
Abstract
Abstract
Background:
Our study investigated the influence of the cannula's inner diameter (ID) and of its removal on the expected respiratory dose of amikacin, using three different jet nebulizer configurations (Sidestream®): vented (N1), unvented with a piece of corrugated tubing attached to the expiratory limb of the T attachment (N2), and unvented alone (N3).
Methods:
The jet nebulizer was filled with amikacin (500 mg/4 mL) and was attached to the tracheostomy tube. A lung model simulating spontaneous breathing was connected to the tracheostomy tube. A filter was connected between the nebulizer and the tracheostomy tube to measure the inhaled dose, and between the tracheostomy tube and the lung model to measure the respiratory dose. Different cannula IDs were tested (6.5, 8, 8.5, and 10 mm), and aerosol lost in the cannulas was determined.
Results and conclusions:
Respiratory dose varied between 96±1 mg and 44±3 mg, with higher values observed with N2. The aerosol lost in the cannula was significant and represented up to 63% of the inhaled dose. There was a negative correlation between the cannula's ID and the aerosol lost in the cannula. After removal of the internal cannula, an increase in the respiratory dose of up to 31.3% was observed. We recommend removing the inner tracheostomy cannula to nebulize a larger amount of drug through a tracheostomy tube. Among the three jet nebulizer configurations studied, we recommend the unvented one with a piece of corrugated tubing attached to the expiratory limb of the T attachment.
Introduction
Disposable jet nebulizers are widely used, especially for hospitalized patients needing nebulization for a short period and to avoid the risk of bacterial contamination.(24) T-piece interface between the tracheostomy tube and the nebulizer is more effective than a tracheostomy mask(23,25) and should be used in spontaneously breathing patients with tracheostomies. Despite this recommendation, many nebulizer sets with different interfaces adapted for tracheostomy, including different masks and T-pieces, are commercially available. Among the commercially available jet nebulizers, the Sidestream® vented jet nebulizer is widely used and has been extensively studied. The Sidestream jet nebulizer delivers nebulized drug with a very constant droplet-size distribution when used with the Portaneb Compressor.(26) A previous study found that a modified unvented Sidestream coupled with an extension increased amikacin lung dose deposition in healthy subjects.(27) We have found several commercially available “Sidestream for tracheostomy sets” with a tracheostomy mask or different T-piece models directly connected to the reservoir, some blocking and others allowing the extra vent.
Aerosol administration through an artificial airway such as a tracheostomy tube could be influenced by parameters including the ID, length, and curvature of the cannula, and nebulizer type.(25)
From a clinical perspective, the primary objective of our study was to examine whether the inner cannula should be removed during nebulization in spontaneously breathing tracheostomized patients. The secondary objectives were, first, to evaluate the influence on drug delivery of the cannula diameter of two adult dual-cannula tracheostomy tube models, and, second, to evaluate how different jet nebulizer configurations (a standard jet nebulizer alone or with corrugated tubing, and a vented jet nebulizer) affect drug deposition when nebulizing through a tracheostomy tube, in order to find the most efficient jet nebulizer setup to deliver antibiotics to the lung.
Materials and Methods
Nebulizers
Three configurations of a well-known and validated jet nebulizer (Sidestream; Medic-Aid, West Sussex, UK) were used; one with a T-piece (18F; Medic-Aid, UK) allowing an extra vent (N1), and two with the T-piece (22M; Medic-Aid, UK) blocking the extra vent: with the T-piece connected to a 110-mL piece of corrugated tubing (N2), and with the T-piece alone (N3) (Fig. 1). The nebulizer was driven by a suitable compressor (Portaneb, driving gas flow 6 L/min; Medicaid, Pagham, UK).
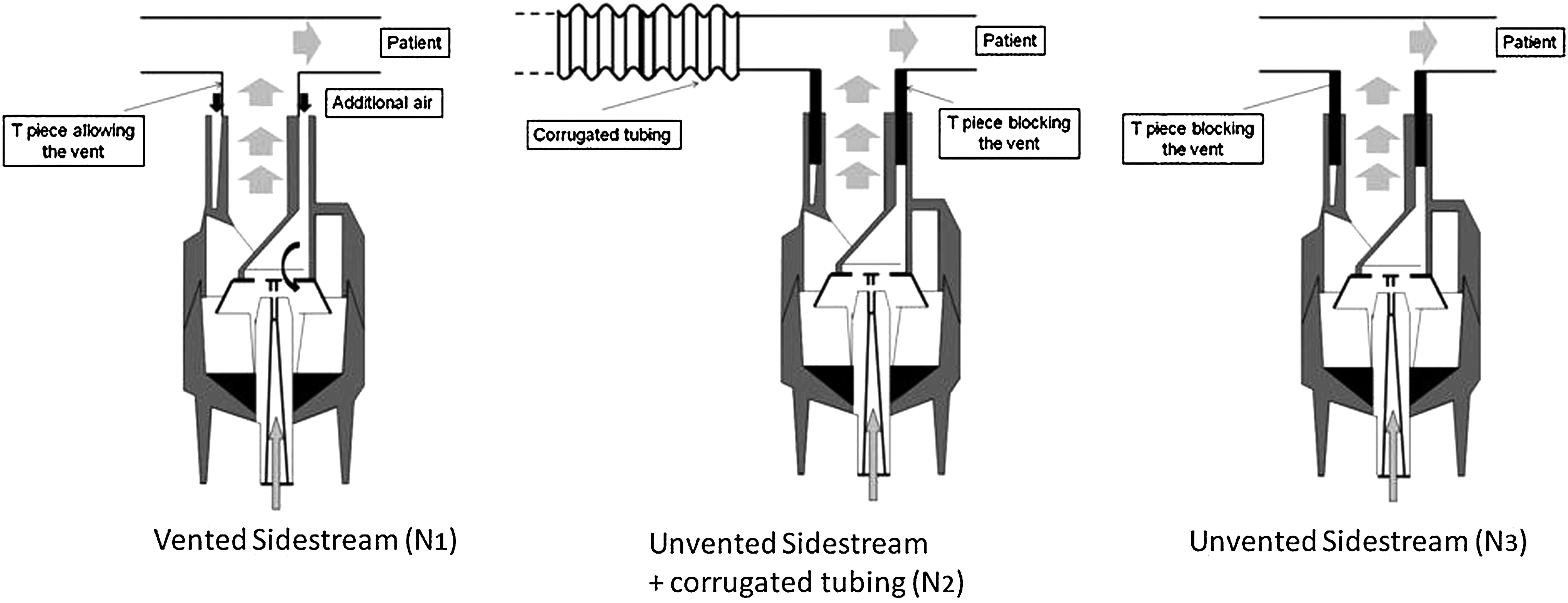
The three jet nebulizer systems (Sidestream; Philips-Respironics, Pittsburgh, PA): one with a T-piece allowing an extra vent (N1), one with a T-piece blocking the extra vent and a 110-mL corrugated tube connected to the expiratory side (N2), and one with a T-piece blocking the extra vent (N3).
Tracheostomy tubes
Two cuffed dual-cannula tracheostomy tubes (tubes A and B) (Portex® Blue Line Ultra®; Smith, UK) were used, each with a disposable inner cannula and an external cannula (see Fig. 2). The IDs of the external cannulas were 10 mm (A) and 8 mm (B), and the IDs of the inner cannulas were 8.5 mm (A) and 6.5 mm (B). The length of the cannulas was 87.5 mm and 75.5 mm for A and B, respectively.
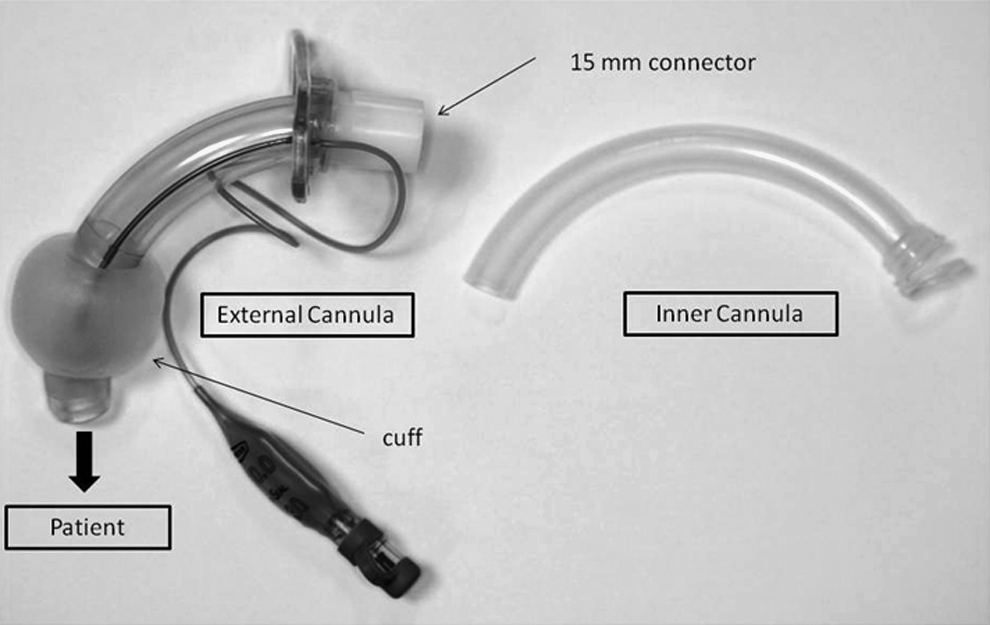
Illustration of the cuffed dual-cannula tracheostomy tube, with external and inner cannulas, used in the experimental setup (Portex Blue Line Ultra; Smith, UK).
Particle-size measurement
Particle-size distribution from both nebulizer device configurations was assessed using a Malvern Mastersizer-X laser particle sizer (Malvern Instruments Ltd., Malvern, UK) following the protocol described by Majoral and colleagues.(12b) Nebulizers were filled with 4 mL of 125 mg/mL amikacin solution. All measurements were performed in duplicate with three samples for each nebulizer configuration.
Particle size measurements were performed in standing cloud during 1 min of nebulization. The dispersion code was “polydisperse,” and the optical presentation was “2QAA.” Analyses were carried out with Mastersizer-X software (Malvern Instruments Ltd.), and results were expressed as median mass aerodynamic diameter (MMAD). The fraction of the mass of drug contained in particles with a diameter of between 1 μm and 5 μm was considered as the respirable fraction (RF%) of the aerosol mass, reflecting particle deposition in the bronchial tree.
In vitro assessment of inhaled dose, respiratory dose, and respiratory drug output rate
In vitro experiments were performed to quantify the inhaled dose, the respiratory dose, and the respiratory drug output rate. The inhaled dose was defined as the quantity of drug recovered at the entrance of the tracheostomy tube. The respiratory dose was the quantity of drug delivered to the exit of the tracheostomy tube, corresponding to the dose that would penetrate the lower airways, including part of the trachea and lungs in a patient.
The respiratory drug output rate was expressed as the respiratory dose divided by nebulization time.
The inhaled and respiratory doses were assessed using the residual gravimetric method,(13) as previously used to compare nebulizer configurations.(27,28) Each nebulizer was filled with 4 mL of amikacin solution (125 mg/mL) (Amukin; Bristol-Myers Squibb, Braine l'Alleud, Belgium) and was weighed empty, after filling, and at the end of nebulization. The mass of the solution emitted was the difference between the weights after filling and at the end of nebulization. The nebulizers were connected to a lung model (5600i Dual Adult Training/Test Lung; Michigan Instrument Inc., Grand Rapids, MI) and were set at 20/min frequency, 440 mL tidal volume, 10% inspiratory pause, and 33% inspiration/expiration ratio.
A filter holder containing a dry filter (Air Safety Ltd., Lancashire, UK), weighed before nebulization, was placed in two different positions depending on the dose studied: between the nebulizer and the proximal part of the tracheostomy tube to obtain the inhaled dose (position A, Fig. 3), and between the lung model and the distal part of the tracheostomy tube to measure the respiratory dose (position B, Fig. 3). The solution was nebulized until 1 min after the sputtering point for the three Sidestream configurations. To avoid condensation droplets falling onto the filter, the tube was placed horizontally and condensation droplets were trapped in the filter holder. At the end of the experiment, the filter was dried for 24 hr at ambient temperature. Drug mass was calculated by subtracting the initial weight of the filter from its weight 24 hr after nebulization. Inhaled mass was calculated by multiplying the drug mass by the relative mass of active compounds. The inhaled dose was measured in triplicate for each nebulizer configuration. All measurements were performed under the same hygrometric conditions. Weights were calculated using a high-precision scale (Mettler AE166; Mettler Instruments, Zurich, Switzerland; 0.0001 g precision).
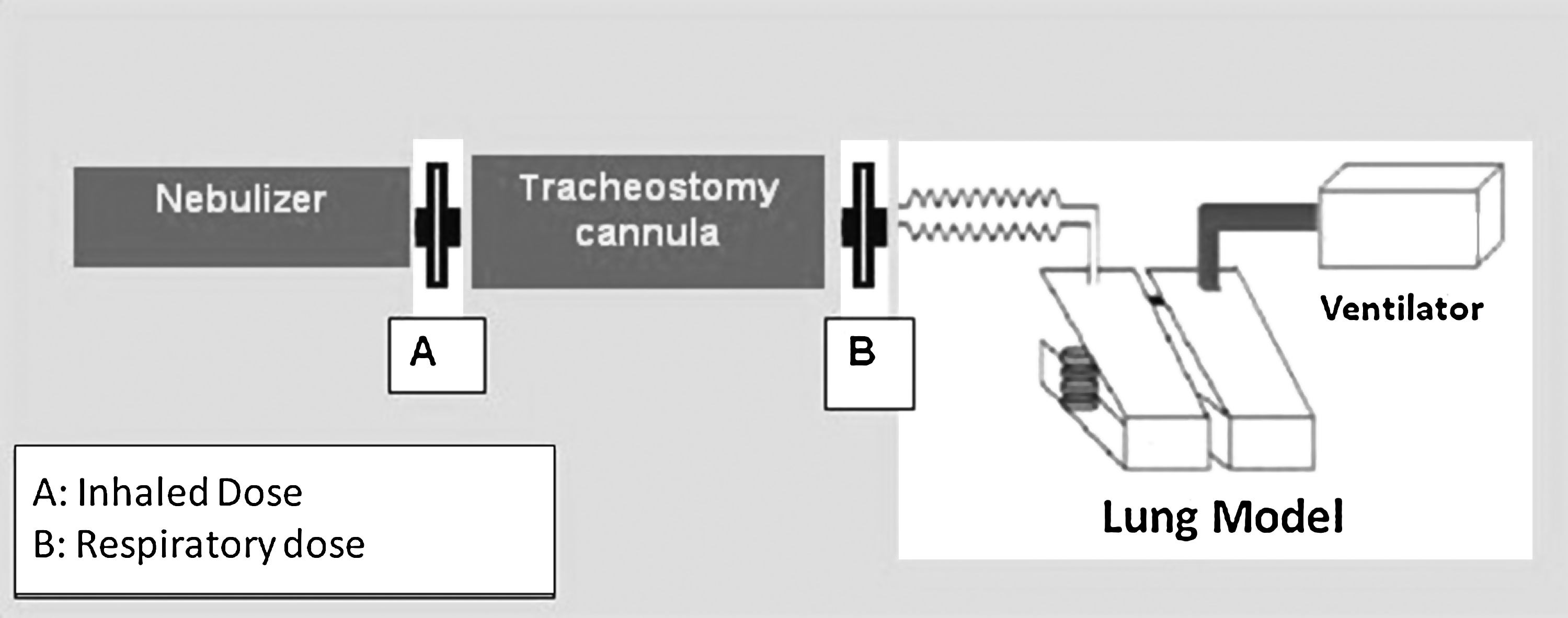
Experimental setup for the bench measurement. The filter placed in position A collects the inhaled dose, and the filter placed in position B collects the respiratory dose.
Furthermore, the mass of amikacin lost in the tracheostomy tube was calculated as the difference between the inhaled dose and the respiratory dose. The percentage of amikacin lost in the tracheostomy tube in terms of inhaled dose was calculated as the ratio between the mass of amikacin lost in the tracheostomy tube and the inhaled dose.
Statistical analyses
Results are presented as means±SD. The significance of the differences between devices was assessed by ANOVA. When appropriate, between-group comparisons were made using a post-hoc test with a p level of 0.05 using the Holm-Bonferroni correction. Comparisons between the inner and external cannulas were made using the unpaired Student's t test. The correlation between the drug lost in the tracheostomy tube and the tracheostomy tube ID was assessed using the Pearson correlation test. In all cases, significance was based on p≤0.05.
Results
Influence of the inner cannula
Table 1 shows the results for the 10-mm and 8-mm ID external cannulas and the 8.5-mm and 6.5-mm ID inner cannulas (cannula A and B, respectively). Removing the inner cannula resulted in an increase in respiratory dose varying from 3.7% to 31.3%. For cannula A, removing the inner cannula was associated with a small and not statistically different increase in respiratory deposition with N1, whereas this increase in respiratory dose was statistically significant for N2 and N3 with 21.2% (p=0.002) and 17.1% (p<0.001), respectively. For cannula B, removing the inner cannula was associated with a statistically significant increase in respiratory dose of about 17.1% (p=0.002), 31.3% (p<0.001), and 30.3% (p<0.001) for N1, N2, and N3, respectively. The mean respiratory dose measured with the two tracheostomy models studied using the three jet nebulizer configurations (Fig. 4) was significantly increased when the inner cannula was removed (70.8±14.2 mg without the inner cannula vs. 56.2±11.8 mg with the inner cannula; p=0.002).
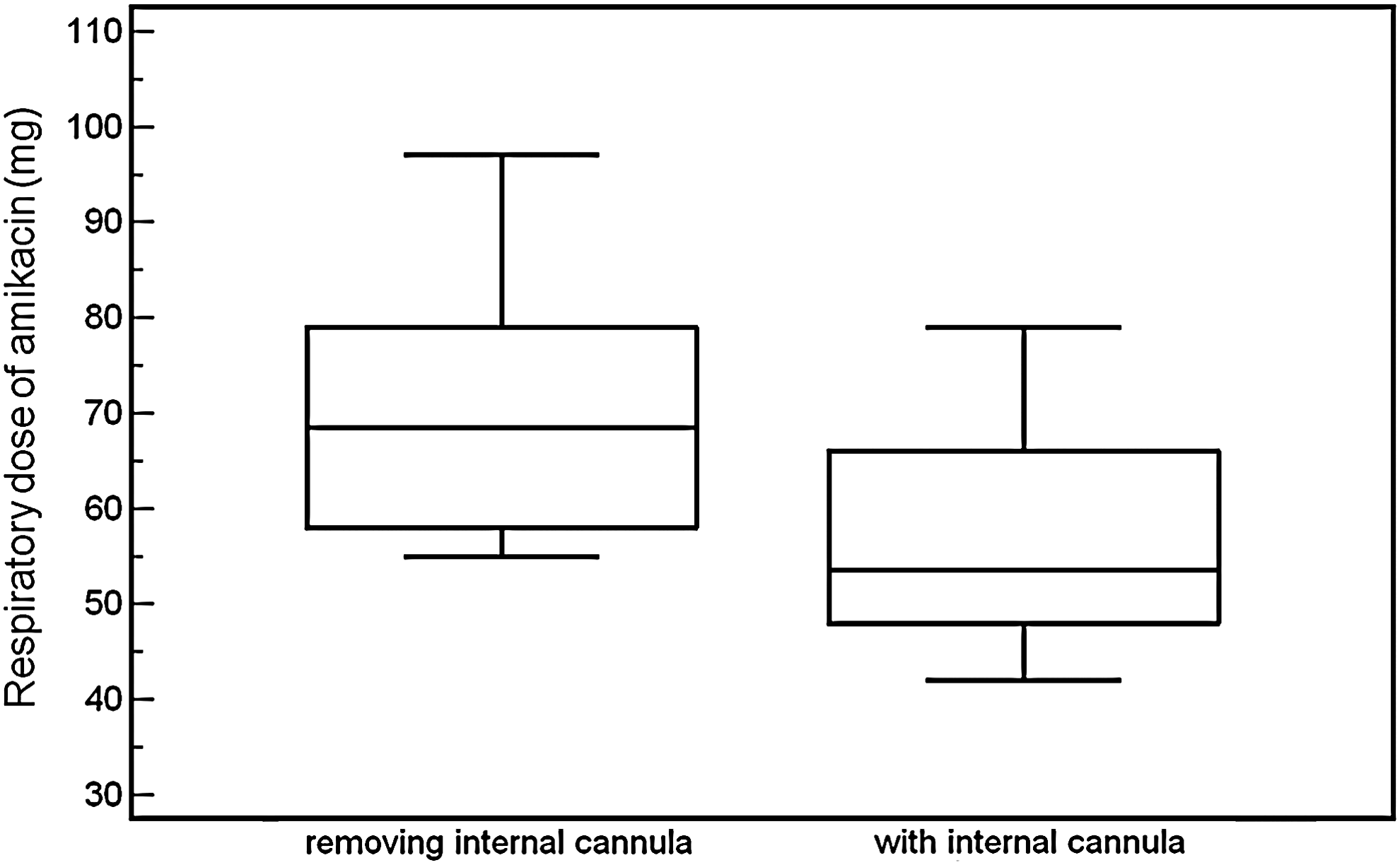
Influence of removing the inner cannula on in vitro respiratory doses obtained during nebulization with vented (N1), unvented with spacer (N2), and unvented alone (N3) jet nebulizers (Sidestream, Philips-Respironics), using two different external and internal tracheostomy cannulas. Results are expressed as means±SD.
Results are expressed as means±SD.
Influence of the ID
Results regarding the influence of ID are presented in Table 1. Reducing the ID of the cannula had no impact on inhaled dose for any of the nebulizer configurations (p=0.874, p=0.438, and p=0.953 for N1, N2, and N3, respectively). A significant difference between inhaled dose and respiratory dose was always observed, demonstrating that the cannula reduced the amount of drug administered (p<0.001). The impact of ID on respiratory dose differed according to the nebulizer configuration. With N1, a significantly lower respiratory dose was observed for the 6.5-mm ID cannula compared with the other three cannulas. With N2 and N3, a significantly higher respiratory dose was observed with the 10-mm ID than with the other three ID cannulas. No significant differences were observed between the 8.5- and the 8-mm ID cannulas. Significantly lower respiratory doses were found with the 6.5-mm ID cannula compared with the other three cannulas. Figure 5 shows a negative correlation between the percentage of amikacin lost in the tracheostomy cannula [(respiratory dose – inhaled dose)/inhaled dose] and the decrease in tracheostomy ID for the three nebulizer configurations (r=−0.96 for N1 and −0.99 for N2 and N3; p<0.001 for N1, N2, and N3).

Descriptive plot of correlations between the loss of amikacin in the tracheostomy tube, expressed as a percentage of the inhaled dose, and the four ID tracheostomy cannulas (10, 8.7, 8.5, and 6.5 mm) during nebulization with vented (N1), unvented with spacer (N2), and unvented alone (N3) jet nebulizers (Sidestream, Philips-Respironics).
Influence of nebulizer configurations
Particle size measurements are presented in Table 2. MMAD decreased and respirable fraction increased with N1 compared with N2 and N3. MMAD and respirable fraction did not significantly differ between the two unvented jet nebulizer configurations.
Results are expressed as means±SD.
MMAD, median mass aerosol diameter; RF, respiratory fraction.
Inhaled doses, respiratory doses, and respiratory drug output rates are presented in Table 1. Inhaled dose differed significantly between the nebulizers for all the cannulas (p<0.001). Significantly lower inhaled doses were observed with N1 than with N2 and N3 (p<0.001 for all cannulas). Significantly higher inhaled doses were observed with N2 than with N1 and N3 (p<0.001 for all cannulas), whereas intermediate values were observed with N3. The respiratory dose differed significantly between the nebulizer configurations for the three largest cannulas (p<0.001 for 10-, 8.5-, and 8-mm ID cannulas). Significantly higher respiratory doses were observed with N2 than with the other two configurations. The nebulizer drug output rates differed between the three nebulizer configurations for the 8.5-, 8-, and 6.5-mm ID cannulas (p<0.001 for 8.5-, 8-, and 6.5-mm ID cannulas). A significantly higher respiratory drug output rate was observed with N1. Intermediate values were observed with N2, and N3 presented significantly lower values than the other two nebulizer configurations.
Discussion
In the present study, we used two dual-cannula tracheostomy tube models. The inner cannula was disposable. The use of an inner cannula allows it to be cleaned and replaced at different intervals. It can also be removed to restore the airway diameter when the tube occludes.(29) Our study revealed that removing the inner cannula always increased drug deposition beyond the cannula. This can be explained by the increased ID with the inner cannula removed, resulting in less particle deposition in the cannula. Our results show that cannula removal has a greater influence with smaller cannulas and with unvented nebulizers. However, in a clinical setting, we cannot always choose what nebulizer to use, but removal of the inner cannula is always possible and is a simple way of increasing respiratory drug delivery. In our bench model, the cannulas were washed and dried before each measurement. In a clinical setting, removing the inner cannula could also allow nebulization through a cleaner cannula; the presence of secretion in the inner cannula narrows its ID, leading to less drug deposition beyond the cannula. Removing the inner cannula has also been shown to decrease the work of breathing for a spontaneously breathing patient.(30) This could change the respiratory pattern and influence respiratory deposition.
The amount of aerosol delivered at the distal part of the cannula varied between 9% and 19% of the nominal dose. This maximal amount is similar to findings in the literature.(25) Some factors could help explain the considerable variation in the amount of drug delivered, including variations in the ID of the tracheostomy tubes and in the amount of inhaled drug.
Endotracheal tubes have long been considered to be significant barriers to the deposition of inhaled drugs,(31) and the influence of endotracheal tube size on aerosol deposition has been widely reported in the literature.(19–22,32) In our study, we also highlighted the influence of the tube ID on aerosol deposition. We observed a decrease in aerosol delivery with smaller tracheostomy ID. These results are comparable to those of Pedersen and colleagues,(22) who compared aerosol deposition in a mechanically ventilated patient model through endotracheal tubes with internal diameters of 6, 7, and 8 mm. Delivery of aerosol to the extremity of the endotracheal tube decreased with smaller diameters.(22) The difference of aerosol deposition observed when reducing the cannula ID can be explained by an impaction effect characterized by the Stokes number, which depends on air velocity and particle size. For the same flow rate, the air velocity in the cannula depends on the ID of the cannula; the smaller the ID, the greater the velocity and the greater the impaction of particles in the tube. During nebulization with N2 and N3, a large proportion of the aerosol was visually observed as deposit on the tracheostomy tube. The smaller the tube, the more this condensation was observed resulting from the impaction of particles on the tube. These visual observations are confirmed by our results (Fig. 5) showing a negative correlation between the percentage of amikacin lost in the tracheostomy cannula and the ID of the cannula: as the ID decreases, so the amount of amikacin lost in the tube increases. An alternative explanation of the influence of the ID tube on drug deposition could be that small-diameter tubes create more turbulence as gas enters from the larger diameter connector site, resulting in higher impaction.(32,33) This was not the case in our study as shown by the calculated Reynolds numbers (ReN=air density * air velocity * tube diameter/air viscosity), which were below 2,700 for the four cannulas (1,247 for the 10-mm tube, 1,433 for the 8.7-mm tube, 1,468 for the 8.5-mm tube, and 1,915 for the 6.5-mm tube), indicating that the flow was not turbulent. In tracheostomized patients, higher inspiratory flow and secretions in the tube, narrowing its ID, could result in the laminar flow becoming turbulent.
Particles are captured in the tracheostomy tube during inhalation and exhalation. In a previous study on ventilated tracheostomized patients, the majority of aerosol deposition (7 out of 10% of the nominal dose) occurred during exhalation.(16) In our spontaneously breathing tracheostomized patient model, no difference was observed between deposition during inhalation and exhalation. As our filter was directly connected to the tip of the tube, it reduced the normal anatomical dead space, and a significant proportion of the inhaled drug reaching the distal part of the tube could impact on the filter.
In a previous report on mechanically ventilated tracheostomized patients, the average deposition on the tracheostomy tube was 38.6% of the inhaled dose (tube deposition+respiratory deposition).(16) The average deposition in the tracheostomy tube calculated in our study was similar, with 31.5±15.4% of the inhaled dose. Nevertheless, we observed a huge variation in drug deposition in the tracheostomy tube between the three nebulizers studied. Two phenomena could explain this disproportionate drug loss in the tracheostomy tube. First, the smaller particle size with N1 than with N2 and N3 may have reduced impaction in the tube. The larger the particle, the more readily it will be influenced by gravity and thus removed from the airstream, impacting the tracheostomy tube.(34) Second, as the inhaled dose was higher with N2 than with N1 and N3, the amount of drug impacted in the tube was greater. This could potentially modify the internal geometry of the tube, reducing the ID, which could again favor greater impaction.
O'Riordan and colleagues found that variations in endotracheal tube size (7 vs. 9 mm ID) did not significantly influence delivery.(35) In mechanically ventilated tracheostomized patients, no relationship was found between deposition and the size of the tracheostomy tube ID (between 6 and 10 mm).(16) The difference in the influence of ID between our data and previous findings can be explained by the nebulizer used. O'Riordan and colleagues(16) used a nebulizer with an MMAD of 1.1±1.8 μm, whereas the MMAD of the nebulizers in our study varied between 3.3±0.4 and 3.8±0.1. Aerosol particle size is critical in determining the outcome of drug delivery, larger particles becoming trapped in the tracheostomy tube during inspiration,(18) and this could explain the influence of ID in our study. Our data show that reducing the cannula ID affected the respiratory dose more when used with the two unvented jet nebulizer configurations than with the vented one.
Variations between drug depositions observed in our study can also be explained by the significant differences in the amount of inhaled dose observed between nebulizer configurations, which could explain the variations in respiratory dose between the nebulizers. Nebulizer efficiency has previously been shown to be the predominant factor in delivering aerosol to the lung in ventilated tracheostomized patients.(16) Our data show that the quantity of inhaled dose influences the respiratory dose in tracheostomized patients. We confirm that adding a piece of corrugated tubing to the distal part of the T-piece increased the inhaled dose.(27,36,37) This can be explained by the bolus of aerosol trapped in the corrugated tube during the expiratory phase, allowing a higher quantity of aerosol to be generated during the inspiratory phase. We found that the inhaled dose with the unvented jet nebulizer with corrugated tubing was double that with the vented configuration. The unvented nebulizer alone also produced a significantly higher inhaled dose than the vented one. This can be explained by the fact that more of the dose was lost during the expiratory phase with the vented jet nebulizer than with the two unvented nebulizers.(27) Nevertheless, the two unvented jet nebulizer configurations are associated with a longer nebulization time, which could influence patient compliance with the treatment.
Our study has a number of limitations. First, it is a bench study and the results should be validated under clinical conditions. Moreover, we used only three jet nebulizer configurations and four different cannula IDs. Finally, we studied only one drug and one breathing pattern. Future studies should address the role of other variables, such as new generation nebulizers, other drugs, various breathing patterns, and other types of tracheostomy tube. However, we believe that our work provides relevant information for clinical application with spontaneously breathing tracheostomized patients.
From these results, two recommendations can be made regarding nebulization in tracheostomized patients in clinical practice. First, the inner tracheostomy cannula should be removed before nebulization in order to increase the amount of drug delivered to the patient's lungs. This is particularly relevant for patients with smaller ID tracheostomy tubes. Second, the unvented jet nebulizer with corrugated tubing should be used for nebulization through a tracheostomy tube to increase the amount of inhaled drug.
Footnotes
Acknowledgments
This work was supported by the Belgian Fonds National de la Recherche Scientifique (grant no. 3.4529.10).
Author Disclosure Statement
Laurent Vecellio is employed by la Diffusion Technique Française. Laurent Pitance, Grégory Reychler, Grégoire Delval, Hervé Reychler, and Giuseppe Liistro report no conflicts of interest.