
Abstract
Abstract
This article provides a concise review of the use of magnetic resonance imaging (MRI) for measurement of regional aerosol deposition in the lungs. Basic aspects of MRI and its use in lung imaging and measurement of regional ventilation are introduced. Imaging of hydrogen protons (water) and inhaled hyperpolarized gases as the MRI source signals are discussed. The addition of contrast agents to aerosol particles in order to allow measurement of regional aerosol deposition is considered. Existing in vitro human and in vivo animal model measurements of regional aerosol deposition in the respiratory tract demonstrate the capability of MRI in this regard. However, as a tool for human deposition studies, current approaches require contrast agent doses that are too high to be considered competitive with traditional radionuclide aerosol deposition measurement methods. Thus, future use of MRI in human studies of regional aerosol deposition is predicated on improvement over present approaches.
Introduction
Introduction to MRI
Magnetic resonance imaging is an application of the nuclear magnetic resonance (NMR) phenomenon. The strengths of MRI include the use of nonionizing radiation, several diverse intrinsic soft tissue contrast mechanisms, and arbitrary orientations for two-dimensional imaging planes or three-dimensional imaging. The signals used to generate images (or NMR spectra) are acquired from nuclei with integer or half integer values of spin proportional to the nuclei's angular momentum. This nonzero angular momentum is a consequence of an odd number of protons and/or neutrons, as is found in 1H, 3He, or 15Na, for example. The vast majority of clinical MRI is based on imaging of the hydrogen atoms found in water, which is the most abundant substance in living tissues, although imaging of inhaled helium in studies of lung function is now a well established research application of MRI. MRI (and NMR) experiments, regardless of the nuclei of interest, are based on the interaction of nuclear magnetic moments, intrinsic to the sample or tissue of interest, with external magnetic and electromagnetic fields. Although a complete description of the NMR phenomenon requires a quantum mechanics formalism, the vector depiction that follows is an accurate and illustrative description of the basic NMR imaging experiment.
First, a static external magnetic field (B0) is used to magnetize or align the magnetic moments in the sample or tissue of interest (Fig. 1A). The vast majority of MRI scanners use superconducting magnets to generate the required powerful, homogeneous, and stable B0 fields that can range in strength from 0.2 T to 11 T (most commonly 1.5–3.0 T in whole-body human MRI scanners). The net magnetization (magnetic moment per unit volume) can be represented as a vector,

(

Cutaway view of a whole body MRI scanner, showing the orientation of the main magnetic field coils (B0), the radiofrequency (RF) coil (B1) and the magnetic field gradient coils (graphic courtesy of National High Magnetic Field Laboratory, University of Florida).
Contrast mechanisms in MRI
MRI provides unparalleled image contrast based on sensitivity to spin density (number of nuclei per unit volume), T1 and T2 relaxation times, motion (ranging from diffusion to rapid pulsatile blood flow in major arteries), among several other mechanisms, with T1 and T2 as the most widely exploited. Here, T2 is the spin–spin or transverse relaxation constant, which characterizes the exponential decay of the precessing magnetization vector following excitation, while T1 is the spin–lattice or longitudinal relaxation time constant, which characterizes the exponential recovery of magnetization back to thermal equilibrium (repolarization) following excitation. Both T1 and T2 values are strongly dependent on the local environment of the nuclei, where different healthy tissues and pathologies have characteristic values. Typical values for 1H water nuclei are tens of milliseconds for T2 and ∼1 sec for T1, although these values vary significantly with tissue type, B0 strength and with nuclear species. MRI experiments can be designed to produce a desired image contrast, or differences in signal intensities, based on the T1 and T2 values, to differentiate tissue types or pathology. Furthermore, contrast agents can be used to significantly reduce T1 and T2 values, and thus the delivery of agents can be quantified based the changes in T1 or T2 values, or most commonly via the resulting changes in MRI signal intensities using T1 or T2-weighted imaging.
Low sensitivity of MRI
Unfortunately, the polarization of the nuclear spins by the B0 field, shown in the cartoon in Figure 1A, effectively aligns only ∼10 in 106 spins, which is referred to as the Boltzmann equilibrium level. The degree of polarization is directly related to the temperature, the gyromagnetic ratio, and the B0 field strength, ∼γhB0/kT, where h is the Planks constant, k is the Boltzmann constant, and T is the absolute temperature, which is one motivating factor for higher field strength scanners. This low polarization efficiency, combined with the minute spin angular momentum of each spin means that ∼1020 water molecules are necessary to generate an observable signal, in human studies, that exceeds the unavoidable background thermal noise signals (generated by the tissue and electronics used to detect and amplify the induced currents). For water, which is typically 30–40 M concentration in blood and tissue, typical volumes that can be spatially resolved in humans are on the order of 1–3 mm in each dimension (0.001–0.03 mL).
Hyperpolarized gas MRI: Imaging ventilation and aerosol delivery
Compared to water proton imaging, all other NMR-visible nuclei suffer from lower sensitivities as a result of smaller γ and lower concentrations, which is particularly true for the NMR-visible gases 3He and 129Xe due to the lower density of the gas phase (several thousand times less dense than water). To overcome the low density limitation, it is possible to significantly increase the polarization efficiency of gases using appropriately tuned circularly polarized laser beams, in the presence of vaporized alkali atoms (Rb, K) or other forms of 3He atoms.(12,13) In glass polarization chambers, the laser light is absorbed by the atoms and the energy is transferred to the nuclei by atomic collisions in the presence of a weak magnetic field. Hyperpolarized samples of 3He or 129Xe typically have an enhancement of four to five orders of magnitude above the Boltzmann equilibrium level (i.e., increasing polarization levels to 30–70% from 0.001%, for example), with a corresponding increase in observable signal. The enhanced magnetization can only be excited and observed once before returning to the Boltzmann equilibrium level, which must be taken into consideration in the design of imaging experiments. Both 3He and 129Xe have long T1 values (i.e., the half-life of the hyperpolarized magnetization), which enables their use in practical imaging studies, allowing time for transport of the gases to the MRI scanner and for inhalation in imaging studies. T1 values for 129Xe and 3He are tens of seconds in vivo, but T1 values are several minutes for 129Xe and several days for 3He in dedicated storage containers. Hyperpolarization enables imaging of inhaled 3He with a comparable spatial resolution to conventional 1H water imaging. Figure 3 shows 3He ventilation images acquired from a patient with chronic obstructive pulmonary disease (COPD), both before and following the inhalation of a bronchodilator, highlighting the regional nonuniformity of ventilation in this subject, and the ability to measure regional changes in gas delivery. 129Xe has significantly different properties than helium, most notably a smaller gyromagnetic ratio (γ129Xe=11.7 MHz/T) leading to an order of magnitude reduction in sensitivity. Functionally, while helium is largely nonlipid soluble and remains in the lung airspace, xenon is highly lipid soluble and has potential as a biosensor due to its affinity for and sensitivity to biological molecules.(14)

Hyperpolarized 3He ventilation images acquired from a COPD patient pre (
A recent review article provides a detailed overview of the diverse functional information that can be acquired with 3He and 129Xe hyperpolarized gas MRI.(15) Briefly, these inhaled gases can be used to indirectly visualize the airways down to the alveolar level and offer a quantification of ventilation,(16,17) partial pressure of oxygen,(18–20) gas diffusion(21–24) (and lung microstructure(21,25)), and gas velocities.(26) An emerging application of 3He MRI is for the imaging of inhaled superparamagnetic iron oxide particles.(9) The inhaled particles are detected via their direct perturbation of the static magnetic field,(27) and not via the more common mechanism of reduction in T1 or T2 relaxation times. Using conventional field mapping methods, based on the measurement of image phase, the static (B0) field is mapped at baseline and following the inhalation of the particles, using the 3He signals. The amount and distribution of iron particles is solved as an inverse problem based on the change in static field.(27) This method allows for the calculation of regional concentration of iron contrast agents on the airways walls simultaneously with direct imaging of the airways via the conventional 3He imaging. Although the use of hyperpolarized gases shows promise for future in vivo measurements of regional aerosol deposition, the need for specialized on-site production of hyperpolarized gases has limited its use. Also, diminishing supply of 3He and increased demand in government and industry applications may ultimately limit clinical and research applications of helium gas.(28)
Imaging ventilation and aerosol delivery with 1H water signal
The vast majority of MRI studies use the signal provided by hydrogen atom protons, that is, 1H. However, 1H MRI of the lung parenchyma, compared to most other tissues, is confounded by low water density (∼15% water content) and correspondingly reduced MRI signal intensity. Other important technical challenges include the heterogeneous micromagnetic field environment associated with complex air–tissue interfaces (which can rapidly dephase the MRI signal) and cardiac and respiratory motion artifacts. Breathing and pulsatile blood flow artifacts can be overcome with the use of respiratory gating and cardiac (ECG) gating, respectively, and and rapid imaging methods, which can effectively freeze these motions. Signal losses associated with heterogeneous magnetic field effects in the lung can be minimized either by reducing the signal decay from short T2* values using ultrashort echo time imaging or refocusing the decay due to T2* relaxation by employing spin echo imaging.(29–32) The low water density in the lungs necessitates a reduction in spatial resolution compared to other tissues, but several methods have been successfully developed to image ventilation using endogenous contrast mechanisms or to image the delivery of inhaled contrast agents.Regional ventilation can be measured using the changes in lung water density with breathing,(33,34) whereby the regional change in MRI signal intensity has been shown to be linearly related to regional ventilation,(34) although not directly reflecting the delivery of gas or particles.
Inhaled contrast agents
Oxygen is a paramagnetic MRI contrast agent that is capable of reducing the lung water T1 relaxation rates by ∼10%, which can be used to increase the lung parenchyma signal intensity by ∼20% using optimized T1-weighted experiments.(35–38) Oxygen-enhanced ventilation maps are generated by measuring the change in MRI signal intensity from baseline to following a short exposure (1–2 min) of 100% oxygen. It has been shown that the changes in T1 are the result of increased partial pressure of arterial oxygen,(39) and thus the oxygen enhanced imaging reflects the transfer of the gas to the blood and tissues, as opposed to just alveolar delivery.
There have been studies of inhaled aerosolized Gd-DTPA (gadolinium with diethylene triamine pentaacetic acid chelate), a standard clinical MRI contrast agent, for over 20 years. Gd-DTPA is limited in use only is those with severely impaired renal function. Like oxygen, Gd contrast agents are paramagnetic and reduce the T1 and T2 relaxation times of the water in the lung parenchyma, and thus can be used to quantify the regional delivery of the aerosol based on the change in signal intensity with ventilation of the agent. The vast majority of studies have utilized the reduction of T1 times with increasing contrast concentration to detect the agents. Early studies in animals showed the feasibility of measuring ventilation based on the changes in signal intensity.(40,41) Safety and pharmacokinetic studies of these aerosolized Gd-DTPA-based agents showed no changes in hemodynamics, histological effects, or induction of edema in rats.(42) Similar findings were shown in a pig model(43) and a healthy dog model,(44,45) and in a dog model of airway obstruction.(46) A modified Gd-DTPA aerosol was shown to yield a more homogeneous and larger deposition than previously used formulations,(47) again in animal models. Feasibility studies in humans, in the lone single study to date, have shown a similar degree of MRI signal enhancement with inhaled Gd-DTPA aerosols,(48) although no clinical studies have yet been performed. More recently, animal studies by Sood et al.(6,7) again confirmed the feasibility of delivering aerosolized Gd to lungs and the ability of MRI to measure the regional differences in contrast accumulation. These studies expanded significantly on previous works by including a quantification of the contrast accumulation in the lungs and kidneys, showing absolute amounts of agent delivery and alveolar absorption, glomerular filtration, and ultimately renal accumulation of the agent.
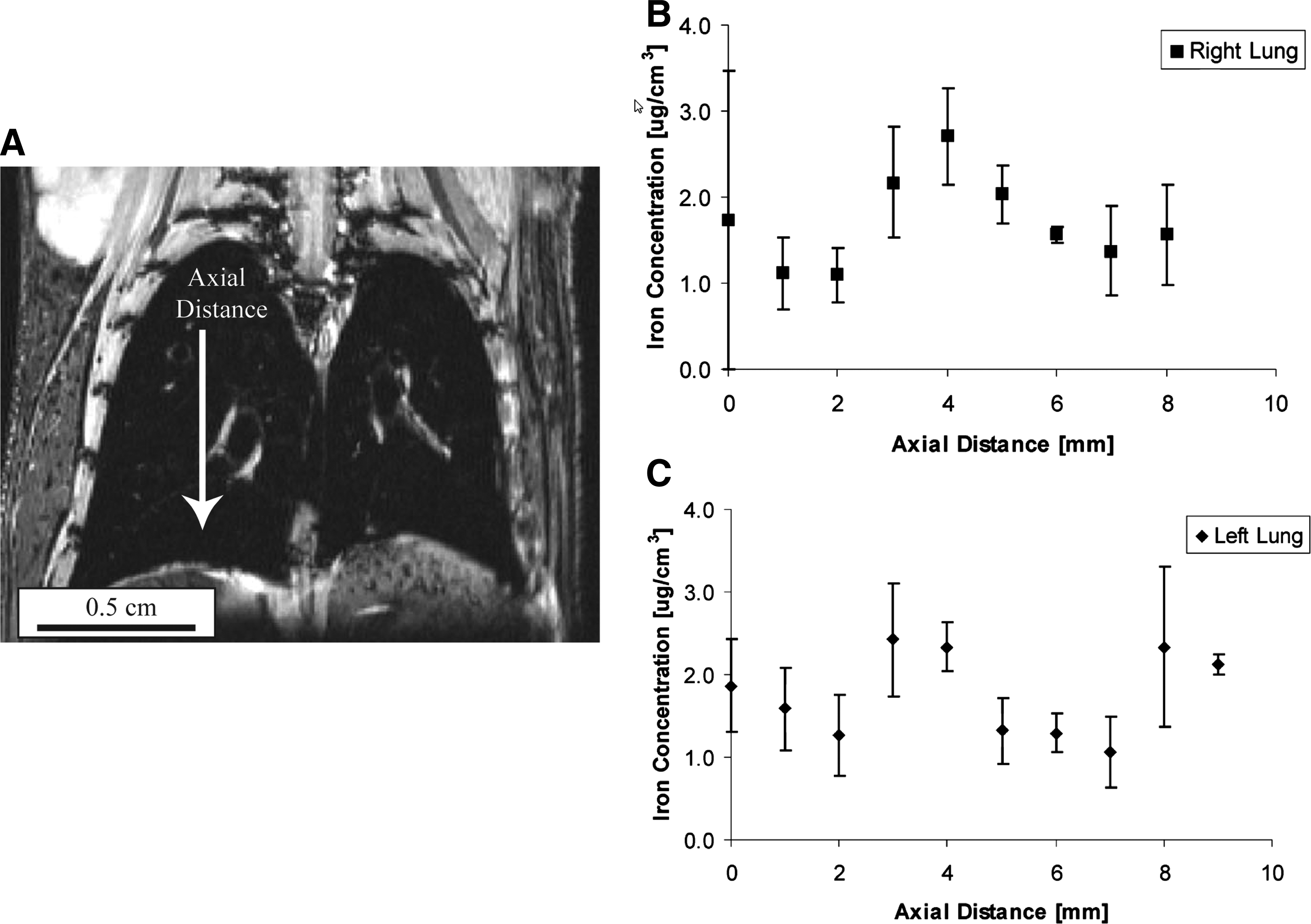
The delivery of aerosolized iron-particle contrast agents has also been studied with MRI. A small study in rabbits, to examine the feasibility of MR lymphography, illustrated that an inhaled iron colloid (cideferron) accumulated in the pulmonary lymph nodes, measured with MRI and confirmed with histology.(49) Changes in tissue T2 relaxation times, as opposed to T1, were used as the contrast mechanism in this study. More recently, the regional delivery of superparamagnetic iron oxide nanoparticles in the lungs has been illustrated in MRI studies of mice.(4) Regional concentration of contrast agent, c, was quantified (μg/cm3) using a calibration of the changes in T1 values to the concentration of nanoparticles (1/T1=1/T10+α·c), where T10 is the baseline relaxation time constant of the tissue (prior to delivery of the contrast agent), T1 is the measured relaxation time constant with contrast delivered and α is a calibration constant termed the relaxivity of the contrast agent. Figure 4 shows the average regional concentration of the inhaled particles in the right and left mouse lung, as a function of position from the base to the apex of the lungs. Deposition can be measured in three dimensions using MRI, but is shown here only as a function of position in a single dimension. A subsequent study from this group, using the same iron quantification methods, evaluated the feasibility of magnetically targeted delivery of high aspect ratio particles loaded with iron oxide nanoparticles, in 19 New Zealand white rabbits.(5) A static magnetic field placed externally over the right lung resulted in an increased right/left deposition ratio in the middle and basal lung regions, as shown in Figure 5.
(
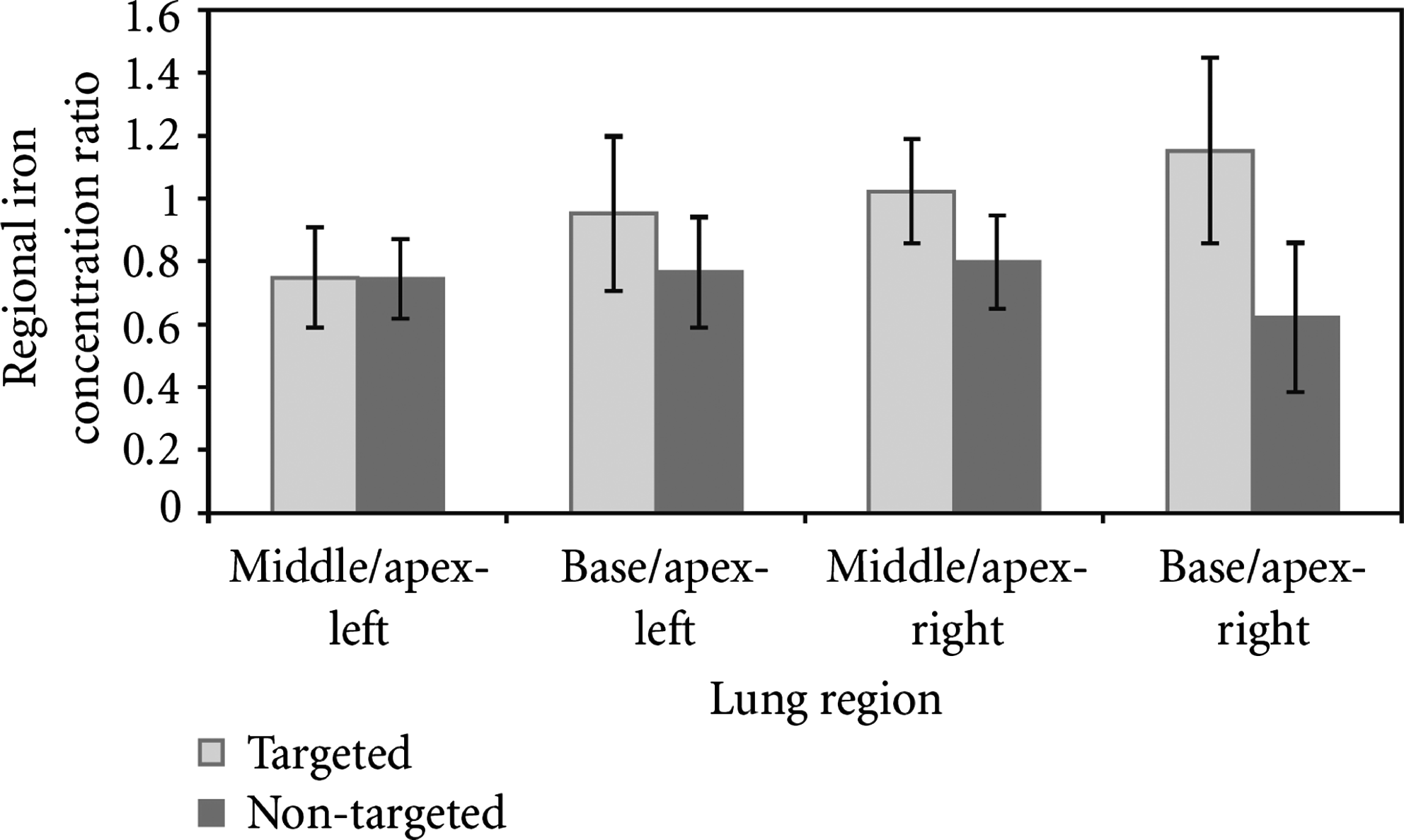
Ratios of iron concentration between middle and apical, and basal and apical regions of the left and right lungs of targeted and nontargeted rabbits. Error bars represent standard errors of the mean (reprinted with permission from the authors).
It should be noted that the use of contrast agents as a surrogate marker for aerosol deposition means that the MRI image gives the location of the contrast agent deposition, and does not give information regarding any other components contained in the aerosol particles. If the aerosol particles contain a therapeutic agent, for example, a drug, then it would be necessary to incorporate the MRI tracer into the drug to enable imaging of therapy delivery, which has been used in radionuclide experiments using PET imaging, for example.
Sensitivity of MRI to contrast agents
The vast majority of aerosolized contrast agent studies using MRI have been based on the reduction in relaxation times, which was observed as either a change in signal intensity or as change in the relaxation time itself, which has the potential to estimate agent concentrations. The sensitivity of MRI for the detection of contrast agents is determined primarily by the relaxivity of the agents (i.e., the change in relaxation time constant per amount of agent) and the achievable signal to noise ratio in the images. Assuming the goal is to quantify the concentration of the agent, sensitivity is governed by the ability to measure changes in relaxation times (e.g., the contrast agent concentration is given by c=(1/T1−1/T10)/α. For example, for a typical image voxel volume of ∼0.03 mL/voxel (i.e., 2 mm×2 mm×8 mm) there is sufficient signal to noise to routinely measure a reduction in T1 values by 10% in the lungs,(50) which would correspond to a tissue concentration of ∼0.09 mmol/L. This amounts to a relatively large amount (∼0.5 mg) of contrast agent per image voxel, or 13.3 mg/mL in the imaging region. These calculations were for the Gd-DTPA contrast agent (α=5 sec mmol/L−1), with T10=1.25 sec (i.e., 0.5 mg=0.089 mmol/L*938 g/mol*0.03 mL/voxel/1000 ml/L*0.2 mL of water/mL of lung space, where 938 g/mol is the molecular weight of Gd-DTPA and a water density of 20% in the lungs is assumed(51)). In contrast, the iron superparamagnetic particles used in the mouse study shown in Figure 4 gave rise to larger T1 effect (∼20% reduction in T1) in the mouse lung with 1.8 μg/mL,4 or three orders of magnitude less agent by mass compared to the Gd-DTPA agent. However, human lungs have volumes of several liters, indicating that even with the enhanced sensitivity per weight of agent offered by superparamagnetic iron oxide material, several milligrams of contrast agent must deposit with the aerosol inhaled into the lungs. Although this may be acceptable for some types of studies, it is too high to be considered feasible for typical inhaled pharmaceutical aerosol formulations, where often less than a milligram of therapeutic agent deposits in the lung. The future of MRI in the study of aerosol science, particularly in human studies, will thus likely depend on the development of more effective contrast agents, to significantly reduce the required dose of agent, in conjunction with optimized methods for their observation. In addition, although superparamagnetic iron oxide contrast agents are approved for human use by intravenous injection, their use via aerosol delivery would need regulatory consideration before widespread adoption is possible. Of course, if the delivered aerosol particles themselves exhibit magnetic susceptibility, then contrast agents may not be needed. Indeed, deposition of micrometer-sized iron oxide particles has been studied in vivo in rats using measurements of transverse magnetization relaxation time T2*.(8) In this study, a larger reduction in T2* measured in the lungs following ventilation with iron oxide particles corresponded to increased accumulation of the particles, with the particle concentration directly proportional to 1/T2*, measured in calibration phantoms. It should be noted that imaging of aerosol deposition using MRI does not suffer from the time limitations associated with the relatively short half lives of radionuclides. Indeed, if the aerosol particles themselves exhibit significant magnetic susceptibility, as in the case of iron oxide particles, it may be possible to explore the clearance and disposition of the deposited particles over longer times than is possible with decaying radionuclides. This is a topic for future research.
Summary
MRI has long been successfully used in human subjects to image lung tissue and ventilation therein. Although the deposition of paramagnetic aerosol particles has recently been measured directly using MRI, most inhaled aerosols do not exhibit sufficient magnetic susceptibility to allow their deposition to be measured in this manner. However, the addition of contrast agents to otherwise nonparamagnetic aerosol formulations, in principle, does give MRI the ability to quantify the spatial location of inhaled aerosol deposition. Indeed, this approach has been used in vitro and also in vivo in animal models by seeding particles with Gd-DTPA or superparamagnetic iron oxide. At present, the amount of contrast agent that must deposit in the lungs to achieve measurements of regional deposition is quite high (hundreds of mgs for Gd-DTPA, and several mgs for superparamagnetic iron oxide particles). Future work is needed if the required dose of contrast agent is to be reduced to the trace levels deemed necessary for MRI to be competitive with more traditional radionuclide aerosol deposition measurement methods.
Footnotes
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.