
Abstract
Abstract
Background
Methods:
PIFRresist and inspiratory capacity (IC) were measured after spirometry was performed in patients with advanced COPD. Repeat measurement of PIFRresist was performed in a subset of patients who returned for scheduled follow-up appointments.
Results:
The prevalence of a PIFRresist of <60 L/min was 19% among 213 patients. The clinical phenotype of these 41 patients included predominantly female gender (80%), shorter height, and lower values for forced vital capacity (FVC) and IC as percentage predicted compared with the 172 patients with PIFRresist of >60 L/min. Multivariate regression analysis performed on all patients demonstrated that age, gender, height, FVC % predicted, and IC % predicted were independent predictors of PIFRresist (R2=36%). Repeat testing showed no difference between the PIFRresist values.
Conclusions:
Approximately one out of five patients with advanced COPD and ≥60 years of age exhibited a suboptimal PIFRresist against the Diskus. For the first time, a clinical phenotype of such patients with a suboptimal PIFRresist was identified. It is reasonable to measure a patient's PIFR against the simulated resistance of a specific DPI if there is concern about clinical benefit using the dry powder medication.
Introduction
Although studies have shown that long-acting bronchodilators delivered via a DPI generally improve lung function and clinical outcomes in patients with moderate to severe COPD,7–11 not all patients experience improvement with a DPI. For example, Jarvis and colleagues 12 reported that six of 12 patients with COPD were “unsure” whether they received any benefit from a DPI. One possible explanation for this is that the patient has “fixed” airflow obstruction with no bronchodilator responsiveness. However, the majority of patients with moderate to very severe COPD demonstrate significant bronchodilator responses in flow [forced expiratory lung volume in 1 sec (FEV1)] and/or volume [forced vital capacity (FVC)] with short-acting bronchodilators.13,13 An alternative consideration is that some patients with COPD are unable to completely inhale the medication from the DPI into the lower respiratory tract due to a suboptimal PIFRresist.
To investigate this possibility, we performed an observational cohort study in patients with advanced COPD. The major questions were as follows: (1) What is the prevalence of a suboptimal PIFRresist in patients with advanced COPD? (2) Is there a clinical phenotype of patients who exhibit a suboptimal PIFRresist? (3) What is the test–retest reliability of PIFRresist? Such information would be helpful to health-care providers in order to consider which individuals with COPD might not achieve the expected benefits with a dry powder bronchodilator.
Materials and Methods
Study subjects
Inclusion criteria were a diagnosis of COPD, 1 at least 10 pack-year history of cigarette smoking, age ≥60 years, and FEV1 of ≤50% predicted. 15 Exclusion criteria were inability to understand verbal instructions, unstable clinical disease, and inability to perform consistent peak inspiratory efforts. Eligible patients were recruited after they completed pulmonary function tests at our institution.
Study design
This observational study was performed between February 2010 and February 2012 in a cohort of patients with advanced COPD. The protocol was approved by the Committee for the Protection of Human Subjects at Dartmouth College (#22175). All patients signed the appropriate consent form.
Testing procedures at the initial and follow-up visits are described in Table 1. After spirometry was completed, patients who met inclusion/exclusion criteria were asked to participate in the study. At follow-up testing (starting in September 2011), spirometry was performed when patients returned for an appointment with their physician. Then patients performed three PIFRresist maneuvers against the Diskus® to test for repeatability of measurement.
Methods
Spirometry and inspiratory capacity (IC) (Collins model CPI, Longmont, CO) were measured using standard techniques.16,16 Values were expressed as percentages of predicted values.15,15 The In-Check DIAL® (Clement Clerke International Ltd., Harlow, UK) was used to measure PIFR at no resistance and at a simulated internal resistance of the Diskus. This testing device has been used widely in previous studies.6,12,19 According to the manufacturer, the In-Check DIAL is accurate within±10% or±10 L/min, whichever is greater. The Diskus was selected because it is a widely used delivery system and has a lower internal resistance than the HandiHaler® and Turbuhaler® DPIs.5,6,19
Each patient was instructed to inhale “as quickly as possible” with the In-Check DIAL after a complete exhalation. The highest PIFRresist value for each patient was used for analysis.
Analysis
Analysis of variance was used to test for any differences among the three PIFR values with no resistance and among the three PIFR against the resistance of the Diskus. Unpaired t tests were used to compare baseline characteristics of patients who had PIFR of <60 L/min and ≥60 L/min. Paired t tests were used to compare the highest PIFRresist at initial and follow-up visits. Chi-square testing was used to compare the number of females in the two groups based on PIFRresist of <60 L/min and ≥60 L/min. Pearson correlation analyses were performed for PIFRresist with age and measures of lung function. A stepwise regression analysis was performed to investigate independent predictors of PIFRresist; these included age, height, weight, and lung function (FVC, FEV1, and IC) as percent predicted. Results are presented as mean and standard deviation values along with confidence intervals (CI).
Results
Descriptive characteristics of the 213 patients with COPD and subgroups based on PIFRresist of ≥60 L/min and <60 L/min are shown in Table 2. There were no significant differences in the three PIFR values with no resistance (p=0.75) and against the resistance of the Diskus (p=0.73).
FVC, forced vital capacity; FEV1, forced expiratory volume in 1 sec; IC, inspiratory capacity; ICS, inhaled corticosteroid alone or in combination with LABA; LABA, long-acting β-agonist; SABA, short-acting β-agonist.
n=211 for total, n=171 for PIFRresist ≥60 L/min, and n=40 for PIFRresist <60 L/min.
Number of patients, with percentages in parenthesis, taking inhaled medications as treatment of COPD.
Forty-one patients (19%) exhibited a PIFRresist of <60 L/min (48.4±8.8 L/min; range, 25–59 L/min). There were significantly more females in those with PIFRresist of <60 L/min (80%) compared with those with PIFRresist of ≥60 L/min (48%) (p<0.001). There were no differences in age (p=0.24), body weight (p=0.06), or FEV1 % predicted (p=0.43) between patients with PIFRresist of <60 L/min and ≥60 L/min. However, the subgroup with PIFRresist of <60 L/min had a lower height (p<0.001; CI: 3.6, 9.6) and lower values for FVC % predicted (p<0.001; CI: 5.3, 16.2) and IC % predicted (p=0.007; CI: 2.3, 14.4).
For the total group, PIFRresist was inversely correlated with age (r=−0.25; p<0.001) and positively correlated with FVC % predicted (r=0.37; p<0.001) (Fig. 1) and IC % predicted (r=0.35; p<0.001) (Fig. 2). There was no significant correlation between PIFRresist and FEV1 % predicted (r=0.11; p=0.11). Multivariate regression analysis performed on all 213 patients demonstrated that age, gender, height, FVC % predicted, and IC % predicted were independent predictors of PIFRresist with an R 2 -adjusted value of 36%. Neither weight nor FEV1 % predicted was accepted into the regression model.
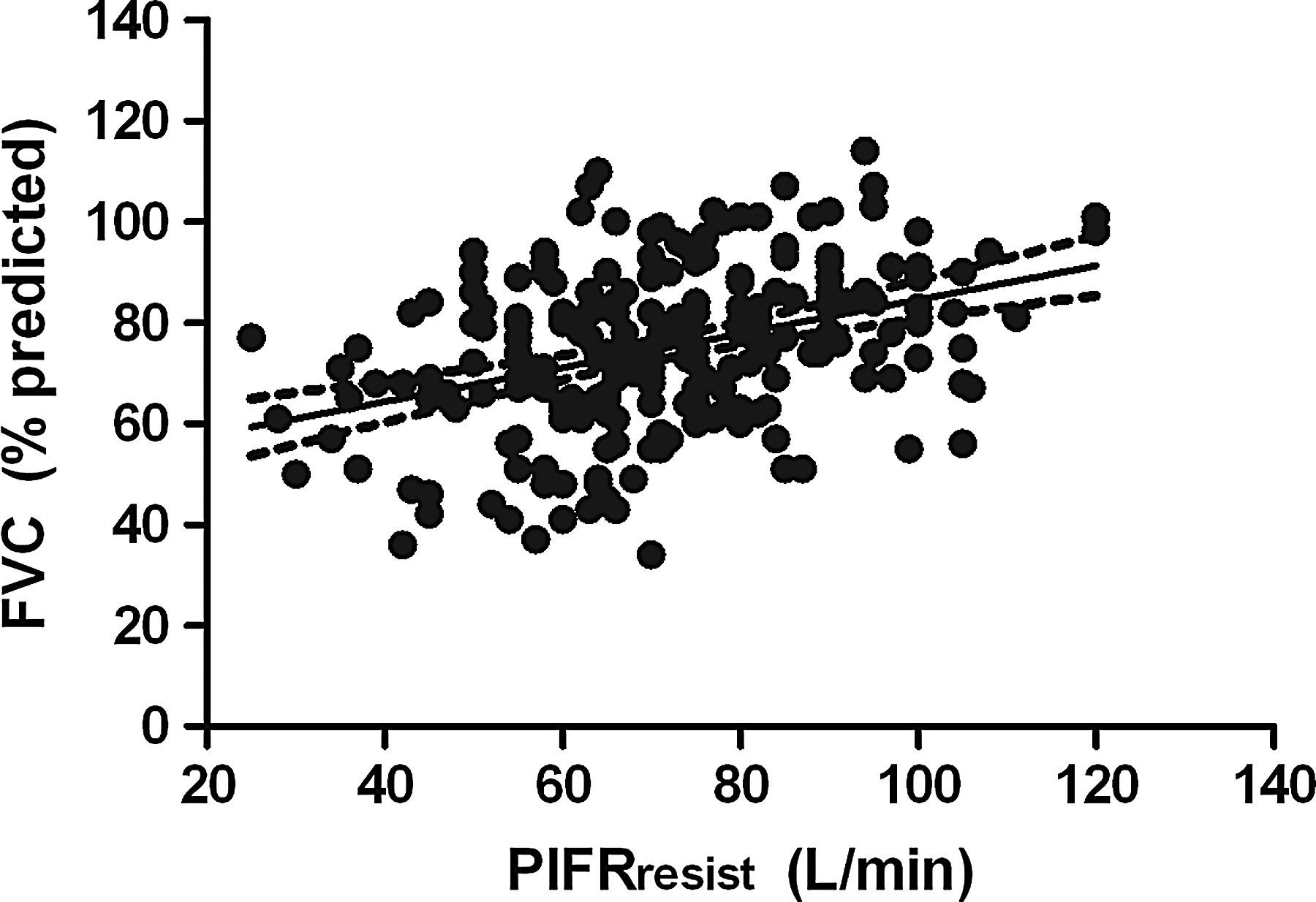
Scatter plot of the relationship between PIFR through the simulated resistance (resist) of the Diskus and FVC % predicted in 213 patients with advanced COPD. The solid line is linear regression for the two variables, and the dashed lines represent the standard deviations. Pearson correlation coefficient was 0.37 (p<0.001).

Scatter plot of the relationship between PIFR through the simulated resistance (resist) of the Diskus and IC % predicted in 211 patients with advanced COPD. The solid line is linear regression for the two variables, and the dashed lines represent the standard deviations. Pearson correlation coefficient was 0.35 (p<0.001).
Forty-five patients (24 females and 21 males) returned for follow-up testing after an interval of 317±225 days. There were no significant differences in highest FEV1 (0.92±0.25 vs. 0.88±0.25 L; p=0.53) or highest PIFRresist (72.8±18.4 vs. 74.9±17.9 cm H2O; p=0.59) between visits.
Discussion
The unique findings of the study were: (1) 19% of 213 patients with advanced COPD and at least 60 years of age exhibited a suboptimal PIFR with the simulated resistance of the Diskus DPI; (2) these 41 patients were predominantly female (80%), shorter in height, and had reduced lung volumes (FVC and IC % predicted) compared with the 172 patients with PIFRresist of ≥60 L/min; and (3) test–retest reliability of PIFRresist was acceptable.
To overcome the internal resistance of a DPI and to deaggregate the powder formulation into fine particles, it is recommended that the patient inhale as deeply and as hard as possible. 20 Although a PIFRresist of at least 30 L/min is the minimal inspiratory flow to achieve some clinical effect, in vitro testing has consistently demonstrated that the total and fine particle doses emitted from a DPI are enhanced when PIFRresist is increased from 30 to 60 L/min.5,21,22 A PIFRresist of at least 60 L/min through a DPI is optimal to generate fine particles of powder (<5 μm) that can be inhaled into the lower respiratory tract.19,19 Pharmaceutical companies have performed in vitro testing of the Aerolizer®, Neohaler®, and Diskus devices at a PIFR of 60 L/min for 2 sec to assess the dose of the emitted powder.24–26 Reports indicate that a high percentage of patients tested achieved a PIFR of >60 L/min through these DPIs.24–26
The prevalence of those who did not achieve an optimal PIFRresist (i.e., <60 L/min) was 19% in our study population. To our knowledge, our results provide the largest number of subjects in whom PIFR was measured against the simulated resistance of a DPI. Previously, Janssens and colleagues 6 found that 18% and 36% of 26 elderly patients with COPD (FEV1=49±20% predicted) had a PIFR of <60 L/min against the resistances of the Aerolizer and Diskus, respectively. In contrast, van der Palen 19 reported that all 50 patients with asthma or COPD (FEV1=72±23% predicted) achieved a PIFR of >60 L/min through the Diskus. These discordant findings in heterogeneous patient populations led us to investigate whether certain baseline characteristics might identify patients with advanced COPD considered to be “at risk” for a suboptimal PIFRresist.
To our knowledge, this study is the first to describe a clinical phenotype—female gender, shorter height, and lower values for lung volumes—for patients with advanced COPD that exhibited a suboptimal PIFRresist. The predominance of females in this subgroup (80%) compared with those with a PIFRresist of ≥60 L/min (48%) is likely due to an absolute threshold value for PIFRresist, and the fact that women have lower overall values for lung function compared with men. The lower height observed in the subgroup with PIFRresist of <60 L/min is consistent with the predominance of females.
We found no difference in FEV1 % predicted values between the two groups. However, patients with PIFRresist of <60 L/min had significantly lower values for FVC and IC % predicted. Although we did not measure residual volume and functional residual capacity in this study, we believe that the differences in FVC and IC % predicted between subgroups are likely due to greater air trapping and hyperinflation, respectively, which are direct consequences of expiratory airflow obstruction. 27 With the development of lung hyperinflation, the vertical muscle fibers of the diaphragm shorten, which results in functional weakening of the diaphragm muscle. This process could affect a patient's ability to generate an adequate or optimal PIFR. An alternative explanation is that the lower lung volumes may be due to a lower inspiratory effort.
For the total population of 213 patients, PIFRresist was inversely correlated with age. This finding reflects the general decline in lung function, including PIFR, with advancing age and confirms previous results.6,6 However, there was no significant difference in age between the two subgroups based on a cutoff value of 60 L/min for PIFRresist. Our results also confirm findings reported by Janssens and colleagues 6 that FEV1 % predicted was not significantly correlated with PIFRresist. The breathing maneuvers for FEV1 and PIFR involve different phases of respiration and require different respiratory mechanics. For the entire group, PIFRresist was significantly correlated with IC % predicted values. Both PIFR and IC require similar inspiratory maneuvers, but are initiated at different lung volumes. Results of multivariate regression analysis support our findings that gender, height, FVC % predicted, and IC % predicted were different between subgroups based on PIFRresist of ≤60 and >60 L/min.
There are limitations to our study. First, we selected patients ≥60 years of age with FEV1 ≤50% predicted whom we considered were more likely than a general COPD population to exhibit a suboptimal PIFRresist. Thus, our data are not representative of the spectrum of patients with COPD. Also, we did not study patients with asthma, because these patients are generally younger and would likely be more facile with inhaling medication from a DPI device. Second, we examined PIFR only against the simulated resistance of the Diskus and did not include other DPIs, such as the Aerolizer, HandiHaler, or Turbuhaler. We did this for patient convenience as each patient performed various pulmonary function tests prior to the six PIFR maneuvers at the initial visit. As both the HandiHaler and Turbuhaler have higher internal resistances than the Diskus,4–6,19 it is possible that the prevalence of a PIFRresist of <60 L/min might be higher with these DPIs compared with the Diskus. Third, we did not measure maximal inspiratory pressure (MIP) in our patients. MIP is a major determinant of the ability of a patient to inhale dry powder medications, and has been shown to correlate with PIFR measured against the simulated resistances of various DPIs (r=0.42). 6
Our results identified a phenotype of patients with advanced COPD (female gender, shorter height, and lower values for FVC and IC % predicted) who might be at risk for not being able to completely inhale dry powder medication into their lower respiratory tract. In such patients, it would be important to query each patient whether he/she experiences improved breathing when using a DPI. If the patient reports no clear benefit, then it is reasonable to measure that patient's PIFR against the resistance of the specific DPI. This will require a specific instrument, such as the In-Check DIAL, because PIFR on the flow-volume loop is performed without any resistance and does not provide relevant information for using a specific DPI. Although instruction and practice of the inhalational technique with a DPI are important, 20 Al-Showair and colleagues 5 found no significant increases in PIFRresist through various DPIs after verbal training in patients with moderate to severe COPD. If a patient does not perceive benefit using a DPI and exhibits a PIFRresist of <60 L/min, then it would be reasonable to measure lung function before and after the patient inhales using the dry powder bronchodilator to examine any increase in lung function. An alternative approach would be to consider a different inhalational method, such as a metered-dose inhaler with a spacer or an aerosolized bronchodilator via nebulization.2,2
Footnotes
Acknowledgments
Dr. Mahler developed the research protocol, supervised data collection, reviewed the analysis, and prepared the manuscript. Ms. Waterman assisted in the development of the research protocol, performed statistical analysis, and reviewed the manuscript. Dr. Gifford reviewed and revised the research protocol, performed statistical analysis, and reviewed the manuscript. Sunovion Pharmaceuticals Inc. provided a grant for this investigator-initiated investigation to the Clinical Trials Office at Dartmouth–Hitchcock Medical Center, but had no role in the conduct of the study, data analysis, or manuscript preparation/review. This study was performed at Dartmouth–Hitchcock Medical Center in Lebanon, NH. The authors thank Louis Milanesi, RCPT, Donald Tomlinson, RCPT, and Joseph Ward, RCPT, for performing lung function testing and collecting data on all patients.
Author Disclosure Statement
Dr. Mahler serves as a consultant to Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Sunovion, and serves on advisory boards of DeepBreeze, Forest, GlaxoSmithKline, Merck, Novartis, and Sunovion. The Clinical Trials Office at Dartmouth–Hitchcock Medical Center has received grant support from Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Sunovion for which Dr. Mahler was the principal investigator. Ms. Waterman and Dr. Gifford have no conflicts of interest.