
Abstract
Abstract
Background:
Good compliance to the prescribed dosing regimen and inhaler instructions for use are critical for asthma/chronic obstructive pulmonary disease (COPD) patients to achieve good control of their disease. We investigated the extent to which a system comprising porous particles delivered with a passive dry powder inhaler could be designed to achieve significant reductions in dose inhalation errors.
Methods:
Porous placebo particles were prepared by an emulsion-based spray-drying method (PulmoSphere® technology). The formulations were administered as dry powders with a portable, blister-based dry powder inhaler (Simoon Inhaler). The inhalation profiles of 69 asthma/COPD subjects were determined with an inhaler simulator with resistance comparable to that of the Simoon Inhaler. Powder emptying from the device was assessed by laser photometry. Aerosol performance was assessed on a Next Generation Impactor, and with the idealized Alberta mouth-throat model using both square-wave and subject-inhalation profiles generated in the breathing study.
Results:
Virtually all subjects could achieve a pressure drop of at least 1 kPa and an inhaled volume of at least 500 mL with the Simoon Inhaler. In vitro measures of particle deposition were found to be largely independent of the inhalation maneuver (flow rate, inhaled volume, ramp time) across the broad range of inhalation profiles observed in the breathing study. The rapid emptying of powder from the Simoon Inhaler minimizes the impact of dose-related errors, such as failure to exhale before inhalation and failure to breath-hold post inhalation.
Conclusions:
Inertial impaction that is largely independent of a subject's inhalation maneuver can be achieved with a drug/device combination product comprising a porous particle formulation and blister-based inhaler.
Introduction
Inhaler errors are defined as “critical” if they can substantially impact dose delivery to the lungs. In a large inhaler handling study encompassing nearly 4,000 subjects, Molimard et al.(1) found that about half of the subjects had at least one critical error. More recently, Rootmensen et al.(7) found that 40% of asthma and COPD patients made at least one critical error, with prefilled dry powder devices the most likely to be used correctly.
Dixon and Simpson(4) classified critical errors into three categories: (a) failure-to-use errors; (b) dose preparation errors; and (c) dose inhalation errors. Failure-to-use errors are related to a number of diverse factors. As pointed out by Everard,(10) poor regimen compliance (also known as adherence) is common to all therapeutic areas. Poor adherence does not correlate with age, socioeconomic status, sex, disease severity, risk of death, or knowledge of disease. Failure-to-use errors include simply forgetting to take a dose, a desire to not be on a regular medication, a failure to understand the importance of regular therapy, or a feeling of well-being (no longer need the drug). There are also failure-to-use errors related to the costs of treatment, and the complexity of a treatment regimen, which may require the patient to inhale multiple medications from multiple devices, several times daily. For example, fixed dose combinations comprising bronchodilators and inhaled corticosteroids in a single inhaler (e.g., Advair®; GSK, Research Triangle Park, NC), simplify the treatment regimen, thereby improving patient compliance.(12–15) Fixed dose combinations comprising once-daily medicines may further help in this regard.
Dose preparation errors are related to the number and complexity of steps required to prepare the dose to be inhaled. These errors are highly device-dependent. According to Everard,(10) poor device compliance may be due to a lack of competence (the inability to use the device correctly) or contrivance (that is, having the competence to use a device correctly, but contriving to use it in a manner that fails to effectively deliver drug to the lungs). In their simplest embodiment, device use instructions may be “open-inhale-close,” where the inhalation maneuver triggers dose release (i.e., breath actuation). In currently marketed multiple-dose dry powder inhalers (DPI), an additional step to prepare the dose is required. In Diskus®, this involves moving a lever, whereas in Turbuhaler®, it requires a twist of the device.
Dose inhalation errors include device-independent and device-dependent errors. Device-independent errors include errors related to the instructions for use (e.g., failure to exhale before inhalation, and failure to breath-hold). These are, in fact, the two most common critical errors observed by Molimard et al.(1) Device-dependent errors include errors related to variations in the inhalation profile [e.g., peak inspiratory flow rates (PIF) too low to achieve effective powder deagglomeration, inhaled volumes too small to empty the powder contents from a dose receptacle, or poor coupling of powder-emptying to peak flow rates].
The key metrics that define the inhalation profile are captured in Figure 1. Subjects use muscles in their diaphragm to create a negative pressure in the inhaler, typically measured in kilopascals. The maximum inspiratory pressure (MIP) that can be achieved is not strongly correlated with the severity of lung disease.(16–22) A better correlation is seen with a subject's age, with the youngest and oldest of subjects similarly unable to generate as high a MIP as a typical adult. The PIF will depend on the subject's inspiratory effort (e.g., forceful or comfortable) and the resistance of the device.(16) The relationship between device resistance (R), pressure drop across the inhaler (ΔP), and flow rate (Q) is given by Equation 1:
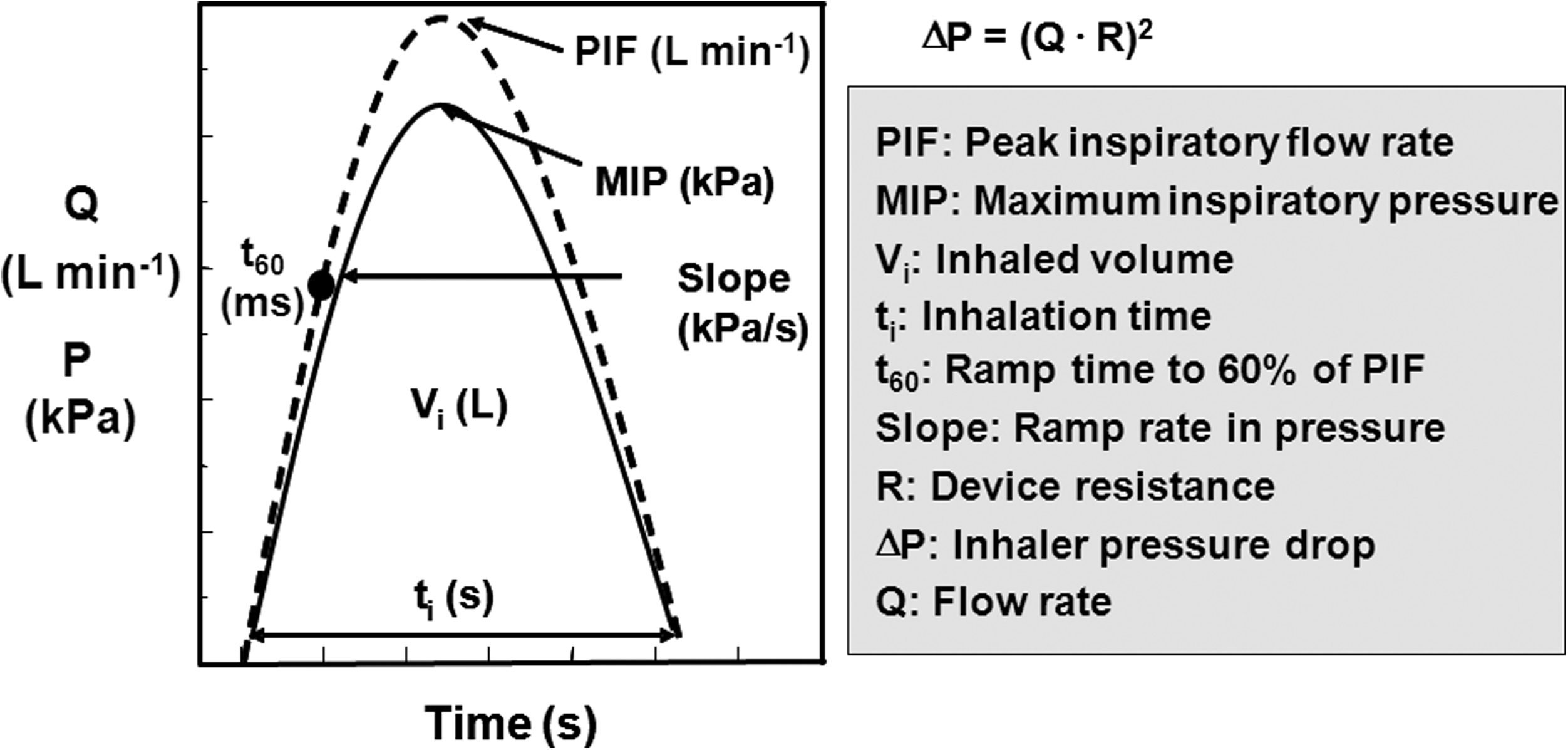
Plot of the key variables that define a subject's inhalation profile (adapted from Ref. 2).
Although subjects may be able to generate significant MIP and PIF values when asked to inhale forcefully through a device, they will often later revert to breathing comfortably through a device in practice.(16,19,20) DeBoer et al. suggest that breathing comfortably occurs at about 0.55 MIP for a wide range of subjects, including healthy volunteers and subjects with lung disease.(19,20) For a given passive dry powder inhaler, higher PIF values generally increase dispersion energy within the device.
Although the industry generally focuses on the PIF required for optimal delivery of a given drug product as a key differentiating factor, this does not tell the whole story with regards to how effectively the product can be delivered across a range of patients. Instead, it is instructive to assess flow-rate dependence in terms of variations in the fine particle dose with the pressure drop across the inhaler. This makes it possible to directly compare the flow-rate dependence of devices with different resistances, where the ranges of flow rates to be tested differ markedly.
Other metrics of importance in the inhalation profile include the inhaled volume (Vi), the ramp time to 60% of peak flow (t60), and the total inhalation time (ti). The inhaled volume varies with a subject's age and the severity of their disease. The key for ensuring effective delivery of therapy with a dry powder inhaler is that there is sufficient inhaled volume to deliver the dispersed powder to the airways. This includes the airflow required to empty powder from the blister or other powder receptacle, any airflow required to create and disperse the aerosol, and sufficient chase air to carry the drug past the subject's oropharynx and into the lungs. It is critical that the receptacle emptying time not be too short, however, as rapid emptying may result in a reduced lung dose due to powder emptying before flow rates are established that are sufficiently high to effectively disperse the powder.(11,19,20)
This article will focus on how drug/device combination products comprising porous particles (i.e., PulmoSphere® formulations) and a portable blister-based dry powder inhaler (Simoon) can dramatically reduce dose inhalation errors. Indeed, the goal is simple: for subjects to receive the same lung dose of medication independent of how they inhale through the device. For the purposes of this article, drug delivery is assessed using in vitro methods (i.e., the Next Generation Impactor and the idealized Alberta mouth-throat model).
Materials and Methods
Materials
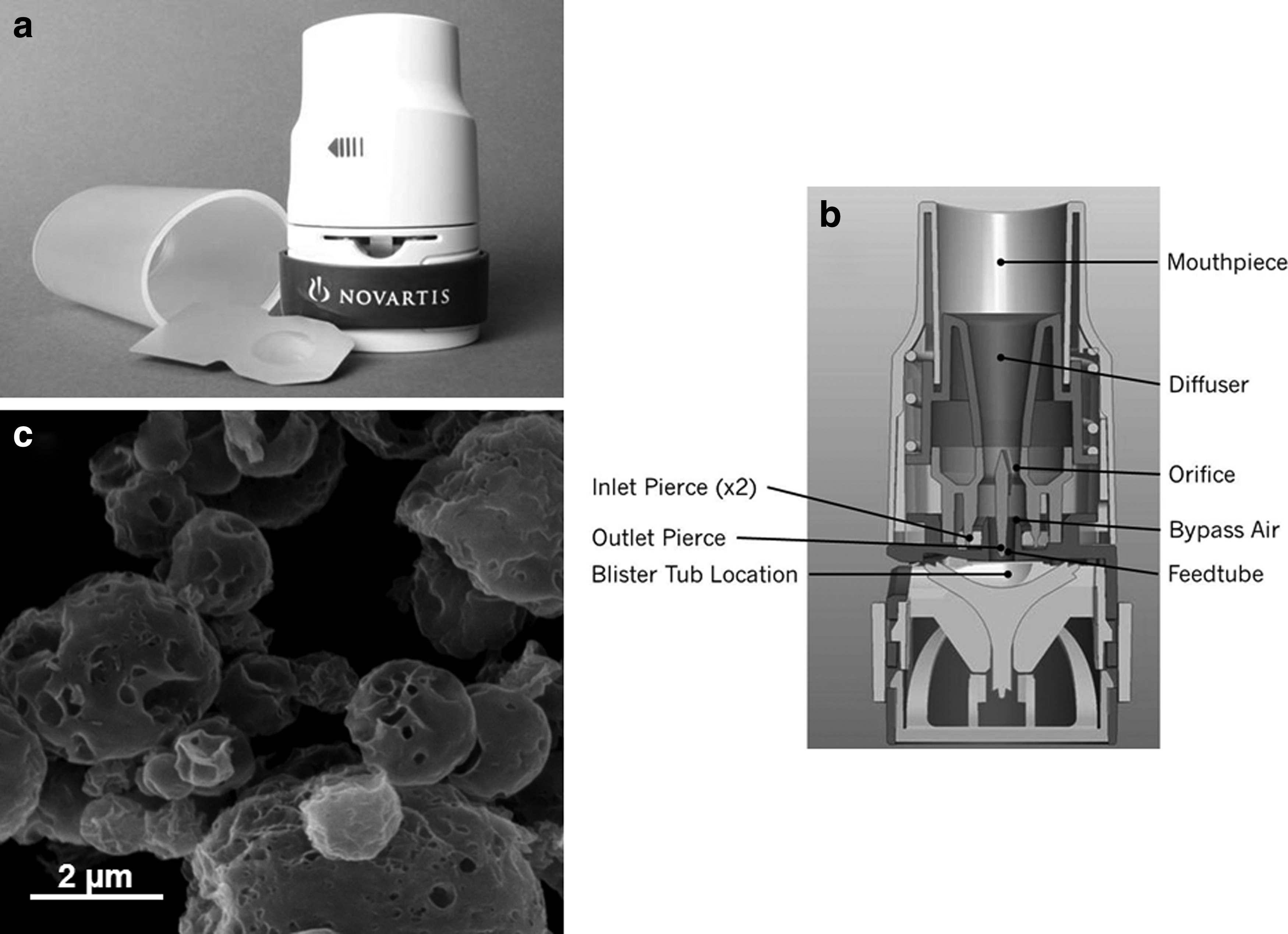
A PulmoSphere placebo powder was manufactured by spray-drying a feedstock comprising an oil-in-water emulsion on a Niro PSD-1 scale spray-dryer (Copenhagen, Denmark) equipped with custom atomization and collection hardware.(23) The porous particles exhibit the sponge-like morphology characteristic of the PulmoSphere process (Fig. 2).(24–27) The particles are comprised of a 2:1 molar ratio of distearoylphosphatidylcholine (DSPC):calcium chloride. The size of the particles (median diameter=3.50 μm) and their tapped density (ρtap=0.04 g cm–3) are controlled by the atomization conditions, drying rate, and the volume fraction of oil in the emulsion. The oil phase is comprised of perfluorooctyl bromide (Atofina, Paris, France). DSPC and calcium chloride were obtained from Corden Pharma (Cambridge, MA) and J.T.Baker (Phillipsburg, NJ), respectively. Additional details regarding the PulmoSphere manufacturing process have been described previously.(24–27)
The drug/device combination was comprised of a spray-dried powder and a portable, unit dose, blister-based inhaler:
Owing to their high potency, the drug loading of asthma and COPD therapeutics in PulmoSphere formulations is generally low (<10%). In this situation, the aerosol properties of the formulation are controlled not by the physicochemical properties of the drug substance, but by the surface composition and morphology of the particles. Thus, the placebo formulation studied herein represents a good surrogate for formulations of asthma and COPD therapeutics incorporated in PulmoSphere formulations.
Spray-dried powders were filled into foil–foil blisters with a proprietary volumetric drum filler (Novartis Card Filler, San Carlos, CA). Key elements of the filler include a powder feed trough used to produce a uniform, fluidized powder bed above a rotatable metal drum containing a row of cylindrical cavities of precise volume. Powder is metered into the cavity by application of a vacuum. The drum is then rotated and pressure applied to eject a compressed powder puck into a row of laminated foil blisters positioned below the drum. A laminated foil lid stock is then heat-sealed onto the card. Filled blisters are conditioned with a pulse of ultrasonic energy to redisperse the compressed pucks. Finally, individual blisters are cut from the card. The nominal fill masses tested were 1 mg or 2 mg. The variability associated with the filling operation was ≤3%.
The Simoon Inhaler (Fig. 2) is a blister-based, unit dose, portable, passive, dry powder inhaler.(28) For this study, devices had a resistance between 0.17 and 0.20 cm H2O0.5 LPM–1 (where LPM is liters per minute). The device components utilized to extract (fluidize), deagglomerate, and deliver the dose are modular in design, and this module is referred to as the “aerosol engine.” The Simoon aerosol engine can be adjusted to accommodate drug formulations with varying physicochemical properties. During inhalation, the total air flow is divided into two flow paths within the engine module: the bypass flow and the blister flow. In the current embodiment, approximately 95% of the total air volume goes through the bypass. Between the bypass air inlet and the final restriction (orifice), high-velocity air flow is created during subject inhalation. This creates a pressure drop on the upstream side of the restriction. The outlet holes pierced in the blister expose the drug to this pressure differential. A small fraction of the total airflow (∼5%) is utilized to fluidize powder and empty it from the blister receptacle, carrying it into the high-speed flow stream comprising bypass air. The resistance of the device is controlled by the diameter of the restriction.
Deagglomeration of the bulk powder occurs in two ways: via turbulent shear created at the edges of the outlet hole in the drug package, and via high-velocity shear on the particles created at the restriction. Typically, devices with low resistance and unconstrained diffusion create a core stream of high-speed particles, resulting in high powder losses and increased patient variability due to high particle deposition in the subject's mouth and throat. The Simoon engine module was designed to achieve high lung delivery with reduced oropharyngeal deposition. This is accomplished by incorporation of three critical design features in the Simoon engine. First, it provides a homogeneous particle distribution across the exit plane of the mouthpiece. This eliminates production of a core stream of high-velocity particles, greatly reducing losses and variability due to impaction in the mouth and throat. Second, the engine design maximizes the change in velocity between the high-speed velocity at the air path restriction and the exit plane of the device. Finally, the design provides a homogeneous plume velocity for the dispersed powder across the exit plane.
The low flow rates through the blister (often on the order of just 1 LPM at 1 kPa pressure drops) make the choice of powder highly critical. Spheronized particles or lactose blends may be less suitable for this type of device due to the higher flow rates required to effectively fluidize and disperse the powder.
Breathing studies in subjects with asthma and COPD
A clinical study (breathing study 1) was conducted to assess the inspiratory flow profiles of asthma and COPD subjects when asked to inhale through an inhaler simulator of comparable resistance, R=0.17 cm H2O1/2 LPM–1 to the Simoon Inhaler. A total of 69 patients of varying age and disease severity completed the study. Inhalation profiles were recorded using an inhaler simulator, a flow meter (TSI Inc., Shoreview, MN), and a laptop computer (Dell, Round Rock, TX) with customized LabView (National Instruments, Austin, TX) software. For cleanliness, a new disposable Simoon mouthpiece was used per subject at each station. Subjects were instructed on how to inhale from the simulator and had time to practice. The main instructions were “Inhale fast and deep until your lungs are full.” Three inhalation profiles were recorded, and the average PIF and inhaled volume from each subject were reported.
In addition, the study measured the MIP for 72 subjects using a modified inhaler simulator with a mounted pressure transducer model 8510B (Endevco, San Juan Capistrano, CA) with a pressure range of 0–2 psi and a drilled 1.5-mm intake hole to allow a small leak for measurement purposes. The transducer was connected to a pressure signal conditioner, Endevco model 4428A, which fed the results to a laptop computer with data acquisition software. The MIP meter also used replaceable Simoon mouthpieces. The main instructions were “Inhale forcefully for at least 2 seconds.” After several practice runs, three MIP profiles were recorded, and the maximum value was reported.
An additional study (breathing study 2) was conducted with the Simoon simulator in 62 elderly COPD patients (age>70 years). In this study, the criticality of not asking subjects to exhale before inhalation was assessed for the Simoon Inhaler/porous particle combination product.
Physicochemical properties of PulmoSphere Powder
Powder morphology was assessed by scanning electron microscopy (SEM). A powder sample of approximately 0.5 mg was coated with gold under partial vacuum (<100 mTorr) using a Denton Desk V sputter coater (Denton Vacuum LLC, Hillsboro, OR). The sample was then transferred to the multisample holder inside the vacuum chamber of the Model XL 30 SEM (Philips, Mooresville, NJ). After the vacuum reached less than 10–4 mbar, the samples were examined with an electron beam at 20 kV. Images were captured by a secondary electron detector.
The primary particle-size distribution was determined by laser diffraction. Measurements were made using a Sympatec Oasis instrument comprising a HELOS unit (with an R2 lens) equipped with a RODOS/M dry powder dispersing unit (Sympatec GmbH, Clausthal-Zellerfeld, Germany). Samples were filled into glass vials and introduced to the instrument via an ASPIROS micro-dosing powder feeder. The following settings were applied for analysis of samples: a sample mass of approximately 10 mg, an optical concentration of approximately 1%, and a driving pressure of 4 bar. Data were collected over a period of 10 sec. Particle-size distributions were calculated from the instrument software using a Fraunhofer model. A total of three replicates were taken per measurement.
Tapped densities were determined by measuring the mass of powder required to fill a cylindrical cavity (a uniaxial compaction, UC cell, of known volume) using a microspatula. The sample holder was gently tapped on the countertop. More powder was added to the cell as the sample volume decreased. The tapping and addition of powder steps were repeated until the cavity was filled and the powder bed no longer consolidated with further tapping.
Aerosol characterization
Emitted powder masses (EPM) from the Simoon Inhaler were determined gravimetrically (N=10). The EPM data were collected at a pressure drop of 4 kPa with a square-wave profile, corresponding to a flow rate of about 35 LPM. The volume of air sampled was 2 L. The powder emitted from the inhaler was collected on a filter (Pall Life Sciences, Ann Arbor, MI; P/N 61631), and its mass determined using a microbalance (Mettler Toledo, Columbus, OH; model AX-26).
The emptying profile for powder emission from the blister was assessed by laser photometry. The laser photometer generates a laser light sheet that intersects the flow path of the emitted aerosol immediately downstream of the inhaler mouthpiece. The obscuration of the laser sheet caused by the emitted aerosol bolus is detected by a photodetector. The photodetector's response is linear with obscuration, and Beer's law is used to convert the response into a relative aerosol concentration. It is “relative” in the sense that we have not corrected for differences in scattering intensity that result from the presence of different-sized particles in the laser path over the period of powder emptying. The signal intensity due to aerosol emission is observed as a voltage pulse whose width corresponds to the duration of the aerosol emission process.
Aerodynamic particle-size distributions (APSD) were determined gravimetrically on a Next Generation Pharmaceutical Impactor (MSP Corp., Shoreview, MN; model 170) without a preseparator. The APSD data were taken at the same device flow rate and sampling volume used to generate the corresponding EPM data. The aerosol deposited at each stage was collected on glass fiber filter substrates (Pall Life Sciences, P/N 60140 and 61663), which were clamped to the bottom surface of each collection cup (MSP Corp., P/N 0170-98-0210A-C). The powder mass deposited on each stage was determined by weighing the filters before and after device actuation on a microbalance (Mettler Toledo, model AX-26). Each APSD measurement required the actuation of six blisters (2 mg fill mass) to provide sufficient mass on the stages for gravimetric quantitation. The validity of using a gravimetric measurement versus a chemical assay to quantify the APSD of PulmoSphere powders has been established previously (data not shown).
An in vitro assessment of oropharyngeal deposition was conducted with the idealized Alberta mouth-throat model.(29–35) The model was developed by Finlay and co-workers and represents the average geometry of 80 subjects whose realistic mouth-throat geometries were obtained by magnetic resonance imaging.(29,30) The Alberta mouth-throat was fabricated from Accura® 60 resin by a stereolithography process based on drawings provided by Finlay (University of Alberta, Edmonton, Alberta, Canada). A 47-mm customized filter holder (Thermo Scientific Nalgene Polysulfone Holder) was placed downstream of the Alberta cast, for in vitro determination of the mass of powder that bypasses the mouth-throat. A polysorbate wetting agent (EMD Chemicals, Gibbstown, NJ; catalog no. 8170072) comprising equal parts Tween 20 and methanol was used for coating the interior walls of the Alberta cast.
Testing with the idealized Alberta mouth-throat was performed using square-wave flow profiles, as well as simulated patient flow profiles previously recorded during the aforementioned breathing studies conducted with asthma/COPD subjects. Simulated patient breathing profiles were generated using a custom breath simulator. The breath simulator is equipped with a computer-controlled proportional solenoid valve. When the system is connected to a vacuum source, the valve opening can be varied in a controlled manner to mimic a patient's flow profile.
The aerosol test laboratory was maintained at a temperature of 21±2°C (70°F) and a relative humidity (RH) of 40±5% RH.
Results
Inhalation profiles in asthma/COPD patients
To assess the goal of achieving lung deposition that is independent of the subject's inhalation effort, we must first understand the range of inhalation profiles that asthma/COPD subjects achieve through the Simoon Inhaler. The 69 subjects included in breathing study 1 were comprised of 17 female and 18 male asthmatics with a mean age of 28±21 years and a 1-sec forced expiratory volume (FEV1) of 82±24% predicted, and 18 female and 16 male COPD subjects with a mean age of 66±11 years and FEV1 of 54±20% predicted. When subjects were asked to inhale forcefully for at least 2 sec through the Simoon mouthpiece attached to a differential pressure gauge, the mean MIP values in asthma and COPD subjects were 6.2 kPa and 5.3 kPa, respectively (Fig. 3). Approximately 90% of the subjects were able to achieve a MIP of at least 4 kPa, and only two of the 72 subjects (a 4-year-old asthma subject and a 79-year-old COPD subject) failed to achieve a MIP of at least 2 kPa. Based on these results and the guidance from deBoer et al.,(19) the average asthma/COPD subject should be able to comfortably achieve a pressure drop of 3.0 to 3.5 kPa (e.g., 0.55×6.2 kPa), whereas those on the “bottom of the curve” should be able to achieve a pressure drop of at least 1.3 kPa.
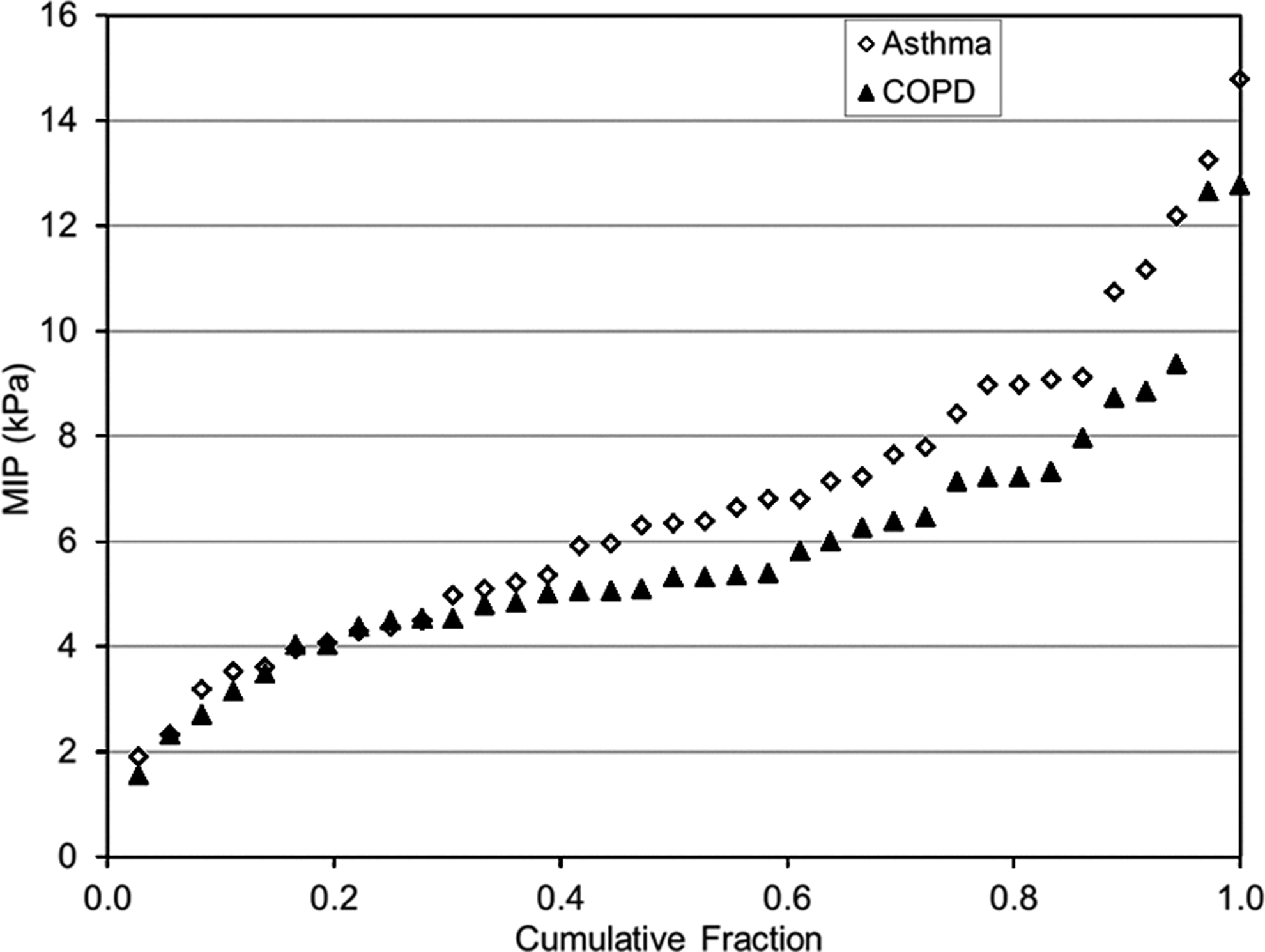
Plot of the maximum inspiratory pressure (MIP) achieved by asthma and COPD patients through a differential pressure gauge attached to a Simoon mouthpiece (breathing study 1). Subjects were instructed to inhale forcefully for at least 2 sec.
A plot of the pressure drop versus inhaled volume achieved by the same asthma/COPD subjects through the Simoon simulator in presented in Figure 4. Based on this plot, it is anticipated that most asthma/COPD subjects (>95% of the subjects in the present study) could achieve a pressure drop of at least 1 kPa and an inhaled volume of 500 mL. Based on these results, we selected ΔP ∼ 1 kPa and Vi ∼ 500 mL as our lower limit targets for in vitro aerosol testing over which the measured fine particle dose or dose post mouth-throat must be equivalent to standard in vitro test conditions (ΔP ∼ 4 kPa, Vi ∼ 2,000 mL). Note these “standard” test conditions are comparable to what is achieved by the average asthma/COPD subjects (see below). The mean PIF values obtained in the breathing study were 39 LPM and 36 LPM for the asthma and COPD subjects, respectively. This corresponds to a pressure drop of about 4 kPa. The mean inhaled volumes were 1,400 mL for asthma subjects and 1,500 mL for COPD subjects. The mean t60 values for the asthma and COPD subjects were 180 msec and 190 msec, respectively.
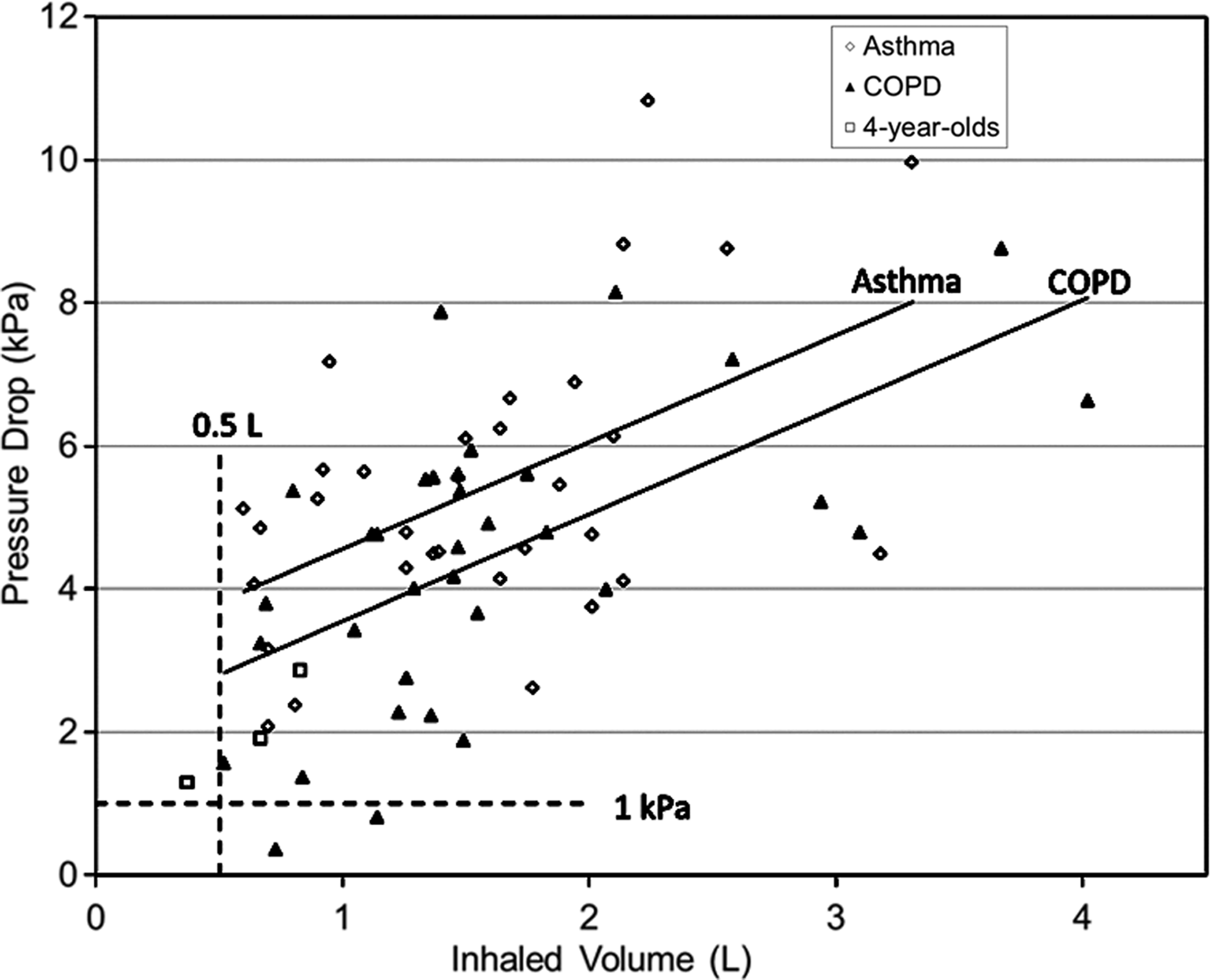
Plot of the pressure drop versus inhaled volume for asthma/COPD patients breathing through a Simoon simulator (resistance=0.17 cm H2O1/2 LPM−1). The instructions were to “inhale fast and deep until your lungs are full.” The solid lines represent linear regressions to the data points for asthma and COPD subjects, respectively (breathing study 1).
The pressure drops achieved by subjects with the Simoon Inhaler simulator are consistent with results observed for a range of marketed dry powder inhalers of varying device resistance.(18) Marketed devices assessed included the Aerolizer®, Diskus®, Turbuhaler®, Clickhaler®, Twisthaler®, and Easyhaler®. Chrystyn(18) found that mean pressure drops achieved by COPD subjects were generally greater than about 2 kPa across a broad range of subject age and disease severity (note: pressure drops were calculated from flow-rate and device-resistance data presented in this article). A trend toward higher pressure drops with increases in device resistance was observed. This is consistent with other studies that suggest that when subjects inhale against a resistance, they will typically achieve higher pressure drops, i.e., exert more inhalation effort.(16,17)
Inhaled volume
To assess the impact of variations in inhaled volume on dose inhalation errors, one must assess the timescale for powder emptying from the Simoon Inhaler. This is measured using laser photometry.(36,37) In this in vitro experiment, a target breathing profile is simulated and powder emptying from the device is assessed by measuring changes in optical density of the aerosol using a laser beam situated in the flow path. The emptying profiles for PulmoSphere placebo powders from the Simoon Inhaler are presented in the context of the inhalation profiles of “average” subjects determined in the breathing studies in Figure 5. Powder emptying occurs very early in the subject's simulated inhalation profile, with the bulk of the aerosol emptying within the first 250 mL. Assuming that an additional 100 mL of inhaled volume is required to pull the aerosol past the oropharynx and into the conducting airways,(38, 39) a total of approximately 350 mL of inhaled volume is needed to effectively deliver the contents of the blister to the lungs.
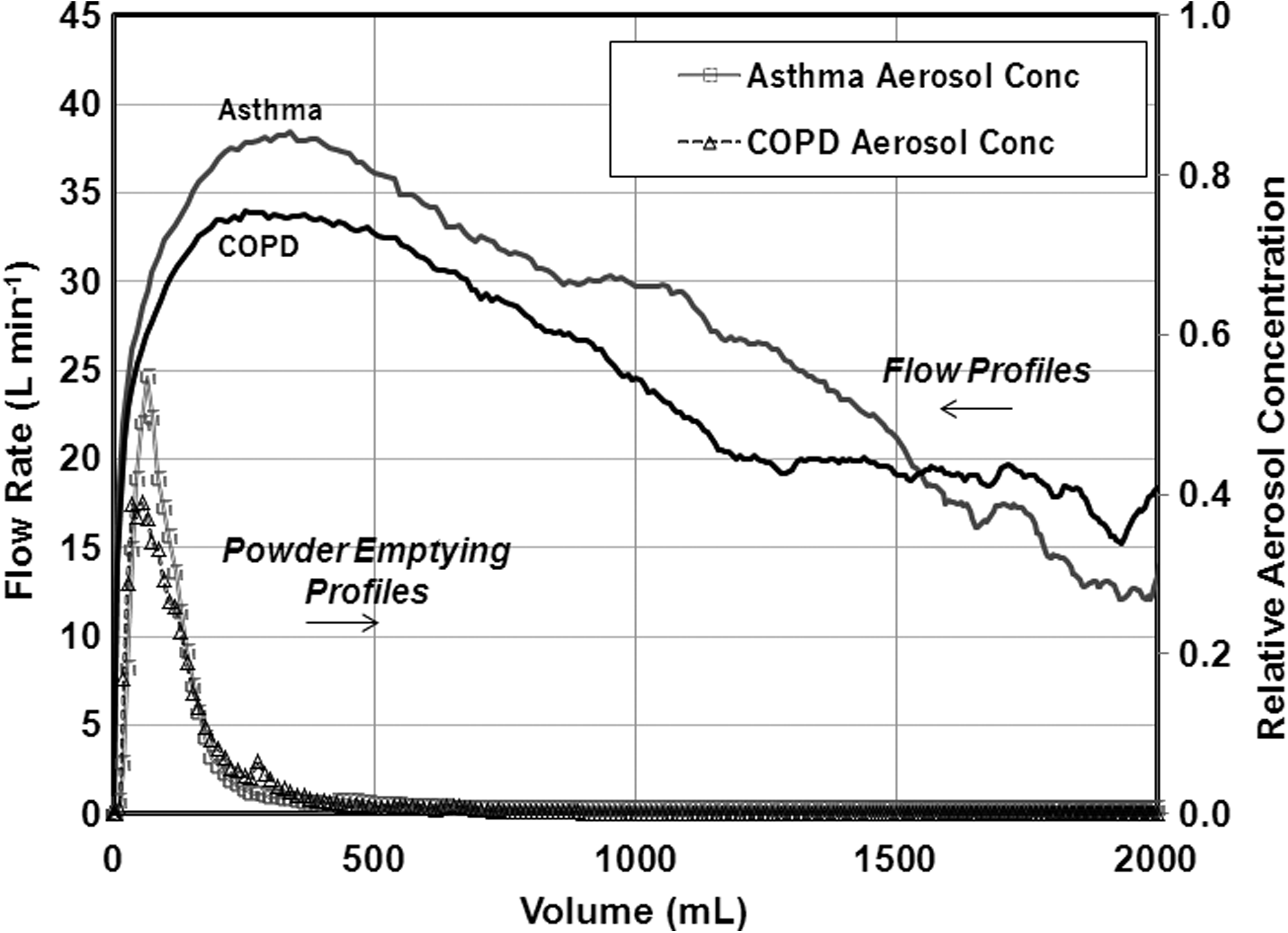
Individual flow profiles representative of average (ΔP ∼ 4 kPa) asthma and COPD subjects through the Simoon simulator from breathing study 1. Also shown are the powder-emptying profiles obtained for these simulated flow profiles by laser photometry.
Using gamma scintigraphic studies, Clark et al.(40) demonstrated that there was no difference in 24-hr clearance and penetration indices for a sulfur colloid for chase volumes of 300 mL to 800 mL. Hence, effective delivery to the lung periphery should be achieved with inhaled volumes of ∼550 mL (250 mL to empty device and 300 mL of chase air). As discussed previously, virtually all asthma/COPD subjects can achieve an inhaled volume of at least 500 mL (Fig. 4). Hence, it is unlikely that differences in inhaled volume between subjects will have a significant impact on pulmonary drug delivery, including regional deposition within the lungs.
Furthermore, the rapid emptying of powder from the blister may decrease the importance of other “critical” errors. For example, the single most frequent critical error cited by Molimard et al. was: “no exhalation before inhalation.”(1) It is believed that without adequate exhalation subjects may be unable to inhale forcefully and deeply enough (i.e., draw a large enough volume) through their dry powder inhalers to ensure deposition of drug in the lungs. Although this is often considered a “device-independent” error, it may be possible that emptying powder as a bolus from the dose receptacle early in the inhalation may mitigate its potential impact. The rapid powder emptying achieved with the Simoon Inhaler means that most subjects will continue to inhale long after the aerosolization event has been completed.
To assess the impact of not exhaling before inhalation on a subject's inhalation profile, an additional breathing study (breathing study 2) was conducted with 62 elderly COPD subjects (age 70 and older). The demographics of the subjects are presented in Table 1 and the results in Table 2. No differences in PIF were observed for the two sets of instructions. Significant decreases in Vi and ti are observed for the modified instructions. Nonetheless, all of the subjects were able to achieve the targeted 1 kPa pressure drop and 500 mL inhaled volume. Hence, failing to exhale before inhalation is unlikely to have a critical impact on drug delivery with the Simoon Inhaler. This observation is likely not unique to the Simoon Inhaler, and will be observed for other blister-based or reservoir-based dry powder inhalers, where powder emptying occurs early in the inhalation profile.
Data are represented as means±SD.
The resistance of the Simoon Inhalers was 0.20 cm H2O1/2 LPM−1. The mean PIF values measured represent a 4-kPa pressure drop.
Another critical error that may be impacted by the “bolus” delivery profile of the Simoon Inhaler and the size of the PulmoSphere particles is the requirement for a breath-hold post dosing.(1) For most subjects, the additional inhalation time after the emptying event (typically>2 sec) allows the particles to sediment prior to exhalation. The low impact of breath-hold for passive dry powder inhalers was demonstrated previously by Newman et al. for the Spinhaler device,(41) where the exhaled fraction for sodium cromoglycate powders increased from just 0.5% to 1.0% without a breath-hold. Exhaled fractions observed clinically with porous particles delivered from capsule-based inhalers are low, typically less than 5%.(26,42) Hence, for the aerosols with an aerodynamic diameter of 3 μm to 5 μm utilized in the present study, significant exhalation of particles is not anticipated, even without a breath-hold. For fine particles with an aerodynamic diameter of approximately 1 μm, the breath-hold would be expected to take on greater importance.(43)
Flow-rate dependence
The flow-rate dependence of PulmoSphere placebo powder from the blister-based Simoon Inhaler was assessed on a Next Generation Impactor (Table 3, Figs. 6 and 7), and with the idealized Alberta mouth-throat model (Tables 4 and 5, Fig. 8).
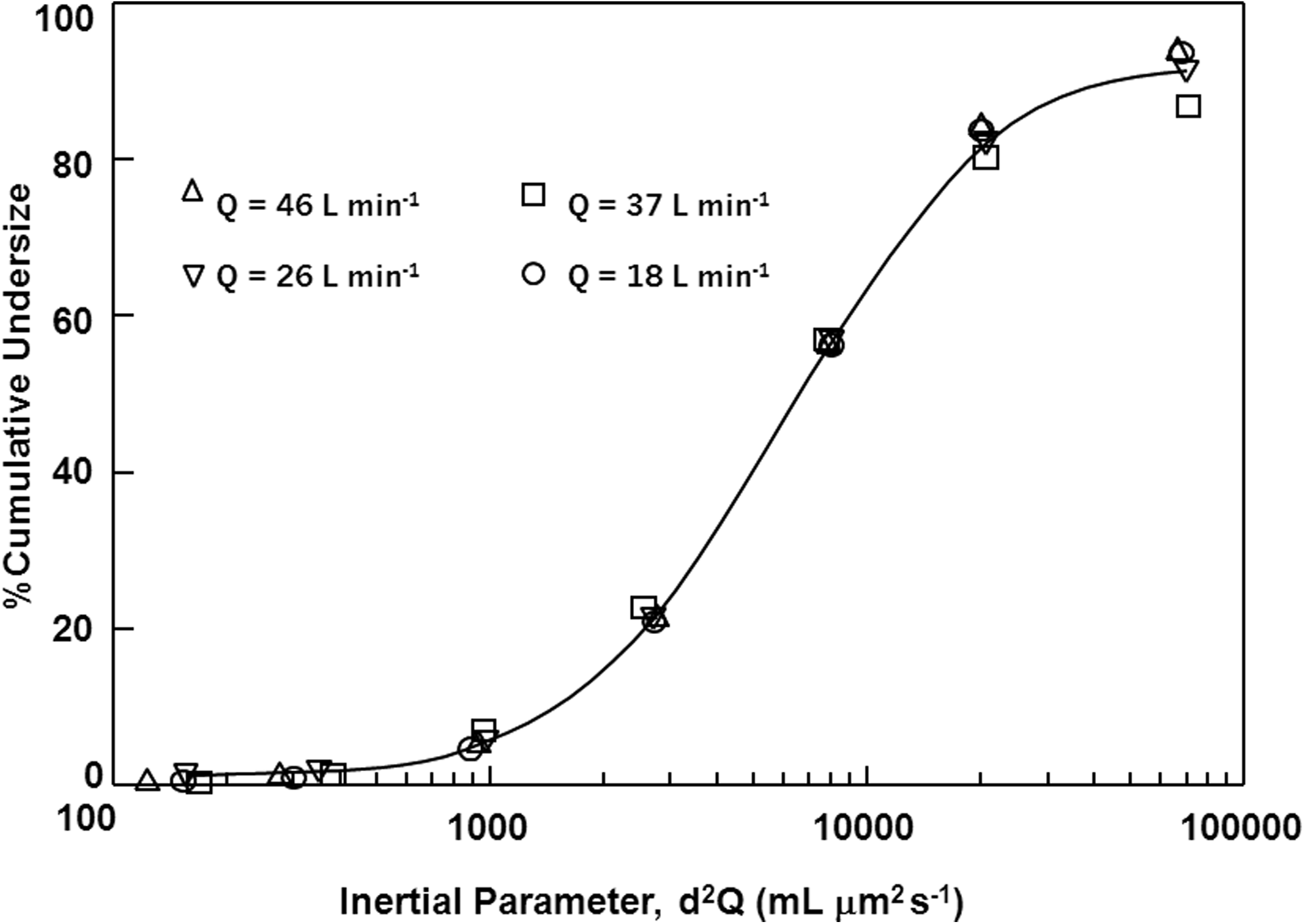
Plot of the cumulative mass distribution as a function of the inertial parameter for various test flow rates in the Simoon Inhaler with a placebo PulmoSphere formulation.
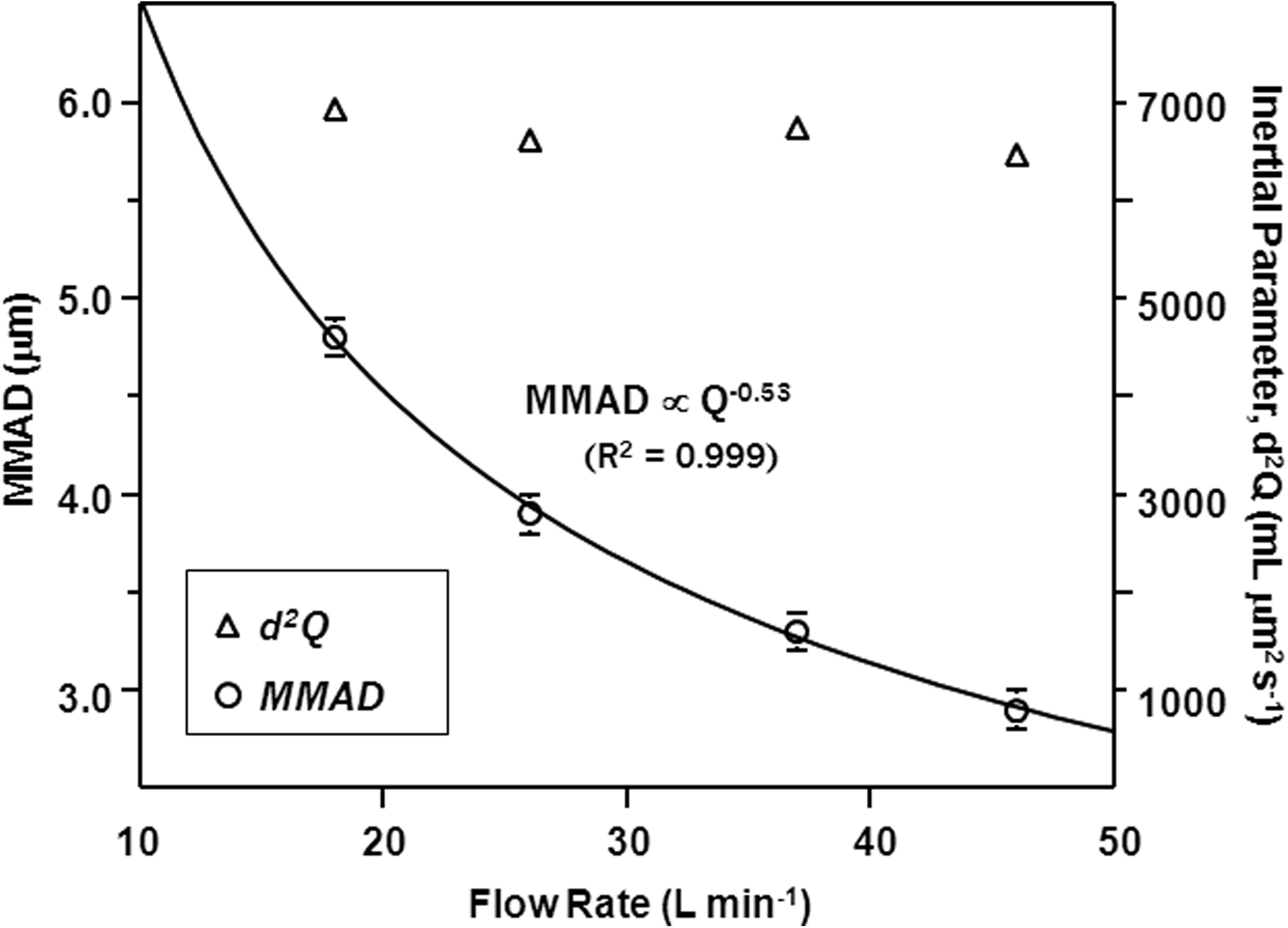
Plot of the MMAD and inertial parameter (d2Q) for PulmoSphere placebo particles delivered from the Simoon Inhaler as a function of flow rate. Each MMAD value represents the mean of three replicates, with the error bars representing the standard deviation.
Plot of mouth-throat deposition as a function of the inertial parameter in the idealized Alberta mouth-throat model. In addition to data from the present study (Table 2), the plot includes points from previous studies using the Alberta cast.(29,31,35)
EPM testing was conducted with a 1-mg fill mass; APSD testing was conducted with a 2-mg fill mass. The impaction parameter was calculated using the MMAD as the diameter. The resistance of the Simoon Inhalers was 0.17 cm H2O1/2 LPM−1.
EPM and APSD testing were conducted with a 2-mg fill mass. The resistance of the Simoon Inhalers was 0.17 cm H2O1/2 LPM−1.
EPM testing was conducted with a 1-mg fill mass; APSD testing was conducted with a 2-mg fill mass. The resistance of the Simoon Inhalers utilized was 0.17 cm H2O1/2 LPM−1.
Table 3 presents various in vitro measures of aerosol performance including the EPM, mass median aerodynamic diameter (MMAD), and the fine particle mass (FPM) for stage groupings S3-F and S4-F. The data are presented as a function of variations in flow rate from 18 LPM to 46 LPM, corresponding to pressure drops across the Simoon Inhaler from 1 kPa to 6 kPa. Increases in EPM are observed with increases in flow rate. This is a reflection of improved powder fluidization and blister emptying at the higher flow rates.
A plot of the cumulative APSDs for the various flow rates tested is presented in Figure 6. Note that the distributions are plotted not as a function of aerodynamic diameter as is customary, but instead as a function of the inertial parameter, d2Q, where d is the aerodynamic diameter and Q is the flow rate. This single parameter captures the combined effect of flow rate and particle size on mouth-throat deposition. The small variation observed in the cumulative distributions reflects that the inertial impaction on the various stages of the Next Generation Impactor is independent of flow rate.
This is further demonstrated in the lack of statistically significant differences in powder deposition for the “respirable” stage groupings (e.g., S3-F, S4-F). The mean FPMS4-F at a standard pressure drop of 4 kPa (Q=37 LPM) was 46% of the nominal dose. At 6 kPa (Q=46 LPM), the mean FPMS4-F was 45%. Similarly, at a pressure drop of 2 kPa (Q=26 LPM), the mean FPMS4-F was 45%. Even at a pressure drop of just 1 kPa (Q=18 LPM), an FPMS4-F of 43% was obtained. Within the context of a Tukey-Kramer one-way ANOVA analysis, there is statistically no difference between any of the pressure drops tested (p<0.05). The small differences in FPMS4-F are driven more by the differences in EPM than by differences in inertial impaction, as demonstrated by the cumulative distributions in Figure 6. Similar results were obtained for FPMS3-F. As discussed previously, the range of pressure drops tested should encompass more than 95% of asthma/COPD subjects.
One consequence of the desire to achieve lung delivery that is independent of flow rate is that the APSD must necessarily get finer with increases in Q. Figure 7 presents a plot of the MMAD versus flow rate, Q. MMAD values decreased from 4.8 μm at 18 LPM to 2.9 μm at 46 LPM. An excellent fit is observed for MMAD∝Q–0.5. Hence, the dependence of MMAD with Q effectively compensates for the increases in mouth-throat impaction anticipated at higher flow rates.
Also presented in Figure 7 is a plot of the inertial parameter, d2Q, as a function of flow rate. The inertial parameter is calculated for d=MMAD. The values of d2Q obtained are independent of flow rate, consistent with the cumulative distributions shown in Figure 6.
The impact of variations in flow rate was further assessed using the idealized Alberta mouth-throat model. Deposition of PulmoSphere placebo particles in the idealized Alberta cast was low (∼13–15% of the nominal dose) and consistent across a range of flow rates from 16 LPM to 40 LPM (Table 4). Again, much of the observed difference in deposition on the filter post mouth-throat is the result of the small increases in EPM observed with increases in flow rate.
The magnitude of mouth-throat deposition observed for the values of d2Q achieved with the PulmoSphere placebo particles is consistent with previous studies of oropharyngeal deposition using the idealized Alberta mouth-throat (Fig. 8). The clustering of the points at various flow rates is indicative of the consistency in the inertial impaction parameter with variations in Q.
Ramp time
For the Simoon Inhaler, powder is emptied through the center hole cut in the blister. Powder emptying is controlled by the diameter of the blister hole and the air flow rate through the blister. A 1.2-mm blister hole diameter is comparable to the holes punched in hypromellose capsules in the marketed TOBI® Podhaler® device (Novartis Pharmaceuticals Corporation, San Carlos, CA).(27) The absence of significant ramp rate effects on in vitro aerosol performance is illustrated in Table 5. The “slow” ramp time, expressed as the time to achieve 60% of the PIF, was about 18–25% slower than the mean ramp times observed in asthma/COPD subjects, whereas the “fast” ramp was 42–45% faster than the mean ramp times. No significant differences in EPM, MMAD, FPMS3-F, or FPMS4-F were observed for the slow and fast ramp times.
Simulated inhalation profiles of COPD subjects
Finally, the in vitro deposition post mouth-throat with the Alberta cast model was determined for a range of simulated inhalation profiles (Table 6). The individual profiles were selected from the user studies to cover the range of profiles anticipated for COPD subjects, and extend from about 1 kPa to 6 kPa (Fig. 9). The inhalation profile for the subject with a pressure drop of about 1 kPa also has a small inhaled volume (Vi<500 mL) and a very long ramp time (t60=510 msec). This profile represents a worst-case scenario for all of the critical parameters characterizing the inhalation profile. Nonetheless, deposition post mouth-throat in the idealized Alberta mouth-throat model remained high (>60% of the nominal dose).
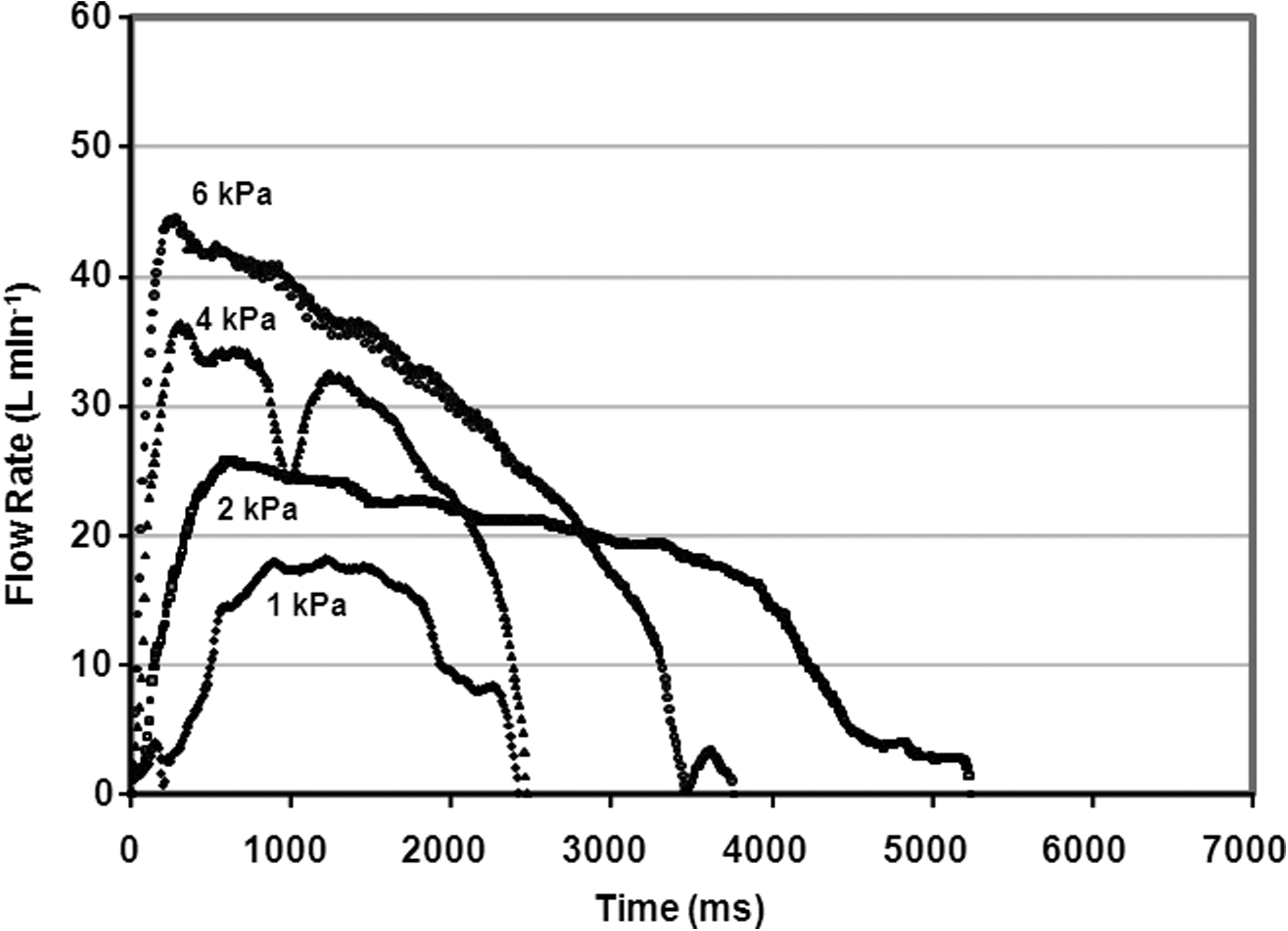
Plot of individual inhalation profiles of diverse COPD patients in the Simoon simulator from breathing study 1.
Each value of the lung dose is an average of three runs±1 SD.
With that said, the mean deposition post mouth-throat values at 1 kPa and 2 kPa pressure drops are about 10–15% lower than the value obtained for the subject profile at 4 kPa, with significantly greater variability (RSD>10%). In each instance, two of the three replicates gave lung deposition values comparable to the values measured at 4 kPa, with the remaining replicate giving significantly less. The increased variability noted for these profiles may be linked to the longer ramp times to peak flow (t60=240 msec and 510 msec). Broeders et al. noted that the longest ramp times occur for subjects with the lowest PIF, consistent with the subject profiles in Fig. 9.(44) The slower ramp times may negatively impact the coupling of the powder-emptying event to the energy of powder dispersion created by the subject's inhalation. To overcome this source of variability, the ratio of blister flow to bypass flow may need to be increased. This will provide greater dispersion energy to the powder at the low flow rates.
Discussion
The goal of the present study was to achieve significant reductions in dose inhalation errors (i.e., variability associated with the inhalation maneuver), by providing pulmonary drug delivery that is largely independent of a subject's inhalation profile. The in vitro results presented for PulmoSphere placebo particles in the Simoon Inhaler are consistent with previous in vitro and pharmacoscintigraphy results obtained for a budesonide PulmoSphere formulation with a capsule-based dry powder inhaler.(26) The budesonide PulmoSphere powder achieved 58% lung deposition (67% of the delivered dose), when inhaled with the capsule-based Eclipse® dry powder inhaler (Sanofi Aventis, Holmes Chapel, UK), independent of whether the subjects were asked to breathe comfortably or forcefully through the device.(26) More broadly, a range of porous particle formulations delivered with different capsule-based dry powder inhalers of varying device resistance were found to be independent of PIF in pharmacoscintigraphy studies across a range of pressure drops from approximately 1 kPa to 8 kPa, with an RSD of just 12%.(45)
Increasing PIF impacts total lung deposition in two competing ways: (a) it increases inertial impaction in the mouth-throat, thereby decreasing lung deposition; (b) it increases powder dispersion, thereby increasing lung deposition. For spheronized particles (e.g., Pulmicort® Turbuhaler®; AstraZeneca, Wilmington, DE), the improvements in powder dispersion achieved with increases in PIF outweigh losses due to inertial impaction, resulting in significant increases in lung deposition with increases in PIF.(26,46) A similar trend is noted for ordered mixtures with coarse lactose, although the magnitude of the effect is not as large, and can be mitigated to some degree through device design.(47) Interestingly, active devices that decouple powder dispersion from the inhalation event lead to “reverse” flow-rate dependence, where increases in lung deposition are noted with decreases in PIF.(47,48) Porous particles fluidize and disperse effectively with little applied energy.(26,49–51) When delivered with a passive dry powder inhaler, the drug/device combination provides a means to balance the two competing effects, enabling flow-rate independence in lung deposition over a wide range of PIF.(26,50,51)
From an in vitro perspective, the pattern of deposition of budesonide PulmoSphere particles on impactor stages was found to be superimposable at 30 LPM and 50 LPM.(26) Given that impactor stage cutoffs are governed by inertial impaction (i.e., proportional to d2Q), the absence of flow-rate dependence in vivo correlates with a constant inertial parameter in vitro. Hence, one goal of the present study was to achieve a constant inertial parameter across the range of inhalation profiles achieved by asthma and COPD subjects with the Simoon Inhaler. This was effectively achieved across a range of flow rates from 18 to 46 LPM, as the data presented in Table 3 and Figures 6 and 7 attest. This range of flow rates represents pressure drops from 1 kPa to 6 kPa and covers the practical range of flow rates anticipated for asthma and COPD subjects with the Simoon Inhaler (Fig. 4).
We also utilized the idealized Alberta mouth-throat model to assess inertial impaction. Casts of human mouth-throat regions have been demonstrated to provide a better correlation with in vivo deposition studies than do induction ports on standard impactors.(52,53)
The analysis assumes that inertial impaction is proportional to d2Q. This may not be strictly correct when one accounts for turbulence in the mouth and throat. Grgic et al.(29) showed that by inclusion of a Reynold's number correction, that inertial impaction in the mouth-throat was more accurately represented by d2Q1.37. Moreover, the results presented in Tables 3 and 4 suggest that small decreases in powder fluidization with decreases in Q will also need to be considered. Ultimately, the dependence of total lung deposition with d and Q will need to be established clinically, and the drug/device combination adjusted to achieve consistent lung delivery with variations in PIF.
The dependence of powder dispersion of porous particles with variations in PIF can be adjusted in the drug/device combination via optimization of device features (e.g., blister hole diameter, flow rate through the blister, flow rate through the bypass, device resistance), and/or by optimization of specific powder properties (e.g., geometric size, density, porosity).(54) A recent study by Ung et al.(54) highlights how these properties can be tuned in the PulmoSphere/Simoon drug/device combination.
A key factor controlling in vivo variability during dose inhalation is biological differences in the anatomy of the mouth-throat. Borgström et al.(55) retrospectively analyzed lung deposition data from 71 gamma scintigraphic and pharmacokinetic studies. The results revealed significant reductions in intersubject variability when total lung deposition exceeded 40% of the delivered dose. The mean lung deposition for currently marketed asthma/COPD dry powder inhalers comprising micronized drug is typically in the range of 10–30%.(56) This results in mean RSD values in lung deposition of 30–50%. In contrast, porous particles delivered from capsule-based inhalers exhibit RSDs of just 10–20% (40–70% lung deposition).(26,38,45,50,51)
Assuming that the inertial parameter provides a reasonable yardstick for estimating mouth-throat deposition, one can compare the inertial parameters from previous PulmoSphere pharmacoscintigraphy studies to provide an estimate of in vivo lung deposition and associated variability in the present study (in vitro/in vivo correlation). The budesonide PulmoSphere formulation delivered from the Eclipse Inhaler achieved 67% lung deposition (12% RSD),(26) with an inertial parameter of 4,800 mL μm2 sec–1, whereas a tobramycin PulmoSphere formulation delivered with the Turbospin Inhaler(42) achieved 42% lung deposition (17% RSD), with an inertial parameter of 8,400 mL μm2 sec–1. In the present study, the inertial parameter was about 6,700 mL μm2 sec–1, suggesting that total lung deposition may be around 50–55%. Based on the data of Borgström et al.,(55) the variability in lung dose is likely to be on the order of 10–20%. Given the flow-rate independence noted above, this source of variability is likely to be the principal source of error for these drug/device combinations.
A key difference between capsule-based and blister-based inhalers lies in the time frame for powder emptying from the receptacle. For capsule-based inhalers, the powder is “shaken” from the capsule, with an emptying time determined by the fill mass in the capsule. As the fill mass increases, the subject's inhaled volume becomes a critical attribute in determining whether the dose can be emptied in a single inhalation. For blister-based inhalers, such as Simoon, powder emptying is very rapid. In this case, one must be concerned that powder empties the receptacle before significant dispersion energy in the form of the subject's PIF is achieved. In other words, the powder-emptying event may be poorly coupled to powder dispersion.
The blister flow resistance, and thus the flow rate through the blister, can be controlled by varying the diameter of the blister hole and the ratio of flow through the blister and bypass.(54) For example, powder flow through a blister with a small opening diameter (0.8 mm) is delayed and prolonged compared with powder emptied through a 2.5-mm blister hole.(54) This leads to improved coupling of powder emptying to the dispersion energy supplied by the subject's inhalation. The improved coupling ultimately leads to a reduced impact of the ramp time to 60% of peak flow on in vitro aerosol performance, and an improved fine particle dose. In the present study, dramatic increases in ramp time, as observed in the extreme patient profile in Figure 9, still result in high in vitro aerosol performance with the combination of blister hole size and ratio of blister to bypass flow. The rapid emptying of powder from the Simoon Inhaler and other bolus aerosol delivery devices also decreases the criticality of exhaling before inhalation and the subsequent breath-hold post inhalation.
This article has focused on the potential for reducing dose inhalation errors with a drug/device combination comprising porous particles and a passive blister-based unit dose inhaler. In particular, we have focused on design of the aerosol engine in the Simoon device and the particle properties required to achieve a constant d2Q with variations in Q. The Simoon Inhaler represents a stepping stone to a multidose blister-inhaler with a similar aerosol engine, where a significant reduction in potential dose preparation errors may also be achieved.(7,57)
Conclusions
In vitro methods (Next Generation Impactor and idealized Alberta mouth-throat model) were used to assess the impact of variations in inhalation profile on inertial impaction for drug/device combinations comprising PulmoSphere powders and a blister-based unit dose dry powder inhaler. The inertial parameter, d2Q, was found to be largely independent of variations in simulated inhalation profiles of asthma/COPD subjects, taking into account the ranges of flow rate, inhaled volume, and ramp time to peak flow observed in breathing studies. The magnitude of the inertial parameter measured for the PulmoSphere/Simoon drug/device combination is predicted to result in 10–20% variability in lung delivery in vivo, by effectively bypassing deposition in the mouth-throat region. Given the relative independence of inertial impaction with variations in inhalation profile, the errors associated with oropharyngeal filtering are expected to be the major source of variability with the inhalation event.
Footnotes
Author Disclosure Statement
All of the authors are employees of Novartis Pharmaceuticals Corporation, receiving salaries and other compensation.