
Abstract
Abstract
Background:
Metered-dose inhalers (MDIs) have become a firsthand therapeutic strategy for the management of respiratory diseases, mainly for chronic obstructive pulmonary disease (COPD) and asthma. It has been determined, however, that patients do not always use these devices correctly. Our primary goal was to establish the level of technical knowledge of patients with COPD and/or asthma on the use of MDIs, as well as other associated factors related to the effective use of this delivery method.
Methodology:
This study was performed with 191 patients (49.2% male, 50.8% female) diagnosed with COPD and/or asthma at Hospital Universitario Mayor (Bogotá, Colombia). The agreement between different observers on nine aspects of the use of the inhaler was assessed by testing the unweighted kappa correlation coefficient and its significance. The correlations between demographic variables, risk factors, and proper knowledge of the adequate use of inhalers were established by means of the Pearson chi-square test (also called Fisher exact test) (expected values less than 5). Statistical tests were evaluated at a significance level equivalent to 5% (p<0.05).
Results and Conclusions:
The study detected deficiencies in educational factors, specifically regarding the initial contact with the patient and regular follow-up by the team of health professionals. It also showed insufficient strategies for the training of patients in the use of the inhalers. There were no significant differences by gender (p>0.05) in the implementation of the various aspects of the proper use sequence for MDIs. However, there were significant differences related to education levels, socioeconomic status, age, and current occupation. A worse inhaler technique was associated with lower education level (0.034), higher age (p=0.003), and absence of job (p=0.005). Changes in the education of patients on the issue, together with the use of the spacer/valved holding chamber proved to be valid strategies that, with the support of the patients' health-care team, were able to improve the MDI technique of the studied group.
Introduction
One of the most widely used systems for inhaled drugs is the metered-dose inhaler (MDI).(2) The MDI's most useful characteristics are that it is portable, small, and easy to use, that it can deliver multiple exactly metered doses, and that it has a rapid effect, all of which make it ideal for the treatment of lung diseases such as chronic obstructive pulmonary disease (COPD) and asthma.(3,4)
The success of an inhaled therapy depends on the proper use of the device, which can significantly influence the amount of drug that is deposited in the lower airway. Deposition can be enhanced with a slow, deep breath, coordinated with the activation of the MDI, and by holding one's breath for at least 10 sec after inhaling.(5,6) However, MDIs are poorly used; only 43% of the patients carry out all of the steps correctly.(7) Melani et al. reported that nearly 20% of the patients were making mistakes in the use of MDIs; this compromises the effectiveness of the dose.(3)
The main problems in the use of MDIs are coordination between shot and inhalation,(8) failing to hold one's breath, inhaling too fast, and failing to shake the device properly before use.(9) Other problems include the patient's inclination to stop breathing when the spray makes contact with the oropharynx, activating the inhaler at the end of the inspiration or activating it repeatedly in a single respiratory effort, and inhaling through the nose.(10–12) These mistakes can be associated with cognitive mental status, emotional problems, old age, grip strength, level of education,(13) and the lack of group support.(11,14,15)
Furthermore, we noted that health professionals have a lack of skills in the use of MDIs, perhaps due to inadequate training in this specific treatment method. Physicians prescribe MDIs, but they very often fail to teach the proper use of the device to their patients, thus harming the desired results.(16,17) In addition, the patients are not aware of the importance of the technique and of its role in granting them the benefits of their medication. Patients need to know the nature of their illness, but also the benefits, side effects, dosage, mode of administration, and correct use of MDIs. The proper use of MDIs can be achieved through monitoring the patients and giving them feedback,(5) taking into account their particular circumstances and backgrounds, and the characteristics of MDIs.(6,7)
The strategies to improve the efficiency of MDIs include the use of a spacer or holding chamber.(9,18) Correct usage of MDIs increases to 55% if they are used with a spacer.(7) Another strategy to reduce frequent mistakes in the use of MDIs is education. The education on the proper use of MDIs and its monitoring have a positive effect, increasing the percentage of patients making no mistakes to 63% when using just the MDI.(7) Clavel et al. showed that almost 20% of the French Cystic Fibrosis Care Centers did not include education for aerosol therapy, and that the technique was monitored less than once a year or never in 22% of those centers.(19)
Inadequate use of MDIs has an impact on the quality of life of patients with respiratory diseases like COPD and asthma, and increases the costs for health systems as the management of the disease is poor.(20) Better controlled asthma patients use fewer resources when they know how to use inhalers as a strategy for self-management of the disease.(21) It is clear that a correct technique in the use of MDIs is crucial for the effectiveness of the medication, and that there are a number of factors involved in this. The primary goal of this study was to establish the level of technical knowledge presented by patients, and some other factors related to the effective use of MDIs by patients with COPD and/or asthma, in a university hospital of the Social Health System in Bogotá, Colombia. The study was approved by the Research Committee of the Universidad del Rosario and by the Hospital Universitario Mayor.
Materials and Methods
Subjects
The sample was estimated based on the study “Comprehensive management program for COPD patients from EPS SANITAS,” which showed 68.6% prevalence in the improper use of MDIs, with a precision of 5% and a reliability of 95%. The minimum sample size was thus determined to be 191 patients. The subjects were selected sequentially, over a period of 4 months at the Corporacion Hospitalaria Juan Ciudad Mederi–Hospital Universitario Mayor (HUM).
Some of the inclusion criteria were that the patients: (1) were either being hospitalized with a primary diagnosis of COPD and/or asthma or were pulmonology outpatients, diagnosed with COPD and/or asthma; (2) had a prescription for MDIs; (3) had the ability to answer to the interview; and (4) used MDIs on their own, were over 18 years of age, and agreed to participate in the study.
The patients were admitted into hospitalization in the emergency department due to an exacerbation of COPD or asthma and were surveyed once they were stable without signs of respiratory distress, within 24 to 48 hr after their admission to inpatient services. The severity of the disease was evaluated with the Modified Medical Research Council Dyspnea Scale,(22) as well as with symptoms like cough and sputum production. Patients with altered states of consciousness and those that did not adequately answer the survey or presented inconsistencies in the answers were excluded.
Data collection
We had two types of instruments. The first one is a structured questionnaire aimed at the patients. The first part of this questionnaire included questions on demographic characteristics of the subject, such as age, gender, educational level, and occupation, as well as other questions aimed to identify risk factors for lung disease symptoms. In the second part, the questions assessed the patients' degree of knowledge on the proper use of MDIs, as well as how long they had used it, the MDI drugs that had been prescribed to them, their dosage and schedule, whether they had been given instructions, how these had been given, and who had given them (Fig. 1). The assessment form was adapted from the one used in the study by Durán and Vargas.(23) The modified questionnaire was revised and validated by respiratory medicine specialists from the HUM.
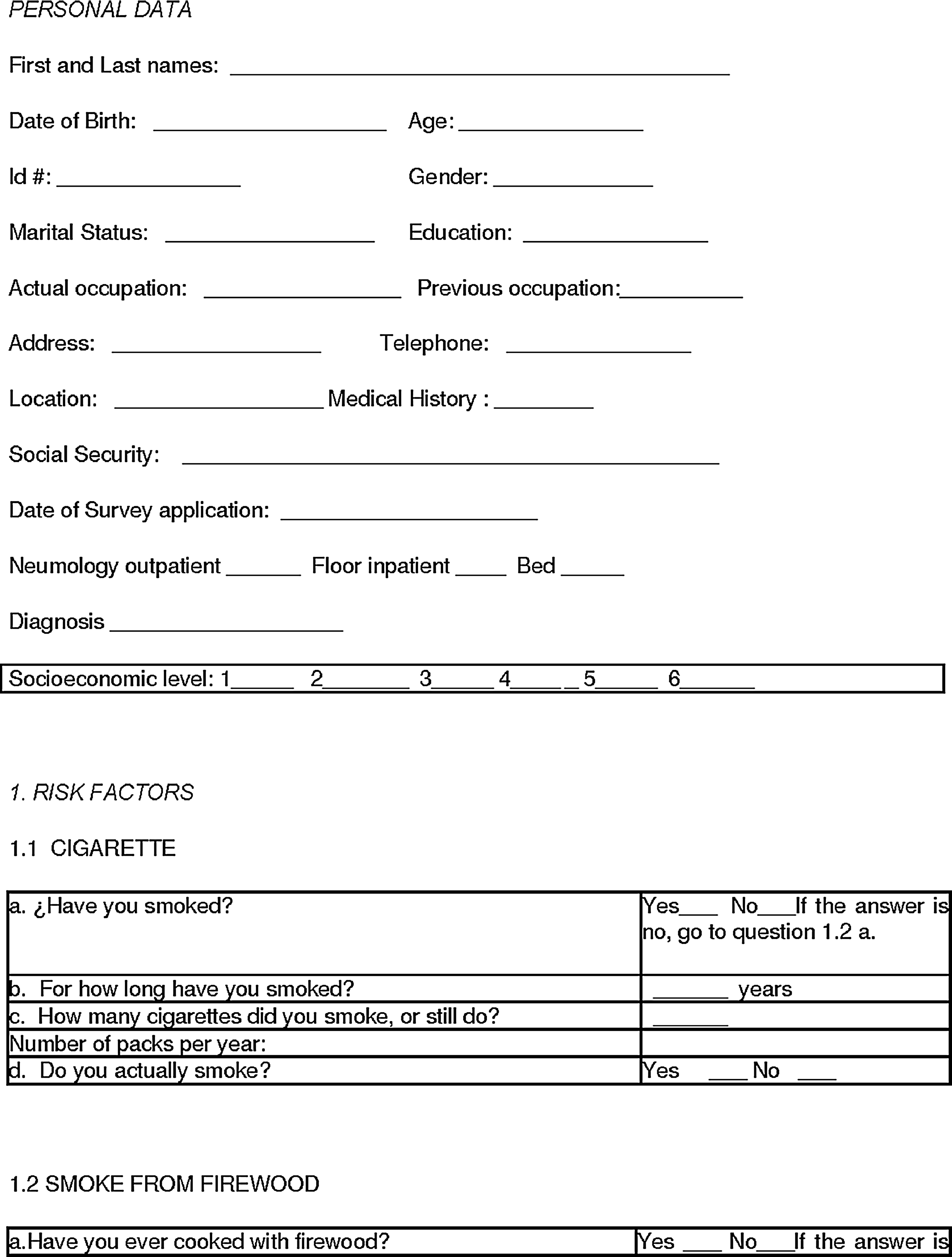
Survey for patients who use MDIs.
The other instrument consisted of an evaluation of the patients' use of an MDI, comparing it with the process for the proper use of MDIs determined by literature.(5,6,24–27) This evaluation was done through observation; the patient was requested to do an inhalation according to his usual method while the evaluator observed and determined whether the different steps were correctly carried out and recorded it in the assessment format. No feedback or corrections were given before or during the evaluation, but such was done at the end of the process if a mistake had been detected in the use of the MDI. To reduce the classification bias in the observation of the technique, the evaluation was conducted simultaneously by two evaluators who recorded each observation separately.
The evaluation form was previously applied to a group of 95 patients as a pilot in the Simón Bolívar Hospital. With this background, we made some adjustments to the structured questionnaire for the patients in order to continue to the next phase of implementation in the HUM. Before collecting data, the researchers did a workshop with the evaluators to review how to contact, interview, and assess the subjects included in the study. The workshop reviewed the steps for the use of MDIs, the use of spacer devices, and each of the questions in the interview. The data collection process was supervised and supported by researchers approved by the Research Committee of the Universidad del Rosario and the Hospital Universitario Mayor.
Data analysis
The descriptive analysis of the categorical variables was performed using absolute and relative frequency distributions expressed as percentages. Quantitative variables were studied by means of central tendency measures and dispersion measures. The agreement between different evaluators in the observation of the nine aspects for the proper use of the inhaler was assessed through the unweighted kappa coefficient and its test of significance.
The correlation between demographic variables, risk factors, and knowledge of the proper use of inhalers was estimated using the chi-square Pearson test (also called Fisher exact test) (expected values less than 5). The data significance level of the statistical analysis was 5% (p<0.05).
Results
Demographics
The study group consisted of 191 patients diagnosed with COPD (86.9%) or asthma (13.1%), with ages ranging between 18 and 95 years, with an average of 69.6±13.5 years and a median of 72 years; the most common marital status was married, followed by widowed and cohabiting. The predominant educational level was elementary education, followed by secondary education. The most frequent occupations were “stay-at-home people” and “currently unemployed,” followed by occupations such as unskilled workers and operators. Other occupations were present with frequencies of less than 10%. The socioeconomic level varied from I to IV (in Colombia, the socioeconomic level is ranked on a scale from I to VI, and each level is called a stratum), with more than 90% for strata I and II (Table 1).
Risk factors and symptoms
Smoking was present as a risk factor in 51.3% of the studied population, and 51.8% of the studied patients had cooked with wood stoves. In work-related activities, 41.4% of the patients had been continuously exposed to mineral particles, chemicals, and/or organic particles. According to the Medical Research Council, the group of patients reported dyspnea at the following levels: 5/5 (19.8%), 4/5 (15.2%), and 3/5 (5.8%). 97.9 percent of the patients had been hospitalized due to lung disease within the last year; the average number of hospitalizations was 1.62±0.93, with a median of one time.
Treatment
The percentage of patients who had received treatment with MDIs before admission was 97.9%: 57.0% of them had been using MDIs for more than 3 years, 17.7% between 1 and 3 years, and 19.9% from 1 to 6 months. The most widely known drugs used with the MDIs among the patients were ipratropium bromide (76.6%), salbutamol (68.1%), and beclomethasone (64.9%).
Training
98.4 percent of the patients reported that they had received information about MDIs, 98.9% had been told how to use MDIs, and 84.6% recalled the information they had received. In most of the cases, it was a physician who had provided the training (69.6% of the cases); a nurse had given it in 36.6% of the cases, and a therapist in 15.7%.
96.3 percent of the patients had been shown how to use MDIs, but only 11.0% of them had been given written instructions. 24.1 percent of the patients had been asked again about their usage of MDIs. 44.5 percent had been informed whether or not to use a spacer or valved holding chamber. 84.7 percent of the patients to whom the use of a spacer/valved holding chamber had been prescribed had been taught to use it. Currently, 50% of the patients used a spacer/valved holding chamber, but at the moment of the evaluation only 13.6% had a spacer/valved holding chamber with them. This situation prevented us from objectively comparing the technique with and without a spacer or valved holding chamber.
Only one patient correctly followed the steps for the use of MDIs. The aspects that were most commonly omitted in the use of MDIs were “take a deep breath,” “exhale all the air from the lungs,” and “hold the air for 10 sec” (Table 2).
Concerning the instruction “exhale all the air from the lungs,” significant differences were found based on educational level, with better performance by patients with a higher education level (none: 33.3%; elementary: 33.6%; secondary: 51.4%; and university: 64.7%; p=0.034, chi-square test without correction). The completion of the step “shake the inhaler for more than 15 sec” also increased with the patient's educational level, nearly showing significant differences (p=0.06, exact likelihood ratio). The accomplishment of the step “place the inhaler in the mouth” was significantly better in patients of lower socioeconomic status (100% vs. 89.8%; p=0.001, exact likelihood ratio), and the compliance to “press the inhaler button once” also showed significant differences (96.1% vs. 89.8%; p=0.074, chi-square test without correction) (Table 3).
The patients showed significant differences in “exhale all the air from the lungs” based on the current occupation variable; those who have a labor activity tended to follow this instruction better, as compared with stay-at-home patients and unemployed patients (65.6%, 34.4%, and 34.9%, respectively; p=0.005, chi-square test without correction). The group had a similar behavior toward the steps “take a deep breath” (56.3%, 27.1%, 30.2%, respectively; p=0.008, chi-square test without correction) and “hold the air for 10 sec” (71.9%, 49.0%, 39.7%, respectively; p=0.012, chi-square test without correction). Significant differences were also found based on previous occupation on the fulfillment of the steps “exhale all the air from the lungs” (p=0.015, exact likelihood ratio) and “place the MDI in the mouth” (p=0.018, exact likelihood ratio); patients who were professionals were found to present a higher compliance with these steps when compared with those from other occupations; the instruction “press the inhaler once” was also close to showing significant differences toward this same behavior (p=0.052, exact likelihood ratio).
Significant differences were found among age groups concerning the instructions “exhale all the air from the lungs” (p<0.001, uncorrected chi-square), “take a deep breath” (p=0.013, chi-square test without correction), “hold the air for 10 sec” (p<0.001, chi-square test without correction), and “shake the inhaler for more than 15 sec” (p=0.008, chi-square test without correction), with greater frequency of compliance in younger patients, specifically in those under 60 years of age. Regarding age and the question “have you been asked again how you are using MDIs?” there are major differences in younger patients (p=0.003, chi-square test without correction).
Patients with higher socioeconomic status showed differences in the use of spacer/valved holding chambers (p=0.039, chi-square test without correction) and regarding the question “have you been taught how to use a spacer/valved holding chamber?” (93.0% vs. 76.2%; p=0.031, chi-square test without correction). Training in the use of the spacer/valved holding chamber showed significant differences among educational levels (p=0.006, exact likelihood ratio).
There were no significant differences by gender (p>0.05) in the compliance with the steps for the proper use of MDIs. No significant differences were found in training on the use of inhalers based on current occupation (p=0.003, exact likelihood ratio), neither were there any significant differences based on this categorization regarding whether the subjects had been handed written instructions for the use of MDIs (p=0.057, exact likelihood ratio) nor concerning the question “have you been asked again how you are using MDIs?” (p=0.043, chi-square test without correction). The proper technique for the use of inhalers had been most frequently given by the patient's physician (p<0.001, exact likelihood ratio).
Significant correlation was found among evaluators, as all items showed an observed concordance above 75%. Items with the most agreement were “if you use more than one puff, wait at least 1 min for the next puff” (89.7%) and “shake the inhaler” (88.7%). Items with the lowest percentages were “once you press the inhaler, take a deep breath immediately” (75.8%) and “hold the air for at least 10 sec” (76.7%) (Table 4). These results show that the steps in which most patients fail to perform the technique properly are also the ones in which the observations of the evaluators disagree most often.
Because only one patient was correctly following all the steps in the use of MDIs, it was not deemed appropriate to use logistic regression models to explain the proper use or misuse of MDIs.
Discussion
MDIs have become a therapeutic strategy for the management of respiratory diseases, but it has been determined that these devices are not always used in the most appropriate way by the patients. This study found deficiencies in the use of the spacer/valved holding chamber and in the educational component regarding the initial contact and monitoring by the health team. The results show that the use of educational strategies such as the delivery of written material, a periodic review of the technique, talks, and workshops has been insufficient.
In the implementation of the various aspects of the sequence for the proper use of MDIs, there were no significant differences by gender. There were, on the other hand, significant differences based on educational level, socioeconomic status, age, and current occupation.
Like other studies,(8,13,26) this one found that the main problems in the use of MDIs in the target population were the failure to exhale all the air from the lungs before inhaling and not shaking the inhaler for more than 15 sec. To a lesser extent, the frequency of the failure to place the inhaler in the mouth is consistent with the findings of Rau,(10) Sandrini et al.,(14) and Pinto et al.(15)
The occurrence of these mistakes in the use of the inhaler is thought to be correlated with the patient's educational level.(16) This was shown to be the case in the studied population, in which we found significant differences, specifically regarding the steps “exhale all the air from the lungs” and “shake the inhaler for more than 15 sec”; in these two aspects, a better performance was found in patients with higher education levels.
Significant differences were found concerning the items “exhale all the air from the lungs,” “take a deep breath,” “hold the air for 10 sec,” and “shake the inhaler for more than 15 sec,” with better mastery of the technique in younger patients, in accordance with previous studies(16,20) that associate age and inhaler use technique. There were no significant differences by gender in the implementation of the various aspects of the sequence of the proper use of MDIs, as reported in the literature.(18)
Moreover, there are studies(9,18) that recommend the use of spacers or valved holding chambers as a strategy to improve inhaler use technique; it was used by half the patients in the studied population, and they had been informed of its proper use to a lesser extent.
Another strategy to reduce frequent errors in the use of inhalers is education on their proper use and monitoring how patients are actually using them. In the literature review, we found that, in the training process, it is necessary to teach, demonstrate, and assess the proper use of the inhaler, and that the technique should afterwards be reassessed at each visit using the device.(24) Training should include activities such as reading, educational talks, and workshops at the group level, the latter being the most effective strategy.(28,29) Along the lines of thought of these studies, it was found that the demonstration of the inhalation technique is among the most common educational activities in most patients, but that the distribution of written information on the use of MDIs to the patients was not sufficiently implemented.
The information was most often given by the doctor at the first contact with the patient; the second most common source was the nurse, similar to what the literature describes,(17,30) wherein it was found that doctors usually prescribe these methods of inhalation therapy, but frequently do not teach their proper use so as to achieve the desired results. Respiratory therapists play a most relevant role in the educational component within the team that addresses the patient,(31) but in this study only a small percentage of the patients had been given instructions by a therapist.
Studies(19,30,32) show that, during the disease process, no suitable monitoring is provided by the entire health- care team. It was also found in this study that only a quarter of the patients have been asked again how they use an MDI, which shows deficiencies in follow-up educational strategies.
The most frequent mistakes by the health team in teaching the technique were found to be related to not shaking the inhaler and not explaining that the patient should exhale before the inspiratory effort at the time of activation or puff.(19) In the current study, a concordance analysis was done among evaluators; this showed that the steps that were less consistently assessed were “once you have pressed the inhaler, take a deep breath immediately” and “hold your breath for at least 10 sec.” The results of this study show that these are also the steps in which most patients fail to perform well when implementing the technique; this suggests that the health team must reorganize and work harder on the educational approach to the patient.
We concluded that the educational component and the use of the spacer/valved holding chamber are strategies that could improve inhaler use technique. The first one can have high impact, because it relies solely on the health-care team in charge of the patient. Further studies that take into account other variables, such as the type of institution (public vs. private institutions), the use or lack of use of a valved holding chamber, and the training provided by the health team, are needed. As the cost of the spacer/valved holding chamber is high, the use of a nebulizer might be a cost-effective alternative to the MDI, because it may overcome some of the problems associated with MDIs.(26)
Scope and limitations of the study
This study assesses the issue of the technique for the use of MDIs; it found deficiencies not only on the patient's side, but also in the performance of health-care professionals. Hence, this aspect needs to be evaluated regarding the management and mastery of the technique by both populations.
The study was conducted at Hospital Universitario Mayor. It would be ideal to be able to conduct studies in other public and private institutions for purposes of characterization of the users with COPD and/or asthma.
Conclusions and recommendations
With regard to the technique used by patients using MDIs, it was found that only one patient was correctly following the steps for the use of MDIs, and the steps that were most commonly missed (by more than half the patients) were “take a deep breath,” “exhale all the air from the lungs,” and “hold your breath for 10 sec.”
Although it was not possible to conduct a comparative analysis between patients who used the valved holding chamber, it is recommended to consider this for a new research approach, because this is one of the strategies that might ensure correct use of MDIs, but the chamber was not available to all patients.
The study found deficiencies in the educational component, with regard to initial contact and monitoring by the health team, showing insufficient use of strategies such as the delivery of written material, periodic review of technical talks, and workshops. Although health-care personnel were not assessed, it is in any case important that they also be taught how to use MDIs correctly so that they can teach it adequately.
No significant differences were found by gender in the implementation of the various aspects of the sequence of proper use of MDIs. Significant differences were found by educational level: people with higher educational levels tended to have a more adequate technique. In relation to socioeconomic status, significant differences were also found in the use of MDIs.
Significant differences were found related to current occupation; effectiveness was higher in patients who have a labor activity when compared with unemployed and stay-at-home patients. Significant differences were found between age groups, with higher rates of effectiveness in the technical implementation of MDIs in younger patients, especially in those under 60 years of age.
The study shows a problem in the way patients use MDIs and the way they are being taught to use them, with no continuation of this education whatsoever. Therefore, we suggest that strategies that promote education, reinforcement, and feedback be implemented through a well-organized educational program, one that also allows impact assessment.
Footnotes
Acknowledgments
This work was supported by the Universidad del Rosario and the Corporación Hospitalaria Juan Ciudad Méderi–Hospital Universitario Mayor (HUM, Bogota, Colombia).
Author Disclosure Statement
No conflicts of interests exist for any of the authors.