
Abstract
Abstract
Background:
Inhalation of hypertonic saline and mannitol improve mucociliary clearance in patients with bronchiectasis, but little is known about how the relative osmotic strengths of these compounds affect ciliary beat frequency (CBF) of ciliated human bronchial epithelial cells (HBEC). Our aim was to compare in vitro the direct effects of osmotically equivalent solutions on CBF of HBEC.
Methods:
HBEC were acutely (10, 30 min) exposed to comparable osmolar solutions of saline (0.03–0.48%), mannitol (0.19–3%) and dextran (10%–39.39%). Effects of higher % solutions, reversibility of responses, and prolonged treatments (15–20 h) were also compared. CBF was measured using digital videomicroscopy at baseline and at all time points.
Results:
CBF of HBEC increased significantly after acute exposure to mannitol (0.19%, 0.38%), decreased with dextran and remained unchanged with saline. Prolonged exposure to mannitol at high (3%, 6%) osmolar concentrations reversibly suppressed CBF. In comparison, acute and prolonged treatment with 39.39% dextran (equivalent to 3% mannitol) reduced CBF irreversibly. Furthermore, acute and prolonged treatment with 1% saline (equivalent to 6% mannitol) suppressed CBF with only the acute effect being reversible.
Conclusions:
Mannitol had a direct osmolarity-independent cilio-stimulatory effect at lower % solutions and a reversible cilio-inhibitory effect at higher % solutions, and prolonged exposure to mannitol inhibited CBF reversibly. Both the acute and prolonged effects of mannitol compared to dextran and saline on CBF of HBEC in vitro, imply a unique mechanism of action for mannitol on ciliary beating and might contribute to the improved clearance observed in mannitol-treated patients.
Introduction
Inhalation of dry powder mannitol (200–400 mg) resulted in increased mucociliary clearance in asthmatic and healthy subjects(9) and had a marked acute effect in patients with bronchiectasis.(10) Further studies in patients with bronchiectasis showed that mannitol helped patients to clear mucus within 2 h that would have taken 24 h to clear without mannitol.(11) In another study, mannitol (400 mg daily) improved cough clearance, and significantly improved the health status over 12 days in patients with bronchiectasis. This improvement was maintained for 6–10 days after cessation of treatment.(12) In cystic fibrosis patients, mannitol was shown to be equally effective as 6% hypertonic saline in improving ciliary and cough clearance.(6,13) Early studies of the direct effect of hypertonic saline on cilia, reported that the concentration of hypertonic saline should not exceed 7% because higher concentrations (12–14%) resulted in slowing of the cilia and irreversible ciliostasis.(14–18) Evidence from basic(19) and clinical studies indicated that the effect of hyperosmolar agents on clearance of mucus extends beyond the acute phase(7,11,12) stressing the importance of looking at CBF responses over time.
Proper in vitro comparisons of osmotically equivalent solutions on CBF of freshly isolated human bronchial epithelial cells (HBEC) are needed. Little is known about the relative osmotic strengths of mannitol and saline and how these compounds can directly affect the CBF of ciliated HBEC. Evaluating the direct effect of saline, mannitol, and dextran on CBF of HBEC could lead to a better understanding of how these agents can modify mucociliary clearance. Therefore, the aim of this study was to compare in vitro the direct effects of osmotically equivalent solutions of mannitol, saline, and dextran on CBF of normal HBEC. Acute and prolonged exposures were compared. The presented studies provide new insights into the direct (acute and prolonged) effects of hyperosmolar agents, specifically mannitol, on the function of ciliated HBEC. Some of the results of these studies have been previously reported in the form of an abstract.(20)
Materials and Methods
St. Joseph's Healthcare Ethics Review Board (#07-2832; May 3, 2007) and the Tissues and Archives Committee, London Health Sciences Centre and the University of Western Ontario Research Ethics Board (#12574E; December 20, 2006) approved this study and its protocols. Informed written consents and bronchial tissues were obtained from 20 patients undergoing lung surgery, ages 55–81 years. Bronchial airway segments distal to the diseased areas were harvested by the surgeon at LHSC following lung surgery (lobectomy). There were no patient identifiers, and other information about the subjects was not allowed to be collected. All reagents were purchased from Sigma (Sigma-Aldrich, Oakville, ON, Canada) unless otherwise stated.
Bronchial Epithelial strip isolation
Segments of bronchial tissue (≤0.5-cm diameter) were placed by the surgeon in a vial of cold (4°C) Earle's Balanced Salt Solution (EBSS, pH 7.4) and transported to our laboratory within 24 h. Tissues were rinsed, then trimmed and placed in Earl's Balanced Salt Solution (EBSS). Freshly isolated ciliated strips and clumps of epithelium were brushed using a 3-mm bronchial cytology brush and suspended in 5-mL EBSS at 37°C until examined within 1–2 h.
Measurement of CBF of bronchial cilia
CBF was determined at 37°C using a modified method of Rossman et al.(21) (Fig. 1). A 0.5-mL aliquot of the HBEC was transferred to a perfusion chamber that delivered perfusate at the rate of 0.25 mL/min. The CBF of HBEC was recorded using high-speed imaging (Redlake Inc., San Diego, CA, USA). Recordings were analyzed using ProAnalyst software (XCitex, Cambridge, MA, USA). Please view Figure 1 for details.
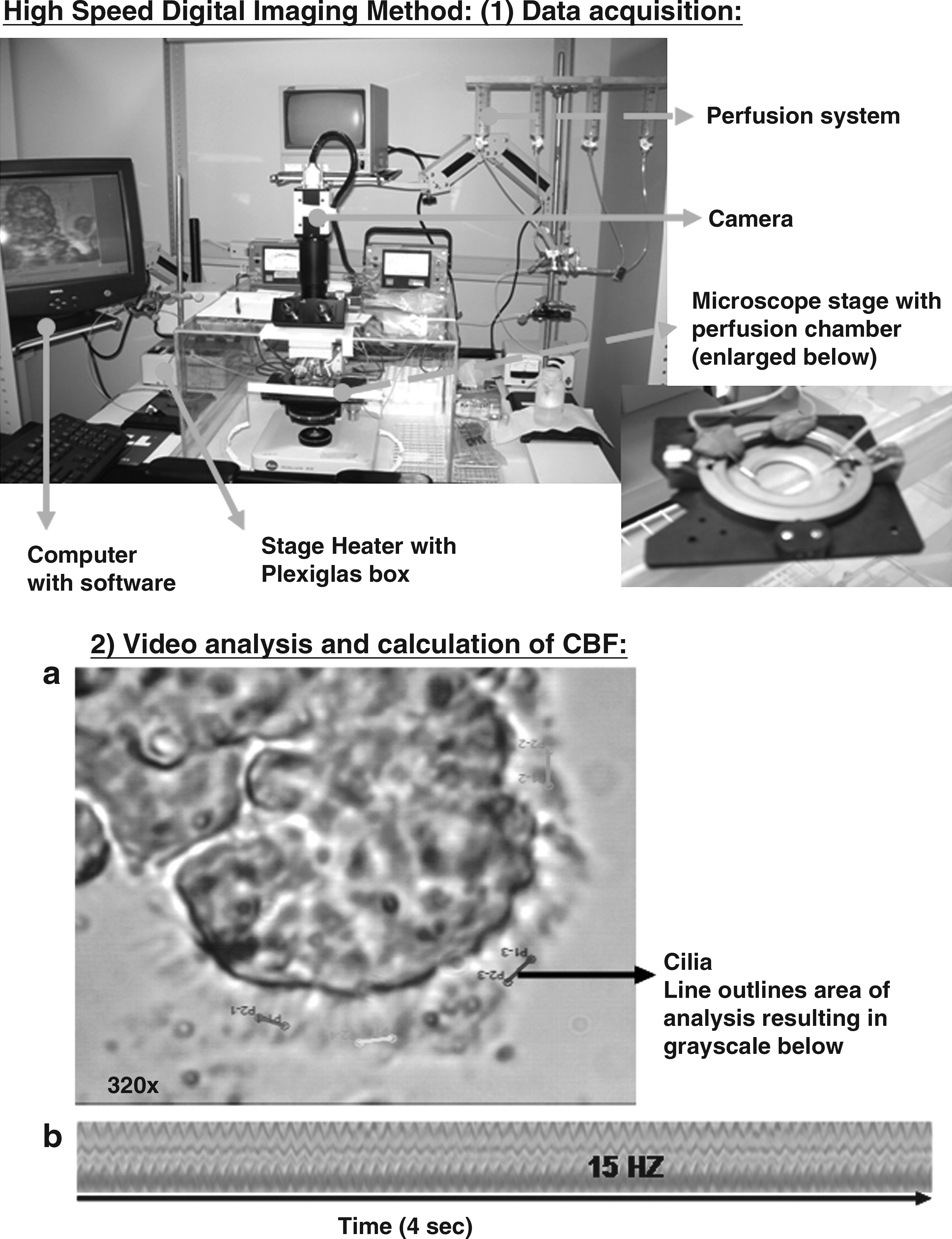
Measurement of CBF of bronchial cilia. High-Speed Digital Imaging Method: (1) Data acquisition: The Motion Analyzer System attached to the microscope (MotionScope 1000 S monochrome, High Speed Digital Imaging System from Redlake Inc.). A ciliated epithelium specimen was placed in a perfusion chamber (Dvorak-Stotler, Nicholson Precision Instruments Inc., Bethesda, MD, USA) attached to a gravity feed perfusion system that delivers perfusate at 0.25 mL/min. The chamber was placed under the phase contrast microscope (E. Leitz, Wetzlar, Germany). A Plexiglas enclosure and an air stream stage heater (Nicholson Precision Instruments Inc.) maintained the 37°C temperature. A high-speed digital camera and PCI application software, running in Windows 2000 (Redlake Inc.), was used for image acquisition. A video segment was recorded for each area. Each video segment was stored in a file for later retrieval and analysis (2). (2) Video analysis and calculation of CBF: the video recordings were analyzed using ProAnalyst video imaging processing software (XCitex). Areas on the edge of the epithelium with beating cilia are analyzed using the one-dimensional tracking algorithm included in the motion analysis software. A line was drawn across a segment of cilia (
Hyperosmolar agents used
The effect of comparable osmolar solutions (Table 1) of saline (NaCl), mannitol, and dextran T-40 (35,000–50,000, MP Biomedicals, LLC, USA) on CBF of HBEC was measured. Dextran, a neutral polymer that would not easily permeate human cells, was used as a control for mannitol and saline. We did not observe any changes in cell volumes (i.e., no shrinking and no swelling) after treatment with any of the osmolar agents and at all the concentrations tested.
All agents were prepared in Earl's Balanced Salt Solution (EBSS; 287.3 mosM) and osmolarity was measured on the Advanced MicroOsmometer model 3300 (Advanced Instruments Inc., Norwood, MA, USA). The pH of the perfusion solutions was recorded at 7.4.
ND, not determined; mosM, milliosmolar.
Protocol for in vitro measurement of CBF
The protocol involved two sequential perfusions: (1) baseline perfusion with EBSS, (2) exposure perfusion using one of the osmolar solutions. The chamber containing HBEC was perfused with EBSS (pH 7.4) for 10 min. Baseline CBF was recorded at 10 and 30 min. CBF was determined as the beats/s from 10–12 different sites, each consisting of strips of at least 8–10 intact ciliated cells. Baseline CBF was defined as the mean of all readings and expressed in Hz. CBF was also recorded from 10–12 sites at 10- and 30-min exposure to the different concentrations of hyperosmolar agent in EBSS (pH 7.4). In addition, to determine the reversibility of the effect of hyperosmolar agents on bronchial CBF, a 30-min washout perfusion with EBSS to remove the agent from the chamber was done for some samples and CBF was recorded. All measurements were taken in the absence of flow.
Prolonged exposure to hyperosmolar agents
Aliquots of HBEC were incubated with the agents or EBSS for 15–20 h at 37°C, and CBF was determined.
Graphing and data analysis
All data were expressed as mean±SEM (standard error of the mean). Data were plotted and analyzed using Prism 4 (GraphPad Software Inc., San Diego, CA, USA). The mean baseline CBF for the subjects studied was 13.6±0.5 Hz (n=20 subjects). Baseline CBF (Hz) values before the various treatments are listed in Table 2. Final results were expressed as % baseline CBF and were analyzed as indicated in figure legends. For all tests, a p-value <0.05 was considered statistically significant.(22)
n, number of subjects.
Results
Rationale for choosing the osmolar solutions tested in this study
Because mannitol and hypertonic saline can modify mucus clearance in patients with lung disease,(6,12,13,23–25) we elected to study the direct effects of mannitol on CBF of HBEC in vitro and compare it to equivalent osmolar solutions of saline and dextran. Hypertonic saline is ionic and charged, and thus is absorbed rapidly from the airway mucosa and could easily permeate human cells. In contrast, mannitol is a sugar and is ion free with a low permeability index, and could sustain the osmotic effect for longer than hypertonic saline.(26) Dextran is a neutral polymer that would not easily permeate human cells and could mimic the osmotic effects of mannitol.(7,27) The mannitol osmolar solutions (0.19–6%) that we used in vitro correspond to those used in clinical inhalation studies,(6,9,10,12,28) namely, mannitol at 200–600 mg. We based our calculations on a deposition rate of inhaled powder of 10%(29) and a distribution volume of 100 mL taking into account the geometric factors of the lung and the cumulative volume of deposition in the bronchi (airway generations 3–8).(30) The saline and dextran solutions were prepared at comparable osmolarity to the mannitol solutions (Table 1).
Acute and prolonged exposure to mannitol, dextran, and saline
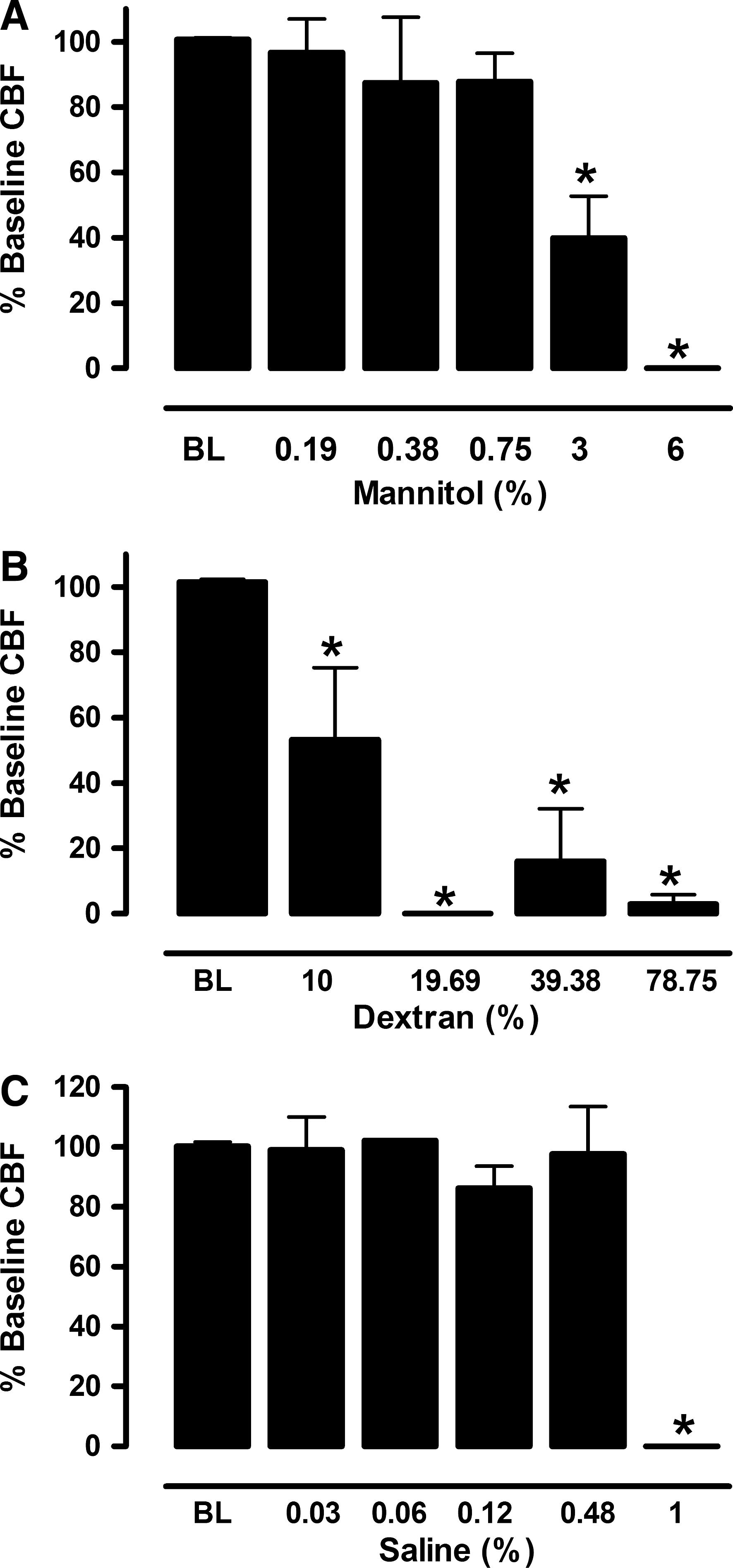
CBF increased after acute (10- and 30-min) exposure to mannitol and decreased with dextran. No significant change in CBF occurred with hypertonic saline (Fig. 2). Prolonged (15–20 h) exposure to high mannitol solutions (3% and 6%) suppressed CBF of HBEC (Fig. 3A) significantly (p<0.01) compared to baseline (BL). Prolonged (15–20 h) exposure to dextran at all concentrations tested suppressed CBF of HBEC (Fig. 3B) significantly (p<0.01 compared to BL). In comparison, only extended (15–20-h) exposure to a high % saline (1% saline) suppressed CBF of HBEC (Fig. 3C) significantly (p<0.01).

Effect of mannitol, dextran and saline on CBF of ciliated HBEC. CBF (Hz) was measured from the same sites (10–12 epithelial cell strips) before and after perfusion with mannitol, dextran or saline for (
The effect of prolonged (15–20 h) treatment with (
Reversibility of exposure to mannitol, dextran, and saline
Reversibility of CBF to acute (10-min) and prolonged (15–20 h) exposure to high % Mannitol (3% and 6%) is shown in Figure 4. Acute exposure of HBEC to 3% mannitol did not affect CBF, but prolonged exposure of HBEC to 3% mannitol suppressed CBF significantly (p<0.01 compared to BL). Both the acute and prolonged exposure of HBEC to 6% mannitol significantly suppressed CBF (p<0.01 compared to BL). The effect of mannitol was reversible after washout (post 3% and post 6%) of HBEC with EBSS for 30 min (Fig. 4). Acute and prolonged exposure of HBEC to 39.38% dextran significantly suppressed CBF (p<0.01 compared to BL) as shown in Figure 5. The effect of dextran was not reversible after washout (post 39.38%) of HBEC with EBSS for 30 min (Fig. 5). Acute (10-min) and prolonged (15–20-h) exposure to 1% saline suppressed CBF of HBEC significantly (p<0.01 compared to BL). Only the acute effect of 1% saline was reversible. Prolonged exposure of HBEC to 1% saline was not reversible after washout with EBSS for 30 min (Fig. 6).
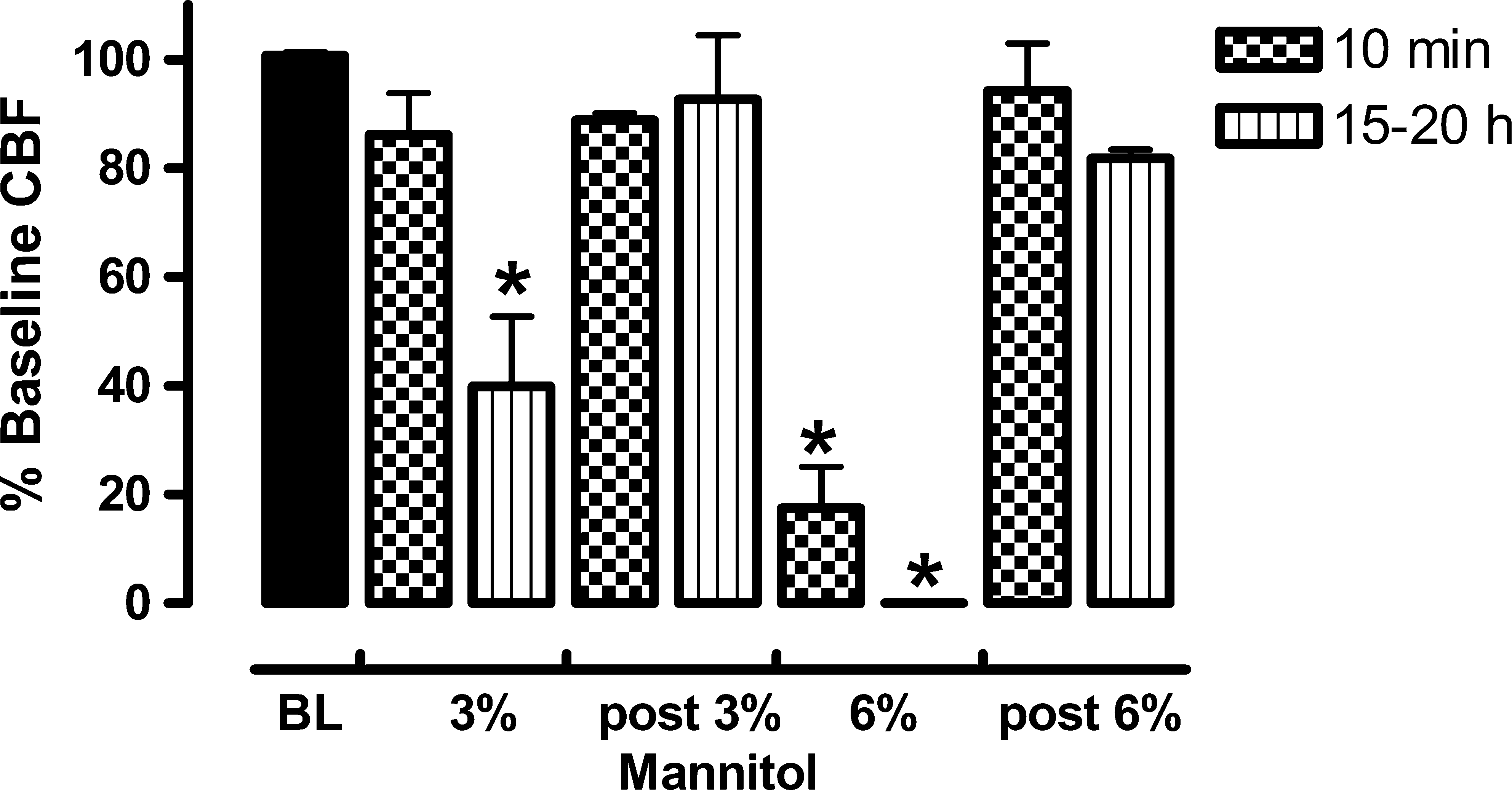
Reversibility of CBF of ciliated HBEC to acute (10 min) and prolonged (15–20 h) exposure to high % Mannitol (n=2–8). Each CBF (Hz) value was measured from 10–12 epithelial cell strips treated with mannitol (3%–6%) compared to BL. Reversibility (post %) of the depressed CBF response was determined by measuring CBF after reperfusion with EBSS for 30 min. Data is shown as % baseline CBF (mean±SEM of n where n=number of subjects). *p<0.001, ANOVA followed by Dunnett's Multiple Comparison Test (p<0.01 compared to BL).
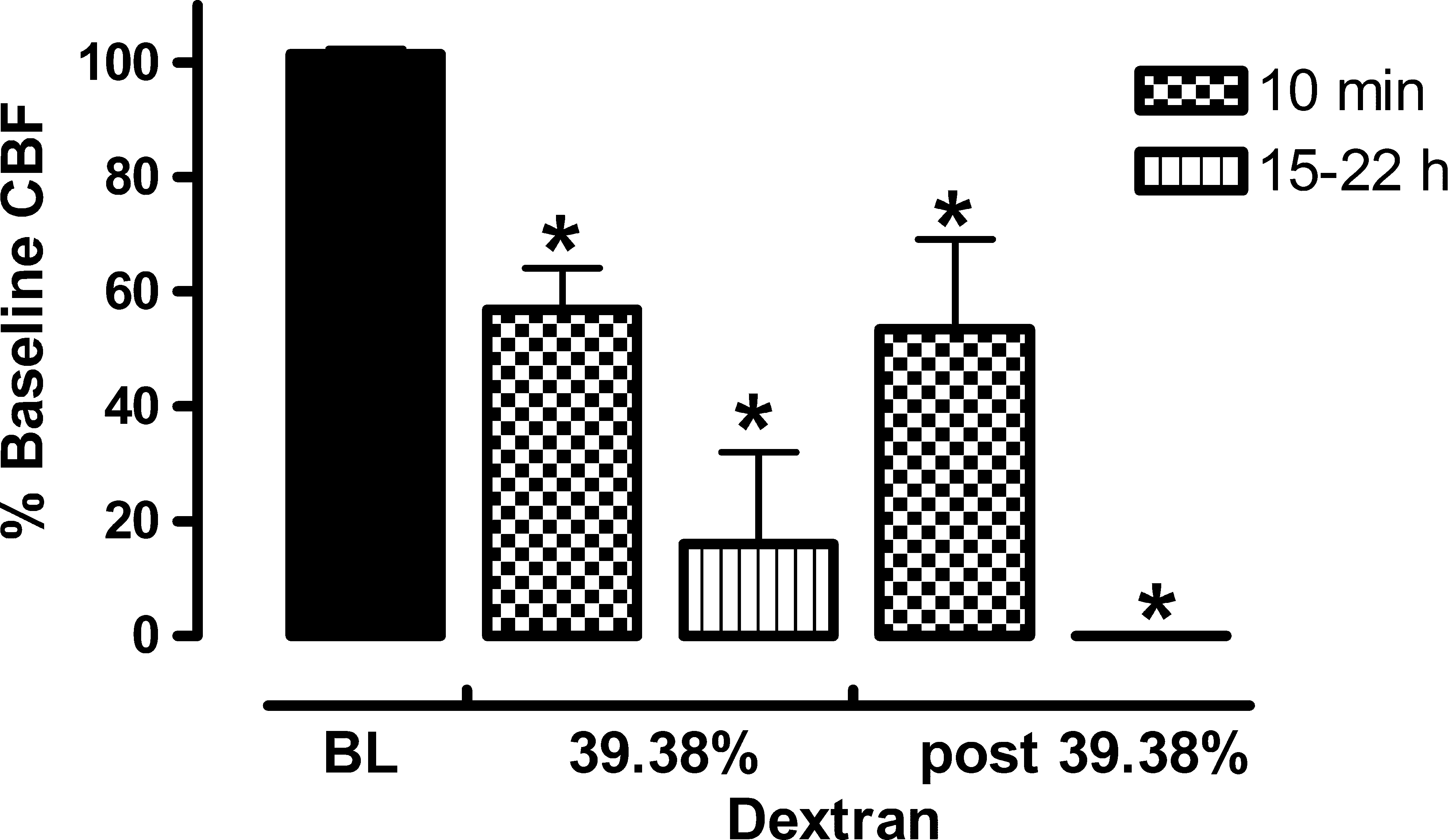
Reversibility of CBF of ciliated HBEC to acute (10 min) and prolonged (15–20 h) exposure to 39.38% Dextran (n=5–6). Each CBF (Hz) value was measured from 10–12 epithelial cell strips treated with dextran compared to BL. Reversibility (post %) of the depressed CBF response was determined by measuring CBF after reperfusion with EBSS for 30 min. Data is shown as % baseline CBF (mean±SEM of n where n=number of subjects). *p<0.0001, ANOVA followed by Dunnett's Multiple Comparison Test (p<0.01 compared to BL).
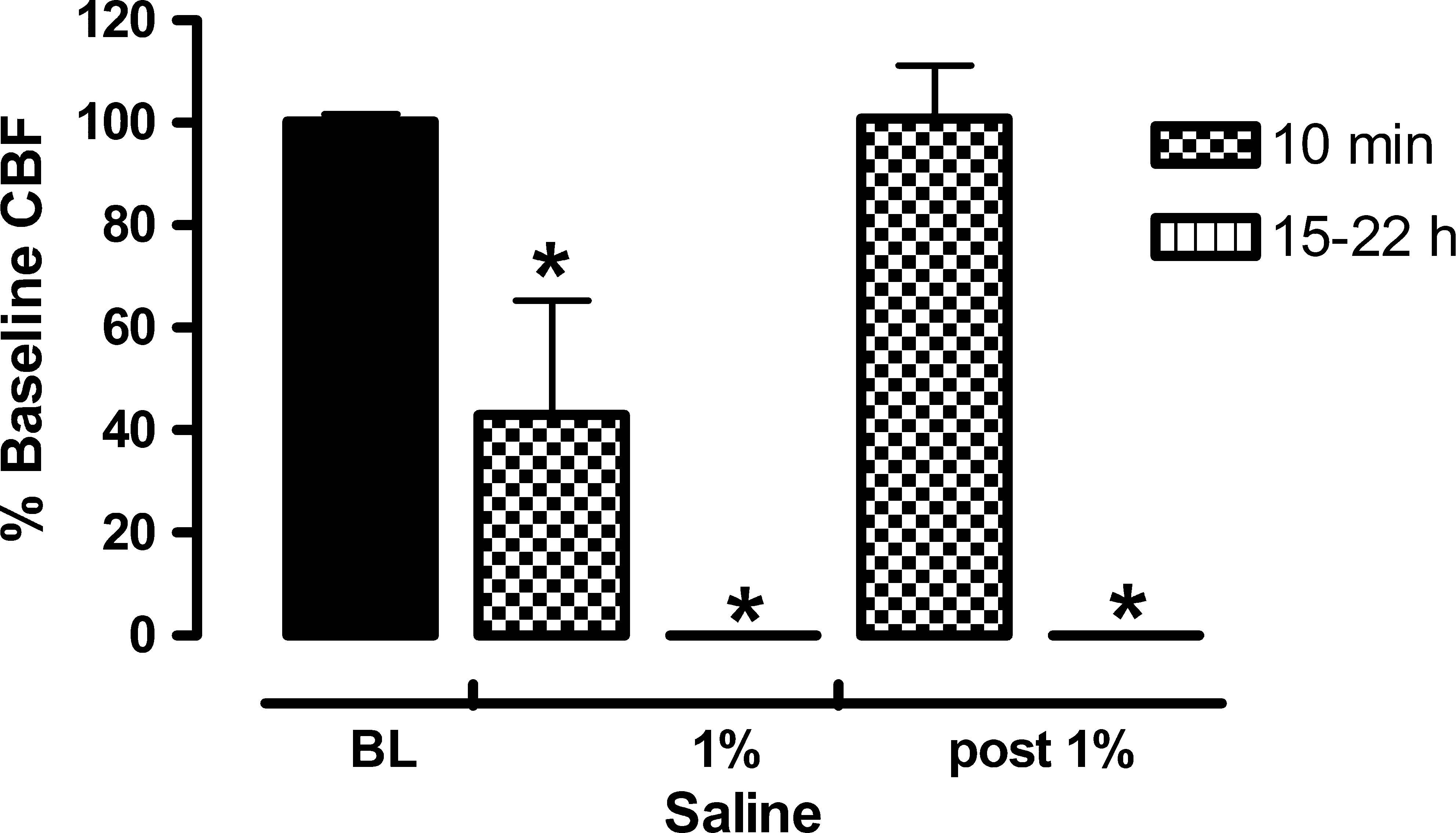
Reversibility of CBF of ciliated HBEC to acute (10-min) and prolonged (15–20-h) exposure to 1 % saline (n=2–3). Each CBF (Hz) value was measured from 10–12 epithelial cell strips treated with saline compared to BL. Reversibility (post %) of the depressed CBF response was determined by measuring CBF after reperfusion with EBSS for 30 min. Data is shown as % baseline CBF (mean±SEM of n where n=number of subjects). *p<0.0001, ANOVA followed by Dunnett's Multiple Comparison Test (p<0.01 compared to BL).
Discussion
The mucociliary system consists of the cilia, periciliary fluid layer, and mucus. The cilia beat in a coordinated fashion and interact with the mucus that is transported up the respiratory tract. Increased clearance occurs due to increased CBF, reduced viscosity of mucus, reduced mucus load, or a combination of these factors. Clinical studies have shown that inhalation of hypertonic saline and mannitol are well tolerated in patients with airway diseases and improve lung function in patients with cystic fibrosis.(5–8) Other sugars such as dextran and lactose have also been suggested to be as effective in clearing mucus through the same mechanism as mannitol.(7) Suggested mechanisms of action of hyperosmolar agents include (1) creating an osmotic gradient that increases water in the airway surface liquid, (2) alteration of mucus properties by affecting the viscosity and adhesiveness of the mucus, and (3) increasing the interaction of cilia with the mucus leading to increased CBF.(7) In this study we measured the direct effects of comparable osmolar solutions of mannitol, dextran, and saline on CBF of freshly isolated ciliated HBEC. When comparing equivalent osmolar solutions, CBF of HBEC increased (15–22%) after acute (10- and 30-min) exposure to mannitol (0.19 and 0.38%; 297.5 and 309.5 mosM, respectively) and decreased (13–43%) with dextran (10–39.38%; 297.5–466 mosM), whereas no significant change was observed with saline (0.03–0.48%; 297.5–466 mosM). Acute (10-min) exposure to 6% (630 mosM) mannitol suppressed CBF of HBEC, but this effect was reversible when cells were reperfused with EBSS. When comparing the effects of prolonged (15–20-h) equivalent osmolar solutions of mannitol (0.19–6%), dextran (10–39.39%), and saline (0.03–1%) on CBF of ciliated cells, only higher mannitol (3% and 6%) and saline (1%) osmolar solutions suppressed CBF of HBEC, whereas all the tested osmolar solutions of dextran suppressed the CBF of HBEC. The prolonged (15–20 h) exposure to 39.38% dextran (466 mosM) and 1% saline (630 mosM) suppressed CBF of HBEC irreversibly, whereas the mannitol effect of reducing CBF at equivalent osmolar solutions of 3% (466 mosM) and 6% (630 mosM), respectively, was reversible. Therefore, when tested in vitro on HBEC, mannitol had a direct osmolarity-independent cilio-stimulatory effect at lower % solutions and a reversible cilio-inhibitory effect at higher % solutions, and prolonged exposure to mannitol inhibited CBF reversibly. Both the acute and prolonged effects of mannitol compared to dextran and saline on CBF of HBEC in vitro, suggest a unique mechanism of action for mannitol on ciliary beating, and might explain the improvement in mucociliary clearance observed in lung disease patients treated with mannitol.(6–10)
Acute and prolonged exposure to mannitol, saline, and dextran
The increased CBF of HBEC treated with mannitol in vitro is in confirmation with what was observed in clearance studies earlier in vivo. Inhalation of dry-powder mannitol (200–400 mg) increased mucociliary clearance in asthmatic and healthy subjects,(9) and had a marked acute effect in patients with bronchiectasis.(10) Further studies in patients with bronchiectasis showed that mannitol helped patients to clear mucus within 2 h that would have taken 24 h to clear without mannitol.(11) In addition, inhalation of mannitol (400 mg) improved cough clearance, and significantly improved the health status over 12 days in patients with bronchiectasis. This improvement was maintained for 6–10 days after cessation of treatment(12) indicating a prolonged response. This in vivo prolonged response could be comparable to the washout (post %) effects on CBF of HBEC observed after acute and prolonged mannitol (3% and 6%) treatment, or to the effects of lower % mannitol (0.19–0.38%), which showed a significant rise in CBF of HBEC. In an in vitro study, adding sodium chloride to sputum from patients with cystic fibrosis and bronchiectasis enhanced its transportability on the mucus-depleted bovine trachea, but incubating sputum or respiratory mucus in hypotonic solutions had a detrimental effect. The transport of sputum by cilia was also increased by increasing the osmolality of the gel by adding the nonelectrolytes glucose, mannitol, and urea, or causing water loss by evaporation.(31) In our in vitro study, only mannitol caused an increase in CBF of HBEC compared to saline and dextran, indicating a direct effect with a unique mechanism of action for mannitol. Early studies of the direct effect of hypertonic saline on cilia, reported that hypertonic saline should not exceed 7% because higher concentrations (12–14%) resulted in slowing of the cilia and irreversible ciliostasis.(13–16,18) In our in vitro study, the cutoff for reduced CBF of HBEC was following treatment with 1% saline, a concentration comparable to the in vivo reported cutoff. In a study where CBF in excised mouse trachea was monitored by varying mucosal shear, CBF increased in response to step increase in shear, and was reduced by mannitol (2.4%), and Dextran (2% and 10%). However, mannitol addition led to prolonged CBF stimulation following the shear challenge with respect to the control stressing the importance of looking at CBF responses beyond acute exposure.(19) Our in vitro results and evidence from clinical studies(7,11,12) also indicated that the effect of hyperosmolar agents extended beyond the acute phase. Although we did not measure the viscosity of the various perfusion solutions, we did observe that all the mannitol and dextran solutions were rather viscous compared to the saline solutions; however, we only saw increased CBF with mannitol indicating that mannitol's direct effect is unique and independent of the viscosity of the solutions.
Reversibility of exposure to mannitol, dextran, and saline
A common in vivo feature of both hypertonic saline and mannitol is that they both can hydrate the airway lumen and reduce the entanglements that mucins form, with the potential for the physical properties of mucus to be altered in favor of clearance.(7) An increase in mucus transport associated with an increase in water has been shown in animal studies in vivo.(32) In a recent study investigating the effect of increasing doses of mannitol and repetitive coughing on the sputum physical properties in bronchiectasis patients, inhaled mannitol and coughing was shown to improve the sputum physical properties in these patients, and this effect was not dose dependent. Changes in sputum properties did not predict efficacy of mucociliary and cough clearance,(28) indicating that the function of ciliated cells might play a bigger role in the effect of mannitol in vivo and in vitro. In comparison, when the effect of hyperosmotic stress on airway epithelial cells was investigated in vitro, hyperosmotic solutions (up to 700 mosM) of the ionic compounds NaCl, NaBr, or LiCl and the nonionic compounds xylitol or mannitol all caused a reversible opening of the tight junctions in 16HBE14o-cultures, resulting in increased permeability of the paracellular pathway and in increased transepithelial water transport. Electrolytes had stronger effects than nonelectrolytes on permeability, but cilia function was not investigated.(33) Earlier studies showed that hyperosmolar agents stimulated the release of inflammatory mediators that could affect CBF of airway epithelial cells.(34–37) Hyperosmotic stress induced production of the inflammatory mediator IL-8 in human intestinal epithelial cells,(38) and IL-8 inhibited isoproterenol-induced increase in CBF in bovine bronchial epithelial cells.(39) Our results and the above studies collectively indicate that a rise in CBF following treatment with mannitol could contribute to the observed improved clearance in lung disease patients. In addition, reversible changes in epithelial cell permeability and the possibility that the release of mediators due to osmotic stress can occur in HBEC cells in vitro could explain the observed reduced CBF of HBEC to mannitol (3% and 6%), saline (1%) and dextran, with the effect of mannitol (acute and prolonged) being reversible.
In this study, acute exposure to mannitol, in comparison to dextran and saline, significantly increased CBF of HBEC in vitro. Prolonged exposure to mannitol suppressed CBF at high (3%, 6%) osmolar concentrations, but this effect was reversible. Both the acute and prolonged effects of mannitol on CBF of HBEC suggest a unique mechanism of action for mannitol on ciliary function. The increase in CBF after acute exposure of ciliated epithelial cells to low % solutions of mannitol but a reversible decrease in CBF after prolonged exposure to high % mannitol solutions should be further investigated. In addition, these observations of the effects of mannitol on CBF of HBEC may indicate a role for a direct effect on mucociliary clearance with relevant clinical implications knowing that mannitol, in addition to its use to treat lung disease patients(7,8,24,25,28) and in diagnosis,(40) could also be used as an excipient for inhaled products.(41–43)
Footnotes
Acknowledgments
The authors are grateful to Drs. Richard Inculet and David McCormack, and the Tissue and Archives Committee, Department of Pathology, at the London Health Sciences Centre (ON, Canada) for providing the bronchial tissues. This work was supported by the Ontario Thoracic Society Block term grant 2007–2008. Asma Yaghi was supported by a postdoctoral Fellowship (2007–2009) from the Father Sean O'Sullivan Research Centre, St. Joseph's Healthcare Hamilton, Ontario, Canada.
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.