
Abstract
Abstract
Background:
Lung cancer is the leading cause of cancer death worldwide. Pulmonary anticancer therapy might offer several advantages over systemic delivery, leading to an increased exposure of the lung tumor to the drug, while minimizing side effects, due to regional containment. Here, we studied if a combination of inhalation therapy and drug targeting holds potential as an even more efficient lung cancer therapy.
Methods:
Transferrin (Tf )-conjugated PEG liposomes loaded with doxorubicin (DOX) were administered using an intracorporeal nebulizing catheter to an orthotopic lung cancer model established in athymic Rowett nude rats. Different DOX formulations and doses (0.2 and 0.4 mg/kg) were tested and the influence on tumor progression and life span of rats was evaluated in comparison with the i.v. administration of Tf–PEG–liposomes loaded with DOX at a therapeutic dose of 2 mg/kg.
Results:
Rats in the untreated control group showed significant weight loss 2 weeks after tumor induction and died between days 19 and 29. Lungs of these animals showed multiple foci of neoplastic deposits, ranging up to 20 mm replacing the entire lobe. Empty Tf–liposomes showed a significant effect on survival time. This might be caused by the secondary cytotoxicity via stimulation of pulmonary macrophages. All animal treated intravenously also perished before the end of the study. No significant (p<0.05) improvement in survival was observed between the groups treated with aerosols of free drug, DOX encapsulated in plain and in Tf-modified liposomes. However, more animals survived in the Tf–liposome groups than in the other treatment regimes, and their lung tissue generally had fewer and smaller tumors. Nevertheless, the size of the groups, and the duration of the trial render it impossible to come to a definite conclusion.
Conclusions:
Drug targeting demonstrated potential for improving the aerosol treatment of lung cancer.
Introduction
The association of anticancer drugs with advanced delivery systems, in particular liposomes, has become a successful strategy to improve the therapeutic effect of these molecules by increasing their concentration at the target site and reduction of systemic toxicity.(3,4) Anthracyclines, such as doxorubicin (DOX), are among the most commonly used drugs for the treatment of both haematological and solid tumors.(5) However, the clinical use of DOX is often limited by the risk of cumulative cardiac toxicity, which may lead to congestive heart failure and death.(6) Liposomal formulations of DOX have shown prolonged systemic circulation times in comparison with the free drug, reduced cardiotoxicity, increased solid tumor accumulation, and increased therapeutic efficacy in many experimental models.(7) Consequently, two different liposomal formulations of DOX have been approved for clinical use, that is, Myocet® and Caelyx® (or Doxil®).
Encouraged by these promising results, liposomal formulations are now being developed for new routes of delivery and with a higher degree of target specificity.(8,9) Among these approaches are target-seeking vesicles that have antibodies or receptor ligands attached directly to the liposome phospholipids headgroups or to the distal end of polyethylene glycol (PEG) chains.(10) Transferrin (Tf ), a glycoprotein responsible for cellular iron absorption, is one such molecule that can be utilized for active targeting.(11) Tf is nonimmunogenic and can be conjugated without losing its biological activity, making it a promising tumor targeting ligand.(12) Previous in vitro studies by us and others have shown that Tf-conjugated, DOX-loaded liposomes showed higher uptake levels and cytotoxicity in lung cancer cells, while they were relatively nontoxic to normal pneumocytes.(13) Other studies using Tf attached to the distal terminal of PEG-chains of sterically stabilized-liposomes have concluded that these systems were able to suppress tumor growth more effectively than PEG-liposomes after i.v. administration into solid tumor-bearing animals.(14) Alternative strategies have used antibodies raised against the transferrin receptor (TfR).(15,16)
Inhalation of therapeutic aerosols is a long established means to deliver drugs topically to the lung or to the systemic circulation.(17) In addition to drug solutions, suspensions, and particulates, liposomal formulations are being developed for aerosol administration.(18,19) Due to their versatility and innoxiousness, liposomes are promising candidates for pulmonary drug delivery that allow delivery of compounds with formulation issues (e.g., lipophilic drugs and sensitive biopharmaceuticals) and to create a drug depot in the lung for sustained release.
Pulmonary anticancer therapy might offer several advantages over systemic delivery, leading to an increased exposure of the lung tumor to the drug, while minimizing side effects, due to regional containment.(2,20) The safety and preferential accumulation of cisplatin in lungs after pulmonary delivery using an intracorporeal nebulizing catheter has been previously reported.(21)
The hypothesis of the present study, hence, was to investigate if a combination of local therapy and drug targeting would result in a more efficient lung cancer therapy, when compared to the corresponding systemic treatment or pulmonary delivery of nonconjugated liposomes.
Tf-conjugated PEG liposomes loaded with DOX were administered using an intracorporeal nebulizing catheter to an orthotopic lung cancer model established in athymic Rowett nude rats. Different DOX formulations and doses (0.2 and 0.4 mg/kg) were tested and the influence on tumor progression and life span of rats was evaluated in comparison with the i.v. administration of Tf–PEG–liposomes loaded with DOX at a therapeutic dose of 2 mg/kg.
Materials and Methods
Materials
Distearoyl-sn-glycero-3-phosphocholine (DSPC), distearoyl-sn-glycero-3-phospho-ethanolamine-N-[methoxy(polyethylene glycol)-2000] (ammonium salt) (DSPE-PEG), and distearoyl-sn-glycero-3-phosphoethanolamine-N-[carboxy(polyethylene glycol)-2000] (ammonium salt) (DSPE-PEG-COOH) were purchased from Avanti Polar Lipids (Alabaster, AL, USA). N-(3-dimethylaminopropyl)-N′-ethylcarbodiimide hydrochloride (EDC) was purchased from Fluka (Dublin, Ireland). N-Hydroxysulfosuccinimide (sulfo-NHS) and the BCA protein assay kit were obtained from Pierce (Rockford, IL, USA). Cholesterol (Chol), human holo-Tf, DOX, and HEPES were obtained from Sigma-Aldrich (Dublin, Ireland). Enrofloxacin, ketamine, and xylazine necessary for the animal experiments were supplied by the Bioresources Unit, Trinity College Dublin. Introcan safety i.v. catheters were obtained from BBraun (Dublin, Ireland).
Encapsulation of DOX into liposomes
The encapsulation of doxorubicin in liposomes was performed by an active loading method according to Abraham et al.(5) with some modifications. Briefly, the relevant lipids, DSPC:Chol:DSPE-PEG:DSPE-PEG-COOH at a molar ratio of 1.85:1:0.132:0.018 were dissolved in chloroform and the organic solvent was removed by rotary evaporation. The formed homogeneous lipid film was hydrated with ammonium sulphate buffer (135 mM, pH 5.4) at 60°C for 30 min. In order to produce a homogeneous liposomal suspension, empty multilamellar liposomes were submitted to extrusion (at 60°C) using a Lipex thermo-barrel extruder (Northern Lipids, Vancouver, BC, Canada), sequentially passing the suspension through polycarbonate membranes Nuclepore (Whatman, Batavia, IL, USA), until an average vesicle size of 0.1 μm was achieved. An ammonium sulphate gradient was created by replacement of the extra liposomal medium with PBS buffer (pH 7.4) using a desalting column (Econo-Pac 10 DG, Bio-Rad, Hercules, CA, USA). A DOX solution (0.5 mg/mL) prepared in phosphate-buffered saline (PBS) was then incubated with the liposomes for 1 h at 60°C at a DOX to lipid molar ratio of 1:3 and 1.45. The nonencapsulated DOX was separated by ultracentrifugation at 250,000×g for 3 h at 15°C in a Beckman LM-80 ultracentrifuge (Beckman Instruments, Fullerton, CA, USA). The pellet was resuspended in PBS (pH 7.4) and Tf was coupled to the liposomes (see below).
Conjugation of Tf to DOX liposomes
The conjugation of Tf to DOX liposomes was achieved by EDC and S-NHS-mediated amide bond formation between the carboxyl groups of DSPE-PEG-COOH and free amine groups of the transferrin molecule.(22) Briefly, to 1 mL of DOX liposomes (lipid concentration: 10 μmol/mL), 1 mL of PBS, 180 μL of S-NHS, and 180 μl of EDC, both freshly prepared at 0.25 M in the relevant buffer (see below) were added. This mixture was allowed to incubate for 10 min at room temperature. Then, 125 μg of Tf per μmol of lipid were added and gently agitated overnight. The unbound protein was separated from the liposomes by ultracentrifugation at 250,000×g for 3 h (15°C) in a Beckman LM-80 ultracentrifuge. To further optimize the procedure, the influence of conjugation buffer on coupling efficiency was studied. PBS (pH 5.9 and 7.4), 2-(N-morpholino)ethanesulfonic acid buffer (MES, pH 5.5), 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid buffer (HEPES, pH 7.4), and citrate buffer (pH 5.0 and 5.9) were compared. The incubation was studied at room temperature and at 4°C.
Physicochemical characterization of liposomes
Liposomes were characterized in terms of mean size, ζ-potential, lipid concentration, DOX content, and Tf conjugation. Liposomal formulations were characterized in terms of mean size and polydispersity index (PdI) by laser light scattering and ζ-potential by laser Doppler electrophoresis using a ZetaSizer, Nano Series (Malvern Instruments, Malvern, UK), after appropriate dilution of the liposomal suspensions in work buffer at 25°C. P.I. ranges from a 0–1 with the higher value representing the highest degree of heterogeneity. The mean size, polydispersity index (PI), and ζ-potential of liposomal formulations was determined using a ZetaSizer, Nano Series (Malvern Instruments, Malvern, UK).
The phospholipid content of liposomal suspensions was performed according to Stewart's assay.(23)
The concentration of encapsulated DOX was quantified by spectrophotometry. Triton X-100 was added to liposomal samples to a final concentration of 1% (v/v). Samples were then placed on a water bath for 30 min at 60°C, before cooling down to room temperature, and measurement in a plate reader (FLUOstar OPTIMA, BMG Labtech, Offenburg, Germany) at 485 nm. Samples were diluted with PBS when necessary.
Tf was quantified using a Bio-Rad protein assay based on the method of Bradford. A calibration curve was prepared using a standard BSA stock solution of 2.0 mg/mL. The standards ranged from 0.5 to 5 μg/well. Liposomes containing Tf were diluted and adjusted to the standard curve range. The absorbance was measured at 595 nm in a plate reader (FLUOstar OPTIMA, BMG Labtech, Offenburg, Germany).
Atomic force microscopy
The liposomal formulation was diluted in ultrapure water (MilliQ, 18.4 MΩ, pH 5.5). Not later than 1 h after preparation, the liposomes were directly transferred onto a silicon chip by dipping it into the liposome suspension. Atomic force microscopy was performed on a Digital Nanoscope IV Bioscope (Veeco Instruments, Santa Barbara, CA, USA). The microscope was vibration-damped. Commercial pyramidal Si3N4 tips (NCH-W, Veeco Instruments) on a cantilever with a length of 125 μm, a resonance frequency of about 220 kHz, and a nominal force constant of 36 N/m were used. All measurements were performed in tapping mode to avoid damage of the sample surface. The scan speed was proportional to the scan size and the scan frequency was between 0.5 and 1.5 Hz. Images were obtained by displaying the amplitude signal of the cantilever in the trace direction, and the height signal in the retrace direction, both signals being simultaneously recorded. The results were visualized either in height or in amplitude mode.
Cell culture
Human large cell lung cancer H460 carcinoma cells (ATCC HTB-177) were obtained from LGC Promochem (Teddington, UK). Cells were grown in RPMI 1640 medium supplemented with 10% foetal bovine serum. Cells to be implanted were washed twice with RPMI 1640 medium, counted in a haemocytometer, and adjusted to a final concentration of 106 cells/100 μL of the RPMI 1640 medium for intratracheal administration (see below).
Animal studies
The study protocol was approved by the Ethics Committee, Trinity College Dublin. Female athymic Rowett nude (rnu) rats (8–10 weeks old) were obtained from Charles River Laboratories (Wilmington, DE, USA). Rats were kept in sterilized cages and fed autoclaved food and water ad libitum. Enrofloxacin was added to the drinking water at a concentration of 0.64 mg/mL. All manipulations were done under sterile conditions in a laminar flow cabinet.
Tumor induction
On the day of inoculation, rats were irradiated with 500 rads from a gamma source. Three hours postirradiation, rats were anesthetized by i.p. administration of a ketamine/xylazine mixture (75 and 10 mg/kg, respectively). Then animals were placed in a work stand for holding them during intubation (Hallowell EMC) and semisuspended by a ribbon hooked around the upper incisors. The animals' mouth was opened with the aid of a cotton tip and the tongue pushed to one side. The vocal cords were visualized by inserting the otoscope into the oral cavity. Under direct vision of the upper ways a guide wire was introduced through the vocal cords via the inside of the otoscope cone through the mouth while the vocal cords are visualized. After ensuring that the guide wire was correctly positioned, a 14-gauge i.v. catheter (BBraun, Ireland) was passed over it. Then the guide wire was carefully removed and the catheter placed in the trachea. The correct intubation was checked with the help of a mirror. The intubated rats received the tum
Treatment schedule and doses
Treatment started 1 week after tum
Monitoring rat growth
Rats were examined daily for signs of morbidity. Morbid rats were terminally anesthetized with pentobarbital (300 mg/kg i.p.). Beginning from the day of implantation, the animals were weighed weekly until sacrifice.
Histopathology
To characterize the growth and metastatic pattern of each tumor, the lungs, spleen, heart, liver, and kidneys were removed from the euthanized animals. The lungs were fixed by tracheal perfusion with 20 mL of 20% buffered formalin. All tissue was weighed and then placed in 10% formalin for at least 48 h. Tissues were then embedded in paraffin, stained with H&E, and examined in a blinded fashion by a registered pathologist (A.R.).
Statistics
In vitro data were analyzed by a two-way analysis of variance (ANOVA) with Bonferroni's post hoc analysis or one-way ANOVA and t-test. A two group analysis of survival was performed using the on-line tool available from the Dartmouth-Hitchcock Norris Cotton Cancer Center (http://biostat.hitchcock.org/BSR/Analytics/CompareTwoSurvivalDistributions.asp) The significance level used was p<0.05.
Results
Optimization of the liposomal delivery systems
Transferrin-modified liposomes for the delivery of doxorubicin have been previously described by us and others.(13,24,25) In a set of initial studies, an attempt was made to further optimize the liposomes with regards to doxorubicin encapsulation and transferrin surface conjugation.
Doxorubicin was encapsulated into liposomes at molar ratios of 1:3 and 1:4.5 DOX:lipid. Liposomes with a mean diameter of 0.13 μm were prepared, and although higher encapsulation efficiency was obtained with a molar ratio of 1:4.5, higher loading capacity was achieved for the initial molar ratio of 1:3 (data not shown).
Next, the influence that buffer composition, pH, and incubation conditions have on the transferrin coupling efficiency was studied. The concentration of Tf/lipid obtained after the conjugation reaction and the corresponding coupling efficiency are shown in Table 2. Surface modification of liposomes with transferrin at 4°C using PBS pH 7.4 or citrate buffer pH 5.9 resulted in almost complete conjugation with an efficiency of 98% in each case. As doxorubicin has a pKa of 8.15, it was concluded to use PBS (pH 7.4) for the coupling reaction as well as loading of DOX liposomes via an ammonium sulphate gradient between the internal aqueous compartment and external medium of liposomes.(26)
The obtained results correspond to mean±SD of three independent samples.
(DOX/lipid)I, initial concentration doxorubicin/lipid; (DOX/lipid)f, final concentration doxorubicin/lipid; E.E., encapsulation efficiency; C.E., coupling efficiency; NA, not applicable.
Physicochemical characterization of liposomes used in the in vivo studies
In the in vivo studies different liposomal formulations were compared: nontransferrin modified DOX liposomes (i.t.), DOX liposomes with Tf attached to their surface (i.t. and i.v.) and empty Tf-liposomes (i.t.). Table 1 summarizes the physicochemical properties of all liposomal formulations. Liposomes generally had mean diameter sizes ranging from 0.13 to 0.15 μm and slightly negative surface charges. Surface modification by transferrin was decreased when liposomes were loaded with DOX. Doxorubicin encapsulation efficiency, on the other hand, was not affected by the presence of transferrin and always in the region of 70%.
Data are shown as mean±SD of three independent samples.
Atomic force microscopy was used to visualize the liposomes and to confirm the particle size and morphology measurements performed by PCS. Liposomes were approximately 0.13 μm in diameter and small globular structures, localized on the liposomal surface became visible (Fig. 1). These particles had a size of around 3 nm. From the molecular weight, the size of a single Tf molecule can be calculated to be in a similar size range.(27)
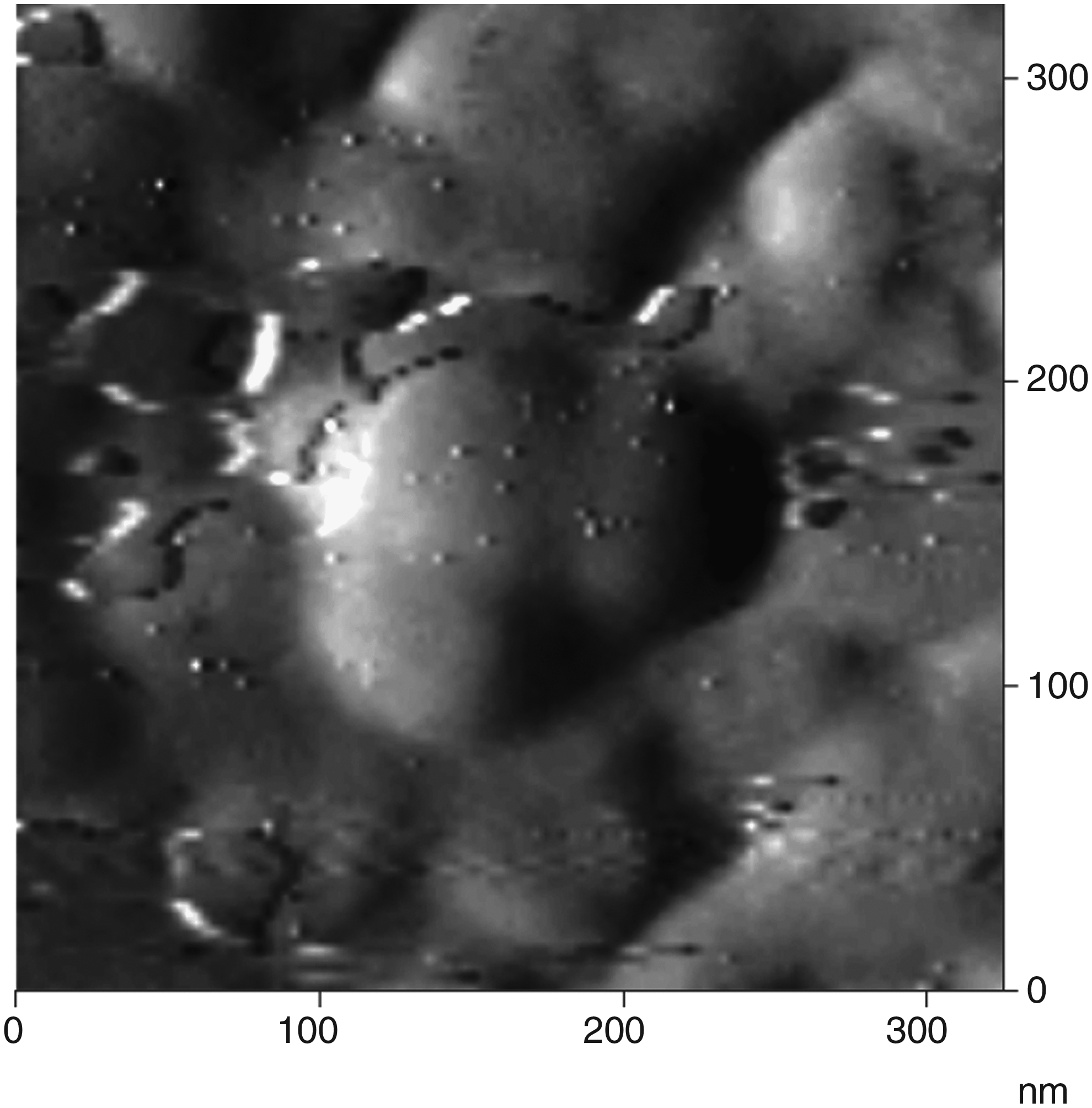
Representative AFM image of transferrin-conjugated doxorubicin liposomes. Small globular structures are visible at the surface, corresponding in size with individual transferrin molecules.
Therapeutic effect of doxorubicin liposomes in an orthotopic model of human lung cancer in rnu rats
The therapeutic effect of the different therapies was assessed by measurement of the rats' body weight, survival time, organ weight, and histopathological studies. Generally, body weight and survival time were closely correlated (Figs. 2 and 3). The orthotopic model of NCI-H460 human nonsmall cell lung cancer (NSCLC) in rnu rats has been reported to have a 100% take-rate.(28) After endobronchial implantation with cancer cells, rats were left to rest, before receiving treatment with the relevant formulations on days 7 and 14 postinoculation.
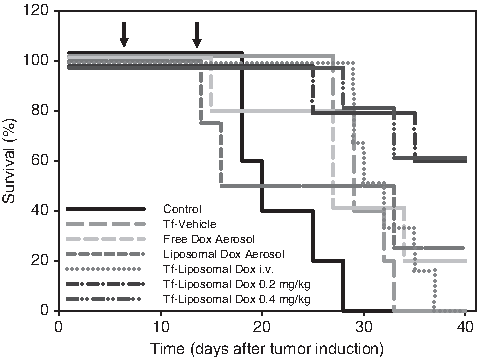
Survival time of rnu rats after intratracheal instillation of 106 NCI-H460 human large-cell lung carcinoma cells. The arrows indicate time points when the respective treatment was administered. A dose of 0.4 mg/kg doxorubicin was administered, except for the i.v. group (2 mg/kg) and one group of animals receiving Tf-modified DOX-loaded liposome aerosols (0.2 mg/kg). Data represent mean±SD, n=4–6.
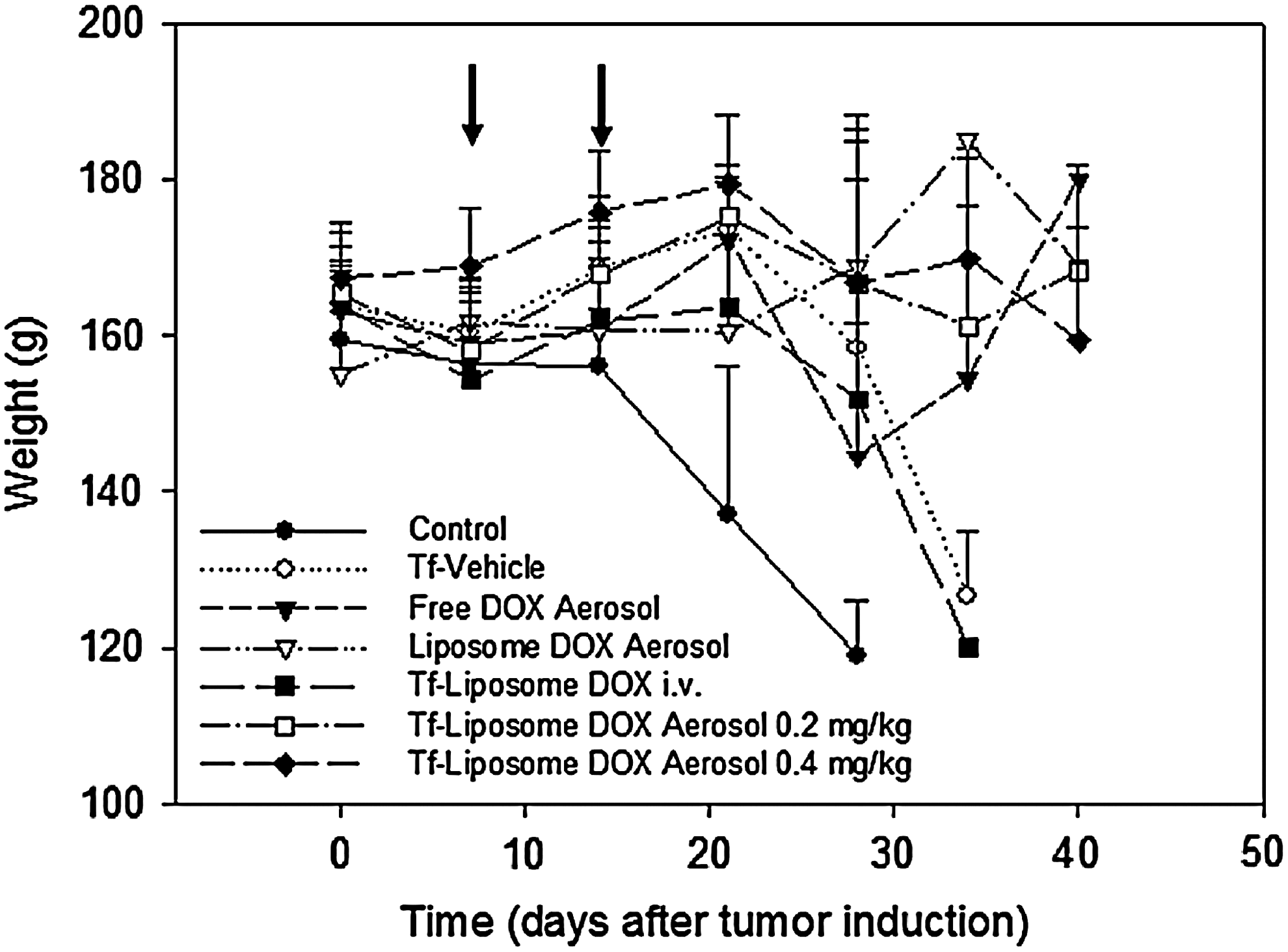
Body weight development of rnu rats after intratracheal instillation of 106 NCI-H460 human large-cell lung carcinoma cells. The arrows indicate time points when the respective treatment was administered. A dose of 0.4 mg/kg doxorubicin was administered, except for the i.v. group (2 mg/kg) and one group of animals receiving Tf-modified DOX-loaded liposome aerosols (0.2. mg/kg). Data represent mean±SD, n=4–6.
Rats in the untreated control group showed no weight gain in the first 2 weeks after implantation, suggesting that the disease process had begun to reduce the animals' growth rate. After 2 weeks, this group showed significant weight loss, indicating cachexia. All rats in the untreated control group died or were sacrificed between days 19 and 29 after tumor inoculation (Fig. 2). Lungs of these animals showed multiple foci of neoplastic deposits, ranging in size from small clusters of cells to large coalesced tumors with maximum diameters up to 20 mm replacing the entire lobe after 19–29 days (Fig. 4A). The large tumors showed central necrosis and scattered inflammatory infiltrates, associated with the lesion. Lymphovascular permeation was present in some lobes. The surrounding lung tissue showed hyperemia, edema, and focal interstitial inflammatory infiltrates, and in one case foci of bronchopneumonia. Tumor growth was also evident by analyzing the lung weight as a percentage of the rats' body weight (Fig. 5). Lung weight was increased in implanted animals, when compared to healthy litter mates. Changes in other organ weights measured, that is, spleen, liver, kidneys, and heart; however, were not significant (data not shown).
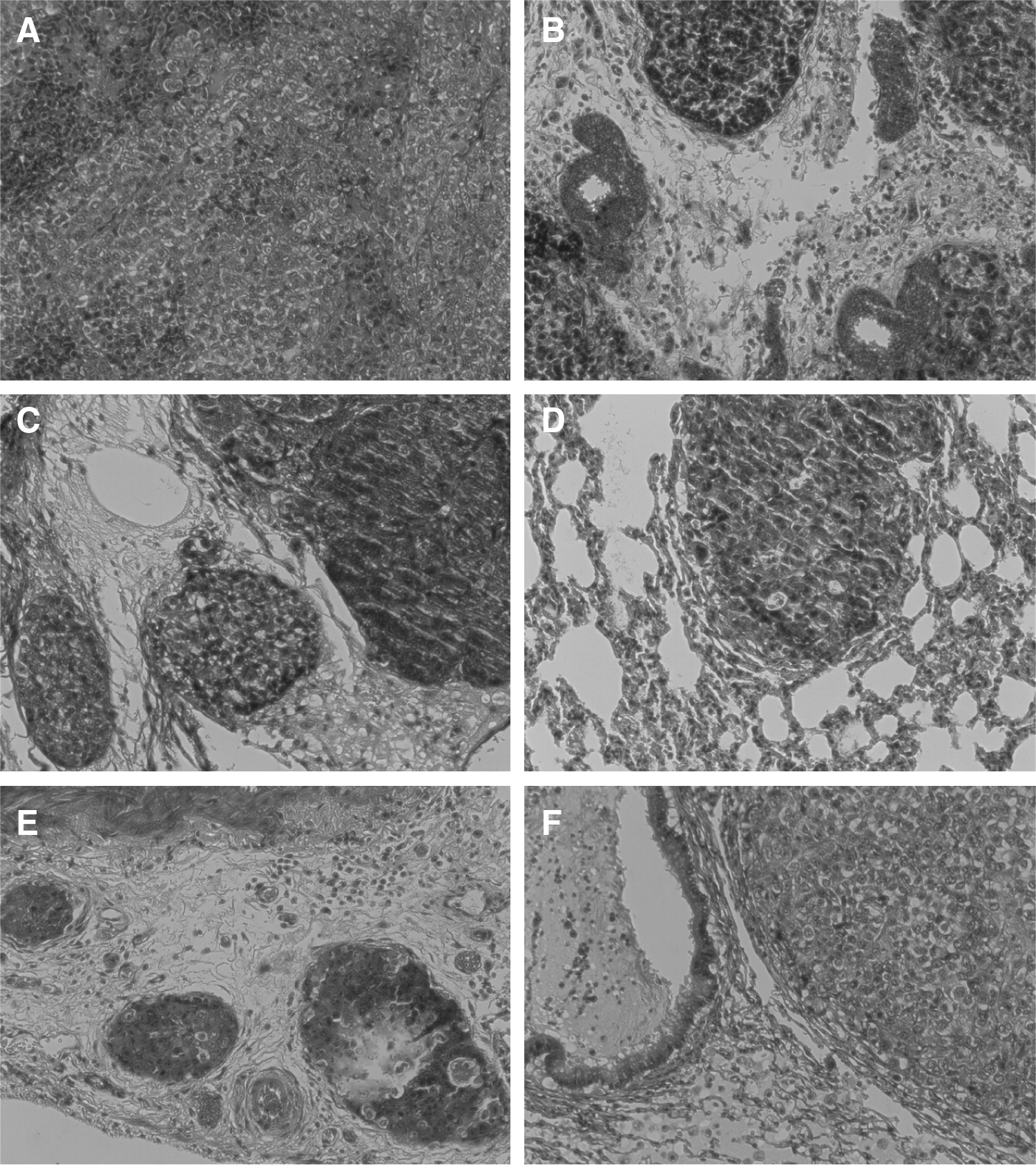
Representative lung tissue section stained with H&E of rnu rats after intratracheal instillation of 106 NCI-H460 human large-cell lung carcinoma cells. (
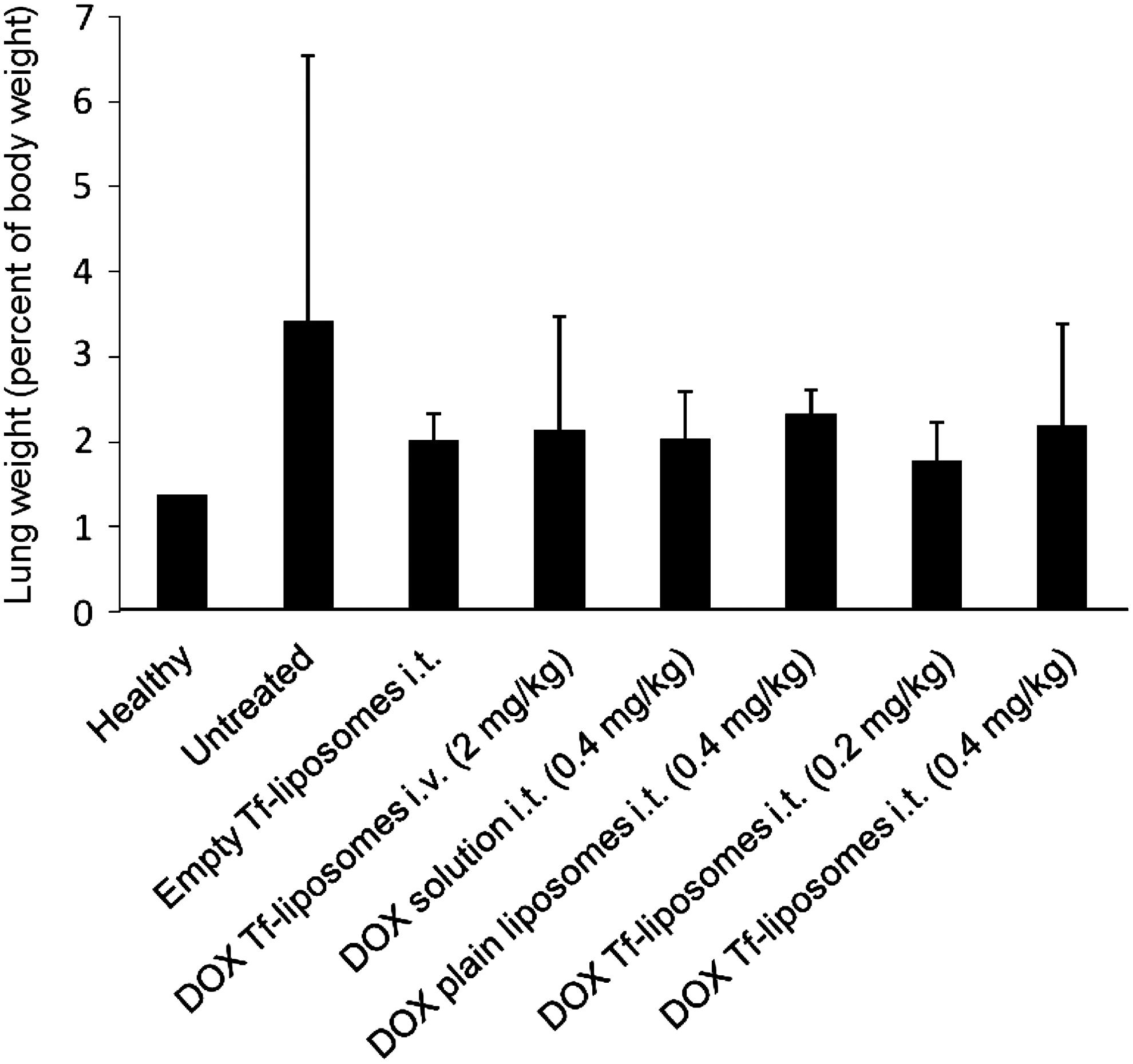
Lung weight of rnu rats shown as percentage of the corresponding body weight measured at time of death. Animals were instilled 106 NCI-H460 human large-cell lung carcinoma cells and then treated as indicated. Data represent mean±SD, n=4–6.
Intriguingly, animals administered the empty Tf-liposome aerosol had a significant (p=0.026) longer survival time than the untreated control group and their lung weight was also reduced. Sections from lungs of these animals contained multiple foci of neoplastic cells, some growing in nests, and some in papillary pattern showing degenerative changes. Aggregates of foamy macrophages were present in some of the alveolar spaces. The maximal diameter of tumors was approximately 10 mm (Fig. 4B).
Treating the rats with 2 mg/kg doxorubicin i.v. encapsulated into Tf–liposomes further increased their survival. The lung tissue contained scattered small aggregates of neoplastic cells with maximum dimension up to 2.5 mm with focal central comedo-type necrosis (Fig. 4C). Small neoplastic thrombi were present in lymphovascular spaces as well as scattered patchy foci of inflammatory infiltrates in subpleural areas.
When DOX solution was directly nebulized into the lungs at 0.4 mg/kg the survival time was further extended, and one animal was still alive when the study was terminated after 41 days. The lung tissue of two rats showed focal hyperemia and edema, but no evidence of neoplastic tumors. The other lungs contained multiple small nests and foci of neoplastic cells with focal central necrosis (Fig. 4D). These tumors had maximal diameters of 12 mm.
In the group treated intrapulmonary with DOX encapsulated into nonmodified liposomes, one animal was virtually free of cancer and another one presented with only one tiny focus of neoplastic cells. Lung tissue of the other two animals showed scattered foci of neoplastic cells with maximum dimensions of 5 mm and central necrosis (Fig. 4E). Lymphovascular permeation was also noted. At the end of the study (day 41), one animal from this group was still alive.
Animals receiving the Tf-modified liposomes had the highest rate of survival; three of the five rats were still alive with no signs of cachexia. There was no statistically significant difference in any of the parameters studied between the two concentrations (i.e., 0.2 mg/kg and 0.4 mg/kg) of aerosolized Tf-conjugated liposomes. Lungs of one of the rats were free of neoplastic disease. Focal foamy macrophages were present in alveolar spaces as well as hyperemia in the interstitium. The other tissues showed patchy scattered tiny foci of neoplastic tumors, ranging in size up to 8 mm. Some of the neoplastic deposits showed central necrosis and associated inflammatory infiltrates. Lymphovascular space permeation was observed. There was also hyperemia, edema, foamy macrophages and peribronchial inflammatory infiltrates present (Fig. 4F).
Of note, due to the termination of the study after 41 days and the comparatively small number of animals per group, no statistical significance was obtained when comparing the DOX-loaded Tf-modified liposomes to the DOX-loaded plain liposomes (p=0.21 and 0.25 for the 0.2 mg/kg and 0.4 mg/kg dose, respectively).
Discussion
It was the aim of this study to investigate, if active drug targeting via transferrin receptor-mediated uptake, can further improve the therapeutic efficiency of localized treatment of lung cancer. An orthotopic human nonsmall-cell lung cancer model in athymic Rowett nude rats was used for this purpose, as we believe as it has a number of advantages over similar experimental models in mice.(28) In the rat model the primary tumors begin within the bronchus, where the majority of lung cancers normally originate. Moreover, there is no intentional injury to the lung and the 10-fold larger animal size allows the use of an intratracheal nebulization catheter for localized pulmonary delivery.
Evidence is mounting that local delivery of anticancer drugs to tumor lesions in the lung has several advantages over systemic treatment, such as higher local doses and lower systemic concentrations.(2,20) There are, however, issues with this approach that need to be considered. Examples are the specific pulmonary toxicity of some chemotherapeutics (e.g., irinotecan, gemcitabine, paclitaxel, and docetaxel), the increased risk of iatrogenic lung disease, the fact that deposition might not match the location of tumor, poor tumor penetration, and obviously the occupational exposure of healthcare workers or family members.(29)
Advanced drug delivery systems such as liposomes and nanoparticles might help to solve some of these issues, and several have been described for pulmonary administration.(30–33) Among the advantages of (mainly colloidal) drug delivery systems are that they can be designed to encapsulate almost any payload, including those with inherent solubility or stability issues.(18,34) In addition, these carriers are relatively easy to modify with targeting structures.(10) Last, there are a number of intrinsic properties of colloidal drug delivery systems that can be exploited in the context of anticancer therapy. Due to their size they often have stealth properties,(35.36) posses the ability to penetrate mucus,(37) an often underestimated barrier in pulmonary delivery, and some have been described to attenuate drug efflux pump function,(36) a major obstacle in chemotherapy, as many cytostatics are substrates of ABC transporters such as P-glycoprotein.
The results of our study are consistent with previous data, confirming that pulmonary anticancer therapy offers the same efficiency as systemic administration, but at lower doses. Tf-conjugation was chosen as our method to achieve active targeting of the liposomes to the tumor. Tf receptors are abundant in many cancerous tissues, and previous studies have shown that Tf-conjugated DOX-loaded liposomes led to an increased intracellular accumulation of DOX and enhanced cytotoxicity in human pulmonary cancer cell lines.(13,24,25) Suzuki and coworkers have demonstrated that the i.v. administration of oxaliplatin encapsulated in Tf–PEG–liposomes suppressed tumor growth more effectively in comparison to nontargeted PEG–liposomes and free oxaliplatin in a murine model of colon tumor.(14) In our study, however, no significant improvement in survival was observed between the groups treated with free drug, doxorubicin encapsulated in plain and in Tf-modified liposomes. More animals survived in the Tf-liposome groups than in the other treatment regimes and their lung tissue generally had fewer and smaller tumors. The size of the groups, however, was too small and the duration of the trial too short to come to a definite conclusion.
It also cannot definitely be ruled out that endogenous Tf competed with liposomal-bound protein for uptake by the TfR, resulting in a decreased efficiency of the treatment. This could have been overcome by using monoclonal antibodies against TfR as target-seeking moieties.(15,16)
A somewhat surprising finding was that empty Tf-liposomes showed a significant effect on survival time. This might be caused by the secondary cytotoxicity phenomenon recently described by Al-Hallak and coworkers(39) in the case of polymeric nanoparticles. It can also be the result of the higher Tf density on the surface of the empty Tf–liposomes, which might have reacted to a higher degree with TfR on tumor cells.
Footnotes
Acknowledgments
This work was supported by a Proof-of-Concept grant (PC/2007/081) from Enterprise Ireland and a Strategic Research Cluster grant (07/SRC/B1154) from Science Foundation Ireland under the National Development Plan cofunded by EU Structural Funds and Science Foundation Ireland.
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.