
Abstract
Abstract
Background:
Macrolide antimicrobial agents are generally given by the oral route for the treatment of respiratory infections caused by pathogenic microorganisms infected in lung epithelial lining fluid (ELF) and alveolar macrophages (AMs). However, because macrolides distribute to many different tissues via the blood after oral administration, systemic side effects are frequently induced. In contrast with oral administration, aerosolization may be an efficient method for delivering macrolides directly to ELF and AMs. In this study, the efficacy of aerosol-based delivery of clarithromycin (CAM), as a model macrolide, for the treatment of respiratory infections was evaluated by comparison with oral administration.
Method:
The aerosol formulation of CAM (0.2 mg/kg) was administered to rat lungs using a Liquid MicroSprayer®. The oral formulation of CAM (50 mg/kg) was used for comparison. Time courses of concentrations of CAM in ELF and AMs following administration were obtained, and then the bioavailability (BA) was calculated. In addition, the area under the concentrations of CAM in ELF and AMs—time curve/minimum inhibitory concentration at which 90% of isolates ratio [area under the curve (AUC/MIC90)] were calculated to estimate the antibacterial effects in ELF and AMs.
Results:
The BA of CAM in ELF and AMs following administration of aerosol formulation were markedly greater than that following administration of oral formulation. This indicates that the aerosol formulation is more effective in delivering CAM to ELF and AMs, compared with the oral formulation, despite a low dose. The AUC/MIC90 of CAM in ELF and AMs were markedly higher than the effective values. This indicates that the aerosol formulation could be useful for the treatment of respiratory infections caused by pathogenic microorganisms infected in ELF and AMs.
Conclusions:
This study suggests that aerosol formulation of macrolides is an effective pulmonary drug delivery system for the treatment of respiratory infections.
Introduction
Macrolide antimicrobial agents are generally given by the oral route for the treatment of respiratory infections caused by pathogenic microorganisms infected in ELF and AMs.(24) Because macrolides distribute to many different tissues via the blood after oral administration,(25) systemic side effects are frequently induced.(26–28) In contrast with oral administration, aerosolization may be an efficient method for delivering macrolides directly to ELF and AMs. Therefore, an enhancement of the antimicrobial effect, a reduction in the dose and avoidance of systemic side effects could be achieved by the aerosolization of macrolides.
In this study, the efficacy of aerosol-based delivery of clarithromycin (CAM), as a model macrolide, for the treatment of various respiratory infections caused by pathogenic microorganisms infected in ELF and AMs was evaluated by comparison with oral administration.
Materials and Methods
Materials and animals
CAM was purchased from Wako Pure Chemicals CO., Ltd. (Osaka, Japan). All other regents were commercially available and of analytical grade. Male SD rats (200–230 g) were purchased from Japan SLC (Shizuoka, Japan). The animal experimental plan used was been approved by the Committee of Laboratory Animal Center (No. 09-009), and conforms to the Guiding Principles for the Care and Use of Experimental Animals in Hokkaido Pharmaceutical University.
Animal experiments and pharmacokinetic analysis
CAM dissolved in phosphate-buffered saline solution (pH 7.4) was aerosolized into rat lungs at a dose of 0.2 mg/0.25 mL/kg using a Liquid MicroSprayer
In order to calculate the concentrations of CAM in ELF, the apparent volume of ELF was estimated using urea as an endogenous marker of ELF dilution.(30) The mean ELF value estimated in the present study was 393 μL/215 g rat. In order to calculate the concentrations of CAM in AMs, the intracellular volume in AMs was determined by a velocity-gradient centrifugation technique using 3H-water,(31) and this was estimated to have a mean value of 4.2 μL/mg cell protein. The concentration of CAM in each sample was measured by high-performance liquid chromatography (HPLC) as described below. The protein concentration in the AMs extracts was determined using Coomassie protein Assay reagent (Pierce Chemical Company, Rockford, IL, USA) with bovine serum albumin as a standard.(32)
For the pharmacokinetic analysis, the area under the curve—time curve from time 0 to time 24 h (AUC) was calculated by the trapezoidal rule. Also, bioavailability (BA) in ELF and AMs was calculated from Equation (1)(33) using the data following the intravenous injection a dose of 50 mg/mL/kg in this study.
where Dformulation is the dose of formulation, Div injection is the dose of intravenous injection, AUCformulation is the AUC following administration of formulation, and AUCiv injection is the AUC following intravenous injection. Div injection was 50 mg/kg wt, AUCiv injection in ELF and AMs were 350 μg*h/mL and 15,441 μg*h/mL, respectively.
Pharmacokinetics/pharmacodynamics (PK/PD) analysis
The antibacterial effects of CAM in ELF and AMs following administration of the formulation were estimated by PK/PD analysis. The ratio of AUC/minimum inhibitory concentration at which 90% of isolates (MIC90) (AUC/MIC90) was calculated as the PK/PD parameters of an antibacterial effect. The MIC90 values against microorganisms infected in ELF and AMs were taken from the literature.(34–38) The estimated effective values of AUC/MIC90 are larger than 100 h.(39) Also, the required dose for effective therapy (RD, a dose required for winning 100 h that is effective AUC/MIC90 value) was calculated from Equation (2).
Determination of CAM by HPLC
The concentrations of CAM in samples were measured by HPLC with electrochemical detection. The samples (50 μL) and added roxithromycin solution (as an internal standard dissolved in acetonitrile, 50 μL) were mixed, and 50 μL aliquots were subjected to HPLC using a system involving a Mightysil RP-18GP column (4.6×150 mm, 5-μm pore size; Kanto Chemical Co., Tokyo, Japan). The mobile phase was 50 mM phosphate buffer (pH 6.8)/acetonitrile/methanol (5:4:1). The separation was performed at a flow rate of 1.0 mL/min at 40°C and the eluate from the column was monitored using an electrochemical detector (Coulochem II, ESA, Bedford, MA, USA). A dual analytical cell was used with the upstream potential set at + 650 mV and the downstream potential at + 800 mV.
Results and Discussion
Pharmacokinetics of CAM
The time-courses of the concentrations of CAM in ELF, AMs, and plasma after administration of the aerosol and oral formulations to rats are shown in Figure 1. The pharmacokinetic parameters are summarized in Table 1. The concentrations of CAM in ELF and AMs following administration of the aerosol formulation were lower than those of the oral formulation. However, the BA of the aerosol formulation in ELF and AMs were 42 and 28, respectively. These values were greater than those of the oral formulation. These findings suggest that the aerosol formulation would have pharmacokinetic efficacy of 42- and 28-fold that of the intravenous injection. Also, the concentrations of CAM in plasma following administration of the aerosol formulation were remarkably lower than those following administration of the oral formulation. This indicates that, in comparison with oral formulation, the aerosol formulation can avoid distribution of macrolides to blood.
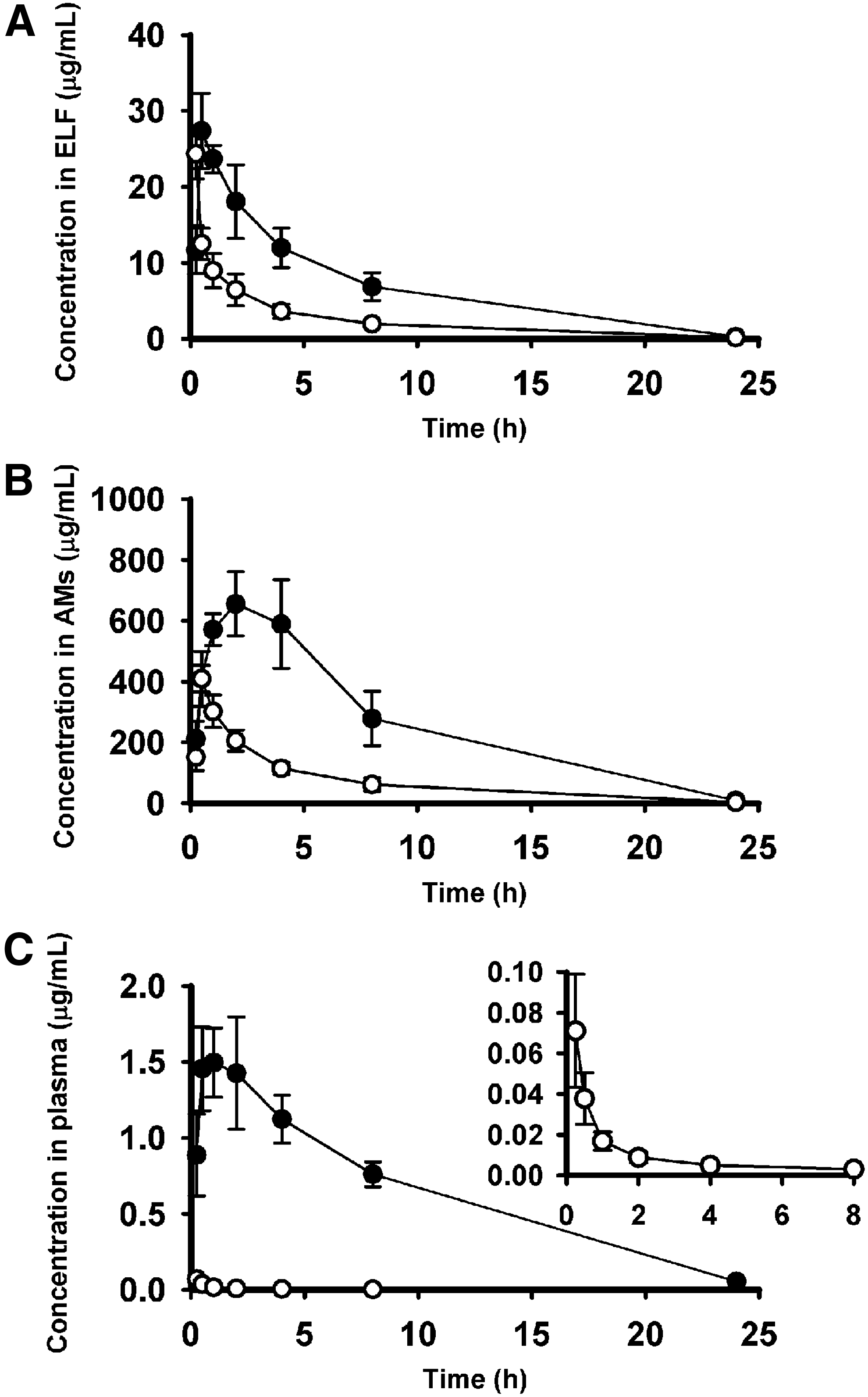
Time courses of concentrations of CAM in ELF (
Each pharmacokinetic parameter was calculated from data shown in Figure 1.
AUC are represented as mean values (n=4).
Macrolides given by the oral route distributes in the alveolus through vascular endothelial cells and alveolar epithelial cells from the blood side. The alveolar barrier consists of three layers, the capillary lumen, connected tissue, and alveolar epithelial cells.(40) The alveolar epithelial cells that are tightly connected by numerous zonulae occludins is considered to provide a significant barrier between the plasma and ELF.(41) There are several efflux transporters expressed in alveolar epithelial type I cells in the human and rat lung, including P-glycoprotein and breast cancer-resistant protein.(42–44) CAM is an MDR1/P-glycoprotein substrate and, thus, CAM can cross from the alveolar epithelium to ELF via an MDR1 transporter.(45) However, transport of CAM to ELF across the alveolar barrier after oral administration may not be as efficient. In contrast, aerosolized CAM was efficiently delivered to ELF and AMs because it was sprayed into the alveolus directly (Fig. 1 and Table 1). Thus, a reduction in the dose and avoidance of distribution to the blood is possible. The AUC ratios of plasma/ELF of CAM following administration of the aerosol formulation were 0.0014 (Table 1). According to our recent report, this significant asymmetry is based on the fact that transport of CAM from ELF to blood is inhibited by the MDR1 transporter on the alveolar epithelial type I cells.(45) These findings suggest that aerosolization can avoid systemic side effects as well as provide efficient delivery of macrolides to AMs and ELF.
The AUC of CAM in AMs following administration of the aerosol formulation is 29-fold greater than that in ELF (Table 1). This indicates that CAM is able to concentrate intracellularly in AMs. Recently, we have reported that uptake of CAM by AMs is mediated by active transport systems.(45) According to previous reports,(46) CAM may be transported to the intracellular region of AMs via active transport systems which require Ca2+ and protein kinase A-dependent phosphorylation, the same as other phagocytes such as human polymorphonuclear neutrophils and J774 murine macrophages, in addition to passive diffusion. In another study, we have also confirmed that CAM distributes to the entire intracellular area of AMs and not the local area (data not shown).
Estimated antibacterial effects of CAM
The estimated antibacterial effects of CAM in ELF and AMs following administration of the aerosol and oral formulation to rats are summarized in Tables 2 and 3. Recently, there has been increasing interest in the relationship between the PK and PD of antimicrobial agents and, therefore, the use of PK/PD parameters is now widespread.(47,48) It is proposed that the PK/PD analysis of an antibiotic treatment is important for selecting a dose and optimizing the treatment of individual patients. The effects of antimicrobial agents are concentration- and/or time-dependent and the PK/PD parameters used generally are the maximum plasma concentration/MIC90 (Cmax/MIC90), AUC/MIC90 and the time above the MIC90. Because the antibacterial effects of CAM depend on the AUC/MIC90,(39) the AUC/MIC90 values in ELF and AMs were calculated in the present study. Also, the RD was calculated to obtain information regarding an effective dose. In the case of the aerosol formulation, despite a low dose, the AUC/MIC90 ratios of CAM against most pathogenic microorganisms infected in ELF and AMs were larger than 100 h that is the effective value. Only the AUC/MIC90 against H. influenzae (3.7 h) was lower than the therapeutic value. However, the RD of the aerosol formulation was slightly 5.4 mg/kg (1/93th of the RD of oral formulation). The oral formulation also had an effective AUC/MIC90 value against most pathogens except H. influenzae. Interestingly, the RD of the aerosol formulation against each pathogenic microorganism for effective therapy was markedly lower than those of the oral formulation. The AUC/MIC90 and RD values showed that efficient antibacterial effects of CAM in ELF and AMs are obtained by aerosolization of a dose lower than that used orally. The antibacterial effect of CAM following aerosol formulation to animals used as models of respiratory infection should be investigated in the future because it was not examined in this study.
AUC in ELF as described Table 1 were used for calculation of PK/PD parameter.
The MIC90 values were taken from the literature.
Okamoto, 2000.(34)
Bozdogan, 2003.(35)
Zhanel, 2003.(36)
AUC in AMs as described Table 1 were used for calculation of PK/PD parameter.
The MIC90 values were taken from the literature.
Miyashita, 2003.(37)
Krishnan, 2009.(38)
For sterilization of pathogenic microorganisms infected in ELF and AMs, it is required that CAM is stable in ELF and AMs following administration of aerosol formulation. We have shown that CAM was stable in ELF and AMs for 48 h at 37 oC in vitro (data not shown). Although AMs produce and secrete various bioactive substances, such as enzymes, cytokines, complements, proteins, lipids, and reactive oxygen species,(49–54) these bioactive substances may not affect the stability of CAM. In addition, it is important that the aerosolized CAM do not injure lung tissues. The aerosol formulation of CAM was found to be nontoxic following administration because no release of lactate dehydrogenase from lung tissue was observed (data not shown). This indicates that the aerosolized CAM does not injure lung tissues, at least at the dose used in this study.
Conclusion
This study evaluated the efficacy of aerosol-based delivery of CAM for the treatment of respiratory infections. We have shown that delivery of CAM to ELF and AMs is possible by administration of an aerosol formulation. Furthermore, it was shown that the efficient antibacterial effect of CAM against various pathogenic microorganisms following administration of aerosol formulation was obtained at a dose lower than that used orally. These findings suggest that aerosolization of macrolides is an efficient method for the treatment of a variety of respiratory infections.
Footnotes
Acknowledgments
This work was supported in part by a Grant-in Aid (No. 20590039) for Scientific Research provided by Japan Society for the Promotion of Science.
Author Disclosure Statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article.