
Abstract
Abstract
The success of inhalation therapy is not only dependent upon the pharmacology of the drugs being inhaled but also upon the site and extent of deposition in the respiratory tract. This article reviews the main mechanisms affecting the transport and deposition of inhaled aerosol in the human lung. Aerosol deposition in both the healthy and diseased lung is described mainly based on the results of human studies using nonimaging techniques. This is followed by a discussion of the effect of flow regime on aerosol deposition. Finally, the link between therapeutic effects of inhaled drugs and their deposition pattern is briefly addressed. Data show that total lung deposition is a poor predictor of clinical outcome, and that regional deposition needs to be assessed to predict therapeutic effectiveness. Indeed, spatial distribution of deposited particles and, as a consequence, drug efficiency is strongly affected by particle size. Large particles (>6 μm) tend to mainly deposit in the upper airway, limiting the amount of drugs that can be delivered to the lung. Small particles (<2 μm) deposit mainly in the alveolar region and are probably the most apt to act systemically, whereas the particle in the size range 2–6 μm are be best suited to treat the central and small airways.
Introduction
The aim of this article is to review key studies of aerosol deposition in health and disease. Because of the large amount of studies undertaken in this area, this review will focus on human studies and primarily on those that used nonimaging techniques to study deposition.
Deposition Mechanisms
It is widely accepted that the main mechanisms affecting aerosol transport and deposition in the human lung include inertial impaction, gravitational sedimentation, and Brownian diffusion, and to a lesser extent turbulent flows, interception, and electrostatic precipitation.
Inertial impaction
Inertial impaction affects mainly particles that are larger than 5 μm and refers to the particle's inability to follow sudden change in gas flow direction such as in the upper airway and at airway bifurcations. Each time the flow changes direction, the momentum of the particles tends to keep them on their existing trajectories, causing the particles to deviate from the air streamlines and to eventually impact on airway walls. The deviation of the particle from the air streamline, and therefore its probability to deposit on an airway wall, is greater the larger the particle mass and the greater the flow rate. Such probability can be expressed as a function of the Stokes' number (Stk), defined by
where dp and ρp are the particle diameter and density, respectively; u and μ are the mean velocity and dynamic viscosity of the carrier gas, respectively; and d is a characteristic length equal to the diameter of the airway. The higher the Stokes' number, the more efficient the inertial transport and the more likely that particles will deposit by inertial impaction.
Gravitational sedimentation
Gravitational sedimentation refers to the settling of particles under the action of gravity and occurs mainly in small airways and alveolar cavities where the distance to be covered by the particles before touching the walls is small. The terminal settling velocity of the particles (vs) is expressed by
where g is gravitational acceleration. Deposition by sedimentation increases both with increasing particle size and with increasing particle residence time in the airways and alveoli. This deposition mechanism is most effective for particle in the size range of 1–8 μm, while larger particles mainly deposit by inertial impaction and smaller particles by Brownian diffusion.
Brownian diffusion
Deposition by Brownian diffusion results from the random motions of the particles caused by their collisions with gas molecules and is most effective in the acinar region of the lung where air velocities are low. Unlike deposition by impaction and sedimentation, which increase with increasing particle size, deposition by Brownian diffusion increases with decreasing particle size and becomes the dominant mechanism of deposition for particles less than 0.5 μm in diameter. Deposition by Brownian diffusion is proportional to the Browninan diffusion coefficient DB defined by
where k is the Boltzmann's constant, T is the absolute temperature, and c is the Cunningham's correction factor that accounts for the decreased air resistance caused by slippage when the particle diameter comes close to the mean free path of the gas molecules.
Turbulent mixing
Turbulent mixing affects aerosol deposition mainly in the upper respiratory tract and the large airways. Such mixing refers to the irregular fluctuations or mixing undergone by the fluid in a turbulent regime, which cause the fluid speed and therefore the trajectories of particles to continuously undergo changes in both magnitude and direction and to eventually deposit on airway walls. Turbulent flows can be described in terms of their mean values over which are superimposed the fluctuations. Deposition due to turbulent mixing results from the flow fluctuations while deposition by inertial impaction is affected by the mean flow.
Interception
Interception is the mechanism by which particles, while following the mainstream flow, come into contact with an airway wall because of their shape and size. Although negligible for spherical particles, this is a dominant mechanism for elongated particles such as fibers.
Electrostatic precipitation
Electrically charged particles close to airways surfaces induce image charges on the surface. Charged particles are then electrostatically attracted to the airway walls, and as a consequence, deposition of charged particles may be greater than that of neutral particles.
Aerosol Deposition in Healthy Lungs
Total deposition in the human lung has been widely studied,(4–7) likely because it can be evaluated relatively simply by measuring the number of inspired and expired particles in each breath using photometer techniques. The main benefit of these measurements is that, with the use of monodisperse nonhygroscopic particles and well-controlled breathing patterns, both the effect of particle size and breathing patterns on total deposition can be assessed in a systematic manner. Representative data are shown in Figure 1 and illustrate the effect of residence time on total deposition.(5) Residence time in these experiments was increased by increasing the tidal volume from 1000 to 2000 mL while keeping the flow rate constant at 250 mL/sec. As such, not only residence time but also penetration of the aerosol in the lung was increased. All curves show a minimum for particle sizes around 0.5 μm, a size for which none of the main mechanisms of deposition are effective for particle transport. For particle larger than 0.5 μm, deposition increases with increasing particle size because of increased gravitational and inertial transport, while for particles smaller than 0.5 μm in diameter, deposition increases with decreasing particle size because of increased diffusive transport. For a given particle size, the increase in deposition with increasing tidal volume, that is, with increasing depth of inhalation and increasing residence time, reflects the increased deposition by Brownian diffusion for small particles and by gravitational sedimentation for large particles, those two mechanisms being time-dependent and most effective in the lung periphery where air velocities are low and airspaces dimensions are small. It is unlikely that any deposition increase at a given particle size result from increased deposition by inertial impaction, as flow rate was kept constant in these experiments.
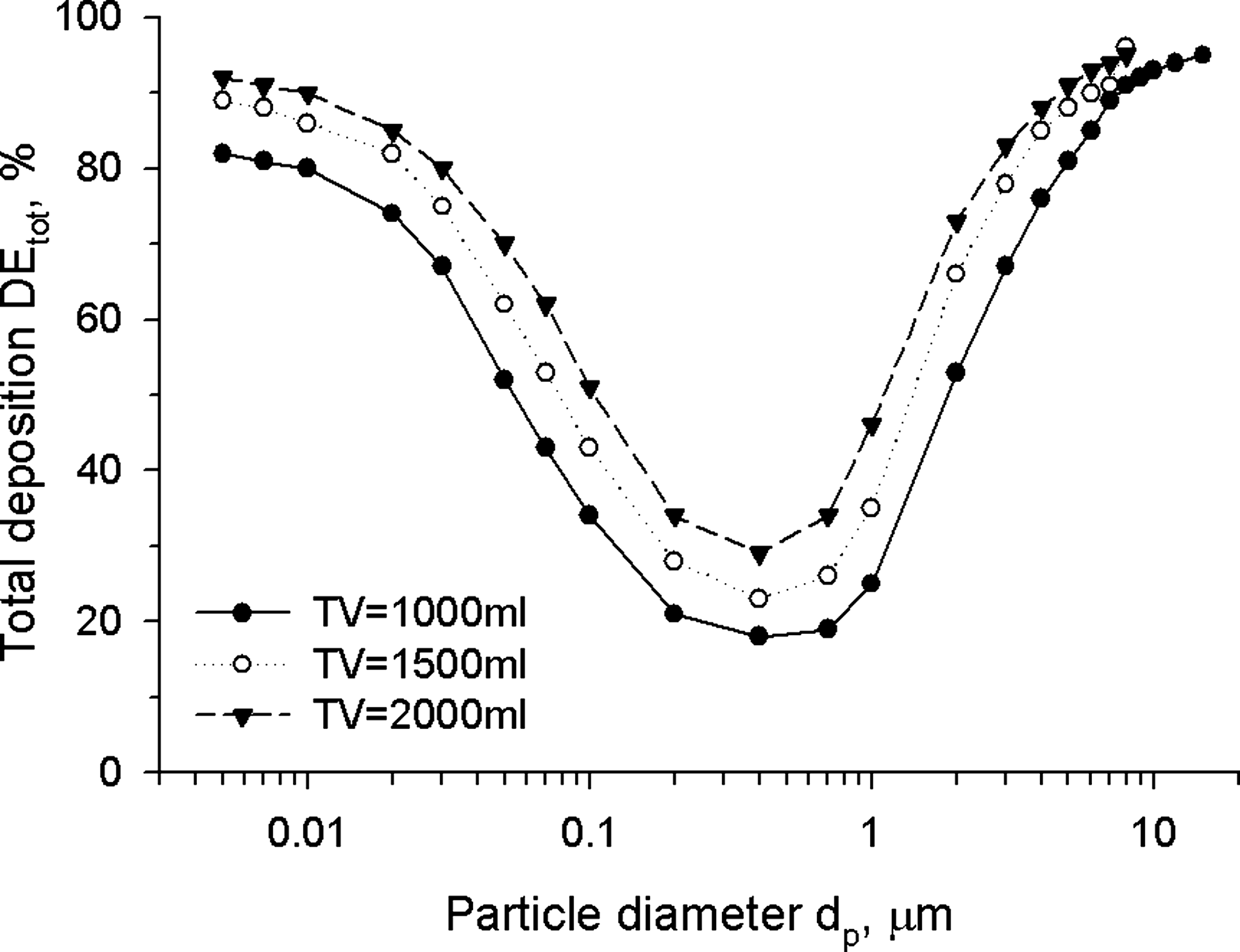
Total deposition as a function of particle diameter at a constant flow rate of 250 mL/sec and variable tidal volume (TV). Data are averaged experimental data obtained in healthy adults by Heyder et al.(5)
In the late 60s, Altshuler(8) showed that the bolus technique was well suited for studying aerosol dispersion and deposition in the human lung. The technique has since then been used by numerous investigators.(9–17) It consists of inserting a small amount of aerosol, a bolus, at a predetermined point in the subject's inspiratory volume and analyzing the distribution of the aerosol bolus during the subsequent expiration. Data from aerosol bolus inhalations provide insight in total deposition measurements by probing deposition at different depths within the lung. Indeed, a bolus inserted early in the inspiratory volume probes the lung periphery while a bolus inserted late in the inspiratory volume probes more proximal lung regions. The depth reached by the bolus is usually referred to as the penetration volume (Vp) and is defined as the volume of particle-free air inhaled from the mode of the bolus to the end of inspiration. In normal subjects, for Vp>100 mL, aerosol bolus deposition has been shown to increase linearly with depth of inhalation of the bolus within the lung (Fig. 2A).(12,16,18,19) For particle size between 0.5 and 2 μm, it has been shown that deposition in the proximal region of the lung (Vp≤200 mL) is similar, whereas deposition in the lung periphery increases with increasing particle size because of the increase in the rate of deposition by gravitational sedimentation. Indeed, when these bolus inhalations were repeated in the absence of gravity during parabolic flights, there was no significant difference in deposition between these particles sizes at any given penetration volume.(20)
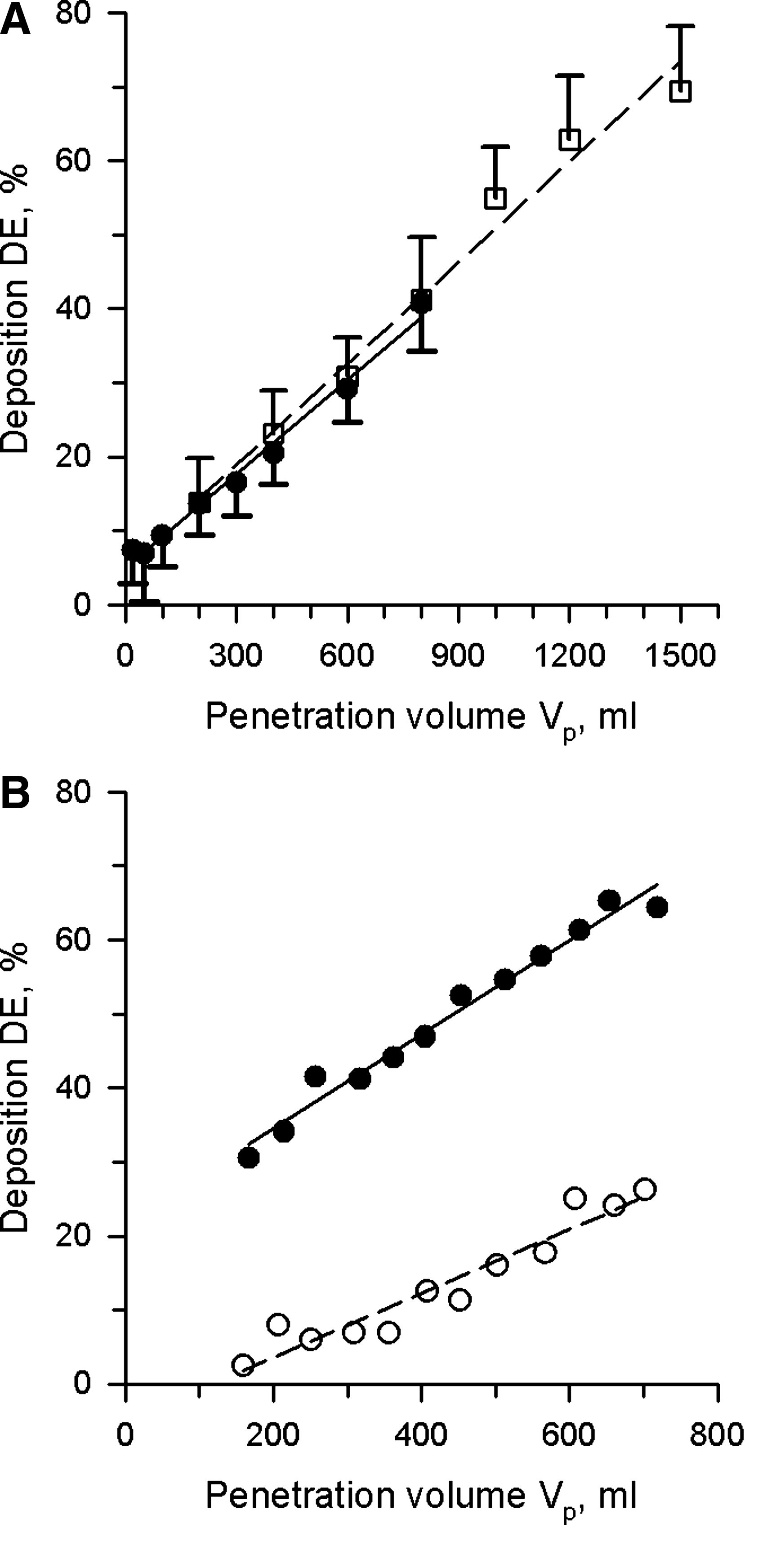
Deposition of aerosol bolus as a function of penetration volume. (
The bolus technique has also been used to estimate local surface dose of deposited aerosols.(17) By delivering small boli of 1, 3, and 5 μm-diameter particles in 50 mL increments to lung depths ranging between 100 and 500 mL, Kim et al.(17) showed that surface dose was larger at shallow penetration volumes (Vp<200 mL) compared to deeper lung regions (Vp=200–500 mL), and that such difference increased with increasing particle size (Fig. 3). Such information provides useful insight when one needs to assess therapeutic effects of inhaled drugs at the tissue level. Indeed, even if aerosol deposition is higher in the alveolar region than in the proximal conducting airways, the marked increase in surface area toward the lung periphery result in a diluted topical concentration of deposited drugs, and as a consequence, may result in a reduced and/or limited therapeutic effect.

Deposition dose per unit surface area, for mouth breathing with tidal volume of 500 mL and flow rate of 250 mL/sec, in local volumetric regions: 50–100 mL (
Aerosol Deposition in Diseased Lungs
Lung diseases are often accompanied by airway narrowing, change in lung compliance, and/or mucus plugging. These factors can significantly influence the distribution of inhaled drugs, and as a consequence, their deposition pattern. Deposition is usually higher in patients with obstructive lung disease than in healthy subjects.(21) Compared to healthy subjects, bronchial deposition is increased at the expense of pulmonary deposition both in patients with asthma and in patients with chronic bronchitis.(22–24) most likely because of decreased airway cross-section in the diseased lung. Several studies have indeed shown an increase in the central to peripheral ratio of lung deposition following bronchoconstriction.(25,26) In the case of emphysema, deposition is also increased in the central region of the lung presumably because of increased deposition during expiration in airways with flow limitation.(27) It should also be noted that deposition patterns are more heterogeneous in the diseased lung than in the healthy lung. Airway obstruction may indeed cause subtended lung regions to be poorly ventilated, with limited inhaled aerosol being able to penetrate and therefore deposit in these regions.
Using the aerosol bolus technique, Anderson et al.(18) have shown that deposition in cystic fibrosis (CF) patients was systematically greater at all penetration volumes when compared to deposition in healthy controls. Figure 2B illustrates typical deposition data obtained in one of the CF patients and one of the normal subjects from that study. Interestingly, as for normal subjects, deposition in CF patients linearly increased with increasing penetration volume. The large increase in deposition observed at low penetration volume between the CF patient and healthy control, and the almost parallel increase in deposition with increasing penetration volume between the two subjects suggest that most of the increased deposition occurred centrally. The mechanisms that are responsible for the increased deposition in the CF patients are most likely those resulting from higher velocities in the narrowed and obstructed airways such as turbulent mixing and increased inertial impaction. Nonuniform ventilation is another potential contributor to the increased deposition measured in CF patients, and would result in an increase in the slope of deposition as a function of penetration volume (DE-Vp slope) in CF compared to healthy subjects. As discussed by Anderson et al.,(18) in the extreme case of ventilation being confined to one lung, deposition of bolus delivered at a given penetration volume should be comparable to that of a bolus delivered at twice that penetration volume in normal lungs, which would result in the doubling of the DE-Vp slope. Using Anderson et al.(18) data, the calculated DE-Vp slope increased by 35% from 0.0492±0.011%/mL (SD) to 0.0664±0.0078%/mL between the healthy and CF group. When correcting for the deeper penetration of the inhaled bolus, deposition in the CF group was reduced from 19.9±8.7 to 16.4±8.8% in the proximal region (Vp=200 mL) and from 59.8±9.1 to 46.0±8.7% in the lung periphery (Vp=800 mL) and was still significantly higher than in the healthy group where deposition in the proximal and peripheral lung region was 6.2±2.5 and 35.8±8.0%, respectively. Although nonuniform ventilation explained ∼25% of the increase in deposition measured at a penetration volume of 200 mL, it accounted for ∼50% of the increase in the lung periphery (Vp 800 mL).
Not all lung diseases affect deposition in a similar manner. Changes in aerosol bolus deposition induced by disease or following a specific intervention have been summarized previously by Blanchard.(28) Compared to healthy controls, increased deposition was observed in asthmatics with abnormal pulmonary function tests (PFTs),(29) in healthy subjects after bronchoprovocation,(30,31) and in CF patients as discussed in the previous paragraph.(18) Patients with restrictive lung diseases(32) and smokers(16,33) or asthmatics(34) with normal PFTs showed no significant changes in deposition, whereas bronchodilating the airways resulted in a decrease in bolus deposition compared to controls.
Effect of Flow Regime on Aerosol Deposition
An important consideration in aerosol deposition in the lung is whether aerosol transport occurs in a laminar or turbulent flow. In laminar flows, transport of fluid elements is dominated by viscous forces and tends to occur in an orderly fashion. Turbulent flows, on the other hand, are inertia-dominated and are characterized by random motions of the fluid elements. Flow regime is characterized by the Reynolds number, a dimensionless parameter describing the relative importance of inertial to viscous forces, defined as
where ρ and μ are the gas density and gas dynamic viscosity, respectively, u is the mean flow velocity in the airway, and d is the airway diameter. In a cylindrical airway, flow is laminar for Re<2100 and turbulent for Re>2100.(35) During quiet and moderate breathing (flow < 500 mL/sec), Reynolds number throughout the intrathoracic airways is below 2100, suggesting laminar flow within the lung. However, before reaching the trachea, the airstream is transported through the upper airway that is characterized by drastic changes in cross-sectional areas with a major constriction located at the level of the glottis. Such constriction generates the so-called laryngeal jet, which produces local turbulences that are propagated further down the bronchial tree over several generations of airways, even for local Reynolds number below 2100, before being completely dissipated.(36)
Levels of turbulence in the respiratory tract are a function not only of the gas velocity but also of gas properties. By lowering the density of the inspired gas, one may convert some or all of the turbulent flow into laminar flow. Although low-density gas such as helium has been mainly used in the clinical setting to reduce the work of breathing, and has seen its greatest application through the use of helium–oxygen mixtures to treat acute obstruction of the upper airway,(37) these gas mixtures have also been assessed for aerosol delivery. A typical mixture of 80% helium and 20% oxygen (heliox) has a gas density about one-third that of air and a viscosity that is about 8% higher than that of air. Therefore, for given flow conditions, the Reynolds number for heliox is approximately one-third that of air in any given airway. Accordingly, turbulent flow is reduced or even absent when breathing heliox. A reduction in turbulent mixing would then theoretically reduce deposition in the upper airway and first generations of conducting airways and allow for targeting aerosol in the more peripheral lung.
Using scintigraphic techniques, Svartengren et al.(38) and Anderson et al.(39) measured the deposition of 3.6 μm-diameter particles following deep inhalations of particles suspended in air or heliox. Svartengren et al.(38) measured less deposition in the throat and mouth when breathing heliox than when breathing air although the difference was not significant (17 vs. 27%, p>0.05), and found no difference in alveolar deposition between the two gas mixtures. Anderson et al.,(39) on the other hand, found a significantly lower deposition in the mouth and throat and a higher alveolar deposition when breathing heliox compared to air. The difference in alveolar deposition between the two studies was more likely due to additional particle deposition occurring during the breath hold following each inspiration in Anderson's study. In another study using the aerosol bolus technique with particles of 1 and 2 μm in diameter, Peterson et al.(40) showed a significant reduction in deposition in the upper respiratory tract of healthy subjects while breathing heliox, and a significant increase in deposition in the peripheral lung (Fig. 4).
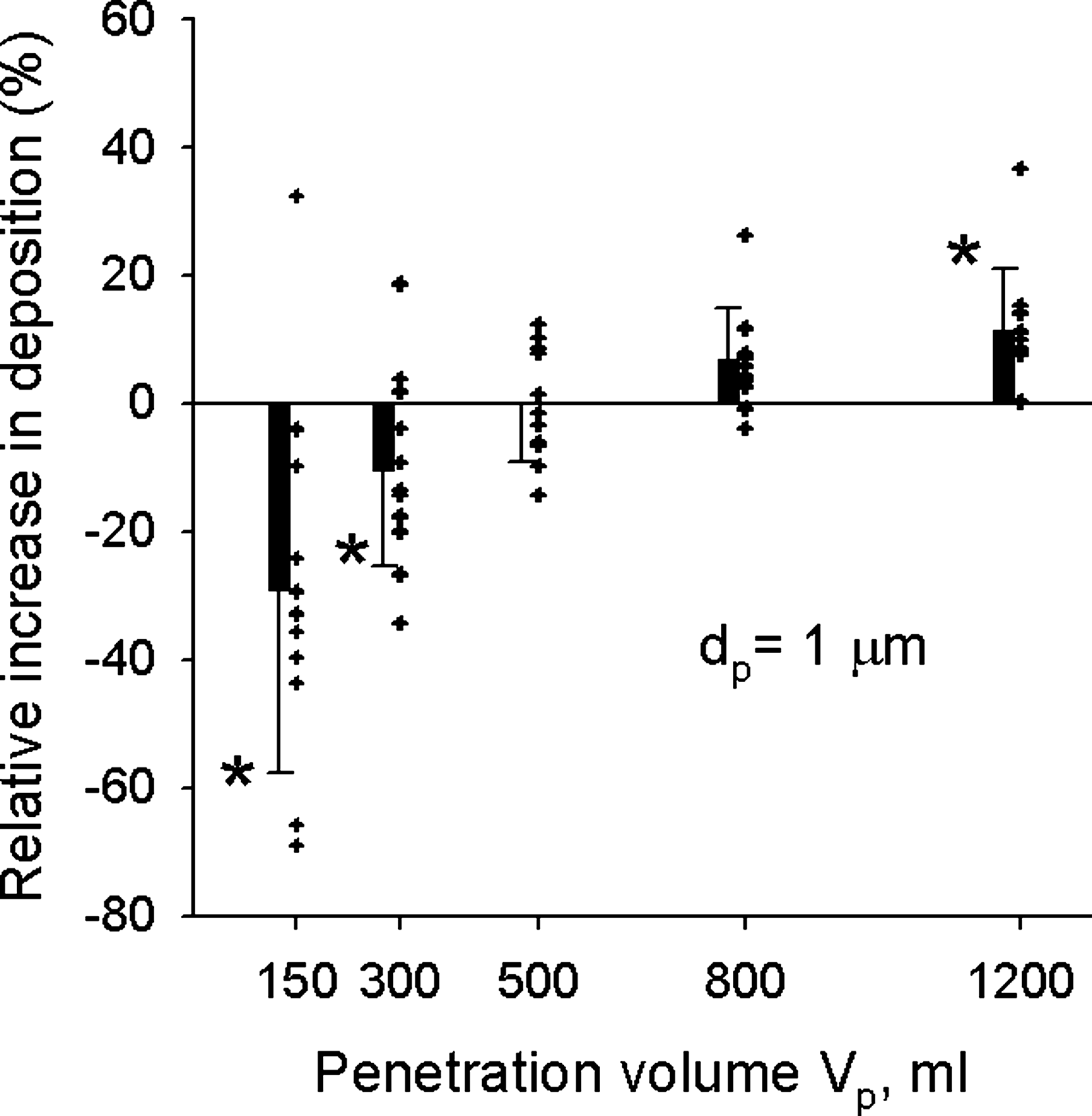
Relative increase in deposition of 1 μm-diameter particles when breathing heliox instead of air. Relate change in deposition ΔDE was defined as (DEheliox – DEair)/DEair, where DEheliox and DEair are deposition in heliox and air, respectively. Data are plotted as a function of penetration volume with the symbols representing individual data from 11 healthy subjects and the bars the averaged data (mean±SD). A negative relative increase corresponds to a decrease in deposition in heliox compared to air. *Significantly different compared to air data (from(40)).
In all these studies,(38–40) because of the reduced density of heliox, reduction in deposition in the upper respiratory tract was attributed to a reduction in deposition by turbulent mixing in the trachea and a reduction in deposition due to secondary transitional flows in the conducting airways. The importance of both turbulent mixing and inertial impaction on particle deposition in the upper airway is highlighted in a computational modeling study by Matida et al.(41) In that study, where both factors could be assessed separately, aerosol deposition of 2.5, 3.7, and 5 μm-diameter particles was predicted in an idealized mouth model for an inhalation flow rate similar to that used in Peterson et al.'s study.(40) When both the averaged values of mean velocities and the fluctuating component of turbulent flow were modeled [large-eddy simulation (LES) case] (Fig. 5), predicted deposition agreed remarkably well for all particle sizes with experimental data obtained in a similar physical model. When only averaged values of mean velocities were calculated (mean flow tracking case) (Fig. 5) and when, as a consequence, only the inertial effects were accounted for in particle transport, deposition predictions were ∼40% of that measured in the physical model. These differences in predicted deposition strongly suggest turbulent mixing as an important mechanism of deposition in the upper airway.
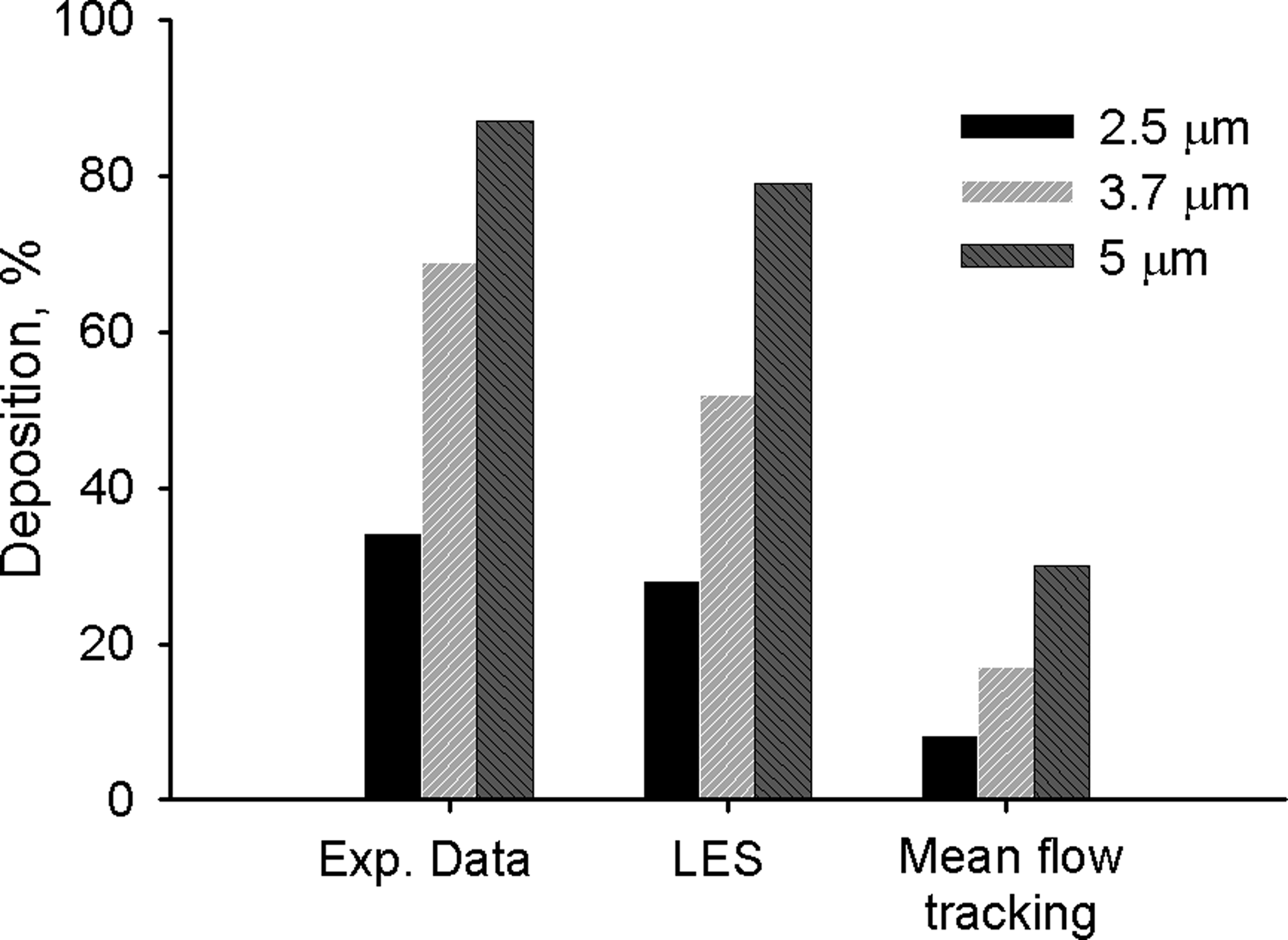
Experimental and numerical results of particle deposition in an idealized mouth model for 2.5, 3.7, and 5.0 μm-diameter particles. Numerical predictions were obtained (1) by modeling both mean flow and turbulent fluctuations using a large-eddy simulation (LES) approach, and (2) by considering only the mean-flow tracking of a Reynolds Averaged Navier-Stokes approach. Both inertial effects and turbulent mixing were accounted for in the LES approach, whereas only the effects of inertial impaction were modeled in the mean flow tracking approach (from(41)).
Reducing deposition in the upper airway allows more particles to penetrate and deposit in the more distal region of the lung, increasing the efficiency of aerosolized drugs. For example, Kress(42) noticed a more significant improvement in spirometry in patients with acute asthma exacerbations after treating them with albuterol nebulized in heliox compared to albuterol nebulized with oxygen, most likely because the low-density gas enhanced albuterol deposition in the distal airways. Anderson et al.(43) also measured enhanced deposition in the lung periphery of stable asthmatics when particles were inhaled with heliox rather than air. They showed a strong negative correlation between alveolar deposition and airway resistance, supporting the concept that reducing flow resistance by breathing low-density gas mixtures allows for more aerosol to be delivered to the lung beyond the large airways.
Aerosol Deposition And Therapeutic Effect
Although there is no doubt that both lung disease and particle size affect the deposition of inhaled drugs, one needs to keep in mind that for an inhaled drug to be effective, it needs to not only deposit in a sufficient amount but also needs to reach the targeted regions of the lung where drug receptors are located. Zanen et al.(44) have shown that delivering monodisperse β-adrenergic aerosols of 2.8 μm in size to mild asthmatics induced greater airway dilation than equivalent doses of monodisperse aerosols of 1.5 or 5 μm in size, as measured by improved forced expired volume in 1 sec (FEV1) and by improved maximum expiratory flow. Similar results were found in patients with severe airflow obstruction(45) to which monodisperse salbutamol and ipratropium bromide were delivered. The difference in bronchodilator response between aerosol sizes was almost certainly due to different spatial distributions of deposited particles. Although deposition was not measured in these two studies, it is likely that the optimal size of 2.8 μm was the combined result of greater aerosol penetration beyond the large airways (the smaller the particle size, the better the penetration) and of optimal site of aerosol deposition (the larger the particle size, the higher the deposition in the targeted medium and small airways and the less in the alveolar region).
In a more recent study, Usmani et al.(46) measured regional lung deposition of radiolabeled monodisperse albuterol in asthmatics subjects. Equivalent doses of 1.5, 3, and 6 μm aerosols were delivered to the patients and their bronchodilator response assessed. Although distal airway penetration and peripheral lung deposition increased with decreasing particle size, the best improvement in FEV1 was observed with the largest particle size (and smallest lung deposition), highlighting the importance of regional targeting. In a modeling study, Darquenne et al.(47) determined the mechanisms responsible for the spatial distribution of inhaled aerosols within the lung. Using a realistic three-dimensional model extending from the trachea to the segmental bronchi, they showed that the delivery of inhaled particles to the lung segments was dominated by convective flow for specific breathing conditions and particle sizes. These conditions were characterized by a single parameter, the Stokes' number Stk (Equation 1). Their predictions suggest that when the Stokes number in the trachea was less than 0.01, aerosol and gas flows were proportionally distributed to the lung segments. Assuming a tracheal diameter of 1.8 cm, Stk number was calculated for the aerosol inhalations conditions in Usmani et al.(46) and Zanen et al.(44,45) studies. Stk values suggest that for all cases, but that of 6-μm aerosols inhaled at high flow rate (60 L/min) for which Stk is 0.023, the inhaled particles that reached the trachea were delivered to the lung segments accordingly to segmental flow distribution.
The newest guidelines for aerosol therapies(48) recommend slow inhalations (<30 L/min) of the aerosol being delivered. At a flow rate of 30 L/min, the Stk number in the trachea of adult subjects will be less than 0.01 for particles up to a diameter of 5.5 μm. Most of the metered dose inhalers, dry powder inhalers, and nebulizers available today produce a mass median aerosol diameter of 6 μm or less, suggesting that all these devices allow for delivering aerosolized drugs to the lung segments according to flow distribution.
In summary, although the lung is an attractive target for drug delivery, several factors need to be considered to ensure an efficient and effective therapy. The main factors are that of particle size and breathing pattern both affecting the extent and site of drug deposition. Total lung deposition appears to be a poor predictor of clinical outcome; rather, regional deposition needs to be assessed to predict therapeutic effectiveness. Spatial distribution of deposited particles is strongly affected by particle size. Large particles (>6 μm) tend to mainly deposit in the upper airway limiting the amount of drugs that can be delivered to the lung. Small particles (<2 μm) deposit mainly in the alveolar region and are probably the most apt to act systemically, while the particle in the size range 2–6 μm are best suited to treat the central and small airways.
Footnotes
Acknowledgments
This work was partially supported by grant ES011177 from the National Institute of Environmental health Sciences (NIEHS) at NIH and by the National Space Biomedical Research Institute (NSBRI) through NASA NCC 9-58 as NSBRI Grant #TD00701.
Author Disclosure Statement
The author declares that no conflicting financial interests exist.