
Abstract
Abstract
Background:
The Abbreviated Impactor Measurement (AIM) concept simplifies determination of aerodynamic size metrics for inhaler quality control testing. A similar approach is needed to compare in vitro particle size distribution metrics with human respiratory tract (HRT) deposition.
Methods:
An abbreviated impactor based on the Andersen eight-stage cascade impactor (ACI) was developed having two size-fractionating stages with cut-points at 4.7 and 1.1 μm aerodynamic diameter at 28.3 L/min, to distinguish between coarse (CPM), fine (FPM), and extra-fine (EPM) mass fractions likely to deposit in the oropharynx, airways of the lungs, or be exhaled, respectively. In vitro data were determined for pressurized metered dose inhaler (pMDI)-delivered salbutamol (100 μg/actuation ex valve) with an “Alberta” idealized adult upper airway (throat) inlet (AIM-pHRT). Corresponding benchmark data for a full resolution Andersen eight-stage cascade impactor with “Alberta” idealized throat (ACI-AIT) and ACI-Ph.Eur./USP inlet were obtained with the same product.
Results:
Mass recoveries (μg/actuation; mean±SD) were equivalent at 100.5±0.7; 97.2±4.9 and 101.5±9.5 for the AIM-pHRT, ACI-AIT, and ACI-Ph.Eur./USP induction port, respectively [one-way analysis of variance (ANOVA), p=0.64]. Corresponding values of CPM were 59.2±4.2; 58.4±2.4, and 65.6±5.8; the AIT captured larger particles more efficiently than the Ph.Eur./USP induction port, so that less large particle mass was apparent in the upper stages of the ACI-AIT (p≤0.037). Equivalent values of FPM were similar regardless of inlet/abbreviation at 41.3±4.2; 38.7±3.0, and 35.9±3.8 (p=0.054), and EPM measures (1.7±0.3; 2.0±0.5; 2.1±0.3) were also comparable (p=0.32).
Conclusions:
The AIT inlet significantly increased the capture of the coarse fraction compared with that collected by the Ph.Eur./USP induction port. Measures obtained using the AIM-pHRT apparatus were comparable with those obtained with the ACI-AIT.
Introduction
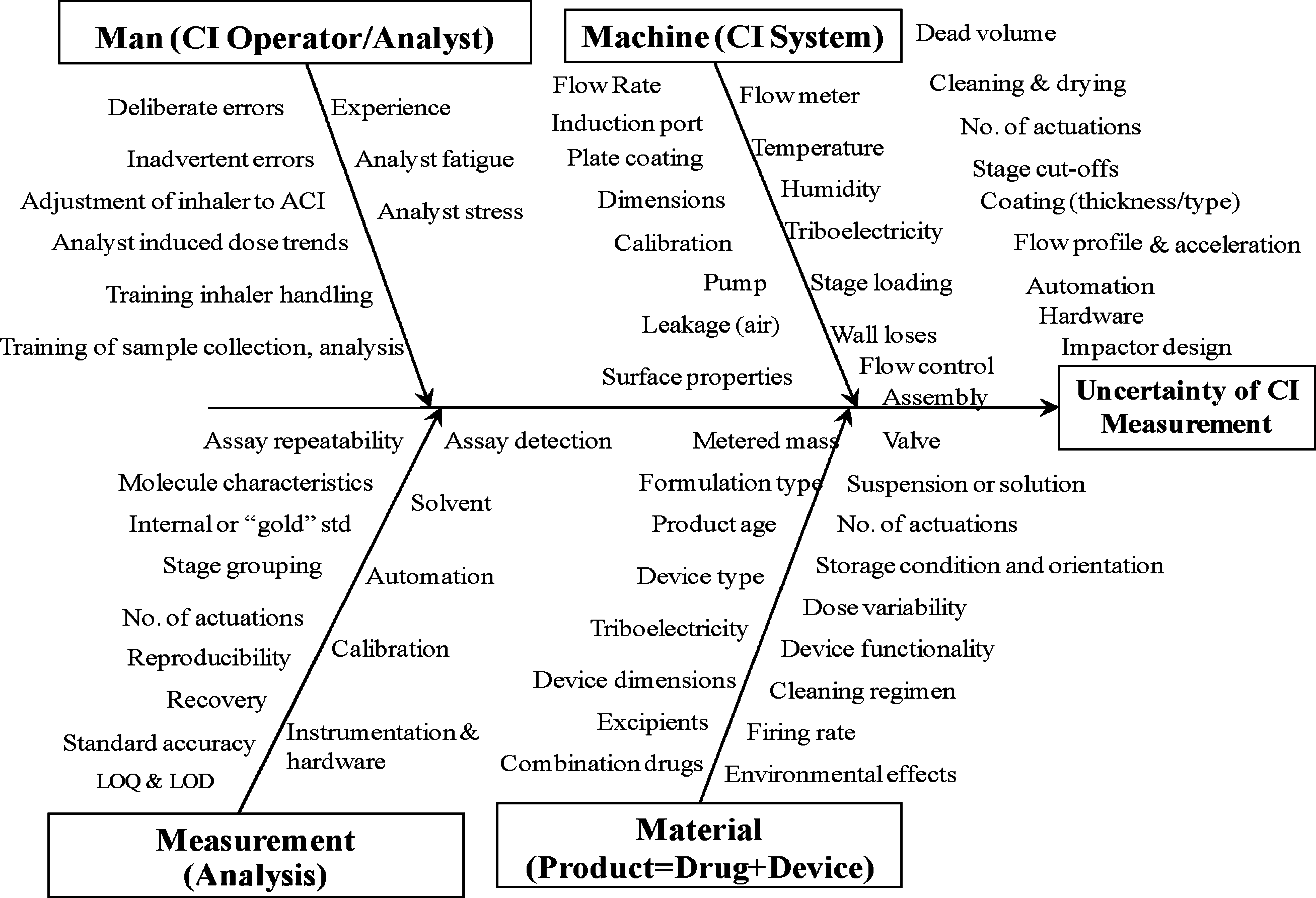
Contributors to variability in the cascade impactor measurement of an OIP-generated aerosol (from Bonam et al.;(2) used with permission).
1. Man—the CI operator/analyst;
2. Machine—the CI system;
3. Measurement—the API recovery and analysis procedure;
4. Material—the inhaler including its drug product
The CI is not a direct simulator of particle deposition in different regions of the human respiratory tract, because the air velocity through the system is constant, unlike the progressively decreasing velocity profile with airway generation number, and individual stage collection efficiency curves are much steeper than the counterparts for size-dependent regional deposition.(3) Nevertheless, it provides APSD data that are indicative of the likely deposition profile of the inhaled particles in the respiratory tract.(4) For this reason, regulatory agencies require cascade impactor-measured APSD-derived metrics, such as coarse, fine, and extra-fine mass fractions as a key component of the in vitro portion of the data in support of OIP registrations. However, it has to be recognized that at the most fundamental level, the CI method is not truly representative of patient inhalation conditions (including the impact of obstructive lung disease), so that that the outcome of measurements made by this technique, including variations of the sort that are the purpose of this article, may be more influenced by differences between this measurement technique and clinical reality.
The abbreviated impactor measurement (AIM) concept was recently developed as a way to reduce the complexity of the full resolution measurement equipment, addressing primarily the man and machine contributions to overall measurement variability.(5) By adopting AIM-based cascade impaction systems, the number of collection stages is reduced to the minimum required to obtain meaningful aerodynamic diameter-related measures of OIP aerosol performance in terms of mass of active pharmaceutical ingredient (API).(6) The following advantages then become possible:(5)
1. Reduced time per determination;
2. The chances of operator-related errors should decrease, as the result of reducing the number of manipulations required to make a measurement;
3. If the time savings are used to make more replicate measurements, data that are more representative of the OIP should be possible as the result of increased coverage of the whole population of possible outcomes;
4. The potential exists for better decision making in the product quality control (QC) environment if Effective Data Analysis metrics are used in place of traditional groupings in terms of mass of API collecting on the multiple stages of a full resolution CI;
5. The use of less solvent for API recovery and quantitation, is more environmentally friendly and in line with green chemistry principles;
6. The simpler apparatus configurations are potentially more amenable to automation.
There are two distinct applications during the OIP product lifecycle in which AIM is applicable (Table 1), and it is important at the outset that the user chooses the appropriate AIM-based approach. In the OIP QC environment, which is not the focus of the current article, all that is needed is a two-stage system that size fractionates the incoming aerosol into small and large particles at a size that is ideally located close to, but does not need to be exactly at its mass median aerodynamic diameter (MMAD).(5) Although AIM-QC systems have the potential to provide powerful decision-making capability in the context of batch disposition when associated with effective data analysis,(5,6) the boundary size between the two mass fractions, by being preferentially close to the MMAD, may not relate well to traditional size bounds that have been associated as being physiologically important. The most important of these is the fine-to-coarse particle division that is set either close to, or exactly at 5.0 μm aerodynamic diameter, if the European Pharmacopeial method for determining OIP aerodynamic particle size distribution (APSD) is being followed.(7) Another important size boundary occurs at close to 1.0 μm aerodynamic diameter, where it may be important to separate the fine particle fraction so that the submicron sized extra-fine particles may be separately distinguished.(8) This additional discriminating capability may be important because extra-fine particles have a higher probability of being exhaled without depositing in the lungs compared with fine particles larger than this limit.(6) It has been also suggested that pressurized meter dose inhaler (pMDI)-delivered corticosteroid submicron particles produced from ethanolic solution formulations in hydrofluoroalkane propellant may improve outcomes in patients as a result of greater penetration into the peripheral airways.(9)
Derived from the table presented by IPAC-RS at the March 2011 IPAC-RS Conference (http://ipacrs.com/PDFs/IPAC-RS%202011%20Conference/AIM%20Workshop/2-CI%20Workshop%20March%202011-Tougas.pdf) as well as at the IPAC-RS Satellite Workshop at Respiratory Drug Delivery Europe 2011 (http://ipacrs.com/PDFs/CI%20Workshop/1-Introduction%20and%20Lifecycle%20-%20Tougas.pdf)—used by permission).
The parallel development of an alternative approach to the AIM-QC abbreviated impactor development has taken place for the purpose of providing size-based metrics that are potentially more relevant as predictors of likely particle deposition in the adult human respiratory tract.(4) Such systems have been termed AIM-human respiratory tract (pHRT) systems, in recognition of their different applicability to those used in OIP QC (AIM-QC systems). The prefix “p” denotes their potential status, as their applicability in support of aerosol measurements pertinent to the understanding of how aerosol particles deposit in the respiratory tract has still to be proven in relation to clinical data.(4)
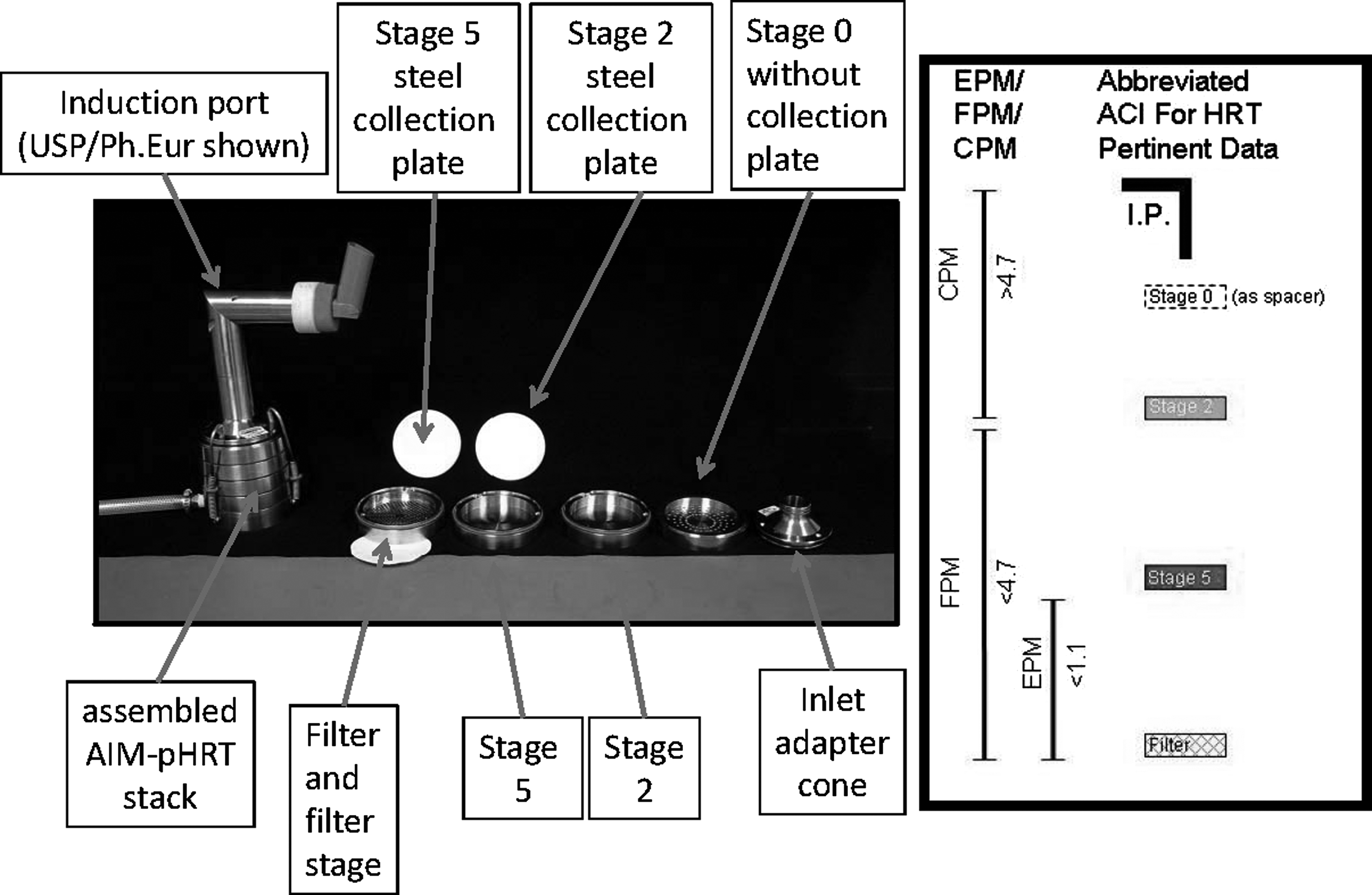
In the past 2–3 years, the AIM concept has been applied to a variety of different CI systems, albeit mostly intended for OIP QC use.(10) The earliest pHRT version was developed and validated in 2008–2009 in a precision study alongside an AIM-QC system and Andersen eight-stage nonviable cascade impactor (ACI), was based on this particular full resolution impactor.(11,12) This apparatus (Fig. 2), together with its counterparts, were each evaluated when equipped with the standard Ph.Eur./USP induction port. This inlet comprises a tapered entry and exit with a straightforward right-angle bend that simulates the adult oropharynx in a rudimentary way.(13) The AIM-pHRT impactor retained stages 2 and 5 and the filter collection stage of the full resolution ACI, so that three subfractions of the incoming aerosol could be classified at a fixed flow rate of 28.3 L/min: coarse particle mass (CPM) >4.7 μm; fine particle mass <4.7 μm and extra-fine particle mass <1.1 μm. Stage 0 was also retained but without its collection plate, as this stage provided additional dead space, matching more closely the internal volume of the ACI before the first size-fractioning stage.
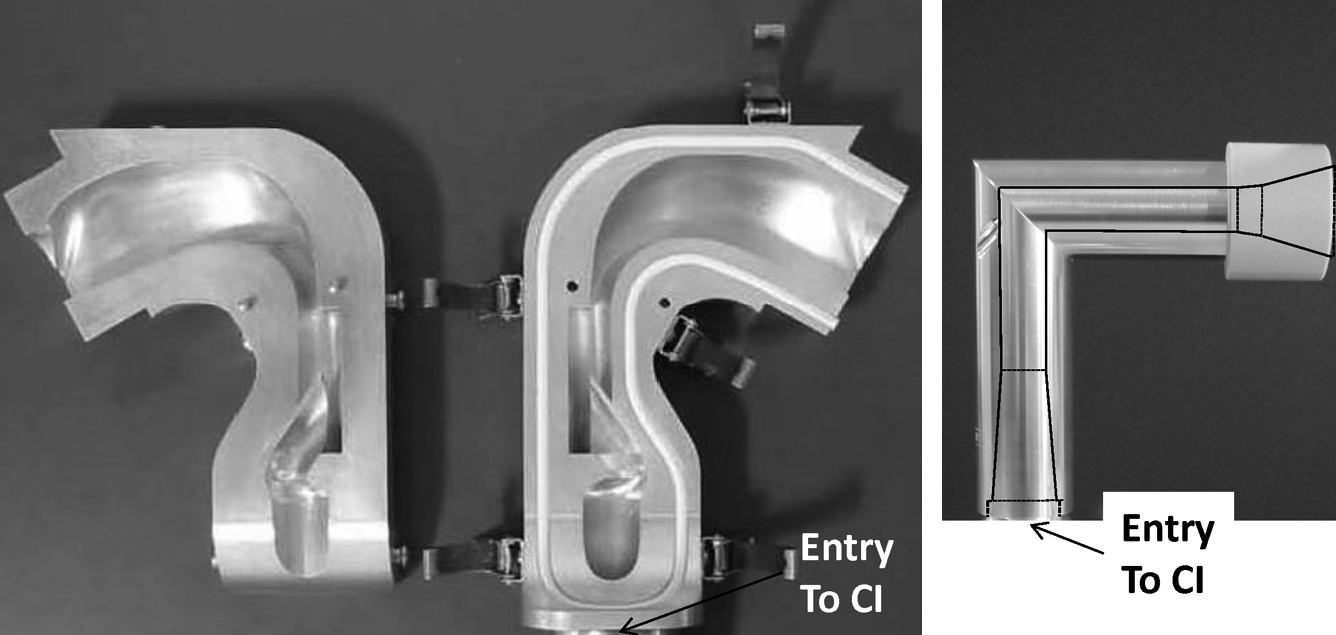
Opened AIT (left-hand side) showing flow pathway and compared with Ph.Eur./USP induction port showing outline of internal flow pathway (right-hand side).
The purpose of the present scoping study was to assess relative performance of the AIM-pHRT when used with the “Alberta” idealized adult throat (AIT) inlet developed by Finlay and coworkers to mimic aerosol interaction as would be the case with an average adult human oropharynx. The AIT(14,15) (Fig. 2) can be manufactured relatively easily in aluminum, in contrast with anatomically correct oropharyngeal models. Apart from its ability to mirror the behavior of particle transport through the oropharynx, the use of metal rather than nonconducting materials in its construction may be important in the context of possibly mitigating the influence of the significant electrostatic charge that is known to be present with pMDI-generated aerosols.(16) Extensive theoretical and experimental work has been undertaken by Finlay and coworkers in order to develop this inlet to the point at which it can be standardized for general use, as has been done for the Ph.Eur./USP induction port.(14,15,17,8) A recent study by Zhou et al.,(19) in which the AIT was calibrated with monodisperse particles, confirmed that its size-dependent particle deposition properties are comparable with an anatomically correct adult upper airway model developed by the Lovelace Respiratory Research Institute in Albuquerque (LRRI model) that is widely used as an inlet in studies where the CI method is being used in conjunction with lung deposition data. Importantly, Zhou et al. demonstrated that particle deposition in both the AIT and LRRI model correlated well with lung deposition data reported in the literature when scaled using the impaction parameter, I:
where dae and Q represent particle aerodynamic diameter and volumetric flow rate through the inlet respectively. On the other hand, the simpler internal flow pathway in the compendial Ph.Eur./USP induction port (Fig. 2) behaved differently to the other two inlets, with its deposition efficiency profile outside the range of the mouth–throat data from the various deposition studies in human adults. Deposition within the Ph.Eur./USP induction port appeared to take place at larger values of I, suggesting that more of the ballistic/coarse particle fraction should penetrate downstream to the impactor at a given flow rate than would be the case with the other more clinically appropriate inlets.
Incorporation of the AIT is therefore the next logical step to develop the AIM-pHRT apparatus to be able to make measurements more appropriate in the context of predicting particle deposition in the adult respiratory tract.(19) It is important to reemphasize that this inlet is not an anatomically correct upper airway, but comprises the “idealized” geometry of its simplified pathway (Fig. 2), possessing particle deposition characteristics that mirror those of an average adult. In this way, it should collect the ballistic fraction of the plume emitted upon actuation of a pMDI in a more clinically relevant way than does the sharp, right-angle bend of the Ph.Eur./USP induction port.(20)
Materials and Methods
All measurements were undertaken with primed and shaken pMDI-delivered salbutamol (Ventolin®, EvoHaler®, GSK plc, UK, lot 9060, expiry date: June 2013), delivered from pMDIs with label claim dose of 100 μg/actuation salbutamol base equivalent ex valve. 5-Actuations from a primed canister were introduced with 30-sec between each actuation into each cascade impactor configuration per determination, shaking the canister between each actuation. The interior surfaces of the AIT (Copley Scientific Limited, UK) were coated with a thin layer of silicone oil, as were the collection plates of each CI. This coating was applied to simulate the mucosa, which are present in the upper airway, as was done by Ehtezazi et al.,(21) in a similar study investigating the pMDI-delivered medication to a cascade impactor via different anatomically correct oropharyngeal models. No attempt, however, was made to grease-coat the interior surfaces of the Ph.Eur./USP inlet with the AIM configuration, as although this practice may be necessary to achieve reliable calibration data, it is not common practice in the laboratory evaluation of OIPs. In the case of the collection stages, oil coating was applied to mitigate particle bounce and reentrainment that had been observed in previously reported measurements with abbreviated Andersen-type impactors.(22) All measurements with either abbreviated or full resolution impactor systems (n=5 replicate measurements/configuration) were undertaken at 28.3 L/min±5%.(11,12)
The AIM-pHRT system (Copley Scientific Ltd) (Fig. 3) was assembled out of ACI components, comprising the inlet cone, stage 0 without a collection plate, stages 2 and 5 and the glass microfiber backup filter to capture the extra-fine particles penetrating the second size-fractionating stage (Fig. 4). Note that the stage numbering in this abbreviated system follows the convention adopted for the full-resolution ACI. The nonoperating stage “0” was included, because previous work with ACI-based systems had shown that it is necessary to match closely the internal dead space of an abbreviated impactor with its full resolution counterpart in order to ensure comparable evaporation behavior with products containing low volatile solvents, such as ethanol.(23) Although the test product used in the present study did not contain low volatile solvent, the basic arrangement was retained to avoid developing more than one configuration of the AIM-pHRT system based on the ACI. Benchmark data were also made with canisters from the same lot of drug product using a full resolution ACI (Copley Scientific Ltd., Nottingham, UK), manufactured in stainless steel and equipped with either the same AIT or a Ph.Eur./USP induction port.

AIM-pHRT Impactor with AIT.
Configuration of the AIM-pHRT system based on the ACI compared with the full-resolution CI system.
Recovery for salbutamol from each stage of the impactor system on test was undertaken using HPLC-UV spectrophotometry by a validated procedure.
Descriptive statistics (MMAD) and geometric standard deviation (GSD) derived from the APSDs for the full-resolution impactor configurations were determined using CITDAS version 3.10 (Copley Scientific Ltd.). Inferential statistical analysis of the mass of salbutamol recovered from the various components of each configuration was subsequently undertaken using Minitab version 16 (Minitab Inc., State College, PA, USA), with p<0.05 deemed to be a statistically significant outcome.
Results
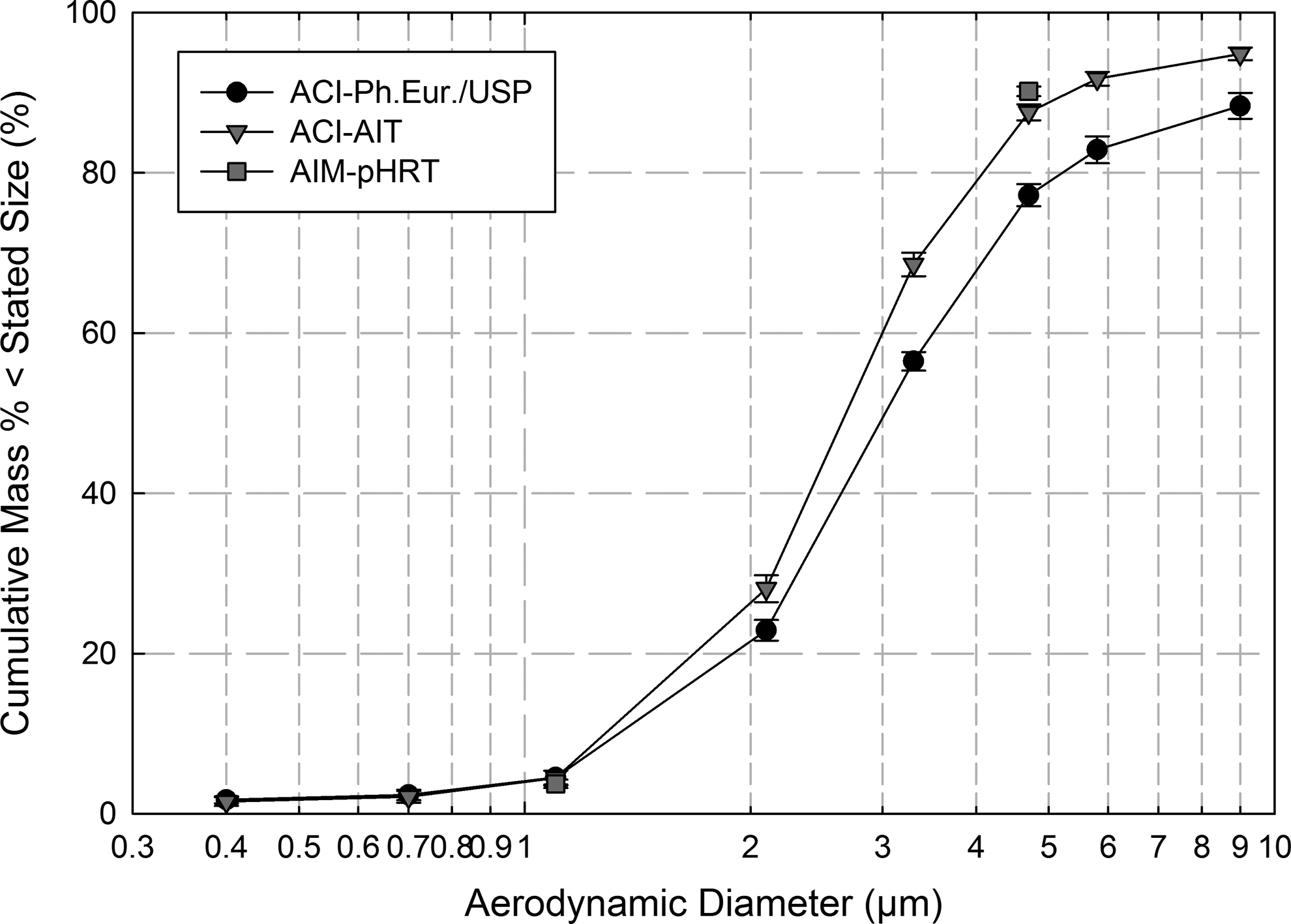
Cumulative mass-weighted APSDs determined by the two full-resolution ACI configurations (ACI-AIT and ACI-Ph.Eur./USP) were observed to be unimodal and close to log-normal within the range between the 16th and 84th mass percentiles, from which the GSD values are calculated. Figure 5 illustrates these data normalized in terms of the total mass recovered from the inhaler mouthpiece, induction port/inlet, and cascade impactor, and equivalent information normalized in terms of just the mass recovered from the impactor is presented in Figure 6. MMAD and GSD values (mean±SD) for the ACI-AIT were 2.7±0.0 μm and 1.6±0.0, respectively, compared with 3.0±0.1 μm and 2.1±0.3 for the ACI-Ph.Eur./USP (Table 2).
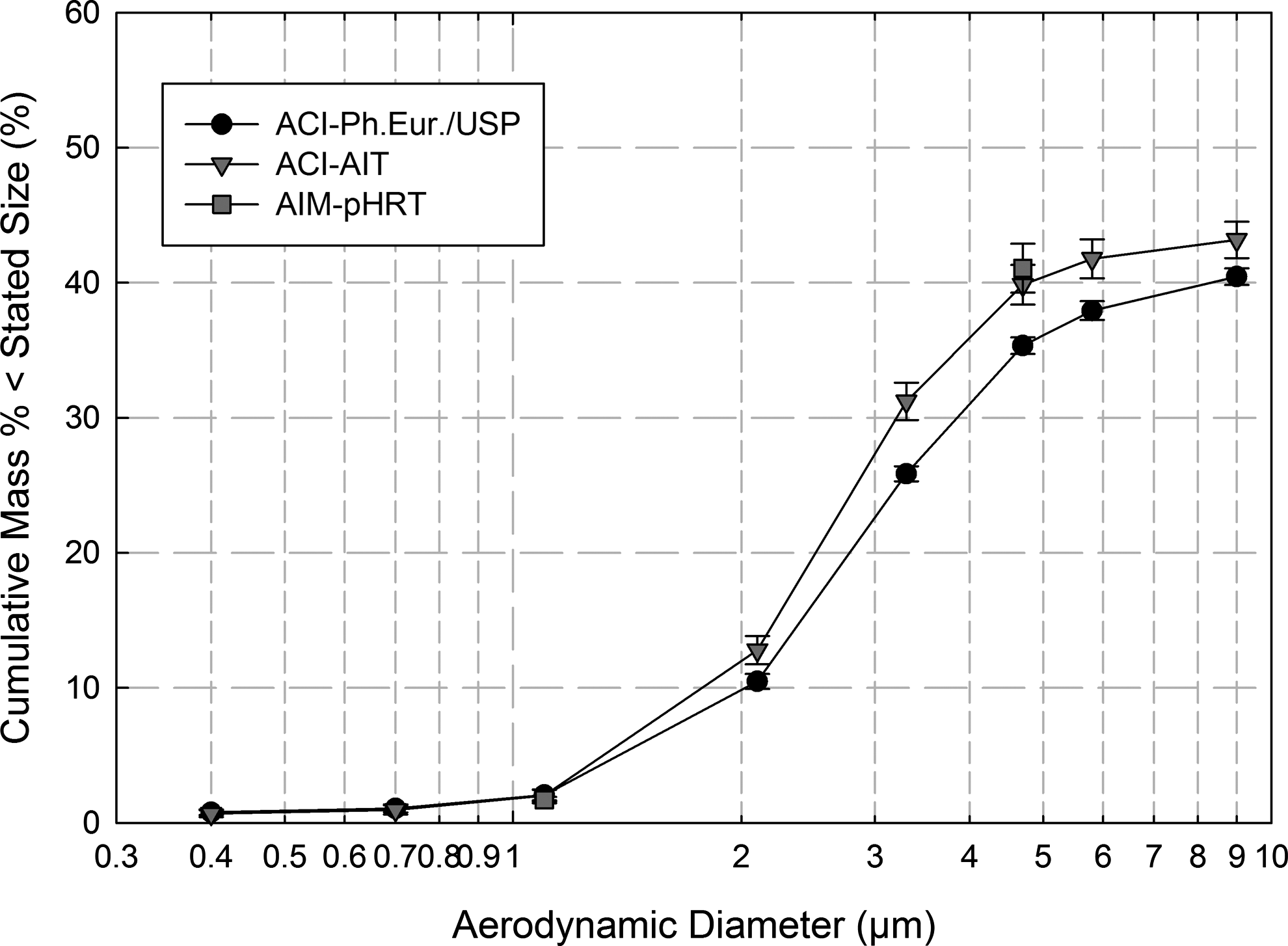
Cumulative mass-weighed APSDs for ACI-AIT and ACI-Ph.Eur./USP configurations with values of EPF, FPF, and CPF compared with measures from the AIM-pHRT apparatus. These data for pMDI-delivered salbutamol (100 μg/actuation) are normalized to the total mass ex inhaler mouthpiece.
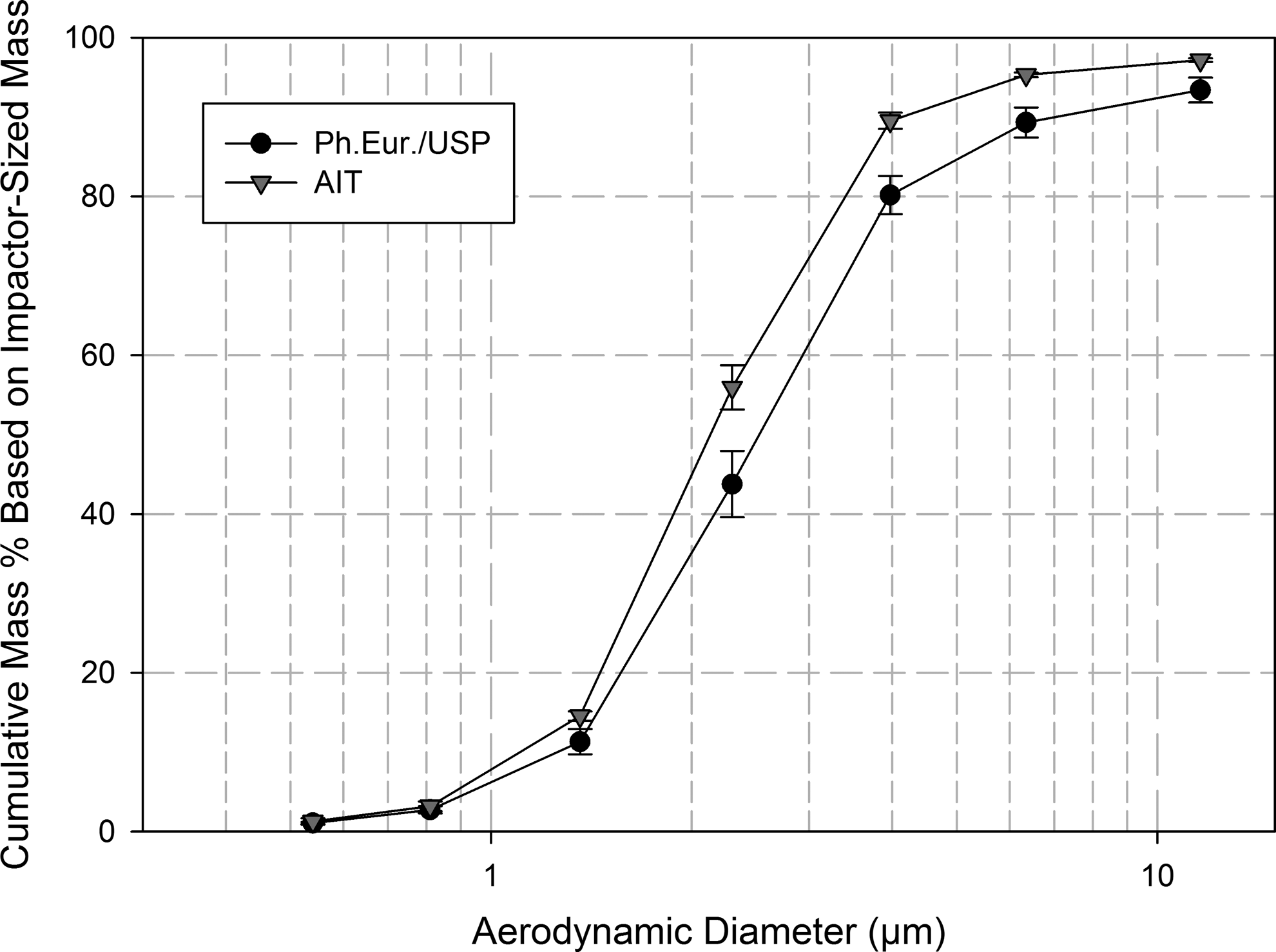
Cumulative mass-weighed APSDs for ACI-AIT and ACI-Ph.Eur./USP configurations with values of EPF, FPF, and CPF compared with measures from the AIM-pHRT apparatus. These data for pMDI-delivered salbutamol (100 μg/actuation) are normalized to the total mass that penetrated beyond the inlet to the impactor.
Individual total mass recovery values for salbutamol were within±16% of the label claim (100 μg/actuation), with most values within±10% label claim. The grouped mass recovery values (μg/actuation; mean±SD) were equivalent at 100.5±7.7, 97.2±4.9, and 101.5±9.5 for the AIM-pHRT, ACI-AIT, and ACI-Ph.Eur./USP configurations, respectively [one-way analysis of variance (ANOVA), p=0.64] (Table 3). Grouped salbutamol mass deposition data (mean±SD) are also summarized in this table on a component-by-component basis. Values of coarse particle mass (CPM), fine particle mass (FPM) and extra-fine particle mass (EPM), all determined ex pMDI valve, were calculated from the individual component deposition data, and are summarized in Table 4. The coefficients of variation (CofV) associated with these measures were comparable across configurations, increasing in magnitude with decreasing absolute mass as would be expected as these values approached closer to the lower limit of detection of 0.1 μg salbutamol/actuation. Coarse, fine, and extra-fine particle fractions (CFF, FPF, and EPF, respectively) were calculated based on the total mass recovered from the inhaler mouthpiece, inlet and impactor in Table 5; the CofVs associated with FPF and CPF were all <5%, with corresponding values in the range from 11.8% to 20% for EPF. The corresponding mass fractions determined based only on the mass captured in the impactor are summarized in Table 6; the CofVs for CPF increased slightly as a consequence of the elimination of the mass recovered from the inhaler mouthpiece and inlet/induction port from consideration.
Discussion
The corresponding APSDs, normalized either to total mass of salbutamol ex inhaler (Fig. 5) or just the mass recovered from the full resolution ACI (Fig. 6), both indicated that replacing the pharmacopeial induction port with the AIT resulted in a slight shift to finer sizes and decreased “spread,” based on comparisons of GSD. However, although the decrease in MMAD determined using the CITDAS software (Table 2) was just below statistical significance for MMAD (signed rank-test, p=0.063), the corresponding decrease in GSD was significant (paired t-test, p=0.011). This behavior is comparable with that observed in a previous investigation using a Next Generation Pharmaceutical Impactor (NGI)(24) with a similar pMDI-delivered formulation containing salbutamol, and sampling at the slightly higher flow rate of 30 L/min (Fig. 7). The AIT inlet therefore significantly increased the capture of the coarse fraction compared with that collected by the Ph.Eur./USP induction port.
Comparative APSDs of pMDI-delivered Salbutamol for a next generation pharmaceutical impactor (NGI) equipped with either Ph.Eur./USP induction port or AIT and operated at 30 L/min.
CI-determined APSDs are usually interpreted in terms of the total mass ex inhaler, as is necessary, for example, when examining the impact of add-on devices such as spacers and valved holding chambers on the emitted aerosol.(13) In the present investigation, which was focused on a change of inlet entry to the CI system, this type of analysis is most appropriate. When the absolute mass data obtained in this way (Table 4) are examined more closely, EPM with the two ACI variants (2.1±0.3 μg/actuation for the ACI-Ph.Eur./USP; 2.0±0.5 μg/actuation for the ACI-AIT) were statistically equivalent to 1.7±0.3 μg/actuation for the AIM-pHRT (one-way ANOVA, p=0.323). This outcome was anticipated as the change of inlet type would not likely propagate through the CI to affect the mass of particles passing through the second size-fractionating stage, especially as particle bounce and reentrainment of particles from the first impaction stage (stage 2) was mitigated by the use of a silicone oil coating.(22)
Likewise, FPM from the ACI-Ph.Eur./USP (35.9±3.8 μg/actuation) and ACI-AIT (38.7±3.0 μg/actuation) was comparable with 41.3±4.2 μg/actuation obtained by the AIM-pHRT system (p=0.054).
Interestingly, CPM obtained with the ACI-Ph.Eur./USP configuration (65.6±5.8 μg/actuation) was marginally larger than corresponding values obtained with the ACI-AIT system in either full resolution (58.4±2.4 μg/actuation) or abbreviated (59.2±4.2 μg/actuation) configurations, both of which were equivalent (unpaired t-test, p=0.73). These findings support the outcomes illustrated by the descriptive APSD statistics (Table 2), and also the observation of Zhou et al.,(20) that the Ph.Eur./USP inlet increased the mass of salbutamol that penetrated to the upper stages of the impactor compared with the situation that existed when the AIT was used, resulting in an increase in GSD, associated by a marginal increase in MMAD.
In contrast with measures of EPM and FPM, where differences between these systems were small, measures of CPM, that here included the mass of salbutamol recovered from the induction port and inhaler mouthpiece together, were significantly higher with the ACI-Ph.Eur./USP configuration (65.6±5.8 μg/actuation) compared with corresponding values using the AIM-AIT system (58.4±2.4 μg/actuation) or the AIM-pHRT configuration (59.2±4.2 μg) (p=0.042). Assuming that differences in mass recovery values from one apparatus to another were inconsequential (p=0.64), it appears that the Ph.Eur./USP induction port removed about 7 μg/actuation more of the combined ballistic/coarse particles emitted from the inhaler. However, closer examination of these data revealed that most of the difference was associated with an increase in mass collecting upon ACI stages 0 to 2 from 5.5±0.3 μg/actuation to 10.6±1.1 μg/actuation, rather than being associated with the mass collected in the induction port itself (Table 3).
The reproducibility in EPM, FPM, and CPM between all three configurations was within expectations, given the inhaler-to-inhaler variability associated with cascade impactor-based measurements,(2,25) and well within the±15% limit allowed for pMDI-emitted aerosol mass balance variability in the 1998 FDA Draft Guidance concerning Chemistry Materials and Controls for oral inhalers.(26)
Values of CPF, FPF, and EPF calculated as percentages of the total aerosol mass emitted from the inhaler (Table 5) were similar numerically to their counterparts determined in terms of absolute mass because the label claim unit dose from this particular drug product was 100 μg/actuation salbutamol base equivalent.
Inhaler aerosol CI APSDs may also be derived just considering the total mass of API that penetrates beyond the inlet into the impactor stages.(13) This type of analysis can be more revealing about the fine and extra-fine portions of the emitted aerosol, as the ballistic fraction and coarse particulate captured by the inhaler mouthpiece and inlet are removed from the analysis. Apart from the relatively small amount of API collecting on the first impaction stage of the ACI, for which there is no upper-bound size determined, the aerosol is fully size analyzed by the impactor. On this basis (Table 6), CPF, which was based solely on the mass collecting upon either impactor stages 0 to 2 for the two ACI configurations, or on the first stage of the AIM-pHRT system was substantially greater for the ACI-Ph.Eur./USP system (22.8±1.4%), compared with the ACI-AIT (12.5±1.0%) (p<0.001). The value of 9.8±0.6% for CPF with the AIM-pHRT system was also slightly lower than that obtained with ACI-AIT configuration (Mann-Whitney rank-sum test, p=0.008). This latter difference could potentially be anticipated from a theoretical analysis of the effect of removing intermediate stages on performance as the result of the imperfect size-selectivity of practical impactor stages, reflected by deviations in their collection efficiency-particle aerodynamic size profiles from step-functions at the effective cutoff diameter appropriate to each stage.(27) Measures of FPF for the ACI-Ph.Eur./USP (77.2±1.4%) were significantly lower than the equivalent measures for the AIM-AIT system (87.5±1.0%) or the AIM-pHRT configuration (90.2±0.6%) (p<0.001). The difference in this metric for the two configurations with AIT (Mann-Whitney rank-sum test, p=0.008) is likely to be more a reflection on these highly reproducible measures than a real difference. Measures of EPF with the ACI with either inlet configurations were identical (4.5±0.9%) and comparable with the equivalent values of EPF from the AIM-pHRT system (3.7±0.5%) (p=0.027).
The slight shift in impactor-measured APSD to finer sizes with the AIT, whichever way the APSD data are normalized, is consistent with the finding from the recent inlet comparison study already referred to in connection with the descriptive APSD statistics delivering pMDI-salbutamol to an NGI (Fig. 7). In that investigation, the MMAD of the impactor-sized portion of the aerosol (excluding the mass collecting in the induction port and on the first stage of the impactor, which does not have an upper size limit in the absence of its preseparator), was shifted slightly toward finer sizes from 2.5±0.1 μm to 2.2±0.1 μm, when pMDI-delivered salbutamol was sampled via Ph.Eur./USP and AIT inlets respectively.(28)
Placing the outcomes from the present measurements into context with other independent work, the Ph.Eur./USP induction port would be expected to be less efficient than the AIT at retaining coarser particles, based on the findings of the recently published inlet calibration studies of Zhou et al.(20) with monodisperse particles at 30 L/min. The estimated cut-point size, at which an uncoated Ph.Eur./USP induction port has 50% collection efficiency (D50), is more than 20 μm aerodynamic diameter, compared with approximately 10 μm aerodynamic diameter for their AIT, having a similar interior surface preparation by grease-coating to that used in the present investigation. However, it should be noted that in both instances that the particles in the Zhou et al. study were sampled from the aerosol generation equipment at a constant flow rate imposed by the vacuum source attached to the inlet on test. In contrast, in the present investigation, the aerosol plume entering each inlet from the inhaler mouthpiece was initially produced by propellant flash evaporation when the pMDI was actuated. Such plumes are ballistic in nature,(29) and therefore, at least to begin with, particle motion is largely not influenced by the flow generated downstream by the vacuum pump to which the impactor is connected. It has therefore to be recognized that the pMDI-generated polydisperse APSDs obtained with the two inlets in the present study (Figs. 5 and 6) and in similar work with the NGI (Fig. 7) cannot be directly compared with the inlet collection efficiency curves derived from monodisperse particle-based calibration measurements of inlet D50. Nevertheless, the relatively narrow separation between APSDs obtained with the two different inlets compared with the corresponding D50 values from their respective calibrations, might be taken as indicative that ballistic deposition dominated over inertial deposition for the particular pMDI used in the present study. However, it should be recognized that propellant expansion characteristics vary quite widely for different pMDI products,(29) making the likely distribution between ballistic and inertial deposition mechanisms inhaler product-dependent for this class of OIP.
Newman and Chan,(30) in an assessment of the reasons why it has thus far proven difficult to achieve robust in vitro–in vivo correlations in association with the various OIP formats, have commented that agreement between laboratory and clinical data may be improved by measuring APSD in ways that more closely mimic clinical use, including the use of impactor inlets that simulate the human upper airway anatomy. An important purpose of the present study has been to respond to this suggestion, in the context also of developing simpler techniques to determine aerodynamic size-related measures of OIP performance in the laboratory. Their correlation of fine particle fraction <5.8 μm aerodynamic diameter obtained by ACI-Ph.Eur./USP systems against whole lung deposition for hydrofluoroalkane-propelled aerosols similar in APSD to the product used in the present work, is also suggestive that the compendial inlet allows more of the coarse particulate/ballistic component from the inhaler to penetrate to the impactor. On this basis, the AIT, by retaining more of the coarse ballistic fraction entering the system would appear to have enabled the AIM-pHRT system to size-fractionate the incoming aerosol in a way that may be more representative of the likely situation in clinical use. However, the present study, which was scoping in nature, will need to be extended to encompass a variety of other oral inhaler-generated aerosols, in particular, those from DPIs and nebulizers, before its more general applicability to OIP measurements can be confirmed. Furthermore, correlation with whole lung deposition data from imaging studies, similar to the process described by Newman and Chan,(30) would be necessary before the value of this particular AIM-pHRT system can be established for use in developing reliable in vivo–in vitro relationships/correlations.
Conclusions
The AIT slightly reduced the mass of coarser particulate emitted from a salbutamol pMDI entering either full resolution ACI or AIM-pHRT configurations compared with the situation when the compendial Ph.Eur./USP induction port was used. The resulting APSDs were also narrowed when the AIT was present. This behavior is consistent with findings from a previous experimental pMDI-based study with an NGI, in which the effect of inlet change on impactor-measured APSDs was also compared. An AIM-pHRT apparatus based on the reduced ACI, equipped with the same AIT, was observed to provide substantially comparable values of coarse, fine, and extra-fine particle mass to the equivalent measures obtained from benchmark data with the ACI-AIT system. This abbreviated impactor–inlet configuration may therefore be helpful as a rapid-to-use substitute for the full resolution ACI system in studies that are focused more on comparing in vitro data with measures relating to regional deposition in the HRT.
Footnotes
Acknowledgments
The authors would like to acknowledge members of the Cascade Impactor Working Group of the International Pharmaceutical Aerosol Consortium on Regulation and Science (IPAC-RS) for their advice concerning the development and application of the AIM concept outlined in ![]() . A preliminary version of this work was presented in June 2011 as part of a podium talk at the 2011 Congress of the International Society for Aerosols in Medicine (ISAM).
. A preliminary version of this work was presented in June 2011 as part of a podium talk at the 2011 Congress of the International Society for Aerosols in Medicine (ISAM).
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.