
Abstract
Abstract
Background:
Concentration of nitric oxide in exhaled air (FeNO) was revealed to decrease as a result of immunotherapy. However, individuals who are exposed to environmental allergens are characterized by elevated values of FeNO. The aim of this study was to analyze the effects of subcutaneous immunotherapy (SCIT) on the dynamics of FeNO determined during consecutive pollination seasons.
Methods:
This study, performed between 2005 and 2008, included 41 patients with confirmed sensitivity to grass pollens and predominating symptoms of seasonal allergic rhinitis, randomly assigned to desensitization by preseasonal or maintenance SCIT. FeNO was measured prior to and during each pollen season (November–January and May–July, respectively). The results were conferred to data on grass pollination intensity in 2006–2008 (air concentration of grass pollen grains, seasonal number of days when air concentration of grass pollen reached at least 50 grains per 1 m3).
Results:
Median content of FeNO in exhaled air was significantly higher in 2007 compared to 2006 and 2008 pollen seasons. During 2007 and 2008 pollen seasons, significant increase in FeNO was observed compared to the respective preseasonal values. Median number of days with air concentration of grass pollen ≥50 grains per 1 m3 of air during 4 weeks preceding seasonal FeNO measurement was significantly higher in 2007, corresponding to higher FeNO value recorded during this pollen season. However, no significant correlation was observed between seasonal number of days with ≥50 grass pollen grains per 1 m3 of air and FeNO in exhaled air (r=0.09, p=0.362).
Conclusions:
Most seasonal allergic rhinitis patients show physiological levels of FeNO prior to the pollen seasons and a marked increase in this parameter, probably proportional to pollination intensity, is observed within the seasons.
ISRCTN Registry: ISRCTN86562422
Introduction
Pollination intensity during consecutive years usually differs in terms of pollen concentration per 1 m3 of air and the number of days with grass pollen concentrations that are sufficient to induce clinical symptoms in all sensitive individuals.(8) FeNO was revealed to decrease as a result of effective anti-inflammatory treatment of asthma patients(9) and similar outcomes can be obtained with immunotherapy.(10) The primary goal of our research was to compare the effectiveness of two protocols of subcutaneous immunotherapy (SCIT), preseasonal and maintenance, and their influence on specific and nonspecific bronchial responsiveness in seasonal allergic rhinitis patients (in press). However, empiric observations made during this study encouraged us to analyze the effects of SCIT on the dynamics of FeNO determined during consecutive pollination seasons.
Materials and Methods
Participants
This research was conducted between 2005 and 2008. All procedures were approved by the Ethics Committee of the Medical University of Bialystok and the subjects and/or the parents of the underage participants gave their informed consent before the start of any procedure.
Forty-one patients with sensitivity to grass pollen (as confirmed by the skin prick tests) and predominating symptoms of severe acute respiratory syndrome (SAR) were included in this study. The power of this sample was 81.6%; required sample size providing 90% target power was 32 patients per one protocol of SCIT. Characteristics of study participants are summarized in Table 1. The patients were randomly assigned to desensitization by preseasonal (n=20) or maintenance SCIT (n=21).
Of predicted value.
Interquartile range.
Immunotherapy
Immunotherapy was based on Allergovit® 006-grass 100% preparation (Allergopharma, Germany). In both groups, immunotherapy began with a build-up phase, that is, gradually reaching the maintenance dose (increasing volumes of 0.1, 0.2, 0.4, and 0.8 mL were administered subcutaneously in 7- to 14-day intervals from vial A containing 1,000 therapeutic units (TU)/mL of allergoid, followed by 0.15, 0.30, and 0.6 mL from vial B containing 10,000 TU/mL of allergoid). After reaching the maintenance dose, usually equal to 6,000 TU of allergoid, this dose was administered every 2 to 4 weeks or every 4 to 6 weeks in the preseasonal and maintenance protocols, respectively.
Every year before the pollen season, patients who were desensitized using the preseasonal protocol were given one package (one vial of A and B), usually divided into 10 injections, corresponding to 30,000 TU yearly dose of allergoid. Patients assigned to the maintenance protocol, after reaching the highest well-tolerated dose not exceeding 0.6 mL, were given booster injections for a period of three years (Fig. 1).
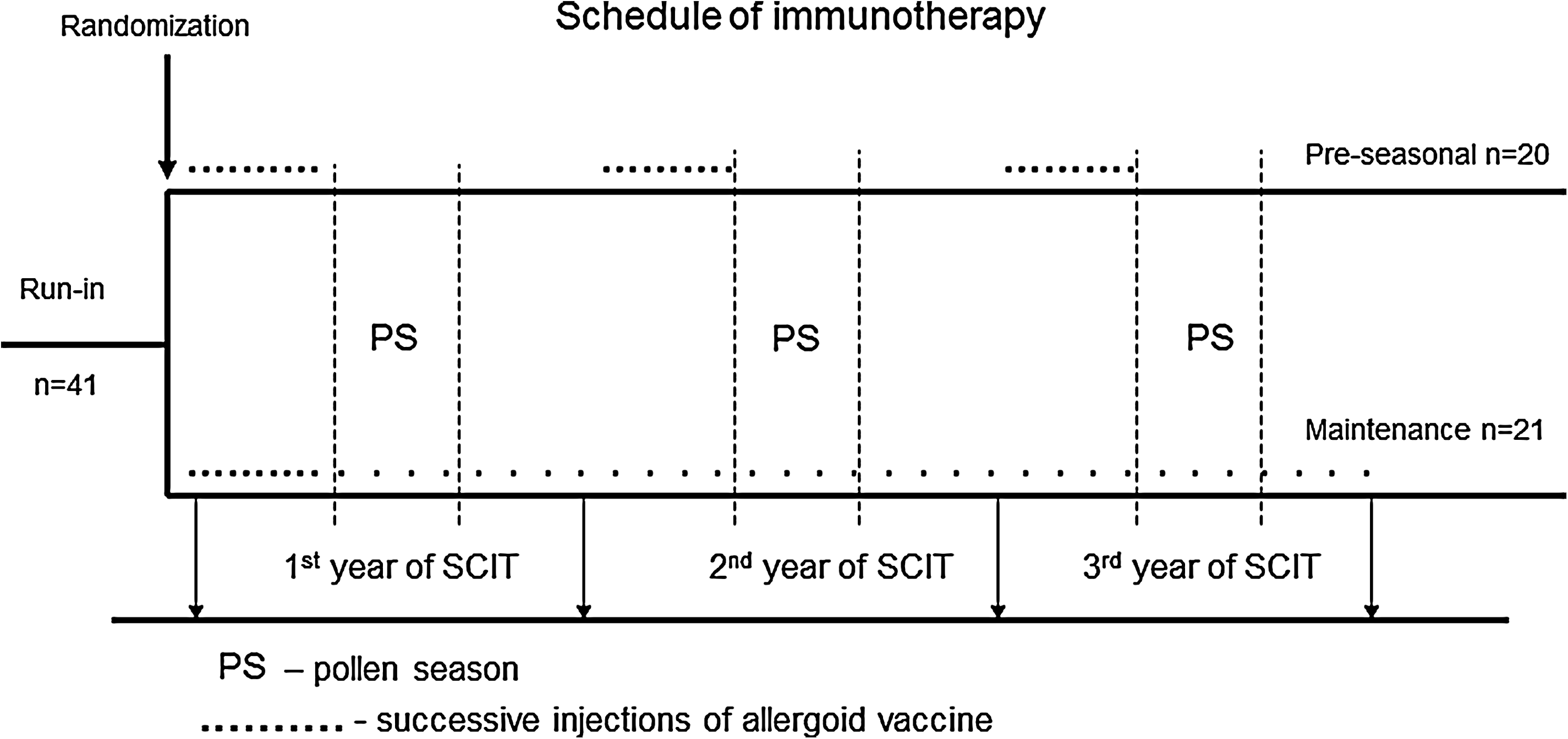
Schematic presentation of the schedules of two protocols of SCIT used in this study.
The average total number of injections received by patients who were desensitized using the maintenance protocol was 41±3 throughout the entire course of immunotherapy, with the total dose of allergen equaling 179,059±11,120 TU on average. Correspondingly, patients receiving preseasonal immunotherapy averaged 30±1 injections and 86,863±2,972 TU of allergen.
FeNO
FeNO was measured prior to and during each pollen season (November–January and May–July, respectively). The examination was performed in accordance with ATS/ERS consensus guidelines(11) using a NioxMino® analyzer (Aerocrine, Sweden) at a mouth flow rate of 50 mL/s and at a pressure of 10 cm H2O. At least two measurements were performed to achieve two technically adequate results not differing from each other by more than 10% with a sustained plateau of at least 8 s. The lower result of these two measurements was considered appropriate. The measurement range of the device varied from 5 to 300 pbb and accuracy amounted to±5 ppb for values<50 ppb.
Pollination intensity
Routine-independent pollination monitoring has been performed in Bialystok for several years. Data on grass pollination intensity in 2006–2008 was kindly provided by the Allergen Research Center in Warsaw. Only the data pertaining to periods between May 1st and August 31st was analyzed.
Statistical analysis
The normal distribution of continuous variables was tested using the Shapiro-Wilk test. The significance of time course differences among continuous variables was tested by the Friedman analysis of variance (ANOVA) test and the intraseasonal significance of differences between two protocols of SCIT was verified with the Mann-Whitney test. Additionally, Spearman's rank coefficient of correlation was calculated between the seasonal number of days with ≥50 grass pollen grains per 1 m3 of air or baseline IgE levels and FeNO in exhaled air. All calculations were performed using Statistica 8 (StatSoft®, Poland) software, statistical significance was defined as p≤0.05.
Results
FeNO concentrations in exhaled air
Median content of FeNO in exhaled air was significantly higher in 2007 compared to 2006 and 2008 pollen seasons (Fig. 2). There were no significant year-to-year differences in FeNO determined before 2006–2008 pollen seasons (p=0.268). During 2007 and 2008 pollen seasons, a significant increase in FeNO was observed compared to the respective preseasonal values (Fig. 2).
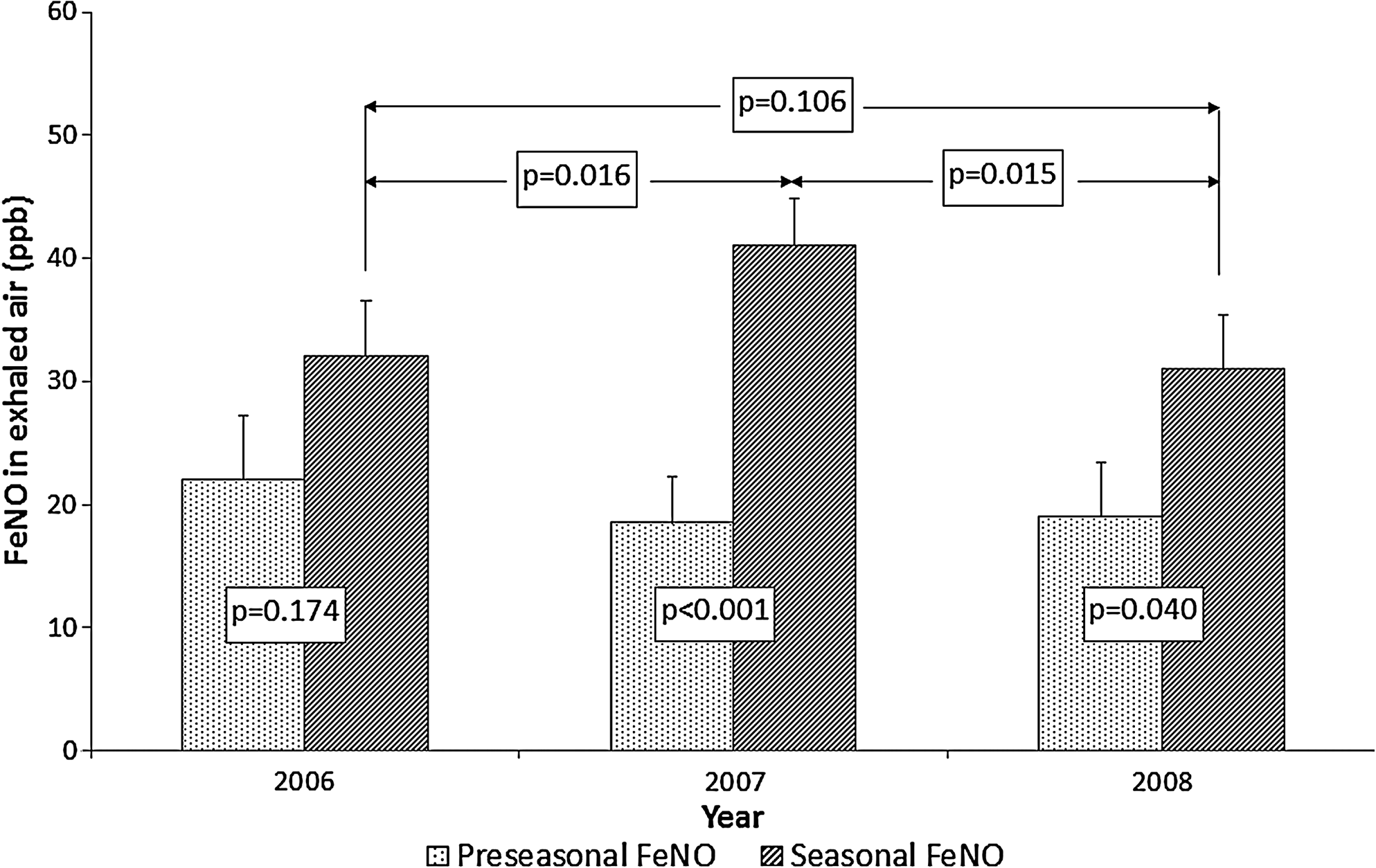
Changes in median FeNO content (ppb, with error bars) in exhaled air of seasonal allergic rhinitis patients subjected to 3 years of SCIT.
Analysis of subgroups subjected to the different protocols of SCIT revealed similar findings. The only exception pertained to group desensitized by maintenance SCIT where significant differences between median preseasonal and seasonal FeNO were observed only in 2007 (Table 2).
Our group included only two individuals with normal baseline IgE levels. This parameter did not correlate significantly with preseasonal (first year: r=0.139, p=0.425; second year: r=0.223, p=0.204; third year: r=0.134, p=0.450) and intraseasonal FeNO levels (first year: r=0.207, p=0.247; second year: r=0.166, p=0.357; third year: r=0.128, p=0.469) determined during consecutive years of this study.
Intensity of grass pollination
Consecutive seasons covered by this study differed in terms of maximal air concentrations of grass pollen (Fig. 3. Additionally, significant differences were noted in the number of days with at least 50 grains of the pollen per 1 m3 of air (Table 3), that is, the days when, according to literature,(8) all the individuals sensitive to grass pollen report clinical symptoms. This data was not useful for the purpose of our study; however, because the seasonal measurements of FeNO were taken during a relatively wide period of time, between the end of May and the end of July; thus, not obligatorily at the end of the pollen season. Consequently, individuals participating in this study could potentially differ in terms of grass pollen exposure prior to the FeNO determination. To avoid this confounder, we determined the number of days with air concentration of grass pollen ≥50 grains per 1 m3 of air during 4 weeks preceding seasonal FeNO measurement in each individual. Median value of this parameter was significantly higher in 2007, corresponding to higher FeNO value recorded during this pollen season (Fig. 4). However, no significant correlation was observed between seasonal number of days with ≥50 grass pollen grains per 1 m3 of air and FeNO in exhaled air (r=0.09, p=0.362).
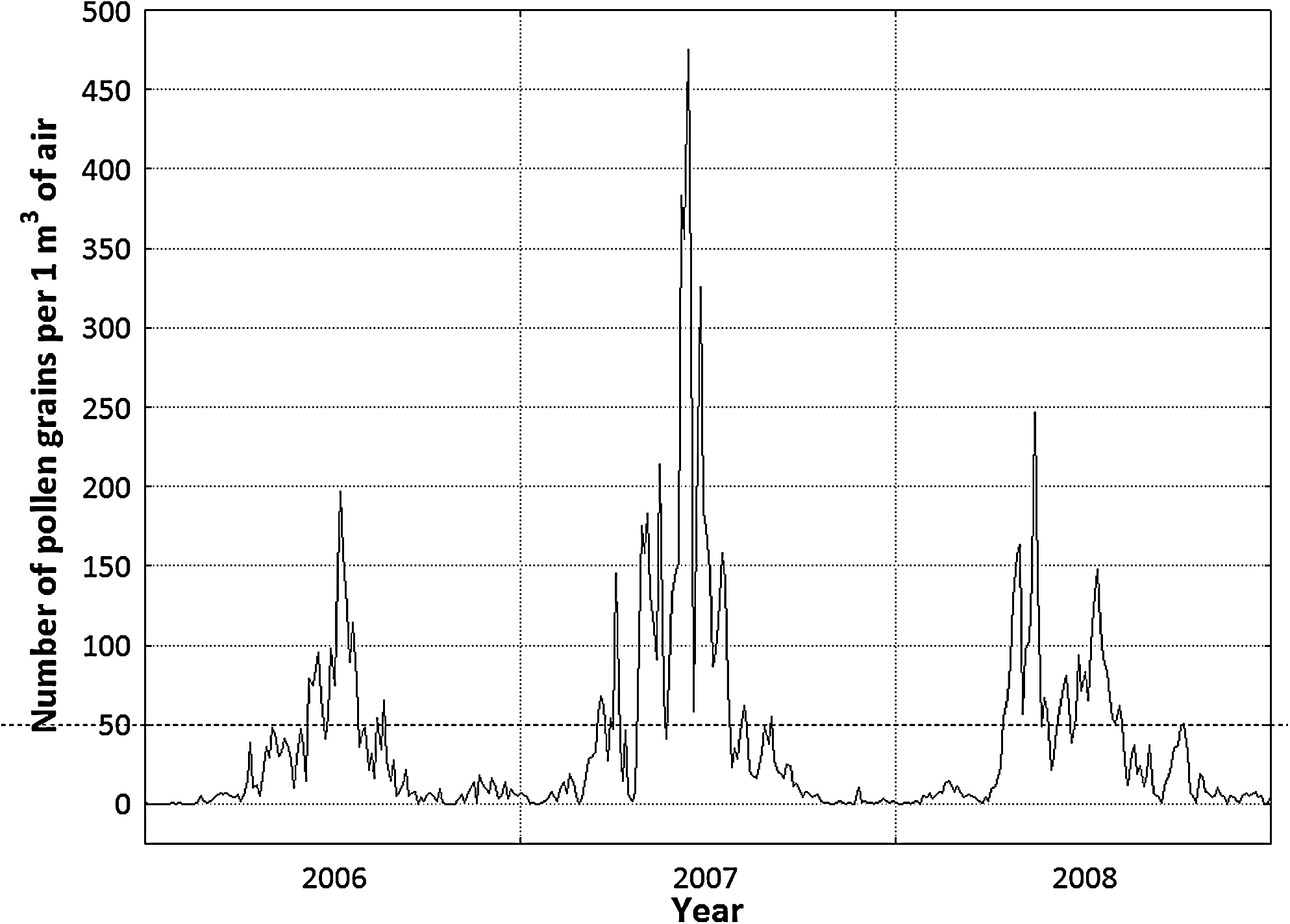
Daily concentrations of grass pollen recorded in Bialystok between 2006 and 2008.
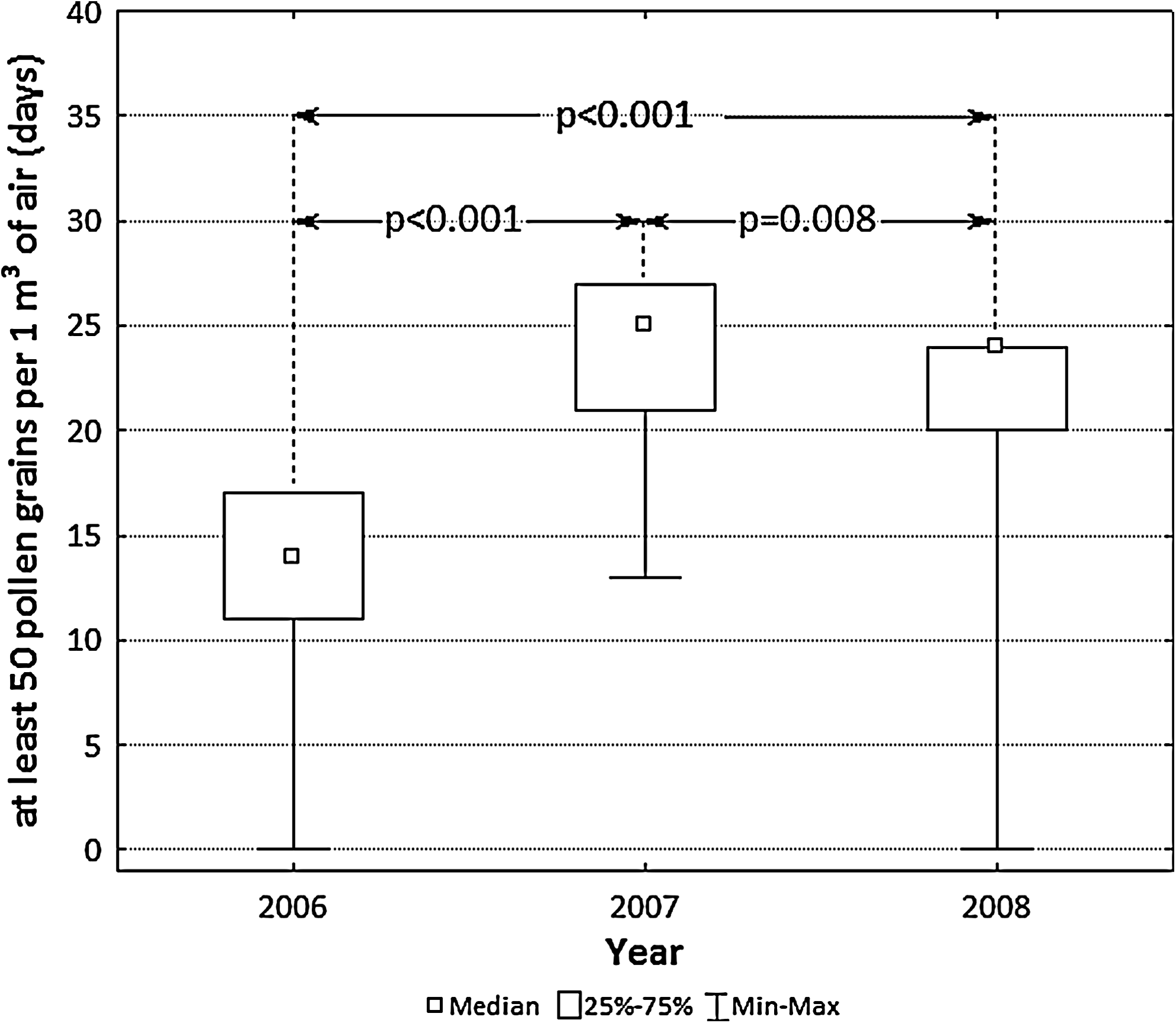
Median number of days with air concentration of grass pollen ≥50 grains per 1 m3 of air during 4 weeks preceding seasonal FeNO measurement in patients subjected to 3 years of SCIT.
With interquartile range.
Significantly lower compared to 2007 and 2008 (p<0.05).
Significantly higher than in 2006 (p<0.05).
Discussion
Median FeNO concentration in exhaled air determined prior to the three pollen seasons covered by this study oscillated around 20 ppb, and therefore was in the range of normal values. However, marked increase in FeNO was observed during each pollens season and it appeared to be dependent upon the degree of exposure to grass pollen.
The results of recently published research suggest that individuals sensitive to dust mites, with longer exposure to the allergen due to sedentary indoor lifestyle, have a markedly higher FeNO levels compared to their more active peers.(12) Another study revealed that subjects sensitive to birch pollen have higher concentrations of nitric oxide in exhaled air during this tree's pollination period.(13)
Surprisingly, our study revealed weak and insignificant correlation between FeNO level and the seasonal number of days with air concentration of grass pollen reaching at least 50 grains per 1 m2. Additionally, our previous experiences suggest that even a single exposure to high allergen dose is reflected in a substantial and long-lasting increase in FeNO in individuals sensitive to grass pollen, including those that are asymptomatic.(3) Plausibly, extremely high pollen concentrations are not needed to raise FeNO in cases of long-term allergen exposure. This possibility was also suggested by the results of our previous study, which revealed that an increase in FeNO during bronchial allergen challenge occurred also in those sensitive subjects who did not show response after grass pollen allergen inhalation.(3) Furthermore, Ihre et al.(14) observed that a 7-day exposure to low allergen doses can stimulate FeNO and bronchial responsiveness to histamine in sensitive individuals despite the lack of other changes in spirometric parameters. Therefore, one can conclude that FeNO may also increase as a result of continuous exposure to low allergen doses. Although our study did not reveal a significant association between the number of days with high air content of grass pollen and the concentration of nitric oxide in exhaled air, the median FeNO was higher during seasons characterized by more intense pollination. According to recently published research, triplicate administration of high allergen doses at 48-h intervals does not modulate early or late reaction in subjects with mild asthma.(15) However, allergen-induced changes in FeNO were not reported in this study.
After 3 years of immunotherapy, we did not observe a seasonal increase in FeNO in subjects who were desensitized with maintenance SCIT. Still, authors who did not confirm protective effects of SCIT in terms of FeNO levels have observed a tendency to lower nitric oxide concentrations in desensitized individuals.(16) Prieto et al.(17) analyzed the effects of 12-month-specific immunotherapy in patients sensitive to Alternaria alternata, and did not observe significant treatment-related changes in FeNO. Our study; however, revealed positive effects of maintenance SCIT not earlier than after 3 years, and therefore, one can conclude that the follow-up period in Prieto's et al.(17) study was too short. In contrast, in another study that included children suffering from asthma due to perennial allergy caused by Dermatophagoides pteronyssinus and Dermatophagoides farinae,(10) desensitization was reflected by a lower FeNO as early as after 4 months; changes in this parameter correlated with clinical response to the treatment. Therefore, one can conclude that positive effects of allergen immunotherapy on FeNO are more apparent in subjects sensitive to perennial allergens. In such cases, the intensity of natural allergenic stimulation is relatively stable throughout the year, resulting in less pronounced seasonal oscillations in FeNO than in the cases of grass pollen sensitivity. Furthermore, one should remember that maintenance immunotherapy, which more efficiently reduced FeNO in our subjects, is considered the desensitization of choice in patients sensitive to dust mites.
In summary, this study revealed that most seasonal allergic rhinitis patients show physiological levels of FeNO prior to the pollen seasons and that a marked increase in this parameter, probably proportional to pollination intensity, is observed within the seasons. Furthermore, maintenance allergen immunotherapy rather than preseasonal SCIT seems more effective in prevention of seasonal FeNO increase.
Footnotes
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.