of simple PIF measurement in clinical settings, and can be useful for both adult and child ranges.(1–3) The optimal PIF to inhale the drug is believed to be 30–90 L/min when using the DiskusR (3,4) and 60–90 L/min when using the TurbuhalerR.(3–5) However, some patients may not achieve sufficient PIF levels in everyday treatment, due to deteriorated lung functioning or poor inhalation technique, and thus may not receive the full therapeutic effect.
In recent years, the asthma control test (ACT) has been suggested as a simple method for evaluating patients' control of asthma.(6) A correlation with forced expiratory volume in 1 second (FEV1) and usefulness as a tool for appropriate treatment decisions,(7,8) or an indicator of future asthma exacerbation in combination with FEV1,(9) have been reported. Assuming appropriate PIF for corticosteroid inhalant to be an important factor relating to the efficacy of ICS and QOL of asthmatics, and assuming also that the correlations differ with different inhalers, improved asthma control may well be achievable by combining these two simple methods of evaluation. Furthermore, ICS is known to predispose to pharyngeal inflammation and hoarseness in adults and children, which are considered to depend on duration of ICS use and/or a type of inhalation device.(10–12) In the context of inhalation, inappropriate PIF might also concern development of hoarseness.
In the present study, adult asthma patients using ICS with the DiskusR and TurbuhalerR were studied to determine whether they had appropriate PIFs for their inhalers. The relationships between these results and ACT scores, as well as the side effect of hoarseness, were also investigated.
Subjects and Methods
Subjects
Subjects were comprised of 100 adult asthma patients making outpatient visits to Aichi Medical University Hospital, divided into two groups: 50 persons consecutively registered as using the DiskusR (fluticasone) for asthma control (D-group), and 50 persons consecutively registered as using the TurbuhalerR (budesonide) for asthma control (T-group). No patients were using combination medications of ICS and long-acting β2-agonist (LABA) with the following devices, fluticasone plus salmeterol via DiskusR or budesonide plus formoterol via TurbuhalerR. In the present study, three medical doctors (i.e., K.B., T.Y., and E.Y.) were involved in the prescribing. Decisions on whether the subjects were prescribed either DiskusR or TurbuhalerR had been made based on synthetic judgments of the attending doctors, so the allocation of devices to subjects was not randomized. All patients were controlling their asthma in accordance with the asthma treatment guidelines and had been trained to use inhaled short-acting β2-agonists and/or oral corticosteroid as needed in the initial stage of an asthma attack, according to the zone therapy system based on peak expiratory flow rate (PEF) values. The patients were therefore measuring morning and evening PEFs using a Peak Flowmeter MiniLightR (Clement Clarke International Limited, Essex, UK) and recording the use of all prescribed medications in a daily log. However, patients developing any degree of acute exacerbation at the time of examination were excluded.
No differences were found between the D-group and T-group in terms of sex, age, severity of asthma as judged by type and dose of control medication, rate of use of inhaled LABA (i.e., salmeterol, administered with another DiskusR), or rate of leukotriene receptor antagonist (LTRA) use. However, the rate of use for bronchodilators given orally or transdermally was significantly higher in the D-group. Overall, the majority of subjects were women, and the most common treatment step was that corresponding to the therapy for moderate persistent asthma (Table 1).
LABA, inhaled long-acting β2-agonist.
Other bronchodilators: procaterol chloride (p.o.), turobuterol chloride (transdermal), or sustained-release theophylline (p.o.).
LTRA, cysteinyl leukotriene receptor antagonist (montelukast or pranlukast) (p.o.); N.S., not significant.
Research protocol
In the outpatient examining room, patients used the In-Check DialR device (fitted with the adapter matching their DPI, i.e., DiskusR or TurbuhalerR) to measure usual and maximal PIFs. Usual PIF was measured when inhaling as if inhaling the usual medication, whereas maximal PIF was measured when the patient inhaled through the In-CheckR with the maximal force they were capable of. Each PIF was measured three times, selecting the best value. Subjects also completed the ACT (see Appendix). Permission to use the Japanese version of the ACT for this study was granted by GlaxoSmithKline as an agent of QualityMetric Inc., a copyright holder of the ACT. Compliance with the use of ICSs determined from the daily log in which the patient recorded the state of drug usage every day during the last 1 month, and was evaluated as the number of neglected uses per week. PEF of each patient was evaluated by averaging daily maximal PEF during the last 2 weeks, expressed as %prediction. We also asked the patients if they had experienced hoarseness after beginning of the current ICS therapy by questionnaire.
Statistical analysis
Data are expressed as median (range). Differences in parameters were evaluated using the Mann-Whitney U-test for comparing the two groups. Differences in proportions between the two groups were evaluated using Fisher's exact test. For factor analysis, uni- and multivariate logistic regression analyses were used. Differences with a value of p<0.05 were considered statistically significant. The ethics committee of Aichi Medical University School of Medicine approved the study, and written informed consent was obtained from all patients prior to enrollment.
Results
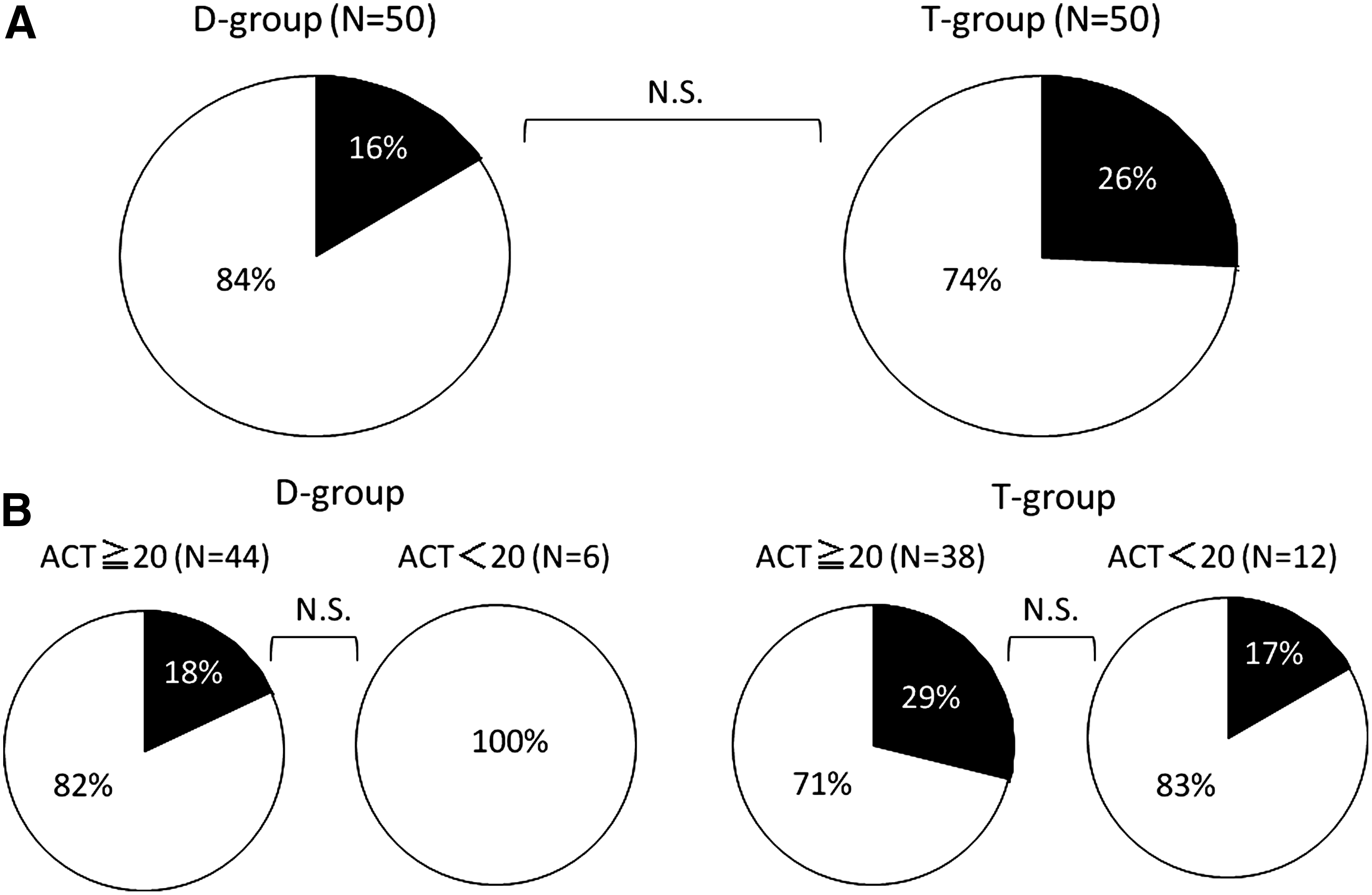
We investigated whether compliance in the use of ICSs was good or poor. “Good” was defined as never neglecting to use the inhalant, while “poor” was defined as neglecting to use the inhalant one or more times a week. Inhalant compliance was good in 84% of D-group patients and 74% of T-group patients, showing no significant difference by inhaler type (Fig. 1A). Figure 1B shows the D-group and T-group divided by ACT score (≥20 vs. <20), with the proportion of patients who never neglected their inhalant (good compliance) and those who neglected it one or more times a week (poor compliance) shown in each. No significant relationship was found between good or poor compliance and asthma control (ACT score) in either the D-group or the T-group.
(
Figure 2 shows the distribution of usual PIF and maximal PIF values in both the D-group and the T-group. In the present study, we regarded the optimal range as a PIF of 30–90 L/min for DiskusR and 60–90 L/min for TurbuhalerR. In the D-group, no patients showed PIF ≤29 L/min, but even with the usual inhalation, 52% of patients showed PIF ≥91 L/min. In the T-group, 3 of 50 patients (6%) had usual PIF ≥91 L/min, whereas only 50% achieved the optimal range of PIF. The remaining 44% had usual PIF lower than the optimal range (i.e., ≤59 L/min). When patients were required to deliberately make a maximal inhalation, the proportion achieving the optimal range of PIF rose to 64%, but 14% still had PIF lower than the optimal range.
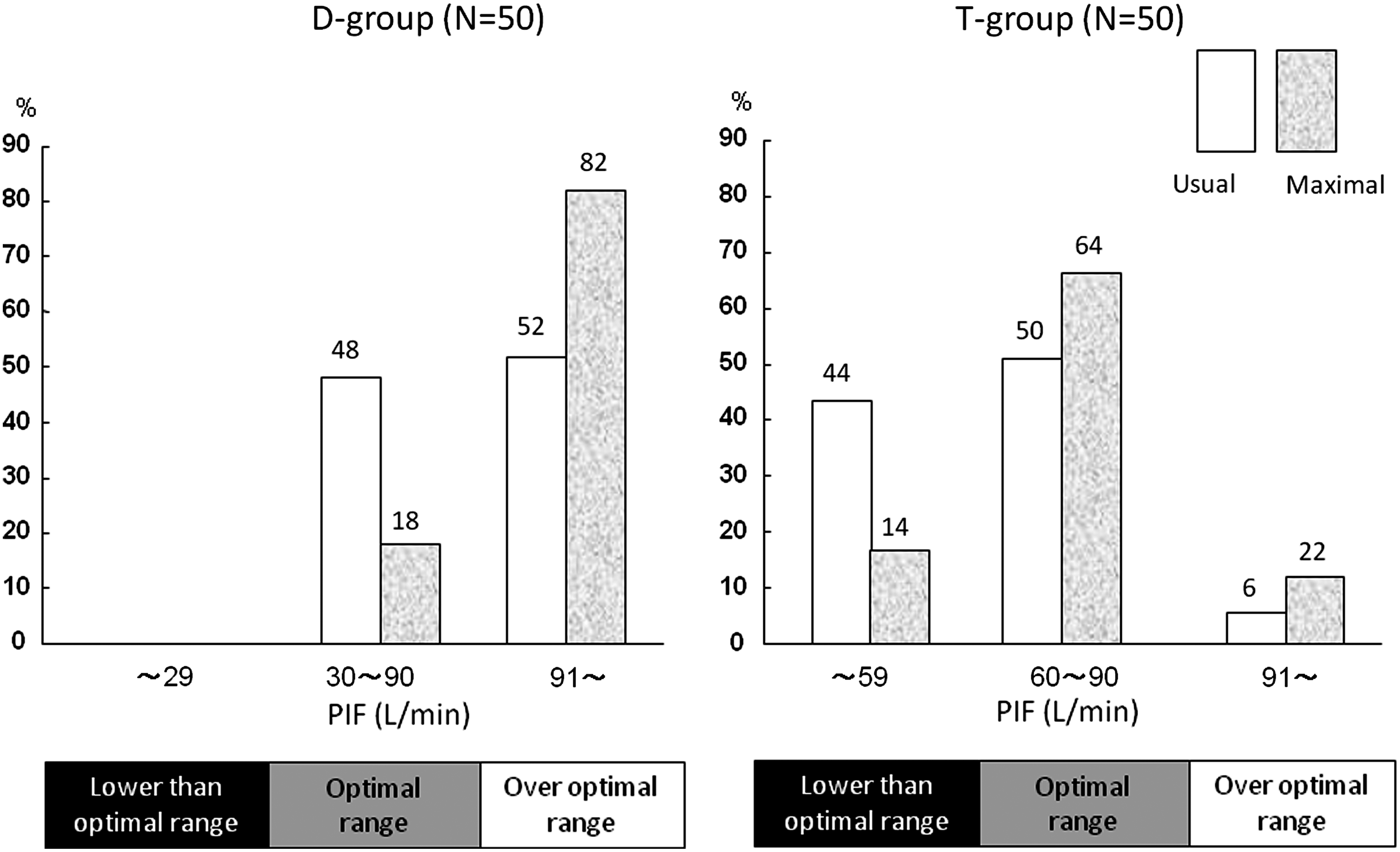
Distributions of peak inspiratory flow (PIF) for the DiskusR use group (D-group) and the TurbuhalerR use group (T-group). White bars show flow at usual inhalation strength, whereas gray bars show flow at maximal inhalation strength. The number on the top of each bar represents the percentage.
Figure 3 shows the distribution of ACT scores for the D-group and T-group. ACT scores indicate control of asthma as follows: 25 points, perfect control; 20–24 points, good control; and ≤19 points, poor control. The proportion of patients in each control category is shown. The proportion of patients with poor control was significantly greater in the T-group than in the D-group, whereas the proportion of patients with good control was significantly greater in the D-group than in the T-group.
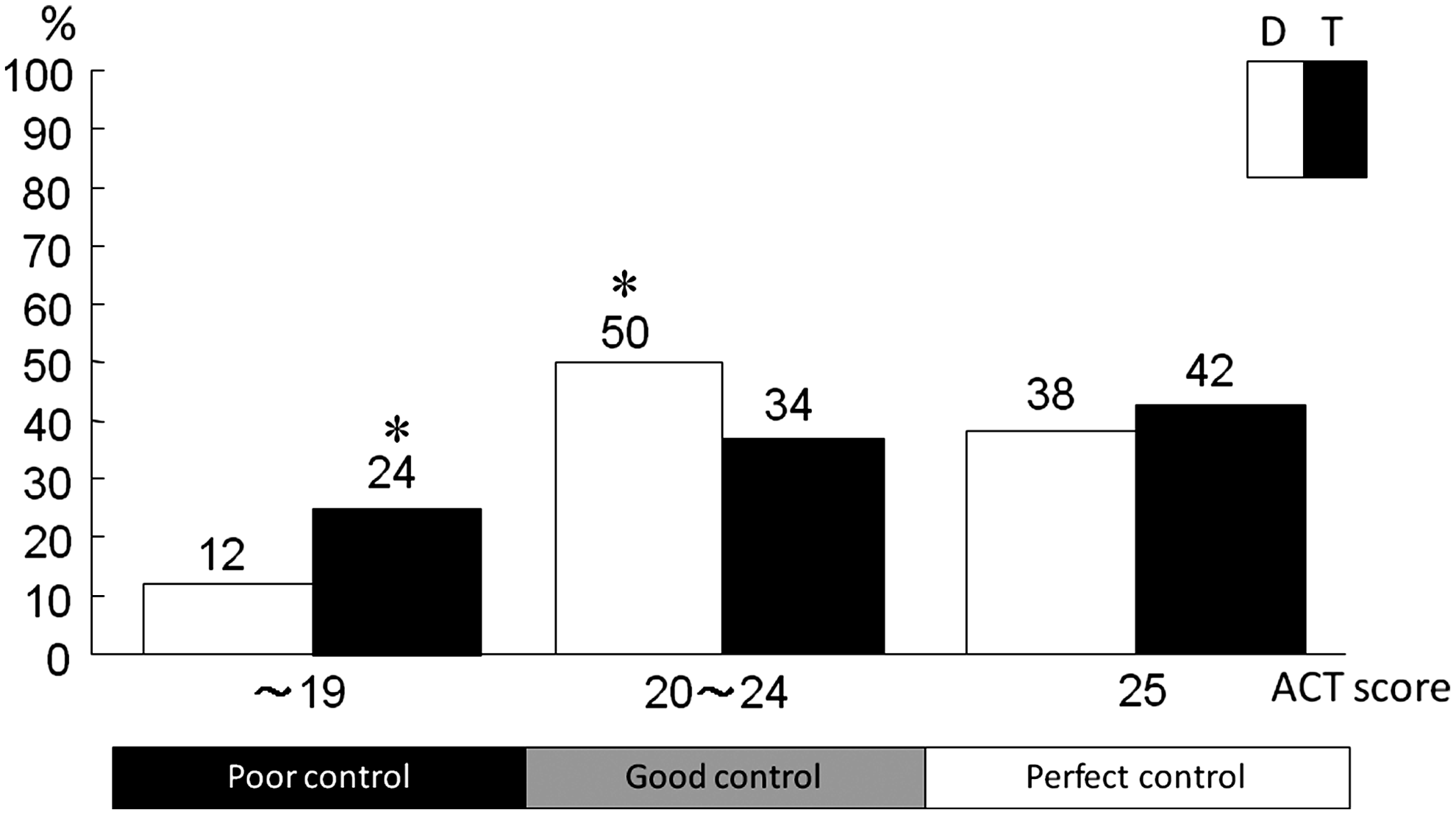
Distributions of asthma control in the DiskusR use group (D-group) and the TurbuhalerR use group (T-group). Asthma control was defined as poor, good, or perfect depending on the ACT score. The number on the top of each bar represents the percentage. *p<0.05, Fisher's exact test.
We investigated factors contributing to poor control in patients with ACT scores <20 points. We performed univariate logistic regression analysis to investigate dose of ICS, compliance, use of LABA, and use of other bronchodilators (orally or transdermally administered β2-agonists, and/or orally administered theophylline), as well as whether the usual PIF was over the optimal range in the D-group or lower than optimal range in the T-group. None of these factors showed a significant relationship to asthma control in the D-group, but PIF <60 L/min tended to be associated with poor control in the T-group [odds ratio (OR), 3.429; 95% confidence interval (CI), 0.872–13.485; p=0.078] (Table 2). Multivariate logistic analysis of these factors was performed, and when the factor %PEF ≥80% was included for the T-group, the odds ratio for the factor PIF <60 L/min changed considerably (OR, 1.712; 95% CI, 0.289–10.138; p=0.5535). This suggests that the factor %PEF ≥80% causes an interaction in the relationship between low ACT score and PIF <60 L/min in the T-group.
LABA, inhaled long-acting β2-agonist; other bronchodilators: procaterol chloride (p.o.) or turobuterol chloride (transdermal); LTRA, cysteinyl leukotriene receptor antagonists (montelukast or pranlukast) (p.o.); ICS, inhaled corticosteroid; N.S., not significant; N.A., not applicable.
Compliance with ICS was not analyzed because no patients in the D-group showed poor compliance with ICS.
Definition of low dose of fluticasone or budesonide is based on Grobal strategy for asthma management and prevention.(21)
The relationship between PIF and age was also examined to investigate factors governing PIF. In the D-group, no significant correlation was found between usual PIF and age, but maximal PIF decreased significantly with age. In the T-group, both usual PIF and maximal PIF decreased significantly with age (Fig. 4).
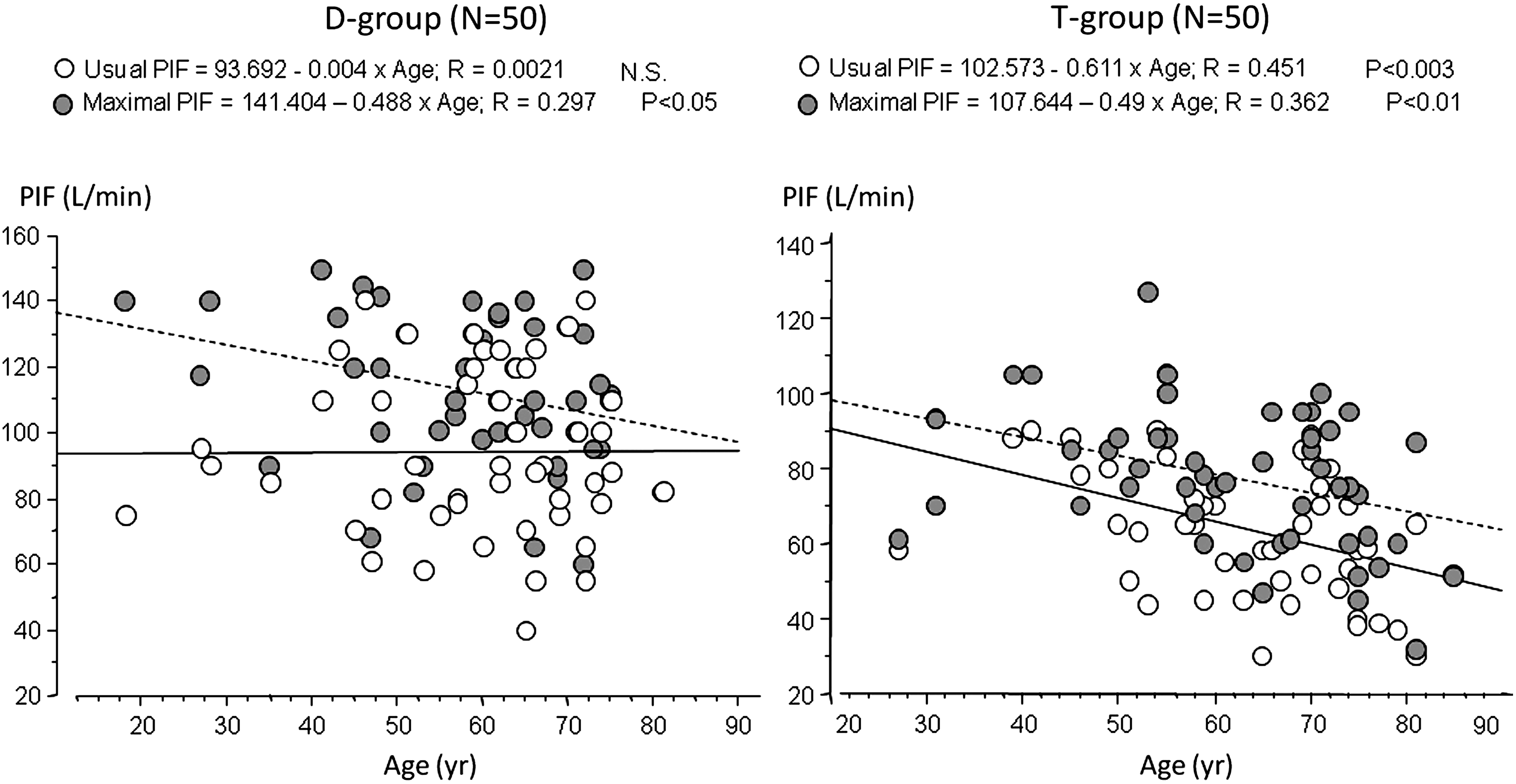
Relationship between age and peak inspiratory flow (PIF) in the DiskusR use group (D-group) and the TurbuhalerR use group (T-group). White circle, PIF at usual inhalation; gray circle, PIF at maximal inhalation.
Figure 5 shows the frequency of appearance of hoarseness (Fig. 5A and D), the relationship between hoarseness and dose of ICS (Fig. 5B and E), and the relationship between hoarseness and usual PIF (Fig. 5C and F). Hoarseness was found in 10 of 50 (20%) in the D-group and 16 of 50 (32%) in the T-group. The frequency of hoarseness was not significantly different between the D-group and the T-group. No significant relationship was found in either the D-group or T-group between hoarseness and dose of ICS, or between hoarseness and usual PIF. There was also no change in the frequency of hoarseness with use of LABA (26.1% with LABA vs. 14.8% without LABA in the D-group, p=0.4804; 35.3% with LABA vs. 30.3% without LABA in the T-group, p=0.7568).
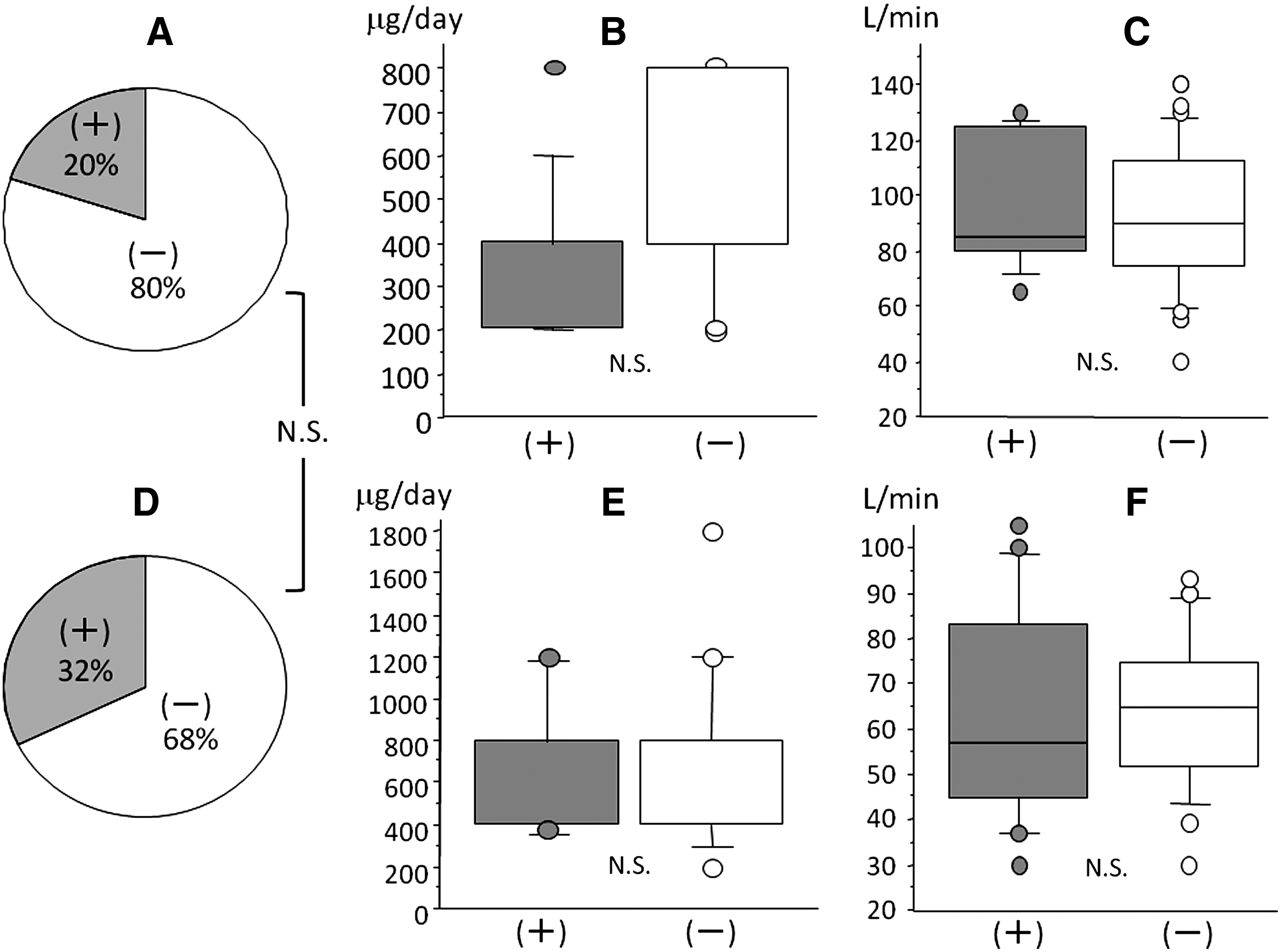
Proportions of DiskusR use group (D-group) (
Discussion
We hypothesized in the present study that inappropriate PIF might cause insufficient efficacy of ICS, which would result in poor control of asthma. Univariate logistic regression analysis revealed a tendency for low PIF to be a factor associated with poor QOL in patients using TurbuhalerR. We also found that the group using the TurbuhalerR became increasingly unable to achieve appropriate PIF levels with advancing age, whereas no reduction in usual PIF was found with advancing age in the group using the DiskusR.
In the present study, patients were not randomized into the two treatment groups, and there may be limitations for analyzing the differences between the two groups. However, we consider that the retrospective analyses comparing the two groups were valid, because the backgrounds of the patients did not differ significantly between groups except for rate of orally or transdermally administered bronchodilator use, which was not considered as a factor in poor asthma control (Table 2). Status of compliance of medications is arguably a subjective variable that is unreliable for analysis. However, information in a daily asthma log including daily PEF, status of medication use, and recorded symptoms is important for evaluating asthma control, and the reliability of the information is based on good relationships between the patient and attending doctors, which were believed to have been established in the present study.
No firm conclusion could be drawn from the present study as to why PIF decreased with age in the TurbuhalerR group. However, multivariate analysis in the present study showed that daily maximal PEF under well-controlled conditions caused an interaction in the relationship between low usual PIF and poor asthma control. Age-related reductions in respiratory muscle strength and irreversible airflow limitation due to chronic obstructive pulmonary disease (COPD), a common comorbidity among older patients, are major causes of reduced PEF, and these factors may be related to decreased PIF among TurbuhalerR users.
Children ≤4 years old have been reported as unable to obtain sufficient PIF from the TurbuhalerR, as the device has high internal resistance.(13) Our results suggest the possibility that this defect in the TurbuhalerR design also affects elderly patients. With DPIs, the rate of powder deposition on the lung periphery is governed by compound factors that include: PIF, which is affected by the internal resistance of the inhalation device; the rate at which fine particles are given off, which depends on PIF; the diameter of the fine particles given off; and the inhalation behaviors of the patient. The level of clinical efficacy of DPIs can be determined based on such factors. The TurbuhalerR reportedly gives off fine particles at a greater rate(14) and has a higher rate of lung deposition than the Diskus,(15) and clinical efficacy is expected, even assuming a PIF of 30 L/min.(5) In the present study, however, evaluation of the effects of asthma therapy using ACT scores suggested that, in the TurbuhalerR group in particular, PIF should be heeded as a possible factor in poor asthma control, although we must be careful in drawing conclusions based only on statistical tendencies. This is an issue that is not the same as compliance in drug use, and attention should be given also to the usage techniques of the inhalation device when aiming for good asthma control.
On the other hand, the DiskusR group included no patients with PIF below the optimal range. Instead, PIF over the optimal range was observed, perhaps because of the low internal resistance of the device. However, no relationship was seen in this study between PIF over optimal range and low ACT score. From a clinical perspective, there appears to be less need to pay attention to PIF in older patients when ICS therapy is given via the DiskusR than when the Turbuhaler is used, provided that precise inhalation behavior is confirmed.
The In-Check DialR device is a simple, noninvasive device to measure PIF. Banno et al.(1) used the In-Check DialR to coach patients with PIF ≤50 L/min, finding improved FEV1 among patients who increased PIF, and FEV1 of patients in whom PIF did not increase could be significantly improved by changing treatment to corticosteroids inhaled via a pressurized metered-dose inhaler (pMDI). From that report and our own results, appropriate measures for patients in whom PIF has been judged as not optimal, would appear to include adequate education regarding inhalation and changing to a different inhalation device if insufficient improvement is obtained using the same device. These measures should be kept in mind with elderly asthma patients in particular. Moreover, appropriate selection of a corticosteroid inhalation device in the early stages of this therapy may be important with older asthma patients. Prospective and randomized controlled research to address this will be a challenge of great interest.
A recent epidemiological study in Japan found that 90% of asthma deaths involved elderly patients ≥60 years old.(16) Severity of asthma reportedly rises with increasing age at onset, as an independent factor affecting asthma severity.(17) Furthermore, elderly (>65 years old) asthmatics have been reported to show worse asthma control than younger adult asthmatics, probably because elderly patients are more likely to be less educated, more obese, and former smokers.(18) These problems in elderly asthmatics may be associated with the pathophysiology of impaired mucociliary clearance, changes to airway neutrophils, eosinophils, and mast cell numbers and function, age-related decreases in specific antibody responses resulting in increased risk of respiratory infections, and trends of cytokine profiles toward Th2 cytokine expression.(19) Considering these issues, special care in controlling asthma among elderly patients is unequivocally important for reducing deaths due to asthma.
Given the above, doctors need to pay careful attention to three points in management of asthma: (1) gaining an accurate understanding of the severity of the patient's condition, with precise selection of control medication based on this understanding; (2) requiring patients to adhere completely to asthma control; and (3) appropriate selection and training in proper use of the ICS device. The current study is significant in that we can put forward a suggestion in relation to the third of these points. Specifically, careful use should be made of indices such as ACT or PIF when considering the particular features of an inhalation device, and an action plan that will lead to effective drug use should be prepared and implemented.
Hoarseness with dry powder fluticasone has been reported to depend on the inhaled amount in patients <65 years old, but not in elderly patients, in whom no relationship has been identified between hoarseness and PIF.(20) Also in the present study, a significant relationship was not found between hoarseness and usual PIF in each device group, despite no significant relationship of hoarseness with dose of ICS. At least PIF does not seem to be a factor for onset of hoarseness irrespective of the inhalation device. However, the present study was unable to analyze the relationship between hoarseness and age, because there were few cases of hoarseness. Hoarseness should not be dismissed as a factor in reduced compliance with inhalant use, and a sufficient number of cases of hoarseness must be accumulated to allow detailed analysis of the factors underlying the onset of hoarseness.
Here we have considered the appropriate use of ICSs, limited specifically to the DiskusR and TurbuhalerR, but corticosteroids are not the only drugs delivered by inhalation devices. In particular, bronchodilators such as anticholinergics and β2-agonists delivered in dry powder form need to be considered in the same way. The same challenges will also have to be addressed in the management of inhalants for COPD.
Footnotes
Author Disclosure Statement
None of the authors have any conflicts of interest to declare regarding the present study.
Appendix
Asthma Control Test (ACT): This is the version used in the United States that can be seen in the following URL; http://www.asthmacomtrol.com/
The ACT has been translated into Japanese through “Translation Process” which is established by QualityMetric Inc. and can be seen in the following URL; http://www.qualitymetric.com/WhatWeDo/LanguageTranslations/tabid/213/Default.aspx. The Japanese version is now used all over Japan. A couple of publications in Japanese(22,23) have confirmed the validity and clinical significance of the translated ACT, although no publications in English are available.