
Abstract
Abstract
Background:
Despite the lack of randomized trials, nebulized Dornase alpha and hypertonic saline are used empirically to treat atelectasis in mechanically ventilated patients. Our objective was to determine the clinical and radiological efficacy of these medications as an adjunct to standard therapy in critically ill patients.
Methods:
Mechanically ventilated patients with new onset (<48 h) lobar or multilobar atelectasis were randomized into three groups: nebulized Dornase alpha, hypertonic (7%) saline or normal saline every 12 h. All patients received standard therapy, including chest percussion therapy, kinetic therapy, and bronchodilators. The primary endpoint was the change in the daily chest X-ray atelectasis score.
Results:
A total of 33 patients met the inclusion criteria and were randomized equally into the three groups. Patients in the Dornase alpha group showed a reduction of 2.18±1.33 points in the CXR score from baseline to day 7, whereas patients in the normal saline group had a reduction of 1.00±1.79 points, and patients in the hypertonic saline group showed a score reduction of 1.09±1.51 points. Pairwise comparison of the mean change of the CXR score showed no statistical difference between hypertonic saline, normal saline, and dornase alpha. Airway pressures as well as oxygenation, expressed as PaO2/FIO2 and time to extubation also were similar among groups. During the study period the rate of extubation was 54% (6/11), 45% (5/11), and 63% (7/11) in the normal saline, hypertonic saline, and Dornase alpha groups, respectively (p=0.09). No treatment related complications were observed.
Conclusions:
There was no significant improvement in the chest X-ray atelectasis score in mechanically ventilated patients with new onset atelectasis who were nebulized with Dornase alpha twice a day. Hypertonic saline was no more effective than normal saline in this population. Larger randomized control trials are needed to confirm our results.
Introduction
Treatment of atelectasis in mechanically ventilated or spontaneously breathing patients usually involves frequent repositioning and suctioning of respiratory secretions, percussion therapy, and kinetic therapy. Incentive spirometry and intermittent positive pressure breathing can also be used in the spontaneously breathing patient.(1) In patients with nonresolving atelectasis, bronchoscopic suctioning may be utilized. Other therapies include the use of nebulized deoxyribonuclease (DNase), despite the lack of randomized trials showing its efficacy in noncystic fibrosis (CF) adult patients. In fact, at the University of Oklahoma Medical Center, 93% of the DNase prescribed in 2005 was for critically ill patients, with an estimated yearly cost of $341,968.
There is little scientific data to support specific use or indications for different nebulized mucolytics in the treatment of lung atelectasis. The aim of the current study is to determine the relative efficacy of nebulized hypertonic saline and DNase compared to normal saline in the treatment of atelectasis in critically ill, mechanically ventilated patients.
Materials and Methods
Study design
This was a prospective, randomized, double-blinded, placebo-controlled trial, conducted between July 2006 and June 2008 at the University of Oklahoma Health Sciences Center (OUHSC) in critically ill mechanically ventilated patients with new onset atelectasis (ClinicalTrials.gov number NCT00671723). The protocol was approved by the institutional review board (IRB#12783) and a written informed consent was obtained from all patients. The trial was designed and executed by the section of Pulmonary and Critical Care Medicine at OUHSC. The investigators were supported by the University of Oklahoma health sciences center while the study drugs were supplied without charge by Oklahoma University Medical Center (OUMC).
Settings and participants
All intubated mechanically ventilated patients in the medical and trauma/neurosurgery ICUs of the OU Medical Center with new onset (<48 h) lobar or multilobar lung atelectasis were eligible for enrollment. Exclusion criteria included history of CF, clinically uncontrolled asthma, severe chronic obstructive pulmonary disease (COPD) with a forced expiratory volume in the first second (FEV1)<30% of predicted, pneumothorax or pleural effusion thought to be causing the atelectasis, lobar atelectasis secondary to compressive tumor, severe hypoxemia defined as PaO2/FIO2 of less than 75, hemodynamic instability, allergy to DNase, use of nebulized acetylcysteine, and pregnancy.
Methods
Patients were identified by daily review of chest roentograms (CXR), and all patients with new onset lobar or multilobar lung atelectasis were invited to be enrolled in the study.
Except for the study drug, patient management was left entirely to the primary team.
This included inhaled bronchodilators, suctioning, ventilatory management, and antibiotics. The need for bronchoscopy was determined by the primary team when other measures were considered to have been ineffective. All patients received daily chest physiotherapy and kinetic therapy. Patients with acute respiratory distress syndrome/acute lung injury (ARDS/ALI) were ventilated with low tidal volumes (6 mL/kg) and positive end expiratory pressure (PEEP) as recommended by the ARDS net, whereas patients with other forms of respiratory failure generally received tidal volumes of 8–10 mL/kg and a PEEP of 5 cm H2O. Atelectasis was defined as patchy or dense areas of consolidation, without air bronchogram, with evidence of loss of volume, following a segmental or lobar distribution, usually appearing abruptly or over 1 to 2 days in a manner more suggestive of atelectasis than pneumonia.
After obtaining informed consent, patients were randomly allocated to one of three nebulized regimens by the research pharmacist at OUMC, with block randomization in groups of three performed.
Group 1 (normal saline) received isotonic saline solution (4 mL of 0.9 % NaCl) nebulized twice daily via an airlife nebulizer, for a fixed period of 15 min, after a 15-min premedication with nebulized albuterol (2.5 mg diluted in 3 mL of 0.9 % NaCl). Group 2 (hypertonic saline) received nebulized hypertonic saline solution (4 mL of 7 % NaCl) twice daily, for a fixed period of 15 min, after a 15-min premedication with nebulized albuterol (2.5 mg diluted in 3 mL of 0.9 % NaCl). Group 3 (Dornase alpha) received 2.5 mg of DNase (Dornase alpha, PULMOZYME®, Genentech, South San Francisco, CA), nebulized twice daily, after a 15-min premedication with nebulized albuterol (2.5 mg diluted in 3 mL of 0.9 % NaCl). All nebulized solutions were dispensed in similar appearing vials. Patients were monitored for the occurrence of wheezing during the administration of the therapy. Treatment in the three groups was continued for 7 days, or until complete resolution of the atelectasis, whichever occurred first. Patients with early resolution continued to be monitored in the study until 7 days after the onset of treatment for atelectasis.
Daily CXR were reviewed by a single radiologist who was blinded to the group assignment. The primary variable monitored was the extent of atelectasis on a portable chest radiograph. Each CXR was assigned an atelectasis score.(2) The absence or presence of contralateral hyperinflation was marked as 0 or 1 point, respectively. The absence or presence of mediastinal shift was scored as 0 or 1, respectively. Atelectasis was scored for each lobe. A partial atelectasis of one lobe was scored as one point, whereas complete atelectasis of a lobe was marked as two points. The distinction between infiltrate and atelectasis as well as the total scoring was done by the interpreting radiologist. These results were summed for each CXR. The baseline score was compared to the scores at 24, 48, 72 hours and at 7 days after treatment.
Demographic data were collected on all patients. The Acute Physiology and Chronic Health Evaluation (APACHE II) score was calculated at the time of randomization into the study. Ventilator characteristics including days on mechanical ventilation, ventilatory mode, and airway pressures including PEEP, were recorded. The PaO2/FIO2 was also calculated.
Complications related to the study medications including any wheezing or hypoxemia were monitored.
Statistical analysis
The primary end point was the difference, between the three groups, in the rate of change in the CXR atelectasis score. Secondary endpoints included the changes in PaO2/FIO2, need for bronchoscopic suctioning, and days on mechanical ventilation.
The mixed model with a repeated factor was used to compare the radiological score and PaO2/FIO2 at baseline, 24, 48, 72 hours, and 7 days between the test and control groups. Based on a prior study done on 24 patients with lung atelectasis,(1) where the median radiological score was 4 and the standard deviation was 1.8, a repeated measures design with one between factor (treatment group) and one within factor (time) required three groups with 11 subjects per group for a total of 33 subjects, where each subject is measured five times. This would provide a 91% power to test for a difference in treatments over time if an F test is used with a 5% significance level and the actual within-subject standard deviation is 1.8.
All pairwise, multiple comparison tests are reported with confidence intervals corrected using the Tukey method. Differences between curves for all three treatment groups and for each pair of treatment groups were conducted using log-rank tests.
Results
As planned, a total of 33 patients were enrolled in the study, 11 per group. The baseline characteristics of these patients were summarized in Table 1. There was no significant difference in the baseline characteristics of the three groups including age, frequency of smoking, white blood cell count, ventilatory mode, PaO2/FiO2, and APACHE II scores calculated at the time of enrollment. Although there were more patients enrolled overall from trauma/neurosurgical ICU (20/33, 60%) than medical ICU (13/33, 40%), the distribution of patients in each group was similar. There were two deaths in the control group, both on day 7 of the study, and one death in the hypertonic saline group on day 3 of the study.
Data are presented as mean±SD unless otherwise indicated.
p=nonsignificant for all comparisons.
At baseline, the magnitude of atelectasis as evaluated by the CXR atelectasis score was similar between the three groups (Table 1). Thirteen (39%) patients had atelectasis in more than one location. Most atelectasis were seen in the lower lobes, with all but one patient having at least one of the lower lobes involved.
Of the patients alive on day 7, 13 had days where no CXR was ordered, and therefore no score could be obtained [a total of 32 time points out of 264 (12%)]. Eleven of these patients were extubated, and the primary team did not believe that a CXR was medically indicated on those particular days.
Primary outcome
Analysis of the change in CXR score from baseline to days 1, 2, 3, and 7 was done as shown in Table 2. On average, patients in the Dornase alpha group showed a reduction of 2.18±1.33 points in the CXR score from baseline to day 7 (Fig. 1a), whereas patients in the normal saline group had a reduction of 1.00±1.79 point (Fig. 1b), and patients in the hypertonic saline group showed a score reduction of 1.09±1.51 point (Fig. 1c). The difference between these changes was not statistically significant (Fig. 1d). Pairwise comparison of the mean change of the CXR score showed no difference between the hypertonic and normal saline groups. Dornase alpha resulted in a 1.09 [95% confidence interval (CI): −0.54–2.73] greater reduction in the CXR score compared to hypertonic saline, and 1.18 (95% CI: −0.45–2.82) greater reduction in the CXR score compared to normal saline.

Chest X-ray atelectasis scores over time in the dornase alpha group (
Secondary outcomes
PaO2/FiO2
Analysis of the PaO2/FiO2 change from baseline to day 7 was done (Table 3). Between baseline and day 7, patients in the Dornase alpha group showed an increase in the PaO2/FiO2 of 57 units, wheres patients in the normal saline treatment group showed a reduction in the PaO2/FiO2 of 2 units, and patients in the hypertonic saline group showed an increase of 77 units. The difference between these changes was not statistically significant.
Bronchoscopy
Two patients in the hypertonic saline group underwent bronchoscopic suctioning, compared to one patient in the NS group and three in the Dornase alpha group. There was no change in the CXR atelectasis score post bronchoscopy. In addition, we found no significant difference between the three groups in terms of the change from baseline to day 7 in the mean airway pressure or the PEEP (p=NS).
Days on mechanical ventilation
During the study period 54% (6/11), 45 (5/11), and 63% (7/11) patients were extubated in the normal saline, hypertonic saline and Dornase alpha groups, respectively. Two patients died on day 7 in the normal saline group and one patient died on day 3 in the hypertonic saline group.
A summary of the cumulative number of patients extubated by treatment group with patient death as a competing event is displayed in Figure 2. The difference between the three treatment groups was not statistically significant (p=0.09).
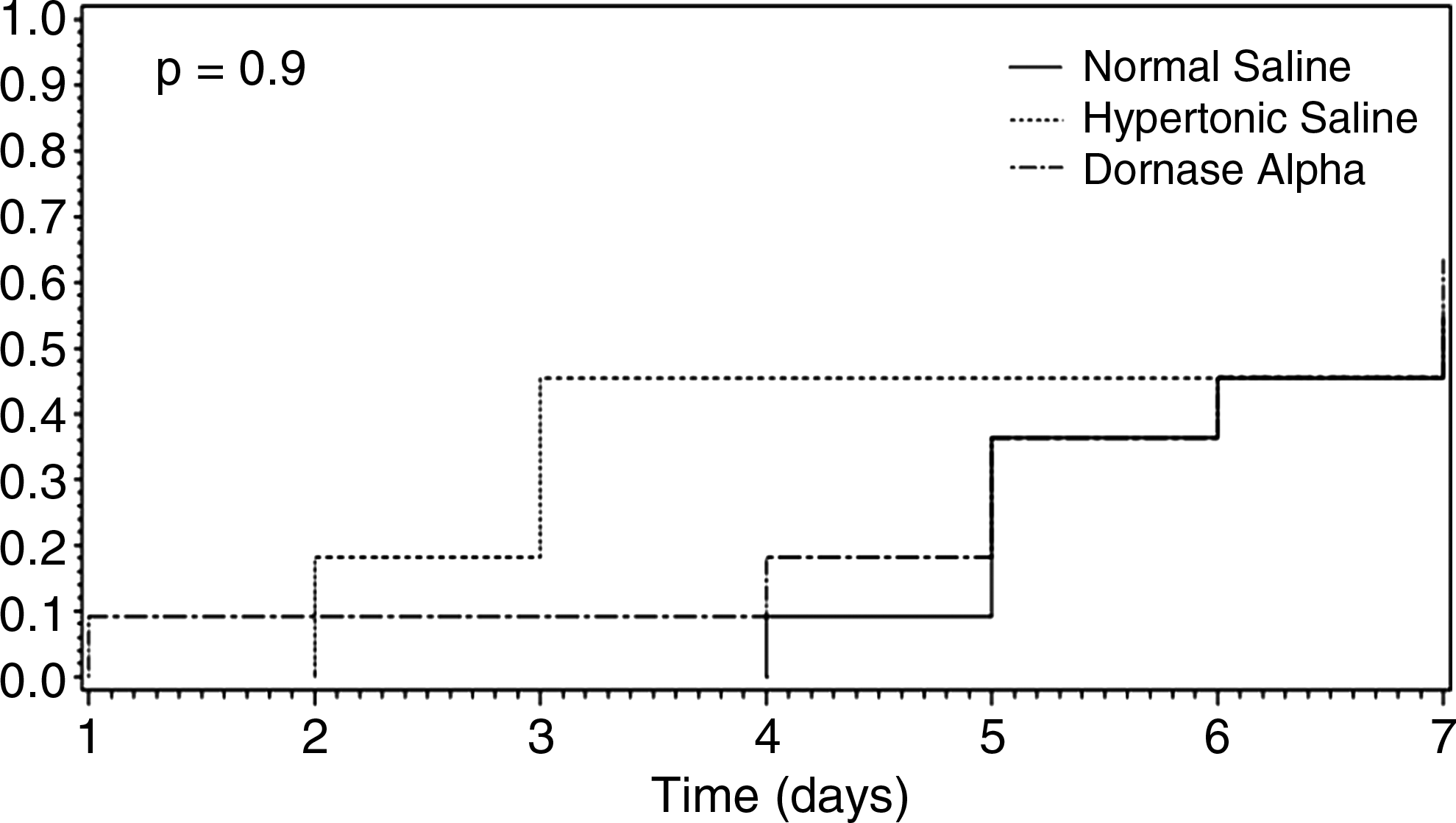
Estimated cumulative incidence curves of time to extubation with death as a competing event.
Side effects
There was no complications such as wheezing or worsening hypoxemia reported during the study related to the nebulized medications.
Discussion
Atelectasis is a common problem in critically ill patients who are unable to cough effectively and have difficulty mobilizing their respiratory secretions. It has been reported in 85% of patients with neuromuscular diseases,(3) 90% of post cardiac surgery patients, and in 20 to 30% of patients following upper abdominal surgery.(4)
Several mechanisms may cause or contribute to the development of atelectasis in intubated patients, including mucosal inflammation and mucus hypersecretion,(5) impaired mucous transport,(6) impaired cough reflex, compression of lung tissue, absorption of alveolar air, and impairment of surfactant function.(7)
Compression atelectasis occurs when the transmural pressure distending the alveolus is reduced to a level that allows the alveolus to collapse. In intubated patients, the diaphragm is relaxed and displaced cephalic and is therefore less effective in maintaining distinct pressures in the two cavities. Specifically, the pleural pressure increases to the greatest extent in the dependent lung regions and can compress the adjacent lung tissue.(7)
Absorption of alveolar air can occur by two mechanisms. After complete airway occlusion, a pocket of trapped gas is created in the lung unit distal to the obstruction. Because gas uptake by the blood continues and gas inflow is prevented by blocked airways, the gas pocket collapses.(8) Under these conditions, increasing the FiO2 increases the rate of absorption of gas from an unventilated lung areas,(9) and may lead to atelectasis.
Mobilizing the respiratory secretions is determined by the efficiency of mucociliary clearance, which depends on the characteristics of the mucus as well as the beating of the cilia.(10) Because the principal polymer components of sputum gels (mucins and DNA) are polyanionic, the concentration of major ions, primarily sodium and chloride, influences the rheology of the mucus.(11) In fact, adding sodium chloride to the sputum significantly enhances its transportability when compared to sputum incubated in hypotonic solutions.(10) Mucus equilibrated with 300–500 mosM saline was maximally transported. It was poorly transported when its salinity was 200 mosM, and almost stationary when equilibrated in 100 mosM saline or water. There was no change in the ciliary beating frequency at these concentrations. Furthermore, there was an inverse relationship between viscoelasticity of respiratory mucus and sputum salinity in the pathophysiological range.(10,12)
Another mechanism responsible for increased mucus viscosity and adhesiveness is the increased concentration of DNA, typically from degenerating leucocytes and epithelial debris. This is encountered in inflammatory secretions,(13) in patients with cystic fibrosis,(14) bronchiectasis,(15) and respiratory syncytial virus (RSV) bronchiolitis.(16) In infections complicated by atelectasis, bronchial secretions and mucus plugs also have high concentration of DNA. Therefore DNase could be an effective treatment in this situation.(16) In addition, treatment of CF sputum with DNase decreases the molecular size of the DNA, thus reducing its contribution to viscoelasticity.(14) In fact, recombinant human DNase has been proven to be an effective treatment of atelectasis in patients with CF.(17,18)
Development of atelectasis is associated with the development of several pathophysiologic effects, including decreased lung compliance, shunt with attendant hypoxemia, increased pulmonary vascular resistance, and development of lung injury.(7) The pooled and stagnant secretions may act as a nidus for bacterial proliferation, culminating in nosocomial pneumonia(19) and the consequences include a significant burden in terms of morbidity,(20) and additional healthcare costs.(21)
Reported therapy for atelectasis in mechanically ventilated patients includes chest physiotherapy, kinetic therapy, vibration therapy, positioning for optimal lung drainage, and endotracheal suctioning. If all these measures fail, bronchoscopy and/or recruitment maneuvers may be attempted.(1,22–24) All these therapy are aimed at mechanical mobilization of the secretions. There is a paucity of information in adults about therapies that target the viscoelasticity of respiratory mucus in mechanically ventilated patients.
Dornase alpha and hypertonic saline have been used in atelectasis caused by hyperviscouse tracheal secretions, with studies reporting benefit in cystic fibrosis patients.(14,25,26)
Elkins et al.(26) showed that the long term use of 4 mL of 7% hypertonic saline solution nebulized twice daily is an inexpensive and safe additional therapy when preceded by a bronchodilator in patients with CF.(26) These patients had improved lung function and reduced exacerbations during the 48-week trial. We used the same dose and frequency in the hypertonic saline arm of our study.
Studies done mainly in intubated children and infants with atelectasis report beneficial effect of Dornase alpha with reduced rate of atelectasis, mechanical ventilation, ICU length of stay, and mean cost.(27,28) In a recent study, 40 newborn with persistent atelectasis were randomized to nebulized 3% hypertonic saline or recombinant human DNase (rhDNase). Patients in the hypertonic solution group had greater chest X-ray scores improvement compared to the rhDNase group (p<0.001). The percentage of atelectasis resolution after 3 days treatment were 90% (18/20) in the 3% HS group and 70% (14/20) in the rhDNase group (p=NS).(29)
An in vitro study comparing the effect of hypertonic saline and DNase in CF patients showed that treatment with hypertonic saline decreased the sputum viscoelasticity index. The effect of DNase was minimal, and adding DNase to hypertonic saline did not result in an additive effect.(30)
To our knowledge, our trial is the first to evaluate the effect of nebulized Dornase alpha and hypertonic saline in the treatment of atelectasis in critically ill mechanically ventilated adults as an add on to standard therapy, including chest percussion therapy, kinetic therapy, and bronchodilators. The majority of these cases involved the lower lobes. Although a greater improvement in the CXR atelectasis score was noted in the Dornase alpha group compared to the hypertonic saline and normal saline groups, the difference was not statistically significant. In addition, there was a trend to improvement in oxygenation as measured by the PaO2/FIO2 with the use of Dornase alpha and hypertonic saline, which also did not reach statistical significance.
Even though it is used for suctioning of secretions causing atelectasis,(1) flexible bronchoscopy followed by respiratory therapy for 48 h has not proven to be superior to respiratory therapy alone with regard to restoration of volume loss, at 24 or at 48 h.(24) The number of patients undergoing the procedure in our study was too small to draw any firm conclusion regarding possible potential effect (procedure done in a total of six patients), but it is worth noting that no change in the atelectasis score was noted on the post procedure chest X-ray.
A limitation of the current study is the missing CXR scores for some patients (14% of the total data points). This occurred typically after the patients were weaned off mechanical ventilation. CXR were ordered by the primary care team who felt the clinical improvement seen in those patients did not justify getting a CXR.
Another limitation is the lack of a validated CXR scoring system for the adult population. We used the current system in order to quantify the response to treatment. Developing and validating a system requires a larger study that would incorporate clinical and radiographic response, but would provide a useful tool for evaluating the extent and the changes of atelectasis over time.
Another factor that could have influenced our results is the concentration of the different study drugs at the level of the airways, which varies depending on the distribution of aerosol deposition. It is possible that the concentration at the level of the obstructed bronchi is less than optimal, and that higher doses or more frequent administration will achieve a better therapeutic effect. In addition, we cannot rule out the possibility that combining Dornase alpha and hypertonic saline may have an additive effect on atelectasis. Our study was not designed to answer this specific question.
In summary, there is a wide range of therapies administered to ICU patients for atelectasis; our study is the first in adult patients to target sputum viscoelasticity in critically ill mechanically ventilated patients with new onset atelectasis. The use of dornase alpha or hypertonic saline did not improve the rate of recovery from atelectasis. Larger randomized controlled trials powered to assess outcome such as ventilator days, ICU, and hospital days are needed.
Footnotes
Acknowledgments
Impact research will have on clinical medicine and basic science: The current study shows that the addition of dornase alpha or hypertonic saline to standard therapy in critically ill mechanically ventilated patients with atelectasis may not result in added benefit. How research adds to knowledge base of the disease process: The use of these agents in such situations may not be endorsed. ClinicalTrials.gov Identifier: NCT00671723
Author Contributions
All authors were involved with the acquisition, analysis, and interpretation of data. Drs. Youness and Keddissi were involved in the conception and design of the study. Kathryn Mathews, was involved in patients' randomization and in obtaining funding. Drs. Elya and Youness were involved in patient recruitment. Dr. Youness was involved in the drafting of the manuscript. Drs. Keddissi and Kinasewitz were involved in the supervision of the study and the critical revision of the manuscript.
Author Disclosure Statement
The authors declare that no conflicting financial interests exist.