
Abstract
Abstract
Background:
The isolated perfused rat lung (IPL) is a suitable model for studying lung-specific pharmacokinetics (PK) of inhaled drugs. So far, little has been known, however, whether the PK measured in the ex vivo organ corresponds to the PK measured in similarly exposed animals in vivo, in particular the endotracheally intubated rat (EIR). The purpose of the current research was to compare the PK of inhaled corticosteroid fluticasone furoate (FF) in the IPL and the EIR.
Method:
Aerosols of FF with mass median aerodynamic diameters ranging from 2.2 to 3.2 μm were generated with the DustGun aerosol generator. The IPL, perfused in the single-pass mode, was exposed via inhalation to 5.6 and 46 μg of FF. Following inhalation, the perfusate was repeatedly sampled for 100 min, after which the lungs were recovered for quantitation of remaining FF. Two groups of EIR were also exposed via inhalation to 7 μg of FF. One group was immediately euthanized for determination of the initial deposition of FF in the lungs. From the second group, four venous blood samples were drawn up to 4 hr after exposure. The animals were then sacrificed for determination of FF remaining in the lungs.
Results:
Following inhalation, FF was slowly disappearing from both the IPL and the lungs of the EIR, with a half-life of pulmonary retention of 4.3–4.9 hr for all three exposure series. For the low exposure levels, the concentration curve of FF in the IPL perfusate was similar in shape to that in venous blood of the EIR, with a Cmax of 1.0 and 0.8 nM for the IPL and the EIR, respectively.
Conclusions:
The results indicate that the IPL and the EIR, when used jointly in PK studies, can provide a detailed characterization of inhaled drugs or toxicants.
Introduction
So far, for single animal exposures with limited amount of test substance, instillation and insufflation methods have been most common. Liquid instillation of solutions or suspensions has been the first choice. Controlled volumes of dissolved or suspended materials are instilled into endotracheally intubated animals. 4 The advantage is an often excellent control over the administered dose. The disadvantage is an uneven distribution of poorly deagglomerated materials in the lungs, quite different from clinical inhalation or ambient air exposures. 5 A further step toward respirable aerosol exposures is the direct insufflation method, where the study material is injected with an air puff directly into the endotracheally intubated lung, either as a liquid spray 6 or as a coarse air-suspended dry powder formulation. 7 With some loss of dosing control, the distribution within the lung is improved, but is still quite uneven with greater deposition in larger airways compared with more peripheral lung compartments.7,8 For single-animal rodent exposures to respirable aerosols, there are fewer methods available. With the modern piezoelectric nebulizers, rats can be exposed to respirable aerosols of dissolved or liquid-dispersed materials. 9 For dry powder aerosols, the DustGun technology is one possibility to perform respirable aerosol exposures of single rodent lungs using small amounts of substance. 10 The combination of the isolated, ventilated, and perfused rat lung ex vivo (IPL) and the DustGun aerosol generator applied for a detailed pharmacokinetic characterization of inhaled drugs has been previously described.11,12 Whereas the IPL is an excellent model for studying the pulmonary disposition of inhaled substances in great detail,11–13 a corresponding inhalation exposure of the endotracheally intubated rat in vivo (EIR) may allow for a complete ADME (absorption, distribution, metabolism, and excretion) determination from a similar clinical-like inhalation exposure, if completed with a suitable intravenous administration of the study substance. Although pulmonary absorption of solutes in the IPL and the EIR have been compared following instillation of a coarse liquid spray, 14 few data exist in the public domain where absorption of the same substance has been compared in the two models after inhalation of respirable aerosols. In the current research, a novel active dosing system (PreciseInhale dispensing system) was introduced, where the measured aerosol concentration and the individual ventilation pattern of the exposed rat lung were used to improve the dosing precision. The overall purpose of the study was to evaluate this novel method for exposing rodent lungs one at a time to dry powder aerosols in terms of dosing precision, substance consumption, and the resulting PK profile following exposures to respirable aerosols of the corticosteroid fluticasone furoate (FF) in the IPL and EIR. Whereas the doses delivered to the rat lungs in the current study were below the label doses of 100 μg of FF used in ongoing clinical trials, 15 because rats have substantially smaller lungs and body weights compared with humans, airway drug concentrations achieved in this study were considerably higher than those that are likely in humans following powder inhalation.
The specific goals of the study were: (1) to generate aerosols of FF, to evaluate aerosol yield and particle size distribution, and to establish the correlation factor for controlling the dosing of the rat lungs ex vivo and in vivo; and (2) to expose the IPL and EIR via inhalation to controlled doses of FF and measure the pulmonary PK of FF in both exposure models.
Materials and Methods
Aerosols were generated with the DustGun technology 10 and then delivered to the exposure subjects with the PreciseInhale dispensing system (Inhalation Sciences Sweden AB, Stockholm, Sweden), containing an active aerosol dosing system integrated into the exposure control program. The control program was developed in collaboration with Flexura AB (Upplands Väsby, Sweden) and is based on the LabVIEW software platform (National Instruments, Austin, TX). Two similar crystalline formulations of the inhaled corticosteroid FF were used (provided by courtesy of AstraZeneca Ltd.): a fine-crystalline formulation (FF-A) in the IPL and a micronized crystalline formulation (FF-B) in the EIR. The materials were used without further treatment.
Aerosol characterization and preparative exposures of the corresponding rat lung phantoms
First, the particle size distribution of the tested formulations was measured for each drug formulation and load level of the aerosol generator with a nine-stage Marple cascade impactor at a final flow rate of 2 L/min. 16 Next, the operator settings for the upcoming dosing of IPL and EIR were established by performing preparative exposures of the corresponding lung phantom. The lung phantom is an in vitro filter test system designed to provide an estimate of the target aerosol dose. The exposure parameters are to be tuned so the target doses of the test compounds can be reached directly in the real lungs during the exposures with the DustGun aerosol system, without any range-finding exposures with animal lungs. The lung phantom consists of a catheter, a tracheal inhalation filter holder with a small inhalation filter (Whatman GF/F, 6 mm; Whatman plc, Maidstone, Kent, UK), and an exposure tubing system (Fig. 1). The inhalation filter is located at a position identical to that of the distal portion of the trachea of either the IPL or the intubated rat and ventilated with a modified rodent ventilator (Harvard Apparatus, Holliston, MA) at rates similar to those of the exposed lungs. During the exposure phase, aerosol was passed over the tracheal catheter at the three-way junction and collected on the end filter (Whatman GF/F, 25 mm) located immediately downstream of the tracheal catheter. The airflow through the end filter, obtained with a precision-controlled vacuum source, was maintained at approximately 2.5 times the ventilation rate of the lung phantom. 17 By keeping the Qfilter flow rate constant downstream of the catheter, the breathing pattern of the lung phantom was monitored during the exposure by the upstream pneumotachograph.
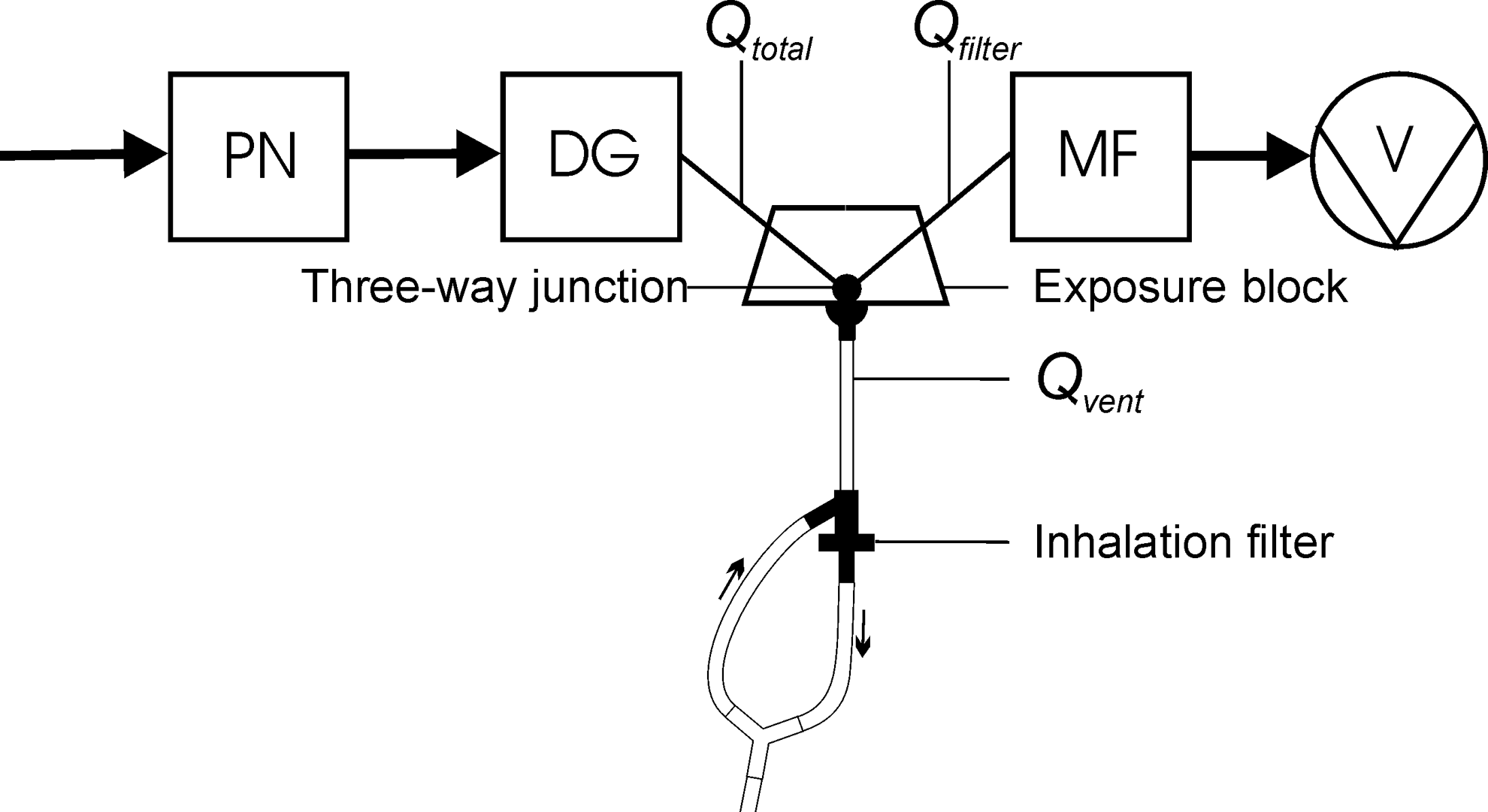
A schematic of the exposure system for the lung phantom exposures. PN, the pneumotachograph; DG, the DustGun aerosol generator; MF, the end filter; V, the vacuum pump; Qtotal, the exposure airflow; Qvent, the ventilation airflow, generated by the lung phantom ventilated with the rodent ventilator; Qfilter, the constant component of the exposure airflow. The balance of the airflow streams at the three-way junction is expressed as: Qtotal+Qvent+Qfilter=0.
During the phantom exposure, the amount of aerosol likely to be deposited on the inhalation filter (Mcas), was calculated based on the real-time measurement of the aerosol concentration by the Casella light dispersion instrument and the ventilation pattern of the lung phantom recorded by the pneumotachograph according to:
where Ccas is aerosol concentration measured by the Casella instrument (in mg/mL) and qinh is flow rate during the inhalation part of the breathing cycle (in mL/min).
After the exposure, the mass of particles deposited on the end filter (MFE) and the inhalation filter (MFI) was measured gravimetrically, and the substance correlation factor (SCF) between the gravimetric and the optical aerosol measurements was calculated according to:
where MFI is aerosol mass (in mg) deposited on the inhalation filter.
The current SCF was subsequently entered into the control program for the upcoming dosing of the corresponding exposure models. Based on the data from the lung phantom exposures, a likely deposition of aerosol during the real lung exposures (Mdep) was calculated from a suitable theoretical model such as the Multiple-Path Model of Particle Dosimetry (MPPD) v. 2.0
18
:
where Fdep is the composite fractional deposition of the aerosol (MPPD v. 2.0).
The theoretical aerosol deposition estimate (Mdep) was used to estimate the inhaled mass (Minh) likely to be required during the lung exposures for reaching the target dose. During the real lung exposures, the control program updated the cumulative inhaled mass after each breath [Minh(n)] until the target dose was reached according to:
where TV is tidal volume of each breath (mL) and Ccas is aerosol concentration measured by the Casella instrument (mg/mL).
At the inhaled target dose, the exposure cycle was automatically terminated.
Aerosol exposures of the IPL and EIR
The experiments were approved by a local ethical review board (Stockholms norra djurförsöksetiska nämnd, N256/09 and N469/09). Sprague–Dawley female rats weighing 290±22 g (mean±SD, n=18) were used in this study. For the IPL exposures ex vivo, the rats were euthanized with pentobarbital natrium (KS Hospital Pharmacy, 100 mg/kg, intraperitoneally). Lungs were prepared as described elsewhere11,19 and placed in the artificial thoracic chamber (Fig. 2). The lungs were perfused via the pulmonary artery in a single-pass mode, at a constant hydrostatic pressure of 12 cm of water. The lungs were ventilated with room air at 75 breaths/min by creating an alternating negative pressure (−0.1 to −0.8 kPa) 20 inside the artificial thoracic chamber. Except during the exposure episodes, tracheal air flow velocity and pressure inside the thoracic chamber were measured with a heated pneumotachograph (8430 Series, 0–3 L/min; Hans Rudolph, Kansas City, MO) and a differential pressure transducer (EMKA Technologies, Paris, France), respectively. The physiological lung-function variables—tidal volume (TV), dynamic lung compliance (Cdyn) and lung conductance (Gaw)—were calculated online by a data acquisition system with the software IOX v. 6.1a (EMKA Technologies). The perfusate flow rate after passage through the lung (Qperf) was measured gravimetrically. The normal stability was achieved concerning all the physiological parameters measured. The baseline values were as follows: TV, 1.8±0.1 mL; Gaw, 97.0±15.9 mL/sec/kPa; Cdyn, 3.0±0.3 mL/kPa; and Qperf, 34.2±4.2 mL/min (average±SD, N=8). The lungs were allowed to stabilize for 30 min prior to aerosol exposures. Before aerosol exposures, the pneumotachograph was removed and the three-way junction of the exposure line was connected to the upper part of the tracheal catheter of the IPL, thus creating a closed system (Fig. 1). The aerosol generation cycle was started by the exposure control program. Two groups of four rat lungs were exposed to target doses of 5 and 50 μg, respectively, deposited per lung of FF-A (Table 1). After exposure, the lungs were maintained for a 100-min perfusate collection period, during which 30-sec perfusate samples were collected with a custom-made sample collector. The midpoints of the sampling intervals were 0, 1, 2.5, 4, 6, 9, 15, 30, 60, and 100 min. At the end of the perfusion period, the lungs were harvested for measuring the total amount of FF-A remaining in the lung.
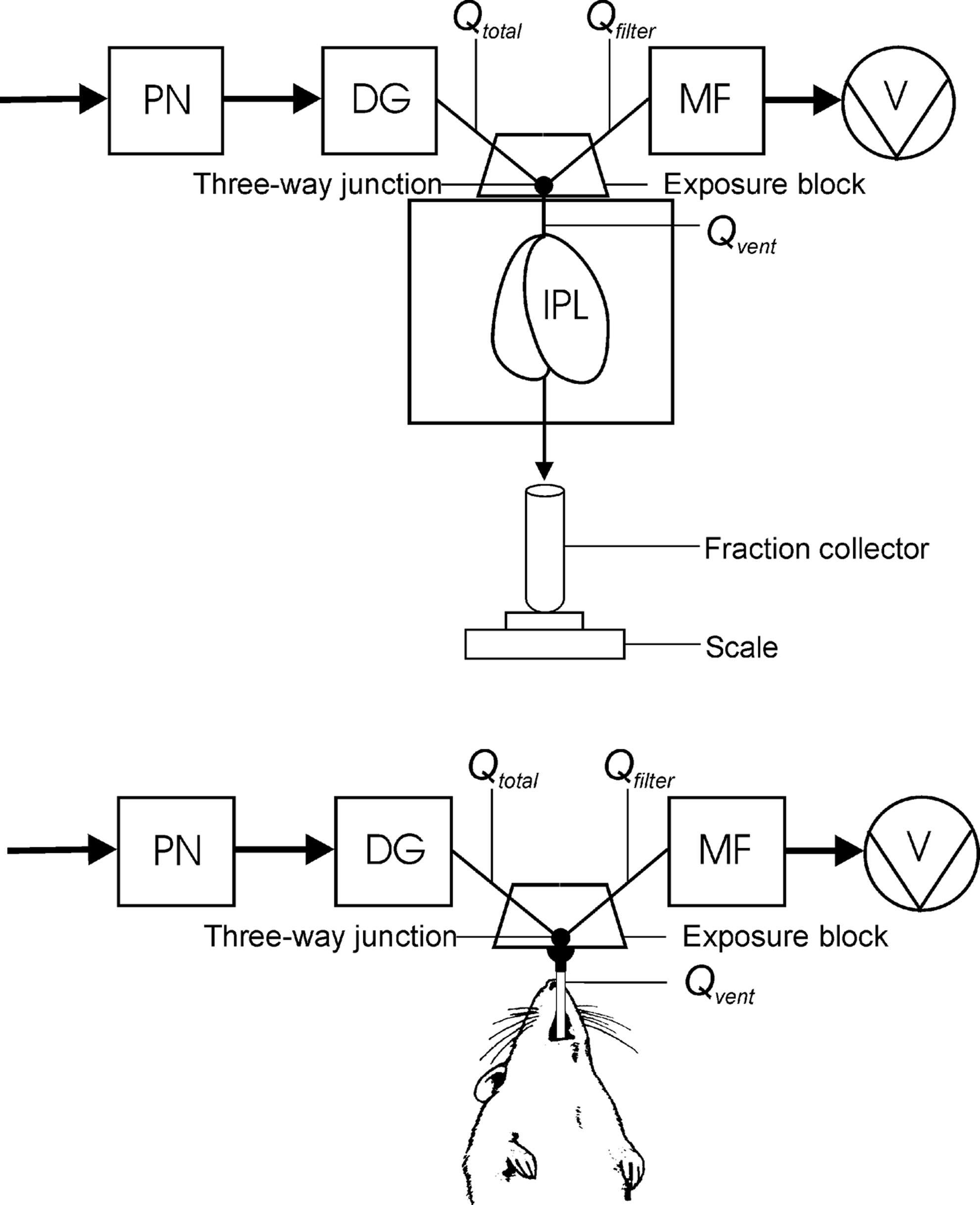
Exposure models tested: the isolated, ventilated, and perfused lung of the rat (upper panel) and the endotracheally intubated rat (lower panel) connected to the exposure platform.
Between the optical and gravimetrical aerosol measurements.
Rats for endotracheal exposures in vivo were anesthetized with Hypnorm+midazolam (solution containing 1 part Hypnorm+1 part midazolam+2 parts water; intraperitonal injection, 0.27 mL/100 g body weight) and suspended in a supinal position on an adjustable table by stringing a wire attached to the table behind the upper incisors (Fig. 2). Animals were placed on a heating pad with a rectal probe in order to control body temperature during the experiment. Endotracheal intubation was performed under a good visual control using a custom-made device as described elsewhere.21–23 A PTFE catheter (outer diameter 2.08 mm, inner diameter 1.68 mm, length 60 mm) was used as an intubation catheter. A ball joint connector was clamped to the proximal end of the tracheal catheter and then connected to the exposure line at the three-way junction using bayonet clips (Fig. 2). A superimposed flow rate was adjusted to approximately 2.5 times the ventilation rate of the anesthetized rat using a constant downstream vacuum source. At this point, the exposure control program calculated the TV and breathing rate in real time. The rat was monitored for 5 min prior to aerosol exposure to ensure a stable spontaneous breathing. The baseline values were as follows: TV, 1.2±0.1 mL; breathing rate, 135±21 breaths/min (average±SD, N=10). The aerosol generation cycle was started with the computer-controlled trigger, and the exposure sequence was executed.
The EIR was exposed to 20 μg/kg FF-B (6.4±0.7 μg; average±SD, N=10) in two groups with five animals in each group. The first group was sacrificed immediately after exposure to determine initial deposition, by measuring the total amount of FF-B remaining in the lungs. The second group of identically exposed rats was maintained intubated and under anesthesia for 240 min after exposure. During this time period, 0.1 mL of venous blood was sampled from the dorsal metatarsal vein at 1.2, 18, 60, and 240 min. The rats were then sacrificed, and the lungs were harvested for measuring the total amount of FF-B remaining in the lungs. FF was quantitated in perfusate, blood, and tissues, using liquid chromatography–tandem mass spectrometry. In-house (AstraZeneca R&D) validated methods for the different matrices were employed, and all samples were evaluated using a seven-point standard curve, which was diluted in the same matrix as the samples.
Pharmacokinetic evaluation
With the IPL, single-pass perfusate was sampled at t0, t1, t2,…tn min midpoint in the sampling intervals, giving solute concentrations of c0, c1, c2,.cn (μg/mL). Each sample interval has a length of Δt (min). The perfusate content of the vials was weighed with weights of m0, m1, m2,…mn (g), and the density of the perfusate was ρp (g/mL). The peak concentration of the test compound in the perfusate (Cmax) and the time at which the peak concentration occurred (tmax) were established. The cumulative clearance was then calculated by trapezoid integration according to:
Following cumulation, the total mass of the initially deposited dose was calculated according to:
where MDEP is total mass of inhaled drug initially deposited in the lungs (μg), Mperf is mass of drug clearing with the perfusate (μg), and Mtissue is mass of drug remaining in the lung tissues at the end of the perfusion period (μg).
Also, the fraction retained over time of the initially deposited dose in the lungs (Fractionret) was calculated according to:
The fraction-retained data were also fitted to a first-order decay function for calculating the retention half-life in the lungs. For the EIR, the lung-retention data at time 0 and 240 min were fitted to a first-order decay function for calculating the half-life of retention in the lungs of the live rat. Because too few blood samples were drawn from this group of rats, the time resolution was too poor for determining the tmax of the time period of study.
Results
For the exposures of the IPL and the EIR, fine aerosols were generated from FF-A and FF-B, respectively, with a mass median aerodynamic diameter (MMAD) ranging from 2.2 to 3.2 μm (Fig. 3). The micronized crystalline material (FF-B) was somewhat easier to deagglomerate than the fine crystalline material (FF-A), and the particle size of the FF-A aerosol increased slightly with increasing powder load of the DustGun generator (Fig. 3). Yet the aerosols were mostly well dispersed with relatively few larger agglomerates. The key parameters of the exposures are shown in Table 1. The aerosol concentrations and the corresponding cumulative amounts of aerosol inhaled by the IPL (low dose) and the EIR are shown in Figure 4. The response time of the aerosol concentration in the exposure line was relatively rapid, with a zero-to-full or a full-to-zero concentration shift occurring within 10 sec of valve actuations. This rapid response is important when using an active dose-control system. The precision of dosing was considerably better for the IPL with a less than±10% SD for the deposited dose compared with±27% SD for the intubated rats. The total substance consumption of both formulations for running the preparative aerosol experiments and exposing in total 18 rat lungs was approximately 55 mg. The overall lung deposition yield was 0.25% based on the total substance consumption for both preparatory and lung exposures. This parameter increased to 2.5% when only the lung dosing exposures were included. If necessary, about 30% of the used drug can be recovered from the uncontaminated fallout in the holding chamber.
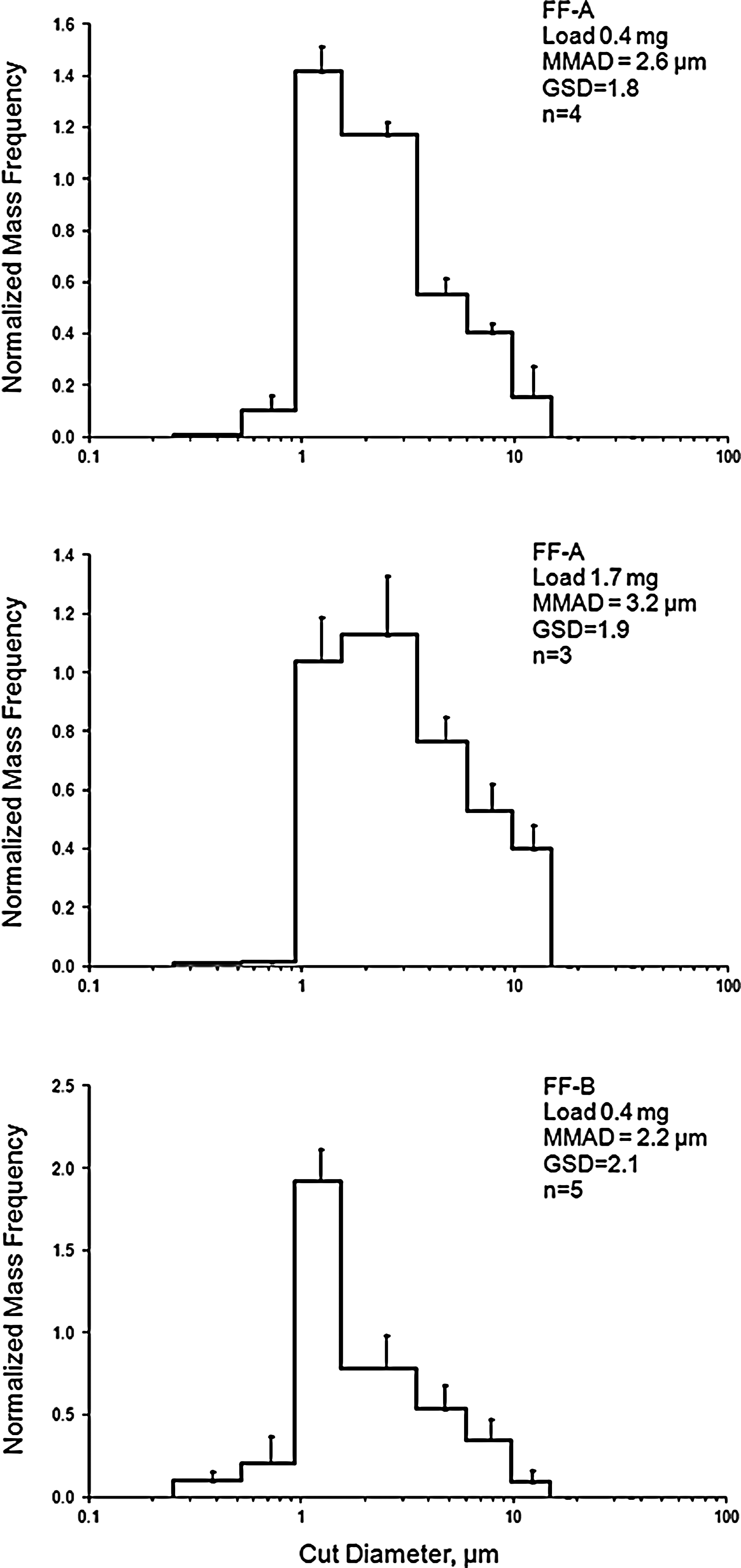
The particle size distribution of the aerosolized FF: the crystallinic material (FF-A) and the micronized material (FF-B).
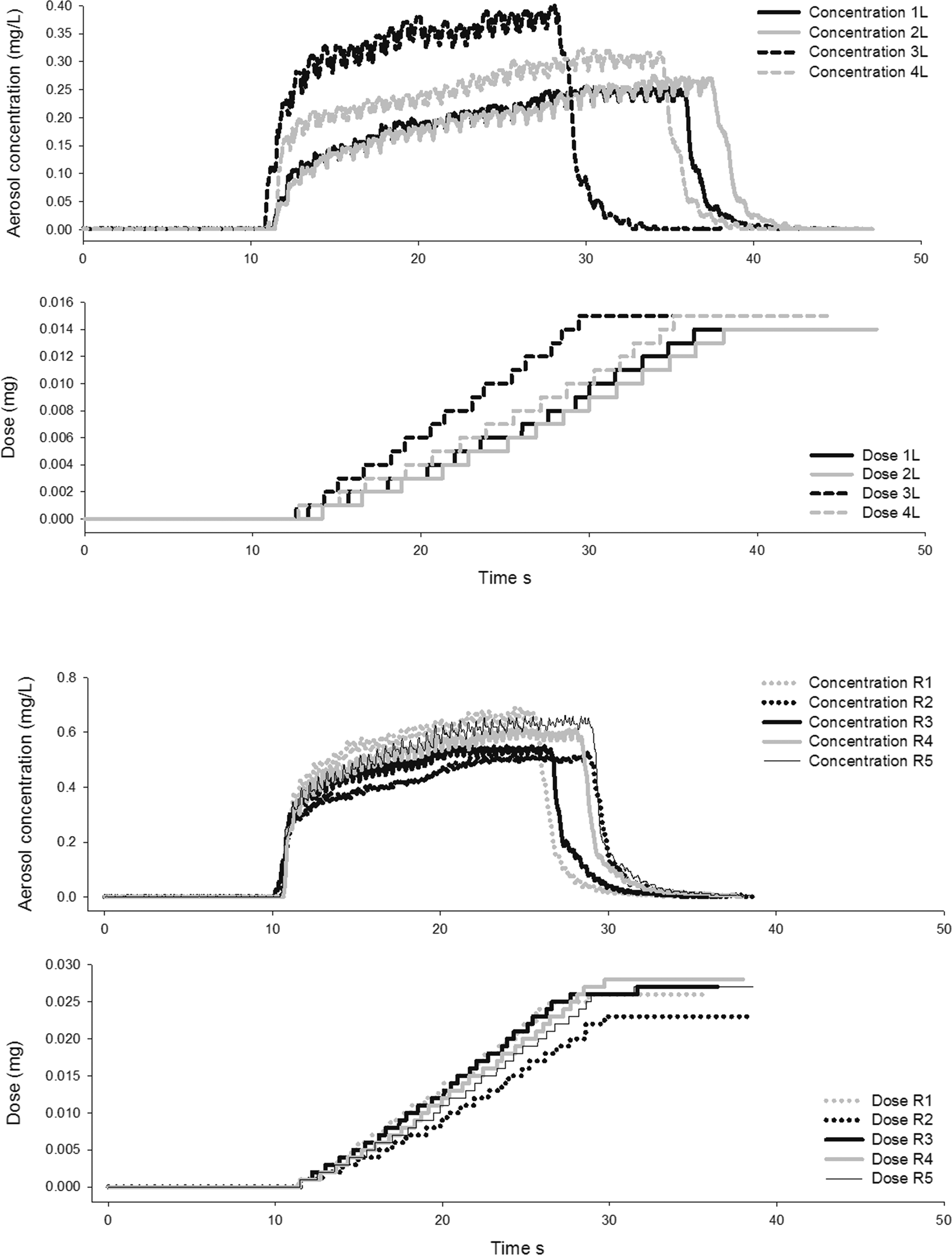
Aerosol concentrations and the recorded cumulative inhaled dose during the low dose exposures of the IPL exposed to FF-A (upper panel) and the EIR exposed to FF-B (lower panel). Note that the IPL was exposed to a fixed lung dose, whereas the intubated rat was exposed to a fixed dose per body weight.
The concentrations of FF in perfusate and blood after the exposures of the IPL and EIR are shown in Figure 5. Even if the sampling points for perfusate and blood in the two exposure models were located on either side in relation to the systemic circulation, the shapes of the FF concentration curves were quite similar. The fractional retention of FF in the lungs after the exposures is shown in Figure 6. For the IPL, lung retention at the intermediary time points was calculated from the overall mass balance of the system. These retention curves, nearly identical for the two dose levels, were only slightly more curved than a monoexponential retention curve. Therefore, as a reasonable approximation, the two time points of the EIR exposures were fitted to a monoexponential retention curve (Fig. 6). Although the assumptions of this approximation will be further examined in the discussion, the fractional lung retention of FF so obtained was quite similar for both exposure models (Fig. 6), with a measured half-life of pulmonary retention averaging 4.6 hr (Table 2).

The concentration of FF as a function of time: FF-A in the single-pass perfusate of the IPL and FF-B in blood from the systemic circulation of the EIR.
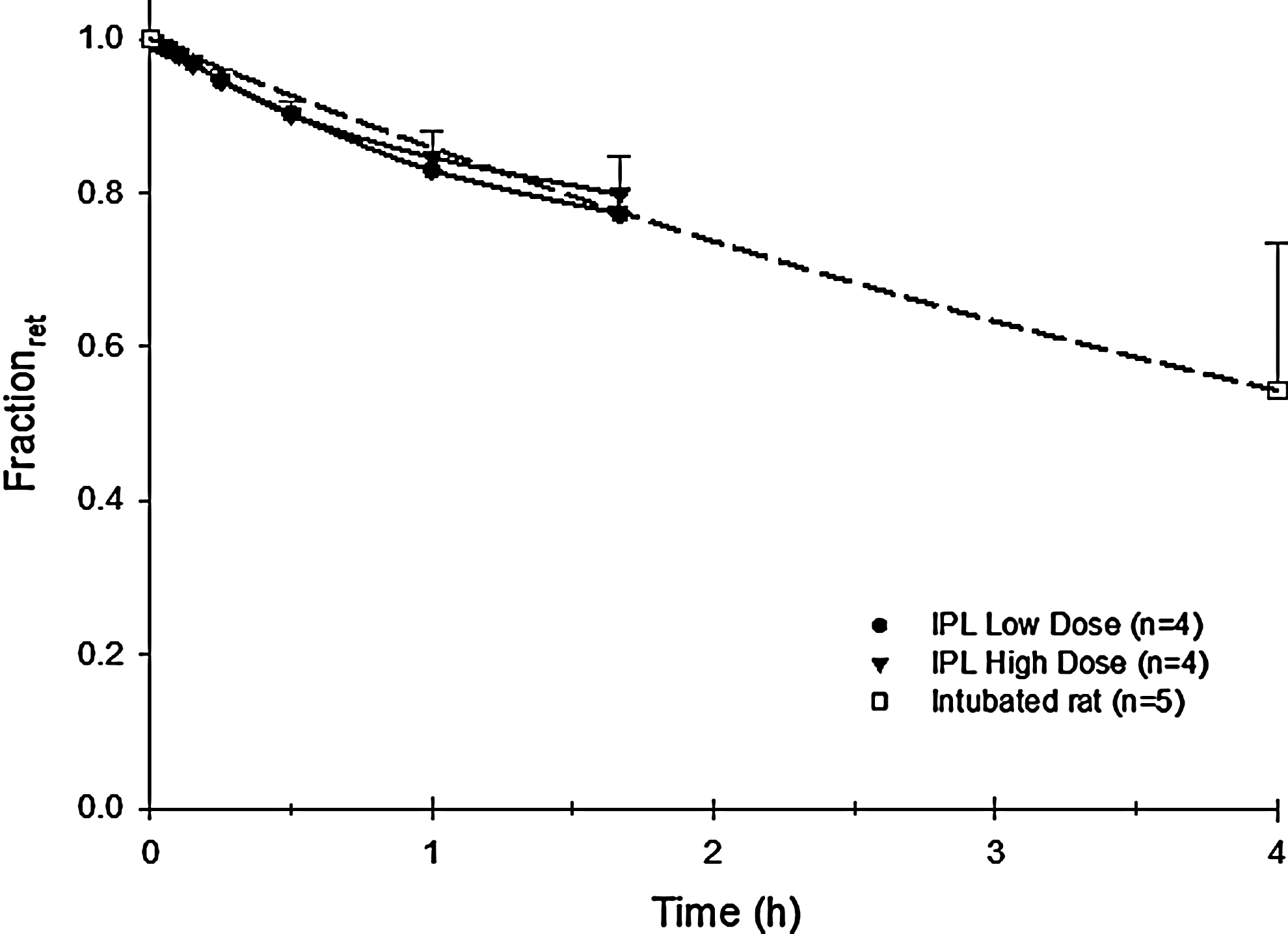
Fractional retention of inhaled FF in the IPL and the EIR as a function of time. The measured lung burdens of the intubated rats killed immediately and 4 hr after exposure have been fitted to an exponential function.
tmax, the time at which the peak concentration occurred; Cmax, the peak concentration of drug in the perfusate or blood; t1/2
Too few time points to be meaningful.
Discussion
With the current platform, different exposure models were exposed to identically generated aerosols, using only small amounts of test substance. The active dosing system was accurate in dispensing aerosol from the holding chamber based on the aerosol concentration and ventilation pattern of the exposure models (Fig 4). The quantitation of powder for loading the generator was therefore not very critical. However, increasing substance load may increase the aerodynamic particle size of the generated aerosols (Fig. 3), so both the particle size distribution and the SCF needed to be determined for each main load level of powder used in the generator. When the achieved doses in the two exposure models are compared, dosing of the IPL was more accurate than dosing of the intubated rat. The longer tracheal catheter made of a polymer material in the case of the intubated rat may cause variable substance losses to the tube walls during the exposures. As an alternative with shorter aerosol conduits, nose-only exposures can be performed in conscious rats with the current exposure system. Despite the advantage of not requiring anesthesia of the animals, the great disadvantage of nose-only exposures is the typical 60–90% deposition of aerosol occurring in the nasal airways.24–25 As a consequence, larger fractions of substance may be absorbed from the nasal mucosa and the gastrointestinal tract, thereby compromising an intended pulmonary disposition study. Because the exposed rats remained endotracheally intubated throughout the blood sampling period, there was most likely just a minimal redistribution of FF with mucociliary clearance to the gastrointestinal tract. It is likely that this material was instead accumulated at the blocking catheter in the trachea similar to the IPL exposures. However, there the material was still subject to blood-borne absorption in the live rat as opposed to the situation in the unperfused extrapulmonary airways of the IPL.
Compared with existing technologies, the current dry powder system provides some notable advantages: respirable aerosols are inhaled during either spontaneous or a similar physiologically relevant breathing pattern, giving high respirability expressed as a high lung lobar to total pulmonary deposition (LLD). 8 For exposures of the IPL to diesel soot (MMAD=0.52 μm) with the DustGun generator, the LLD was shown to be 97%. 10 However, the LLD is likely to decrease somewhat with increasing MMAD according to aerosol aerodynamics. Although the substance utilization may be slightly higher for nebulization methods owing to recirculation of feed liquid, 9 the dose rate will be considerably higher and the required period of anesthesia correspondingly shorter for the dry powder inhalation method, when only the neat substance is aerosolized. In the current study, a 50-μg deposited dose needed a 3-min exposure period when two aerosol generation cycles were required. This period is likely to double to 6 min for a 100-μg deposited dose. Another advantage with powder aerosol inhalation is that sparingly soluble substances such as FF can be delivered neat to the lungs as respirable aerosols without the need for cosolvents or dispersing agents. For chemicals that are difficult to obtain as a micronized powder, a further alternative in the preclinic is to coat such a substance onto an inert carrier particle of mesoporous silica of respirable size at concentrations up to 20% by weight. 26
The pulmonary PK of FF combines a rapid initial breakthrough to the circulation (tmax<5 min) with a slower second phase typical of a sparingly soluble substance, where a slow dissolution/absorption process extends the perfusate concentration curve into a plateau (Fig. 5). For the two IPL exposure series with an eightfold difference in dose, the fraction retained over time was not significantly different. This indicates that the surface density of deposition of FF on the airway walls was not high enough for the dissolving respirable particles to significantly interact and reduce the fractional dissolution and absorption rate in the lungs. If the 46-μg dose of FF was converted to 2.5-μm (average MMAD) unit density spheres of drug, they would number 5.6 million in total. Evenly deposited over the approximate 1-m 2 surface area of the rat lung, 27 the average distance between the particles would be on the order of 400 μm. Even if considerably higher local densities of deposition are likely to occur in the bronchial airways, the general picture emerging is that even at this superclinical dose of FF, dissolution and absorption proceeded at a fractional rate independent of dose, provided that the particle size distribution remained essentially the same with increasing dose. Clinical data for fluticasone propionate point in the same direction, 28 so the PK data obtained from the relatively high exposures levels of the current study may be clinically relevant.
Recent results with liquid instillation and powder insufflation of fluticasone propionate in rats also support this conclusion. When only about 10% of the powder dose constituted a fine particle fraction penetrating to the lower airways, there was a predicted 8.2-hr absorption half-time of the dry powder in the rat lung. 29 In the current study with FF, where more than 90% of the administered dose was fine-particle aerosol penetrating to the lower airways, the absorption half-time in the rat lung was only half that of insufflated fluticasone propionate, despite the fact that the propionate is approximately twice as soluble in water as the furoate. 30 It is likely that if administered as a fine-particle aerosol, the absorption half-time of fluticasone propionate would be shorter and more like that of the corresponding liquid-instilled substance. 29 In the current study, even if micronization influenced aerosol particle size (2.2–3.2 μm MMAD; Fig. 3), we do not expect that the PK was significantly influenced by the property differences of the two powders used in these experiments.
We based our argument that the fractional retention of FF in both exposure models proceeded at similar rates on the following rationale. For low-solubility, lipophilic solutes, most of resistance to absorptive mass transfer from the airways of the lungs is controlled by the dissolution and diffusion of solute from the particles deposited at the air/lining layer interface into the capillary network immediately below the airway epithelium. This phenomenon was investigated previously, using an experimentally validated PK model for absorption of similarly lipophilic solutes in the bronchial airways. 31 Because near-sink conditions are likely to exist in the rich subepithelial capillaries under the deposited particles, the concentration of such a solute sampled in either the single-pass perfusate of the IPL or the arterial blood of the intact rat should be determined both by the level of dilution provided by the perfusion flow rate and, in the living animal, by the concentration of solute that may enter the lungs with the venous blood. 32 The fact that the concentration curves of FF in perfusate and blood had the same general shape in the two exposure models (Fig. 5), combined with the known rapid hepatic clearance in the rat of 75 mL/min (data on file, AstraZeneca), implied that FF was absorbed from the lungs at similar rates in both models. This would support the assumption (Fig. 6) that monoexponential clearance of FF from the in vivo rat lung occurred between 0 and 4 hr and that this correctly represented retention of FF in the lung over time. However, despite the similar lung retention of FF measured in the two exposures models, it is only in the IPL model that the absorption rate in the lungs can be deduced from the substance concentration in the perfusate and where lung retention can be calculated through a mass balance in a single group of exposed lungs. In the in vivo model, measuring pulmonary absorption rate either requires repeated simultaneous sampling of blood on both the venous and arterial sides of the circulation in a single group of animals, 32 which is not possible in a small mammal, or retention data must be obtained from lungs in groups of identically exposed animals analyzed at different time points after exposure.
Of the two possible modes of supplying the IPL with perfusate—the currently used single-pass mode or the recirculation mode 33 —it would seem that the single-pass mode has the greater advantage. Clearly, one drawback of the single-pass mode is the larger 4-L perfusate volume required to maintain the IPL for a 2-hr single-pass experiment, compared with some hundred milliliters in the recirculation mode. On the other hand, one substantial drawback of the recirculation mode, particularly pronounced for lipophilic solutes, is the keen partitioning of such solutes from the perfusate into the more lipoid lung tissues. Consequently, as drug accumulates in perfusate, it may reach equilibrium with the lung tissues. This may artificially halt the clearance of drug with perfusate from the lungs at considerable lung retention levels. 33 This is not likely to happen with the single-pass IPL or with the intubated rat, because of the continuous elimination of drug from the lungs via the perfusate or blood, respectively. Another great advantage with the single-pass IPL is the translatability and correspondence of data between the single-pass IPL and the intubated rat. Parameters such as Cmax, tmax, and t1/2 have a closer relationship in the two exposure models when the IPL is not perfused in the recirculation mode. Hence, data from this study encourage the measurement of PK both in the single-pass IPL and in intubated rodents. Furthermore, the results call for the establishment and validation of more detailed physiologically based pharmacokinetic (PBPK) models describing the mechanisms of pulmonary absorption of inhaled drugs. The detailed kinetics of absorption that can be derived from studies in the IPL can greatly improve the accuracy of full-body PBPK models for soluble inhalants in the rat in vivo. Because the live animals are exposed during spontaneous breathing under light anesthesia, they can be as easily recovered as following a conventional endotracheal liquid instillation procedure. 5 The set of precision data from dry powder inhalation exposures described here is typical of those that can be obtained from the two complementary exposure models; two dose levels were studied by using 24 animals and spending less than 100 mg of drug substance (FF).
In conclusion, the current study demonstrated an excellent correlation of lung PK between intact animals and the IPL after the administration of small portions of respirable dry powder aerosols. Although only small amounts of test substance are consumed, this may result in earlier access to pharmacokinetic data from dry powder inhalation exposures than previously possible and, in combination with PBPK simulations, more accurate predictions of future human inhalation exposures in the clinic.
Footnotes
Acknowledgments
This study was part of a postdoctoral collaboration for Dr. Ewing between AstraZeneca R&D, Inhalation Sciences Sweden AB, and Karolinska Institutet.
Author Disclosure Statement
Drs. Gerde and Ryrfeldt are minority shareholders in Inhalation Sciences Sweden AB.