
Abstract
Abstract
Background:
Inhaled bronchodilators are frequently used in patients with chronic obstructive pulmonary disease (COPD). However, there has been no efficient way to administer the long-acting anticholinergic tiotropium to mechanically ventilated patients. The aim of this in vitro study was to compare the fine particle dose (FPD) output of a specifically designed adapter with other accessory devices for the delivery of bronchodilators using the Respimat® (RMT) inhaler by simulating the specific inhalation flow profiles of patients with COPD.
Methods:
Using characteristic flow profiles from COPD patients being weaned off mechanical ventilation, an in vitro study was performed analyzing the FPD achieved with different accessory devices (connectors, spacers, AeroTrachPlus valved holding chamber), which can be used to deliver drugs from pressurized metered dose inhalers (pMDI) and RMT inhalers to artificial airways. Fenoterol pMDI, tiotropium RMT, and a fixed-dose combination of salbutamol and ipratropium delivered by pMDI or RMT, were used as bronchodilators. Aerosols were collected by a next-generation impactor.
Results:
The RMT inhaler, combined with a new in-line adapter, was superior to other inhaler device connector or spacer combinations in FPD delivery during simulated mechanical ventilation (p<0.01). The outcome with the RMT inhaler/RMT adapter combination during simulation of mechanical ventilation was comparable to the measurements with the RMT/AeroTrachPlus valved holding chamber during simulation of spontaneous breathing. The delivery rates of the RMT adapter were not significantly affected by the administered bronchodilators or by the type of artificial airway (endotracheal or tracheostomy tube) employed.
Conclusions:
The RMT inhaler combined with the prototype in-line adapter was better than the other accessory device combinations in fine particle deposition of inhaled bronchodilators during mechanical ventilation. Further research is required to determine the clinical relevance of these in vitro findings.
Introduction
The efficacy of inhaled drugs is related to the amount of drug, inhaled mass, deposited mass, and particle size distribution.(5) Pulmonary aerosol deposition in ventilated patients differs from that in spontaneously breathing patients and is influenced by various factors including aerosol generator type, particle size, conditions in the ventilator circuit, the artificial airway and ventilator modes.(4) With a proper technique of administration, the efficiency of aerosol delivery during mechanical ventilation has been shown to be similar to that achieved during spontaneous breathing.(6,7) It is important to note, however, that therapy with long-acting anticholinergic tiotropium is currently not available in pMDI or nebulizer forms, and there is still no efficient way of administering tiotropium to mechanically ventilated patients via tracheostomy or endotracheal tube.(8) At present, this means that preexisting maintenance treatment with once-daily tiotropium has to be discontinued in these patients. Even newer generation inhalation devices such as the Respimat® (RMT) inhaler developed for the delivery of tiotropium and fixed-dose combinations of anticholinergics and β2-agonists are not designed for use in intensive care. RMT is a multidose propellant-free active inhalation device generating a fine, slowly moving cloud with high fine particle fraction using a spring-loaded micropump with canister.(9–12) The aim of the present study was to develop a disposable, low-cost prototype in-line RMT adapter and to compare its in vitro performance with other accessory devices used in the context of bronchodilator delivery with pMDI or with RMT during mechanical ventilation and during spontaneous breathing. This report describes a proof-of-concept approach to the efficient delivery of drugs using the RMT by simulating COPD-specific respiratory mechanics during mechanical ventilation. For this purpose we used a breathing simulator to replicate representative flow profiles from ventilator-assisted COPD patients being weaned off invasive mechanical ventilation.
Materials and Methods
Study design
An in vitro analysis was performed using characteristic flow profiles based on preexisting air flow curves from 10 COPD patients (weaning category 3)(13) being weaned off mechanical ventilation in a specialized weaning unit at Kloster Grafschaft Hospital. The selected flow profiles were obtained in patients with tracheostomy tubes. They were used for all experiments to enable comparisons between the different configurations. Using these characteristic flow profiles generated by a breathing simulator, an in vitro study was performed analyzing the fine particle dose (FPD) achieved with different accessory devices (connectors, spacers, AeroTrachPlus valved holding chamber), which can be used to deliver drugs from pMDI and RMT inhalers to artificial airways. The delivery of aerosols in these settings was analyzed with a next-generation pharmaceutical impactor (NGI) (MSP Corporation, Minneapolis, MN, USA). The investigation was conducted in compliance with the Helsinki Declaration and was approved by the Westphalia-Lippe Medical Association Ethics Committee.
RMT valve-free prototype adapter
The RMT prototype adapter [patent identifier WO 2010133294 (A2)] made of medical grade polyoxymethylene copolymere provides an inlet and an outlet port and is air-tight when connected to a RMT inhaler. Figure 1 shows a cross-section of the prototype adapter that fits inside the RMT inhaler mouthpiece. The air leaving the ventilator and entering the adapter is guided toward the back of the mouthpiece. From there the air is directed through an annular opening at the circumference of the nozzle assembly. The air entrains the aerosol generated in front of the RMT nozzle and creates an air sheath that reduces premature deposition of drug on its way through the tubing. Figure 2 shows a three-dimensional diagram of the adapter including a contour plot of the air velocity representation in the symmetry plane. The RMT prototype in-line adapter has a proprietary air duct allowing for an economical two-part design of the adapter.
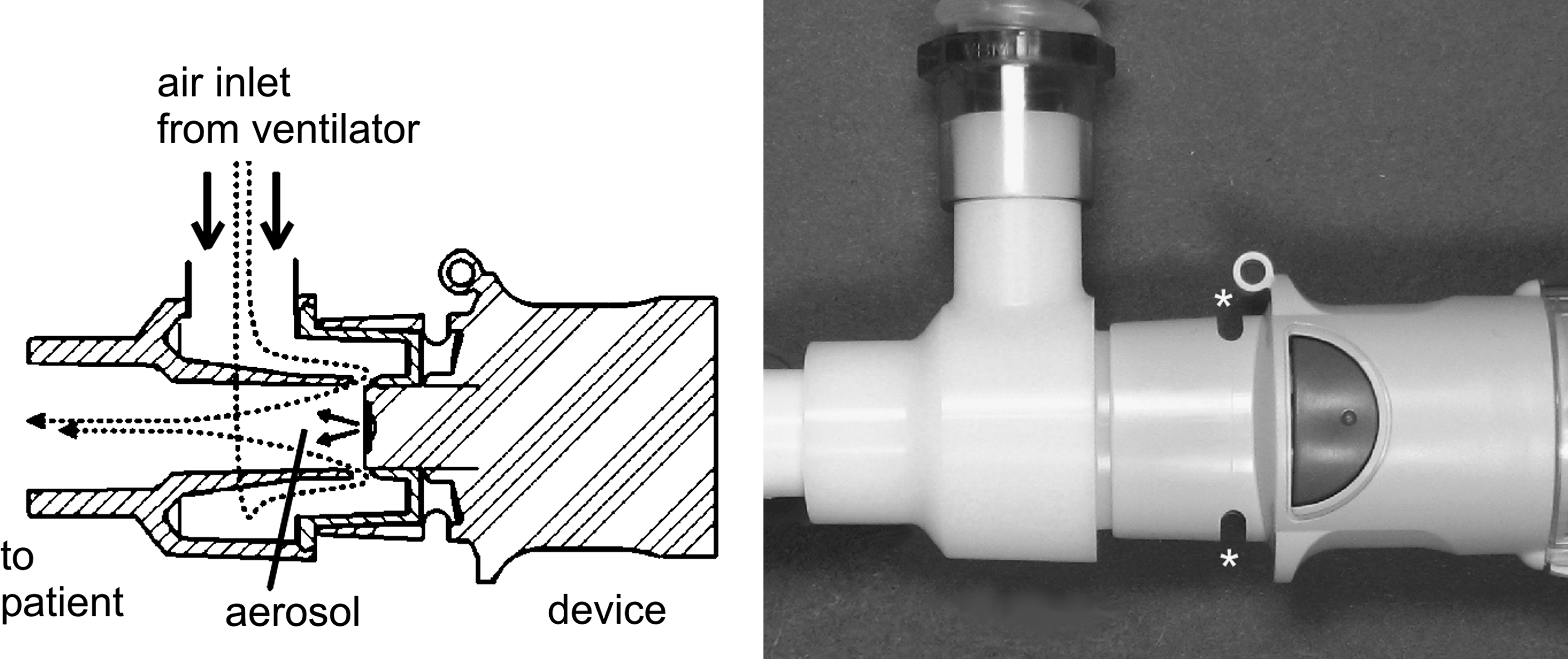
Diagram of the vertical section of the Respimat (RMT) prototype adapter illustrating both the air flow (dotted line) and the aerosol output of the RMT inhaler. The annular air supply creates a sheath of air that encloses the aerosol plume generated by the RMT inhaler and reduces wall losses. The air vents (*) located at the mouthpiece are blocked by the adapter.
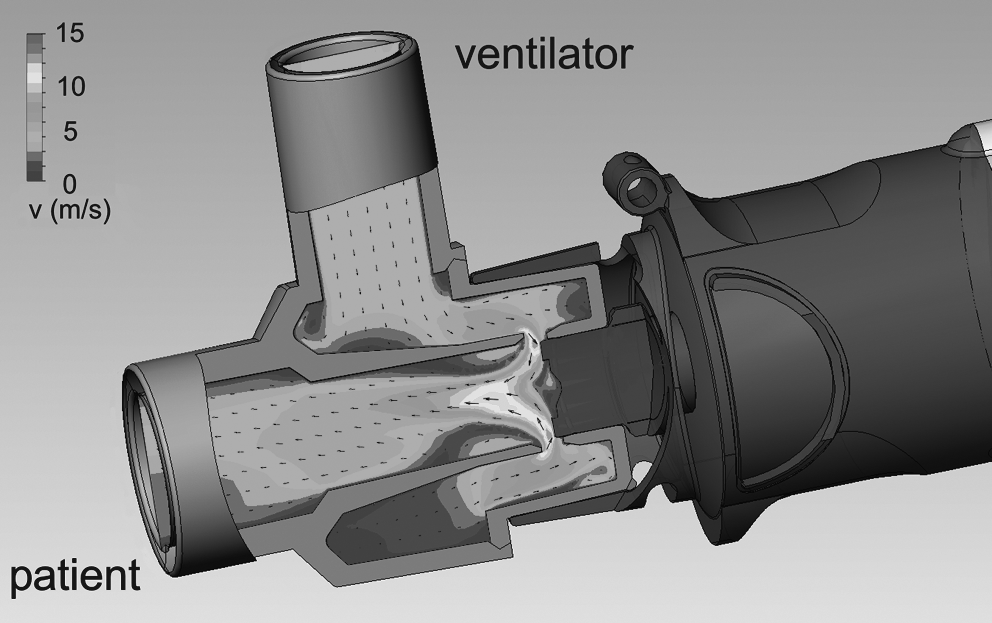
View of the prototype adapter attached to a RMT inhaler. Displayed is a contour plot with arrows indicating the air velocity on the center plane inside the adapter. The contour plot is based on a computational fluid calculation assuming air flow rate of 28.3 L/min. In the vicinity of the nozzle, the light-colored region indicates a velocity of approximately 10 m/sec and an exit velocity of the aerosol slower than 3 m/sec.
Accessory devices
Different groups of accessory devices were used (Table 1).
Illustrations of the different accessory devices used in combination with RMT or pMDI inhalers. The accessory devices were grouped into connectors/spacers (pMDI-T, RMT-Y, RMT-T/pMDI- and RMT spacers), the AeroTrachPlus valved holding chamber, and the RMT prototype adapter based on similar design and performance. The volume and size of each device and the administered inhaled bronchodilator are indicated.
API, active pharmaceutical ingredient; CFC, chlorofluorocarbon, HFA, hydrofluoroalkane; L, length; V, volume; pMDI, pressurized metered dose inhaler.
RMT valve-free prototype adapter
The RMT prototype in-line adapter described above was used in combination with tiotropium (Spiriva® Respimat®) or with a fixed combination of ipratropium and salbutamol (Combivent® Respimat®, currently approved in Mexico).
AeroTrachPlus valved holding chamber
The AeroTrachPlus valved holding chamber (Trudell International, Nottingham, UK) was used for simulation of spontaneous breathing. It was used with a fixed dose combination of ipratropium and salbutamol (Combivent® pMDI; Combivent® Respimat®), and with tiotropium (Spiriva® Respimat®).
Valve-free connectors
These connectors comprised a conventional T-piece pMDI adapter (VBM Medizintechnik, Sulz, Germany) for use with fenoterol (Berotec®), plastic T-piece and Y-piece RMT adapters (Boehringer Ingelheim) for use with tiotropium (Spiriva® Respimat®), and spacers (pMDI spacer; Trudell International, Nottingham, UK) for use with fenoterol (Berotec®) and a modified RMT spacer (Boehringer Ingelheim) equipped with an airtight connector for the RMT mouthpiece for use with tiotropium (Spiriva® Respimat®).
Inhalers
Two different inhaler devices, pressurized metered dose inhalers (pMDIs) and the RMT soft mist inhaler were tested in conjunction with their appropriate accessory devices. pMDIs with two different propellants were applied. Berotec pMDI contains fenoterol hydrobromide and is at present formulated with hydrofluoroalkane (HFA). Combivent® pMDI contains a fixed-dose combination of ipratropium bromide monohydrate and salbutamol sulphate with chlorofluorocarbon (CFC) as a propellant. Combivent®-CFC-pMDI, which is still in use in the United States, was selected as a reference comparator to the Combivent® Respimat® inhaler, because some of the accessory devices (e.g., T-piece pMDI-adapter, AeroTrachPlus valved holding chamber) used in the study had originally been designed on the basis of CFC aerosol properties, and, because the RMT inhaler has been replacing the CFC pMDI.
The RMT inhaler is a hand-held, pocket-size inhalation device that uses mechanical energy to generate a slowly moving, long-lasting aerosol cloud from a metered volume of solution.(14) RMT was filled with an aqueous solution of either tiotropium (Spiriva®) or of a fixed-dose combination of ipratropium and salbutamol (Combivent® RMT®). The design of the RMT inhaler device excludes backflow into the nozzle and has been shown to enable application under conditions of high relative humidity.(11)
Breathing simulator
The ASL 5000 (Ingmar Medical, Pittsburgh, PA, USA) is a fully computerized servo lung that permits reproduction of flow profiles by importing the numerical data into the control program. The correct reproduction of the flow profiles was analyzed using a pneumotachograph (Masterscope, Viasys Healthcare, Hoechberg, Germany).
Mixing inlet
The cascade impactor requires a constant flow of air through its nozzle system to ensure the correct classification of aerosol particle size. In the setup shown in Figure 3, the constant air flow through the impactor was controlled by a separate pump (not shown) sucking air at a given constant flow rate (60 L/min). In the mixing inlet, an air flow balance was maintained at the entry of the impactor.(15)
Experimental setup (
Artificial airway
For the comparisons, all connectors and inhalers were tested with tracheostomy tubes, type ULTRA Tracheoflex® HC PVC (Rüsch Care, Kernen, Germany) with an internal diameter (i.d.) of 8.0 mm and a cuff diameter of 19 mm. The tubes were bent 90° to simulate their use in a patient. In addition, the RMT prototype adapter was attached to an endotracheal tube (Rüsch Care) size 8.0. The tube (bend radius r=50 mm) was held in a stand that ensured a 90° bend to simulate the anatomical situation in humans.
Analytics
The in vitro experiments were carried out in a controlled atmosphere at 23±3°C and 50±5% relative humidity (RH). The equipment was placed in a climatic chamber (KBF 240, Binder, Tuttlingen, Germany). Figure 3 shows the setup, which consisted of a NGI cascade impactor that was flushed with a constant flow of humidified air (flow rate 60 L/min, relative humidity >95%); a mixing inlet; and the breathing simulator ASL 5000. The mixing inlet (MI) was connected to an entry tube in which the tracheostomy tubes or laryngeal tubes were fixed. The flow profiles were programmed into the ASL 5000 breathing simulator and five breathing cycles were performed. After two or three cycles, the RMT inhaler or the pMDI were released manually in synchrony with the inspiratory airflow. This procedure was repeated 10 times in immediate succession. The resulting amount of drug deposited in the adapter, tubes, and cups of the cascade impactor was analyzed. Aliquots of the corresponding solutions were analyzed by validated high-performance liquid chromatography (HPLC, modular system with Agilent components, Agilent, Boeblingen, Germany). For the simulation of a ventilator setting, the programmed amount of humidified air was drawn through the adaptor into the mixing inlet (Fig. 3a) and the surplus was guided into the surrounding air. On simulation of spontaneous breathing (Fig. 3b), air sucked into the servo pump was replaced by air drawn through the inhaler and the AeroTrachPlus valved holding chamber (RH=50±5%). The aerosol was passed through the mixing inlet into the NGI and was classified according to the recommendations of the United States Pharmacopeial Convention.(16) The impactor set up corresponded to Apparatus 6 described in the USP 33, except for the flow rate which was set to 60 L/min, resulting in cutoff aerodynamic diameters of 8.06, 4.46, 2.82, 1.66, 0.94, 0.55, 0.34 micrometer for the stages 1 to 7, respectively.The mass of the individual stages was assessed by HPLC. The FPD was determined by log-linear interpolation, summing up all the mass below 5 μm in aerodynamic diameter. The mass median aerodynamic diameters (MMAD) were determined from the cumulative size distributions.
Assay and quantitation
The drugs used in this investigation were formulated at different concentrations: Spiriva® Respimat®: tiotropium: 2.5 μg per actuation (two actuations=one therapeutic dose). Combivent® Respimat®: 20 μg of ipratropium bromide and 100 μg of albuterol sulfate per actuation. Berotec® pMDI: 100 μg of fenoterol per actuation. Combivent® pMDI: 18 μg of ipratropium bromide and 103 μg of albuterol sulfate per actuation (two actuations=one therapeutic dose). Accordingly, all results were presented relative to the delivered mass exmouthpiece as the percentage of the FPD delivered to the lung. RMT and pMDI devices were applied as recommended in the handling instructions.
Data analysis and statistics
The flow profiles were analyzed using MathCad 11.0 (Mathsoft, PTC, Needham, MA, USA) independently of the settings of the ventilator. Five sequential periods of the volume recordings were analyzed by fitting the time dependence with a simple quadratic model term. Using the method of least squares, the fit provided averaged estimates for times of inspiration and expiration as well as of tidal volumes. According to these values, typical flow profiles were selected. Descriptive statistics were applied. Group-wise comparison of the means was performed using the t-test. Significance was assessed using Fisher's least significant difference (LSD) procedure at a 95% significance level.
Results
Characteristic flow profiles for in vitro simulation
Figure 4 shows three representative flow profiles that were used for the analyses of the various accessory devices with the breathing simulator to ensure equal test conditions. These profiles reflect characteristic volumes and inspiration times to peak volumes [ranging from 1.18 sec (flow profile C), 1.3 sec (flow profile A), and 1.55 sec (flow profile B)] taken from 10 mechanically ventilated COPD patients with a tracheostomy tube.

Characteristic volume representations of flow profiles used for in vitro simulation of COPD-specific respiratory mechanics during mechanical ventilation. The three profiles A, B, and C reflect characteristic volumes and inspiration time to peak volumes chosen from patients [n=10, seven male, mean age: 74 (8) years, tracheal tube size (French scale): 8.3 (0.5)] being weaned off mechanical ventilation (ventilation settings: assisted pressure controlled ventilation (aPCV) mode, fraction of inhaled oxygen (FiO2 %): 35(3), inspiratory pressure (IPAP): 24 (5) cm H2O, exspiratory pressure (EPAP): 7(1) cm H2O, inspiratory time ranging from 1.0 to 1.5 seconds, tidal volume ranging from 0.45 to 0.7 liters. The numbers in parentheses are standard deviations.
Aerosol delivery using different accessory device configurations with RMT inhaler or with pMDI
The FPD, percentage of delivered mass (DM) exmouthpiece delivered into the impactor with the RMT or with pMDI attached to various accessory devices is shown in Figure 5. All the devices were compared in the same three conditions of flow profiles (A–C): for the purpose of the study, FPD data was pooled for the three categories of accessory devices: (a) RMT adapter, (b) AeroTrachPlus holding chamber, (c) connectors/spacers as their performance was largely independent of the applied inhaled drugs and the type of accessory device. Using the AeroTrachPlus valved holding chamber, spontaneous breathing was simulated based on flow profiles A–C, whereas the RMT prototype adapter and the other connectors were used on simulation of mechanical ventilation based on flow profiles A–C. For all flow profiles studied (A, B, and C), the FPD (% DM) achieved with the RMT prototype adapter and the AeroTrach Plus valved holding chamber was significantly higher than with the other connectors/spacers [pMDI-T, RMT-T, RMT-Y, spacers (pMDI and RMT)], p<0.01. The FPD (% DM) achieved with the RMT prototype adapter was similar in magnitude to that of the AeroTrach Plus holding chamber. The FPD was influenced by the chosen flow profile. The longer duration of flow profile B significantly enhanced FPD by ∼10 % for the RMT prototype adapter compared with flow profiles A (p<0.03) and C (p<0.01). When flow profiles A and C were applied, the average FPD (% DM) was moderately but significantly higher with the AeroTrach Plus holding chamber than with the RMT prototype adapter (p<0.03).

Average fine particle dose [FPD, mass median aerodynamic diameter (MMAD) <5 μm] expressed as a percentage of the delivered exmouthpiece mass of drug from RMT inhaler or pMDI in combination with various accessory devices connected to a tracheostomy tube. The accessory devices were grouped into connectors/spacers (pMDI-T, RMT-Y, RMT-T, and spacers for pMDI and RMT; n=5), the AeroTrachPlus valved holding chamber (n=3), and the RMT prototype adapter (n=3). The AeroTrachPlus holding chamber delivered a greater FPD than the RMT prototype adapter with flow profiles A and C, whereas the longer duration of flow profile B was associated with a larger FPD provided by the RMT prototype adapter. The FPD delivered by the connectors/spacers was comparable within this group and significantly lower than that delivered by the AeroTrachPlus holding chamber and the RMT prototype adapter groups (p<0.01). The second quartile (25 to 50%) is grayed, the third quartile (50 to 75%) is hatched, the horizontal line between the quartiles indicates the median, the closed squares indicates the mean, and the error bars indicate 1 standard deviation. The arrows delimit the 95% LSD intervals determined with Fisher's least significant difference procedure. RMT, Respimat; pMDI, pressurized metered dose inhaler; FPD, fine particle dose; DM, delivered mass.
In comparison to the results achieved with the RMT prototype adapter and the AerotrachPlus holding chamber, all connectors/spacers were asscociated with a significantly lower mean FPD over flow profiles A, B, C (p<0.01). Figure 6 shows the average deposition [FPD (% DM)] for each device in relation to the mean of all three flow profiles. Both the AeroTrachPlus holding chamber and the RMT adapter prototype achieved a fairly constant FPD ranging from 23 to 45% regardless of the drugs administered (tiotropium, salbutamol+ipratropium) and of the type of artificial airway (endotracheal or tracheostomy tube). In contrast, the other connectors/spacers provided significantly less aerosol delivery [3% to 18% (FPD; % DM)], p<0.01 for all connectors/spacers in all flow profiles versus RMT prototype, and p<0.01 versus AeroTrachPlus holding chamber) (Fig. 6).
Average FPD (MMAD <5 μm) expressed as a percentage of delivered mass, delivered by various accessory device configurations as related to the mean of the applied flow profiles A, B, and C. The FPD delivered by the AeroTrachPlus valved holding chamber and the RMT adapter prototype was comparable regardless of the drugs administered (tiotropium, salbutamol+ipratropium) and the type of artificial airway [endotracheal tube (ETT) or tracheostomy tube (TT)]. In contrast, the other tested connectors/spacers achieved a significantly lower FPD (% DM) (p-value for all others vs. the group of connectors/spacers p<0.01). The second quartile (25 to 50%) is grayed, the third quartile (50 to 75%) is hatched, the horizontal line between the quartiles indicates the median, the closed squares indicate the mean, and the error bars indicate 1 standard deviation. The arrows delimit the 95% LSD intervals determined with Fisher's least significant difference procedure. Abbreviations: Atr, AeroTrachPlus; CV, combivent; Tio, tiotropium; RMT, Respimat; pMDI, pressurized metered dose inhaler; FPD, fine particle dose; DM, delivered mass.
Discussion
The aim of the present study was to compare the fine particle dose delivery of a prototype valve-free in-line adapter for RMT with other connectors and spacer combinations being used with pMDI or RMT inhalers.
The RMT device in combination with the newly developed in-line adapter outperformed the tested valve-free connectors and spacers combined with RMT or with pMDI in terms of fine particle deposition during mechanical ventilation by more than factor of three. Moreover, FPD was similar to that seen with the AeroTrachPlus valved holding chamber.
When aerosols from a pMDI are delivered into the ventilator circuit via an actuator, the canister has to be separated from its original nozzle and coupled to the actuator. It should be noted that the stem size of pMDIs and the slot dimensions of different actuators are not standardized, nor do the actuator nozzles have the same physical properties.(4) In addition, HFA- and CFC-driven canisters are characterized by different vapor pressure properties. In this context, it is important to note that the use of inappropriate canister/actuator combinations might in fact compromise drug delivery(17) and the corresponding effects of treatment.(18)
By contrast, the combination of RMT inhaler and prototype adapter has been specifically designed to fit RMT inhalers thereby minimizing the likelihood of using an inappropriate combination of inhaler and accessory device. At present, however, only a limited number of bronchodilators are available for use with the RMT inhaler (tiotropium; ipratropium in fixed-dose combination with fenoterol or with salbutamol). The majority of patients being weaned off mechanical ventilation are able to breathe without ventilator assistance for sufficiently long periods to enable administration of inhalation therapy via an artificial airway during spontaneous breathing trials.(8,19–21) An analysis of deposition in this context has so far yet to be performed, however. Previous studies have also highlighted the importance of mimicking in vivo flow profiles during in vitro deposition measurements.(22) To address this issue, we analyzed the flow profiles of mechanically ventilated patients with COPD and established three representative flow profiles in preliminary experiments. Our approach differs from previous investigations in that fine particle output of various inhaled bronchodilators was measured in vitro during simulation of both spontaneous breathing and mechanical ventilation. All experiments relied on identical flow profiles to facilitate comparisons.
Multiple factors, such as the artificial airway itself, the ventilator mode, the circuit, and the relative humidity within the circuit, can impact aerosol deposition into the lung. It is important to emphasize that FPD fractions achieved with the combination of the RMT inhaler plus the RMT adapter during mechanical ventilation did not significantly differ from those achieved with the combination of the RMT inhaler and AeroTrachPlus holding chamber during simulation of spontaneous breathing (Fig. 6).
Whereas the latter combination suggests consistent deposition rates over all three applied flow profiles, the RMT/adapter prototype combination showed higher delivery for the flow profile with longer inspiratory time. It should be noted that the generation of a fine, slow-moving cloud over 1.5 sec by the RMT inhaler might interfere with the application of higher frequency ventilator settings in COPD patients, thereby potentially resulting in shorter inspiration times. Hence, actuation of the RMT during deep inspiration is recommended to minimize dose variability. All other analyzed valve-free connector and spacer combinations with RMT and pMDI inhalers resulted in significantly lower deposition rates in all flow profiles irrespective of the drugs administered.
Consistent with our results, Fuller et al. reported in vivo deposition rates for radioactive-labeled drugs administered via a pMDI plus spacer of 5.65 and 6.33%, respectively.(23,24) By contrast, Rau et al.(25) and Lin et al.(26) reported aerosol deposition rates of 32.1 and 23%, respectively, from a pMDI with spacer. The discrepancy can be explained by methodological differences between in vivo and in vitro measurements. Moreover, correction for tissue adsorption almost doubles the drug delivery reported by Fuller et al.(23,24)
Strengths of the disposable, low-cost valve-free RMT prototype adapter include a more efficient delivery compared with all other tested valve-free connectors/spacers for pMDI or RMT inhalers. The deposition rates achieved with the RMT prototype adapter were of the same order as those achieved with RMT combined with the AeroTrachPlus valved holding chamber and were similar to those observed with the RMT inhaler in ambulatory patients.(27) These findings indicate that the RMT prototype adapter is likely to deliver an effective bronchodilator dose to the lungs, is easy to use, and requires less time and technical equipment compared with nebulizers.
The superiority of the RMT prototype adapter over other valve-free connectors and spacers can be explained by the design of the prototype adapter. The gas-flow geometry within the adapter was designed to allow the air stream to build up a sheath of air that decreases drug deposition within the artificial airway (Fig. 2). The deposition rates yielded with the RMT prototype adapter were also irrespective of the type of artificial airway used (endotracheal or tracheostomy tube) (Fig. 6).
Conclusions
In the present study we have described the in vitro validation of a valve-free in-line prototype adapter for use with the RMT inhaler in mechanically ventilated patients. The results of this proof-of-concept study demonstrate a better fine particle delivery of the RMT prototype adapter compared to various other valve-free connector/spacer devices in use with pMDIs or RMT. Further in vivo studies are needed to evaluate the clinical relevance of our findings.
Footnotes
Acknowledgments
Publication fees were funded by Boehringer Ingelheim, Germany.
Author Disclosure Statement
D.D. has received consulting fees from Boehringer-Ingelheim, Lilly, and Weinmann. T.G., H.W., and M.P. were employees of Boehringer Ingelheim at the time of manuscript submission. D.K. has given presentations at industry symposia sponsored by Astra-Zeneca, Boehringer Ingelheim, Pfizer, GlaxoSmithKline, Weinmann. E.H. and T.B. declare that no conflicts of interest exist.