
Abstract
Abstract
Background:
Inhaled interferon-γ aerosol (aINF-γ) may be effective treatment for idiopathic pulmonary fibrosis (IPF). We evaluated safety and delivery of aIFN-γ (100 μg 3 times/week) in 10 IPF patients using the I-neb (Philips Respironics, Parsippany, NJ).
Methods:
IFN-γ activity in the aerosol was confirmed by viral inhibition. Ten patients with an average age of 68 diagnosed with IPF (American Thoracic Society/European Respiratory Society consensus guidelines) were enrolled. In vivo deposition was measured via a gamma camera. The nebulizer recorded patient adherence to therapy. Pulmonary function tests [PFTs, forced vital capacity (FVC), total lung capacity (TLC), diffusing capacity for carbon monoxide (DLCO)] and the 6-min walk test were measured at baseline, and every 12–14 weeks for 80 weeks. Bronchoalveolar lavage (BAL) of the middle lobe was performed at baseline and 28 weeks. BAL and plasma samples were analyzed for chemokines and cytokines, including INF-γ.
Results:
All 10 patients tolerated 80 weeks of inhaled IFN-γ well, with no systemic side effects. True adherence with aerosol treatment averaged 96.7±4.81% (±SEM). In vivo lung deposition averaged 65.4±4.8μg and oropharyngeal deposition 12.6±3.0 μg. BAL IFN-γ increased 60-fold and profibrotic cytokines (FGP-2, Flt-3 ligand, IL-5) were significantly decreased; IFN-γ plasma levels were unchanged. PFTs showed minimal change in FVC. Post hoc analysis indicated that the slope of decline in TLC and DLCO reversed after beginning therapy. The 6-min walk was unchanged.
Conclusions:
IFN-γ is safe in IPF and can be effectively delivered to lung parenchyma. PFTs remained stable throughout the trial. Reversal of pretherapy PFT decline may define an end-point for future clinical trials.
Introduction
Interferon-gamma (IFN-γ) is the signature Th1 cytokine that is endogenously produced by T cells and natural killer cells and exhibits antifibrotic, antiproliferative, and immunomodulatory properties. Its potential therapeutic role in fibrosis, although supported by in vitro and animal models, was not proven to be effective in two randomized, placebo-controlled clinical trials where it failed to show any benefit.(6,13) Although subcutaneous IFN-γ did lead to some antiangiogenic and immunomodulatory changes in the immune environment of the lung, levels of interferon gamma recovered from the lung were low.(14) Despite the high profile failure of IFN-γ as therapy in IPF, its use remains attractive in view of data supporting the role of a Th2, alternatively activated macrophage lung milieu that may drive fibrosis. As such, we studied the use of aerosol IFN-γ in IPF. With an aerosol, the concentration of drug delivered to the lung may be considerably higher than that achievable by systemic administration. In support of this concept, data from normal volunteers has shown that subcutaneous delivery of IFN-γ does not increase levels of IFN-γ in epithelial lung lining fluid or activate alveolar macrophages, whereas aerosol delivery achieves both.(15) Furthermore, in patients with active pulmonary tuberculosis, inhaled IFN-γ has been shown to induce intracellular signaling of INF-γ-specific transcription factors and to improve clinical response to antituberculosis therapy.(16–18)
Currently there are no data on effective aerosol deposition in IPF patients. In IPF, delivery of a therapeutic aerosol to the peripheral lung may be suboptimal because of airspace enlargement and increased minute ventilation.(19,20) Combined with the inherent inefficiency of conventional nebulizers, delivery and deposition may be inadequate.(16) Controlling ventilatory parameters and using an efficient breath actuated nebulizer may overcome impediments to lung delivery.(21)
The present study was undertaken with several goals: first, to establish that IFN-γ can be aerosolized without affecting activity of the protein; second, to assess the efficiency of a novel breath actuated nebulizer using feedback control to regulate breathing; and finally, to determine the safety of long-term IFN-γ aerosol therapy in patients with IPF as defined according to American Thoracic Society/European Respiratory Society consensus guidelines.
Materials and Methods
In vitro studies
The nebulizer
The I-neb Adaptive Aerosol Delivery (AAD) System (Philips Respironics, Parsippany, NJ) a vibrating membrane aerosol generator is breath actuated, minimizing aerosol losses during expiration.(21,22) In addition, the I-neb AAD system, utilizes “adaptive aerosol delivery,” by measuring the patient's breathing pattern and via feedback, training the patient to perform slow, deep inspirations, thereby facilitating parenchymal aerosol deposition. The I-neb records the treatment date, treatment time, and if the treatment was completed.(21,23) Daily cleaning and monthly replacement maintained membrane performance.
Formulations
Drug activity studies were performed with single vials of IFN-γ (Actimmune, InterMune, Brisbane, CA; 2 million U or 100 μg/0.5 mL). Radioactivity labeling studies and nebulizer function studies were performed with 0.5 mL of albuterol sulfate (2.5 mg/3 mL, Nephron Pharmaceuticals Corp., Orlando, FL) or 0.6 mL 0.9 NaCl (normal saline, NS). Radiolabels consisted of 99m-technetium pertechnetate (99mTc) and 99mTc sulfur colloid (Pharmalucence, Inc., Bedford, MA; 99mTc SC).
Effect of vibrating mesh nebulization on IFN-γ activity
Vials of IFN-γ were nebulized with a continuous mode I-neb vibrating mesh nebulizer (Philips Respironics). The aerosol was propelled by the energy of the vibrating membrane and simply allowed to pass into a glass jar cooled to zero degrees F. In the jar particles circulated and settled out depositing on the walls. The collected aerosols were QS to 5.0 mL with PBS buffer and serially diluted to a final dilution of 1:160,000 of the initial 5.0 mL sample. IFN-γ activity was measured by viral inhibition bioassay (PBL Biomedical Laboratories, Piscataway, NJ).
Aerosol distribution using saline
The I-neb AAD system was connected to a breathing simulator (Harvard pump, Harvard Respiratory Apparatus, model# 618;Millis, MA). To simulate a patient breathing slowly and deeply, the pump was set to a tidal volume of 1.5 L, respiratory rate 5 per min, and duty cycle 0.7. A filter (Pari, Starnberg, Germany) was placed between the nebulizer and the pump to prevent aerosol from returning to the nebulizer during expiration. The breathing mode adopted was targeted inhalation mode (TIM) and nebulizer treatments were run to “dryness.” To measure particle distribution, a cascade impactor (Marple 8-stage impactor, Thermo Fischer Scientific, Waltham, MA, 2 liter per minute flow) was placed in-line between the pump and the nebulizer.(22,24) There was a fixed starting dose of 100 μg and treatment times took approximately 4–6 min to complete. Data were reported as mass median aerodynamic diameter (MMAD).
Correction for sulfur colloid radiolabel using albuterol
To prevent free 99mTc from diffusing into the blood during imaging, it must be bound to a large molecule. The only suitable agent available in the United States is sulfur colloid (SC). Using SC as a radiolabel may lead to an underestimation of drug delivery because the colloid can stick to plastic in the nebulizer.(25) The degree of SC adhesion to plastic can be measured by simultaneous assay of nebulized drug and radioactivity in captured aerosol. To define this process for I-neb, we used 0.5 mL of albuterol sulfate mixed with either free 99mTc or 0.1 mL of 99mTc SC. Using the I-neb AAD system and the Harvard respirator serial filters capturing aerosol particles over different time periods of nebulization provided a range of values. After radioactivity captured on the filter was measured, the same filter was analyzed for drug activity. Drug was extracted using sodium hydroxide solution, vortexed, and centrifuged for 10 min at 2000 rpm. Absorption was measured using a Microplate Spectrophotometer (Spectra Max plus, Sunnyvale, CA) at a wavelength of 243 nm, which quantified the amount of drug.(26) Drug concentration and amount of radioactivity present on the filter were calculated as a percent of that initially placed in the nebulizer and the relationship between radioactivity and albuterol compared using linear regression analysis. Linear equations for formulations with free 99mTc and 99mTc-SC were calculated and utilized to correct human scintigraphy studies to define actual drug deposition.
In vivo studies
Inclusion and exclusion criteria are listed in Table 1. Patients chosen for the study were between the ages of 40 and 75 years old and had a diagnosis of IPF made within 1 year of enrollment defined according to American Thoracic Society/European Respiratory Society consensus guidelines.(27) To facilitate repeated bronchoalveolar lavage (BAL) we excluded patients with severe restriction (FVC <55% predicted).
IFN-γ deposition
To assess nebulizer function and measure lung dose of aerosol IFN-γ, two deposition studies (baseline and after 28 weeks of therapy) were performed using techniques previously reported in detail. In brief, with the patient sitting in front of a computer controlled gamma camera (Maxi Camera 400, General Electric, Horsholm, Denmark, Power Computing, Model 604/150/D, Austin, TX, Nuclear MAC, Version 4.2.2, Scientific Imaging, Inc., CA) a 15 min 99mTc room background was obtained. The lung outline, regional volume, and regional ventilation were all measured by xenon (133Xe) equilibrium and washout.(16) After xenon scanning, the patient swallowed a measured amount (∼500 μCi) of 99mTc-macroaggregated albumin absorbed on a small cracker with water. An image of the stomach was acquired, which allowed the calculation of stomach attenuation. Then, after a repeat background image, the patient inhaled a treatment of radiolabeled IFN-γ, using the I-neb AAD system. Immediately following the treatment the patient drank a glass of water to wash oropharyngeal contents into the stomach. A repeat scan encompassing both the lungs and stomach defined lung and upper airway (stomach activity) deposition.
In order to measure the attenuation correction for chest geometry, a calibrated injection of a known quantity of 99mTc-macroaggregated albumin (5–10 mCi) was given through a peripheral intravenous line followed by an image of lung perfusion. Counts from the previous deposition image were subtracted and net counts from the perfusion image were divided by the activity injected to yield a correction factor for the thorax (units=counts per min per μCi). The chest attenuation measurement was performed once at the time of the first deposition study.
Regional deposition calculations
The 133Xe equilibrium images defined lung volume. Using the computer, an outline was drawn around both lungs representing the whole lung zone. Then a second region centered over the central airways was outlined, which represented the central zone; this zone accounted for about 33% of the entire lung. We subtracted the central zone from the entire lung zone and the remaining area was labeled as the peripheral zone. These images were superimposed on the deposition images and allowed a calculation of regional deposition per unit volume. The ratio between the central and peripheral lung zones per unit volume (sC/P) allowed comparison between patients and a quantification of regional airway deposition. A ratio of 1.0 indicates deposition in small airways and alveoli. As the ratio increases more aerosol is deposited in the central airways.(16)
In addition to the standard central and peripheral regions of interest, we created a region approximating the middle lobe. The RML shape and size was drawn using an approximation of a two-dimensional anatomical outline of the corresponding lobe. Activity in this region was used to correlate deposition with levels of IFN-γ measured in bronchoalveolar lavage (BAL) fluid.
BAL
BAL was performed at baseline and after 28 weeks of treatment with inhaled IFN-γ. The second BAL at 1 h after the treatment near the 28th week.(15) Briefly, after local anesthesia with lidocaine, the bronchoscope was inserted via the nasal passage to the lower respiratory tract, wedged into the middle lobe bronchus, and a lavage was performed using five 60-mL aliquots of normal saline. The BAL fluid was processed on the same day as the bronchoscopy in the following manner. BAL fluid was filtered through two layers of sterile cotton gauze to remove mucus. Alveolar cell populations were counted in a hemocytometer. Cell viability was determined by trypan blue exclusion and all recovered cells showed >90% viability. Cell pellets and supernatants were separated by centrifugation at 1000 rpm for 10 min. BAL fluid supernatant was divided into aliquots and stored at minus 70°C until assayed. The cell pellet was washed twice in serum free RPMI (Cellgro, Manassas, VA) and resuspended in RPMI at 106 cells per mL and cultured in suspension for 24 h at 37°C. Supernatants from the cell culture were collected and frozen at −70°C until assayed. In a single batch, IFN-γ and a panel of potentially important cytokines and chemokines were measured in aliquots from the BAL and the 24-h cell culture supernatant by Luminex Beadlyte ELISA assay. Protein concentrations (albumin) for BAL fluid measurements were corrected with the BCA Protein Assay (Pierce, Rockford, IL).
Treatment protocol
Baseline assessment included physical examination, vital signs, ECG, oxygen saturation by pulse oximetry, and a 6-min walk test. Full pulmonary function testing (PFTs) and blood sampling were performed at baseline and every 12–14 weeks until the conclusion of the study. Retrospective PFT data were obtained by reviewing patient records for 5 months prior to study entry. The same laboratories measured the study and retrospective PFTS. Complete blood count, liver, and renal function were monitored. Plasma and BAL IFN-γ levels were measured at baseline and after the second bronchoscopy. After the initial assessment and signing of consents, the baseline bronchoscopy was performed followed by nebulizer education and the first deposition study. Subjects were treated with 100 μg of IFN-γ via the I-neb AAD system three times a week for 80 weeks. The dose was chosen based on the efficiency of the nebulizer and the measured lung dose from previous studies in tuberculosis patients with less efficient devices.(16,18)
The treatment protocol was performed at New York University Medical Center. The in vitro aerosol studies and the in vivo deposition studies were performed at Stony Brook University Medical Center. All patients gave written, informed consent to participate in the study, which was approved by the appropriate independent institutional review boards of both institutions. The study is registered at ClinicalTrials.gov (NCT00563212).
Data analysis
Deposition, pulmonary function testing, and cytokine levels were analyzed using descriptive statistics including mean and standard error. Linear regression analysis was used to evaluate the aerosol formulations to compare amount of radioactivity and drug present. Wilcoxon matched-pairs rank test was used to compare plasma and BAL cytokine levels pre- and posttreatment. Cytokine data was considered exploratory. In exploratory studies in which data are collected with an objective but not a prespecified key hypothesis, multiple test adjustments are not required. The multiple tests used in this study were for descriptive purposes and not for decision making. Further studies with defined hypotheses will be needed to confirm these possible associations.(28) Patient adherence was quantified by downloading I-neb AAD system usage data at the end of the trial. True adherence was defined as the product of adherence and compliance. Adherence was defined as the number of treatments started by each patient expressed as a percentage of the number of treatments expected in a given time period based on the prescribed regimen for that patient; compliance as the number of treatments started by each patient that were completed (i.e., “Full” dose recorded by I-neb AAD system) expressed as a percentage of the total number of treatments started by the patient.(23)
Results
Effects of vibrating mesh nebulization on IFN-γ
Figure 1 summarizes the viral inhibition assay results from captured aerosols. IFN-γ activity in control aerosols of normal saline (NS) and samples of assay buffer (PBS) was undetectable. Viral inhibition at serial dilutions was consistent with the nominal concentration of interferon in the original vial (e.g., 2 million units/0.5 mL diluted 160,000 times, expected activity 5 IU) confirming that nebulization with the I-neb AAD system did not diminish IFN-γ bioavailability.
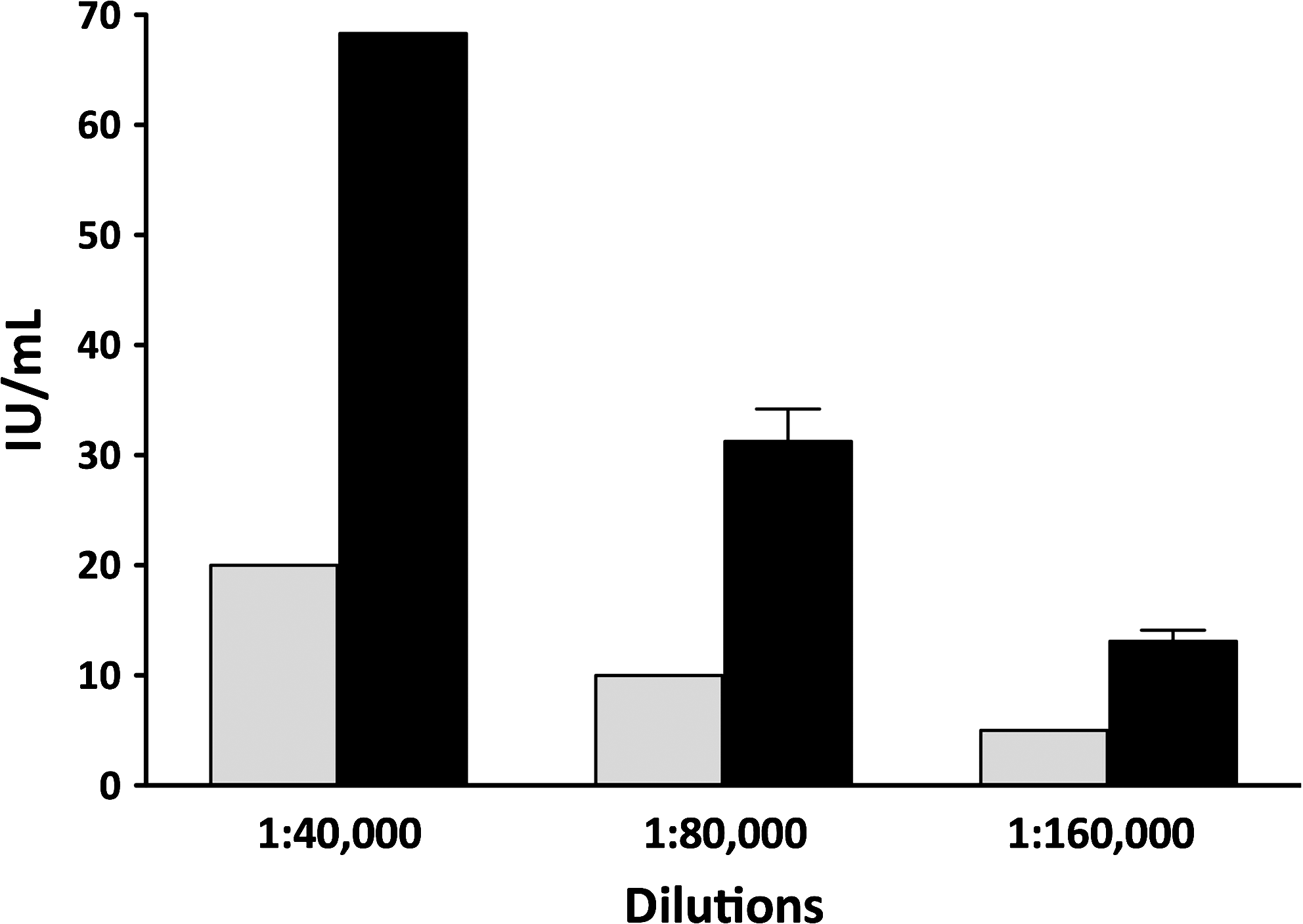
Viral inhibition activity of interferon gamma (INF-γ) aerosol [in international units (IU/mL)] for serial dilutions of aerosol condensate (filled bars), Predicted levels from dilution of nominal dose in vial (2 million IU) (open bars); captured normal saline aerosol and sample buffer controls had undetectable activity.
In vitro correction for sulfur colloid
Figure 2 depicts radioactivity captured on serial filters plotted against albuterol activity both as a percent of nebulizer charge. For aerosols labeled with free 99mTc the data well approximated the line of identity (y=0.946x + 0.272, R=0.983, p<0.001) indicating that free 99mTc accurately represented albuterol activity. For 99mTc-SC there was a shift of the line to the right (y=0.637x + 0.276, R=0.924, p<0.001), indicating that more drug was nebulized per unit of radioactivity. This observation was consistent with retention of 99mTc-SC in the nebulizer.

Radioactivity captured on filters for albuterol aerosols versus drug activity (measured by assay) as percent of nebulizer charge from the same filter: aerosols labeled with free 99mTc lie close to the line of identity (y=0.946x + 0.272, R=0.983, p<0.001) left panel; aerosols labeled with 99mTc-sulphur colloid (SC) are shifted to the right, indicating some 99mTc-SC is systematically retained in the nebulizer (y=0.637x + 2.76, R=0.924, p<0.001) right panel.
Patient deposition and particle diameter
Individual results of deposition studies and particle size expressed as MMAD are listed in Table 2. All deposition data were corrected for SC adherence to plastic using the equation from Figure 2.
Data are presented as percent of initial nebulizer charge.
ML, middle lobe; sC/P, central to peripheral ratio of deposition image divided by 133Xe image; MMAD, mass median aerodynamic diameter.
Percentages refer to the initial amount of drug placed in the nebulizer (100 μg=nebulizer charge).
In vivo lung deposition averaged 65.4±4.8% (±SEM) of the nebulizer charge with 16.5±1.4% depositing in the middle lobe. Variability in deposition was attributed primarily to differences in oropharyngeal deposition. Oropharyngeal deposition averaged 12.6±3.0%. Regional lung deposition, quantified by the ratio of central to peripheral distribution of deposited particles (sC/P ratio), averaged 1.20±0.6 indicating relatively peripheral distribution (1.0 represents undetectable deposition in central airways). Inspection of Table 2 indicates some negative values of deposition as well as values totaling (lung depo plus stomach depo) above 100%. These reflect experimental error.
Particle diameters ranged from 1.2 to 2.8 μm with a mean MMAD of 1.7±0.11 μm.
BAL fluid results
An average of 40 million cells/mL were recovered from BAL both before and after treatment with a macrophage predominance (pre: 76.7% macrophages vs. post: 81.7% macrophages). Pretreatment versus posttreatment changes in cell count and differential were not significant. Cytokine and chemokine analyses were performed on BAL fluid, 24-h cell culture supernatants, and plasma (Table 3). Albumin correction of BAL fluid allowed calculation of cytokine or chemokine per milligram of protein. The mean baseline BAL fluid level of IFN-γ corrected for protein increased from 5.23±3.16 to 320±79.5 pg/mg, p=0.002. Mean 24-h cell culture supernatant levels of IFN-γ also increased from 8.25±5.40 to 36.9±11.0 pg/mL, p=0.027. Mean 24-h cell culture supernatant levels of FGP-2, Flt-3 ligand, and IL-5 were significantly decreased.
BALF, bronchoalveolar lavage fluid, corrected for albumin.
Mean contains value(s) below assay sensitivity; these values were replaced with value of lowest standard in assay.
Mean contains value(s) above assay sensitivity; these values were replaced with value of highest standard in assay.
Data expressed as MEAN±SEM; p-value calculated using Wilcoxon signed-rank test.
Correlation of deposition studies with levels of interferon in BAL fluid
Figure 3 depicts changes in the level of IFN-γ (pg/mg protein/mL) removed by BAL from the middle lobe, plotted against lung deposition (highest of two studies) in the middle lobe region of the gamma camera image (R=0.651, p=0.035, Spearman correlation).
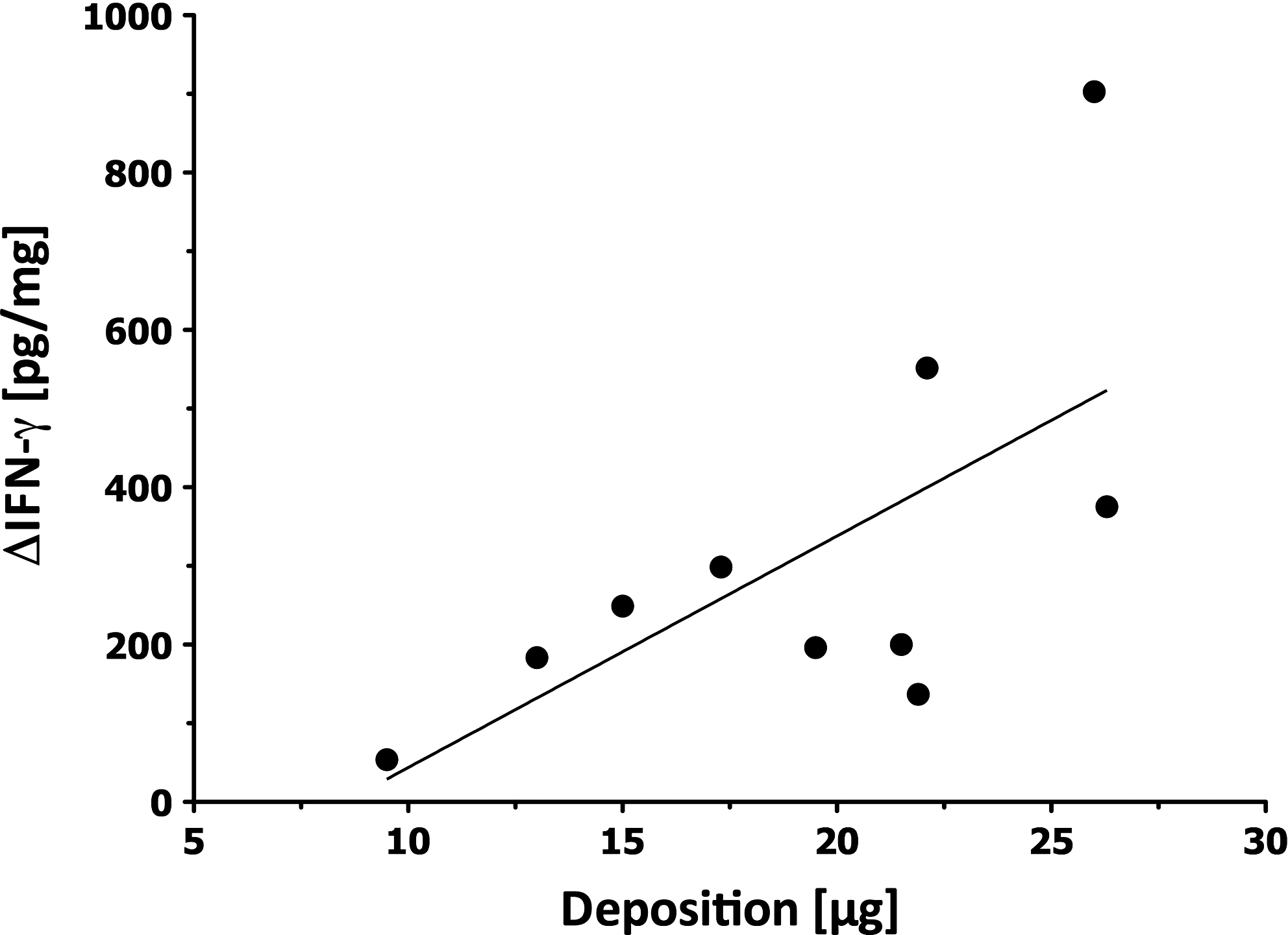
Change in BAL levels of interferon gamma (INF-γ pg/mg protein) following aerosol therapy versus middle lobe deposition (highest of two studies) (y=29.4x − 251, R=0.651, p=0.035, Spearman correlation).
Clinical testing; Safety and tolerability
Ten patients were sequentially enrolled in the clinical trial starting in June 2008. Three patients had a diagnosis confirmed by open lung biopsy reviewed by a pulmonary pathologist while the rest met clinical criteria and had consistent chest high-resolution computed tomography scans. Patients were enrolled within 4 weeks of screening. The last patient finished treatment in December 2009. All 10 patients were followed for a minimum of 80 weeks with a range of 80 to 130 weeks. The majority of patients were male and White, with a mean age of 68 years. Clinical and pulmonary function parameters were similar across the group at the time of entry and details of the demographics are shown in Table 4. All patients completed >90% of scheduled visits.
OBLx, open lung biopsy; CT, CAT scan of the chest; NAC, N-acetylcysteine; FVC, forced vital capacity; TLC, total lung capacity; DLCO, diffusing capacity for carbon monoxide (% predicted).
True adherence with aerosol treatment averaged 96.7±4.81%. Treatment time ranged from 3–20 min.
No significant systemic side effects were reported. The most common side effect was cough, which affected five patients during the initial few breaths of each treatment. Two patients coughed throughout a typical treatment session. There were no significant changes in 6-minute walk test over the 80 weeks of treatment (pre- vs. posttreatment, 386±41.35 vs. 382±49.38 meters, p=1.000).
Pulmonary function tests [forced vital capacity (FVC), total lung capacity (TLC), and diffusion capacity (corrected for Hb, DLCO)] are shown in Figure 4. Values are plotted as percent predicted change from baseline. For most of the patients PFT data obtained from 20 weeks prior to baseline and enrollment are included. TLC and DLCO were declining at the initiation of aerosol therapy. FVC appeared stable, which is consistent with a decreasing residual volume. With therapy the decline in TLC and DLCO reversed and all parameters including FVC improved. After approximately 1 year of therapy values peaked and began to decline.
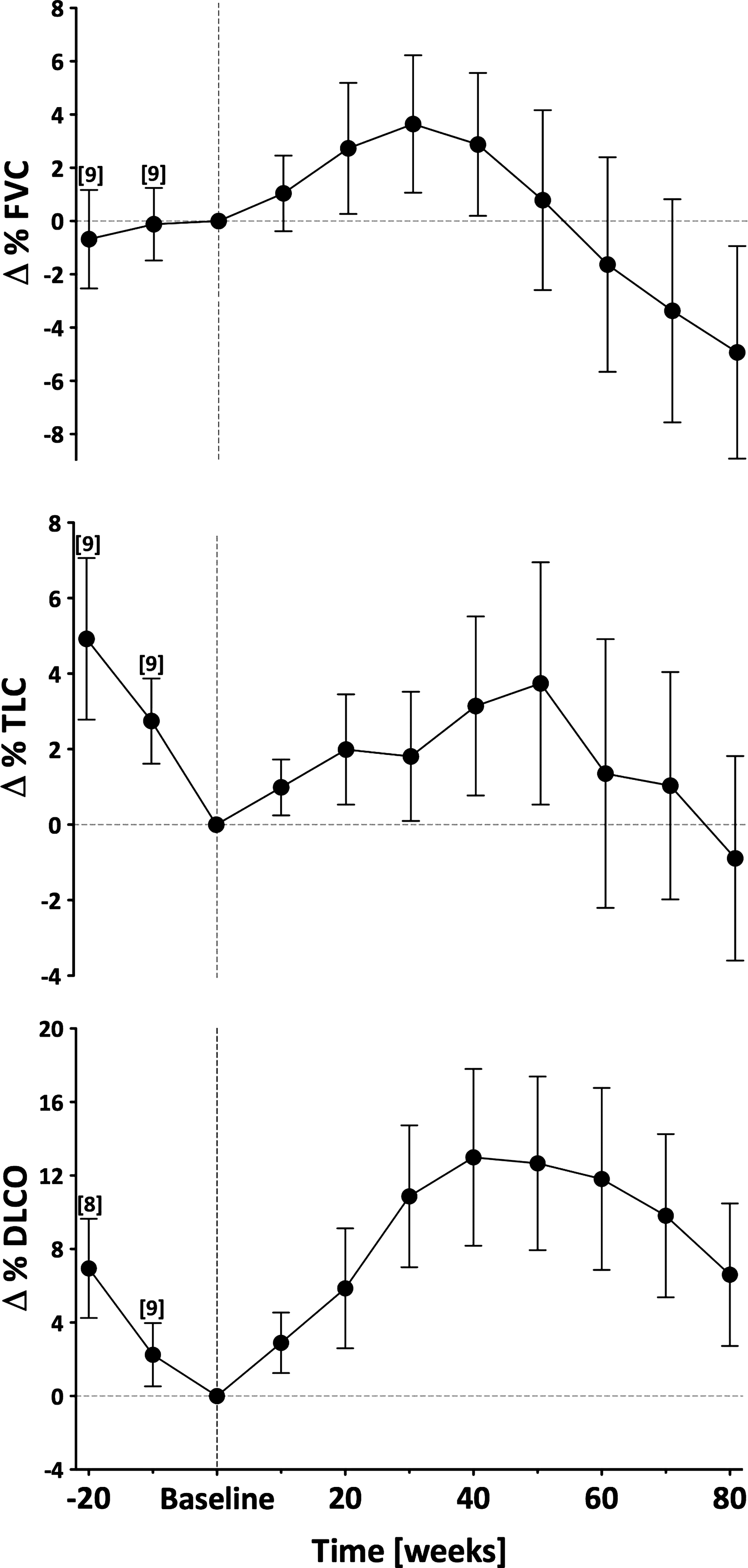
Forced vital capacity (FVC), total lung capacity (TLC), and single breath diffusion capacity (DLCO), plotted as change in percent predicated from baseline. Baseline and posttreatment over a period of 80 weeks (10 patients) are shown as well as retrospective data over 20 weeks prior to initiating treatment (nine patients for TLC and FVC, eight for DLCO). Dotted line represents baseline value and beginning of therapy.
Discussion
This study illustrates the potential use of inhaled IFN-γ as a novel therapy for IPF, bringing pharmacologic doses of the drug directly to the site of disease. We attained levels in BAL fluid that are not possible with parenteral therapy and the systemic effects of subcutaneous IFN-γ were not seen in our study. The most common side effect was cough, possibly secondary to upper airway irritation. It is possible that some patients with airways disease may not tolerate inhaled IFN-γ but the present study in IPF, combined with our previous work with inhaled IFN-γ in tuberculosis, indicates that the drug is safe in most humans with serious lung diseases.(18) Biologic proteins made via recombinant techniques may have to overcome higher safety standards than chemically synthesized aerosolized agents.(29,30) Because of this concern, our study has increased value. All of our patients were treated for 80 weeks and some for up to 2 years, far beyond the usual phase 1 safety study for a new drug. Future studies should include a dose-escalation component to fully assess the range of tolerability. As with all reported studies of proposed treatments for IPF there are no clear indicators of efficacy. Therefore, the optimal level of drug in the lung is unknown. However, we know that the range of lung dose that we have reported in tuberculosis is sufficient to treat that disease, evidence for macrophage activation at the levels reached by our aerosols.
In previous studies we measured deep lung deposition in tuberculosis patients averaging only 7% of the nebulizer charge with more aerosol deposited in upper airways (10% of the nebulizer charge) than in the lungs.(16) In the present study, we achieved an order of magnitude increase in lung deposition per treatment utilizing a novel delivery system (65% vs. the previous 7%). Upper airway deposition remains a problem (13%) likely secondary to the fraction of aerosol particles above 3 μm.(24,31) In the current study gamma camera data confirmed peripheral lung deposition with an sC/P ratio of 1.20. BAL data demonstrated significantly increased levels of IFN-γ in the epithelial lining fluid following aerosol therapy in all IPF patients. These levels appeared to be dose dependent illustrating the importance of choice of the delivery device and control of deposition. The absence of a concomitant increase in plasma levels likely explains the favorable side effect profile of aerosolized interferon gamma when compared to subcutaneous administration.
The effects of pharmacologically administered IFN-γ on the cytokine/chemokine milieu of the alveolar space are unknown. In our exploratory studies in tuberculosis and IPF we have measured a range of cytokines thought to be important. In tuberculosis, we have shown that aerosol IFN-γ treatment leads to significant decreases in pro-inflammatory cytokines in BAL fluid (IL-1b, IL-6, IL-8, and IL-10).(18) In IPF, 24 h cell supernatant levels of IFN-γ were increased while FGP-2, Flt-3 ligand, and IL-5 were significantly decreased. In models of pulmonary fibrosis, cytokine deficient-mice have worsening fibrotic disease with a shift in cytokine balance to a TH2 CD4+ T cell response involving IL-4, IL-5, and IL-13.(32) TH2 driven inflammation is involved in the pathogenesis of both hepatic fibrosis(33) and pulmonary fibrosis.(34) IL-5 has been shown to augment the progression of liver fibrosis by regulating IL-13 activity and it is increased in areas of active fibrosis in a murine model of pulmonary fibrosis.(35) Inhaled IFN-γ may attenuate the fibrotic response in IPF by promoting a TH1 cytokine profile. Other pro-fibrotic pathways may be important. FGF-2 has been associated with increased fibronectin synthesis in fibroblasts of patients with IPF(36) and fibroblast proliferation.(37) Therefore, decreasing FGF-2 activity may be useful in IPF. Flt-3 ligand is important as a hematopoietic cytokine and for the development and function of the immune system.(38) Its activity in IPF may be a measure of cellular proliferative activity secondary to the underlying disease process or associated infection, for example, by a virus.
Our study was designed to assess safety of long-term administration of inhaled IFN-γ in IPF patients; therefore, no therapeutic conclusions can be drawn. However, our observations allow some speculation regarding pulmonary function testing that may be useful in design of future studies. Controlled clinical trials of potential therapeutic agents for IPF have focused on pulmonary function. In all reported studies, both treatment and placebo arms report a 5–10% decline over 50 weeks (primarily changes in FVC).(5–7,13,39) In our study, serial measurements of pulmonary function were obtained with increases in TLC, FVC, and DLCO after initiation of aerosol therapy. This change became more apparent when prebaseline pulmonary function data obtained retrospectively was added (the same laboratories performed the pre- and posttreatment testing). Before initiation of aerosol therapy, the rate of decline in pulmonary function was consistent with that expected in IPF.(39) With initiation of inhaled IFN-γ, the decline seen over the initial 20 weeks of observation did not continue and, in fact, appeared to reverse. If this observation is indeed a signal of a treatment effect, it may serve as a possible endpoint for future clinical trials. It is not known what parameters best signal a drug effect short of a reduction in mortality. In addition to FVC, our study suggests that data analysis may be enhanced if patients are followed for a time before randomization. Those patients with declining function may then be randomized and benefits of therapy more readily detected.
Footnotes
Acknowledgments
The authors thank Lorraine Morra for technical assistance in performing the aerosol studies and preparing the manuscript and Maryann Huie who performed the cytokine analysis. The study was supported in part by Philips Respironics.
Author Disclosure Statement
Dr. Smaldone serves as a consultant to Philips Respironics. Stony Brook University and New York University jointly hold patents in the treatment of IPF with inhaled IFN-γ.