
Abstract
Abstract
Background:
Inhaler orientation with respect to a patient's mouth may be an important variable determining the efficiency of aerosol lung delivery. The effect of insertion angle on regional deposition was evaluated for a series of inhalers using concurrent in vitro and computational fluid dynamics (CFD) analysis.
Methods:
Geometrically realistic physical mouth–throat (MT) and upper tracheobronchial (TB) models were constructed to connect different inhalers at a series of insertion angles relative to the horizontal plane of the model. These models were used to assess albuterol sulfate deposition from the Novolizer® dry powder inhaler (DPI), Proventil® HFA pressurized metered dose inhaler (MDI), and Respimat® Soft Mist™ Inhaler (SMI) following the actuation of a single dose. Drug deposition from Novolizer DPI was studied for Salbulin® and an experimental “drug only” formulation. Albuterol sulfate was recovered and quantified from the device and the MT and TB regions.
Results:
Significant differences in MT and total lung dose (TLD) of albuterol sulfate deposition were not observed for Salbulin Novolizer DPI and Respimat SMI inserted at different angles. In contrast, drug-only Novolizer DPI and Proventil HFA MDI showed a significant difference in MT and TLD deposition using different insertion angles. For drug-only Novolizer DPI and Proventil HFA MDI, the lowest and the highest MT depositions were observed at +10° and −20°, respectively; for Respimat SMI and Salbulin Novolizer DPI, these angles were −10° and +10°, and +20° and −20°, respectively. CFD simulations were in agreement with the experimental results and illustrated shifts in local particle deposition associated with changes in insertion angle.
Conclusion:
The effect of inhaler orientation at the inhaler–mouth interface on MT aerosol deposition appeared to be dependent on velocity, aerosol size, and formulation. These findings not only demonstrate the need for patient education on correct inhaler orientation, but provide important new methods for those designing new inhalers.
Introduction
MT deposition can be dependent on the shape and size of the airway geometry. 3 Significant intersubject variability exists in airway geometries that may be related to differences in height, weight, race, and gender.4,5 Additionally, variables such as position of the tongue during inhalation and airflow resistance of the inhaler can change the shape of the mouth cavity and add to both inter- and intrasubject variability in airway geometry.6–9 Because for most pharmaceutical inhalers, inertial impaction is likely the primary mechanism of MT drug deposition, change in MT shape can significantly change the drug loss in this region. For example, Newman et al. 10 have shown that change in the position of the patient's head while inhaling from an inhaler changed the lung deposition. MT deposition can also be dependent on inhaler design, inhaler airflow resistance, aerosol generation mechanism, and the properties of the generated aerosol, such as aerosol momentum, aerosol density, and plume size.11–13 For example, the Respimat® Soft Mist™ Inhaler (SMI), which delivers a slow aerosol spray, shows considerably lower MT deposition compared with high-velocity spray devices, such as pressurized metered dose inhalers (MDIs).14,15
Unlike most other dosage forms, the drug delivery performance of pharmaceutical inhalers is significantly affected by the way in which patients interact with the device.16,17 It is necessary to educate patients in the use of inhalers to ensure maximum drug delivery efficiency.18,19 However, studies suggest that many patients still do not use their inhalers in a recommended way.20,21 Inhalation at suboptimal flow rates, shallow inhalation, poor coordination, and incorrect inhaler orientation are some of the common mistakes that many patients make. 21 If the inhaler is not used as recommended, it may result in a low and often variable lung dose. 20 Fortunately, in recent years, noticeable efforts have been made in the direction of patient education to minimize such errors. However, these training protocols focus mostly on educating the patients to inhale at the optimal flow rate and rarely correct other errors in technique, such as incorrect inhaler insertion angle at the mouth interface.
In vitro studies using monodisperse aerosols have shown that MT deposition changed as a function of the entry angle. 7 However, the aerosol particle size considered for these studies was significantly larger than that of traditional pharmaceutical aerosols. There are currently a number of open questions related to the effect of inhaler insertion angle on MT drug deposition. It is reasonable to assume that most inhalers are frequently used at angles between +10° and −10° relative to a horizontal axis extending into the mouth inlet; inhaler usage at +20° and −20° is also likely. Considering this potential range of angles, it is unclear if dry powder inhalers (DPIs) or MDIs are more sensitive to insertion angle effects. The high-velocity jets of most DPIs make it likely that the insertion angle is an important factor in MT deposition; the magnitude of this orientation effect on regional deposition could also be formulation-dependent for DPIs. It is not clear if removing the larger carrier lactose particles and producing a more monodisperse aerosol will make MT deposition more or less sensitive to the insertion angle for DPIs. Similarly for MDIs, the inhaler insertion angle may affect the spray momentum associated with the aerosol formation and alter MT drug deposition. Considering SMIs, spray momentum is greatly reduced compared with that of MDIs, 22 which may make these inhalers less sensitive to differences at the patient–device interface. A better understanding of insertion angle effects will potentially improve delivery efficiency and reduce dosage variability to the lungs.
A study was performed to determine the effect of inhaler insertion angle on aerosol deposition using in vitro airway models and concurrent computational fluid dynamics (CFD) simulations. Physical airway models were constructed and used to simulate the airway of an adult inhaling through a DPI, MDI, and SMI, respectively. The inhalers were inserted at a series of different angles relative to a horizontal axis extending into the mouth inlet. CFD simulations were conducted to understand the transport phenomena occurring with different insertion angles and to help interpret the in vitro results.
Materials and Methods
Test inhalers
The MDI used in this study was the Proventil® HFA MDI, which delivers 120 μg of albuterol sulfate as a suspension per actuation from the valve (Schering-Plough, Kenilworth, NJ). The SMI was the Respimat® SMI (Boehringer Ingelheim, Ingelheim, Germany). For Respimat aerosol generation, an aqueous solution formulation (0.6% wt/vol albuterol sulfate in water) was loaded into an empty canister. The DPI was Novolizer® (Meda Pharma GmbH & Co. KG, Bad Homburg, Germany), which was used with two formulations. First, the Salbulin® commercial formulation was implemented, which delivers 120 μg of albuterol sulfate/dose as a drug and lactose blend. Second, a micronized drug-only formulation of albuterol sulfate was considered, which delivers 1,200 μg of albuterol sulfate/dose.
Physical airway models
Physical airway models used in this study were similar to the “medium” airway model described by Delvadia et al. 23 The MT region of the model was based on the elliptical MT geometry defined by Xi and Longest, 24 whereas the upper tracheobronchial (TB) geometry (extended to three generations considering the trachea as generation 0) was developed from the Yeh and Schum 25 lung model by scaling it to match the TB geometry of an average adult as described by Tian et al. 26 The only difference from the previously used model in the studies of Delvadia et al.23,27 was an additional 5-mm inhaler insertion depth in the MT geometries, which was considered important in this study to accurately capture inertial impaction effects on the tongue and back of the throat. To study the effect of inhaler orientation, the mouth inlet of the MT model was customized for each of the three inhalers to produce airtight connections and form insertion angles of −20°, −10°, 0°, +10°, and +20° relative to a horizontal axis extending into the mouth inlet. Negative angles indicate that the inhaler inlet was pointed downward toward the tongue, and positive angles indicate that the inhaler inlet was pointed upward toward the top of the mouth and throat. Figure 1 illustrates the Novolizer attached to the MT models with different insertion angles.
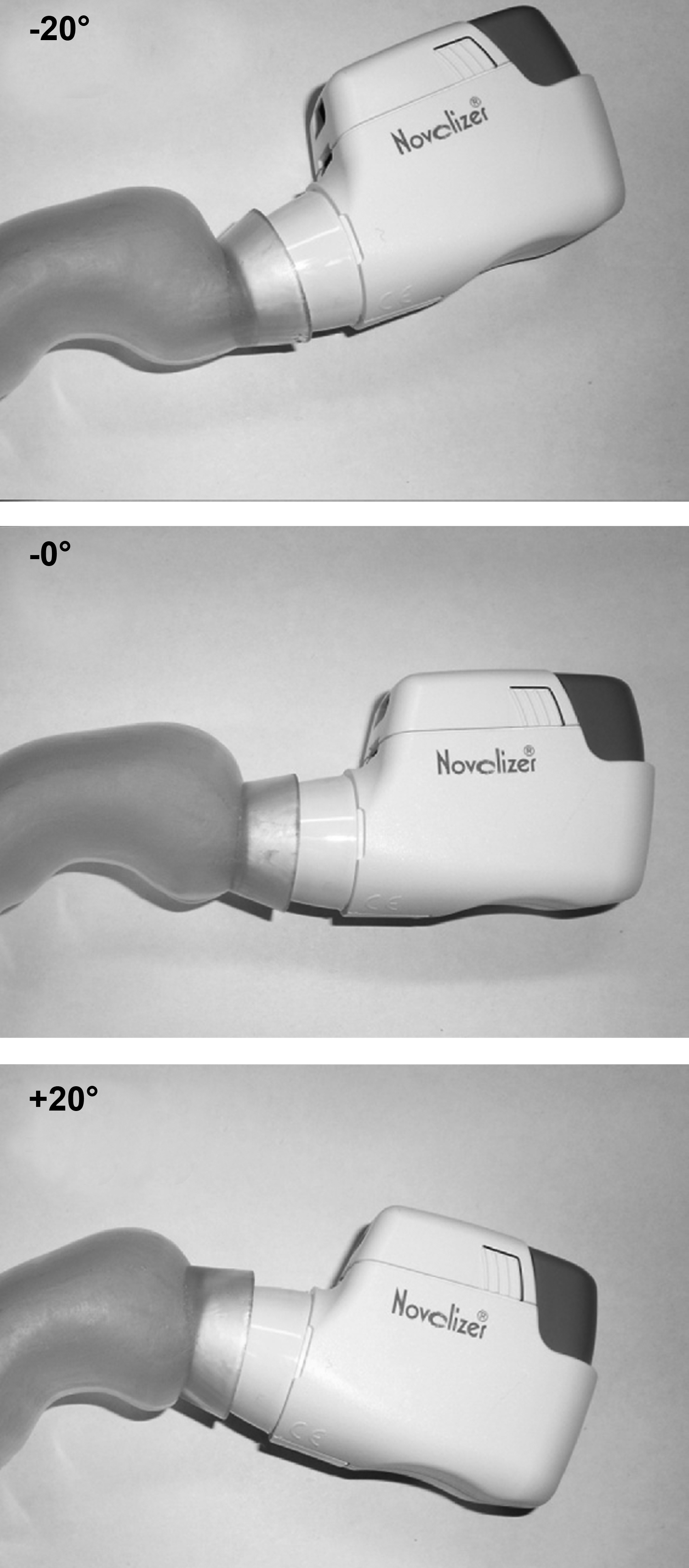
Novolizer DPI attached to the MT geometry at different insertion angles. The insertion angle is measured relative to a plane starting at the center of the MT inlet and extending into the oral cavity. Therefore, negative angles represent the inhaler directed at the tongue, and positive angles represent the inhaler directed at the top of the mouth and throat.
Insertion angle in vitro experiments
Figure 2 shows the experimental setup used to measure the in vitro aerosol deposition from the different inhalers. Previous studies have described the development and validation of this methodology.23,27 The TB region of the airway model was enclosed in an airtight Plexiglas chamber that was connected to a vacuum pump via a low-resistance microbial filter. The internal surfaces of the airway model were coated with glycerol:methanol (1:2) or silicone (Dow Corning® 316 Silicone Release Spray; Dow Corning Corp., Midland, MI) to prevent particle bounce and reentrainment. Single doses were actuated from the inhalers attached to the model using characteristic flow rates and time protocols. For the Proventil HFA MDI and Respimat SMI, a steady flow condition of 30 L/min was established in the model, followed by firing the inhaler and a minimum 10-sec period of airflow after actuation. The Novolizer DPI was actuated using a square waveform with an inlet flow rate of 75 L/min for 3.2 sec using a downstream three-way solenoid valve and vacuum pump. For the spray inhalers, a steady-state profile was considered adequate to differentiate the effects of inhaler angle on deposition, whereas for the DPI a transient waveform was required to actuate the device. In the case of drug-only Novolizer DPI, the MT model was connected directly to the filter, and the TB region and Plexiglas chamber were excluded from the setup. Following each inhalation, albuterol sulfate retained in the device and deposited in the MT, upper TB geometry (if present), and chamber (if present)+filter regions of the model were recovered using appropriate volumes of deionized water. Deposition in the chamber+filter was considered to be total lung dose (TLD). With each inhaler, four replicate experiments were performed for each of the insertion angles.
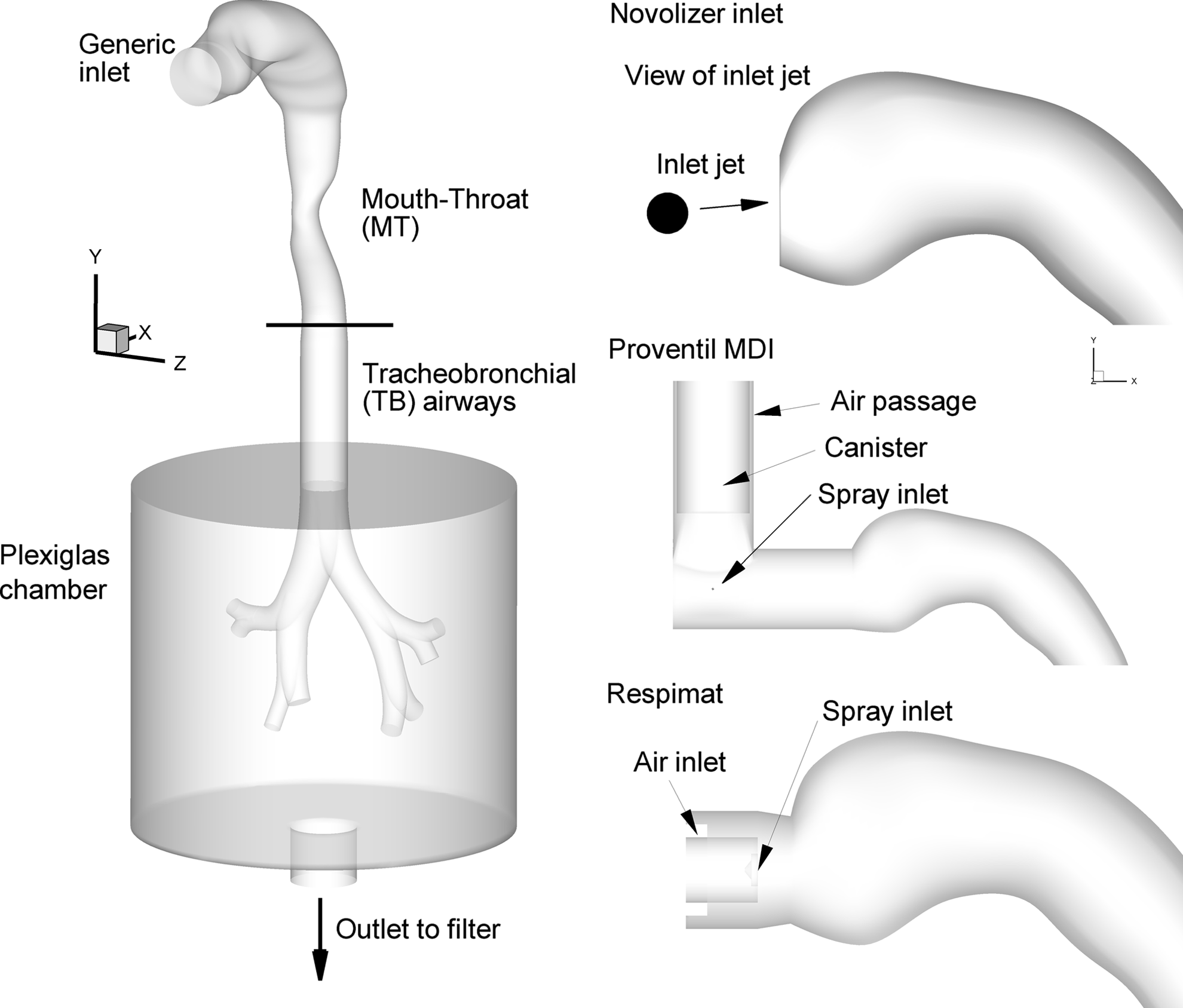
Surface models of the mouth–throat (MT) and upper tracheobronchial (TB) geometry used in the experiments, which extend through the third bifurcation. The in vitro geometry was enclosed in a Plexiglas chamber in order to draw flow through the model and inhalers. Representations of the inhaler inlets are provided in the right-hand-side panels for the Novolizer DPI, Proventil MDI, and Respimat. These inhaler inlet configurations were used as the basis for the CFD geometries at 0° insertion angle.
Aerodynamic particle size distribution determination
Initial aerodynamic particle size distribution data for the aerosols emitted from the inhalers is required for the CFD analysis. Previous studies have reported the initial size distributions for the Proventil MDI and Respimat SMI.14,28 The aerodynamic particle size distributions of the two Novolizer formulations used in this study were determined using a Next Generation Impactor (NGI; MSP Corp., Shoreview, MN). The impactor was held in the vertical orientation, and primed Novolizer inhalers were attached directly to the preseparator. The inhalers were actuated using a constant flow rate of 75 L/min for 3.2 sec (4 L volume). Impactor stages were coated with silicone spray (Dow Corning® 316 Silicone Release Spray) to prevent reentrainment of aerosolized particles. Albuterol sulfate deposited on the impactor stages was recovered using deionized water and quantified using a validated HPLC method. Each experiment was performed four times.
In a separate study, the aerodynamic particle size distributions of the aerosols exiting the −20° and +10° MT models were determined using the NGI for the drug-only Novolizer DPI. In these experiments, the MT model was connected to the preseparator and the DPI was actuated using a flow rate of 75 L/min for 3.2 sec.
Analytical method
Albuterol sulfate concentrations recovered from the different regions of the models, inhalers, and impactor stages were analyzed using a validated isocratic HPLC assay method. The mobile phase was composed of premixed 30% ammonium formate buffer (20 mM, pH 3.4) and 70% methanol. A Restek Allure PFP column (15 mm×3.2 mm, particle diameter 5 μm) was used for separation of albuterol sulfate at a flow rate of 0.75 mL/min and an injection volume of 100 μL. The absorption was measured at 276 nm using Waters 2996 photodiode array (PDA) detector (Waters Corporation, Milford, MA).
Data analysis method
Total drug recovery was calculated as the sum of the individual amounts of drug deposited on the different regions of the model and retained in the device after actuation. Drug depositions in the device, MT, TB, and TLD regions were expressed as percentages of the total drug recovery (drug deposited in region/total drug recovery×100). Statistical analysis of the overall effect of inhaler insertion angle on in vitro drug deposition was performed using one-way ANOVA. Post hoc Tukey's Honest Significant Difference (HSD) test was used to compare the individual angles. The in vitro experimental results were compared with CFD predictions to validate the model results and provide insight about localized drug deposition within the different regions of the MT. Student's t test was used to compare the regional deposition between the different devices. JMP 8 (SAS, Cary, NC) was used for statistical analysis. A significance level of p<0.05 was used in all cases.
CFD model and numerical methods
The inhalers considered in this study produce aerosols using very different mechanisms and are associated with different physical phenomena. The CFD simulations of these systems vary primarily in capturing the physics of the aerosol inlet conditions. Within the MT region, transport becomes more similar among the three inhalers. The MDI flow conditions near the inlet nozzle are transient, multiphase (gas and droplets), multispecies (air and HFA 134a), temperature-dependent, supersonic, and highly compressible. For the Respimat inhaler, spray conditions result in multiphase coupling, but the system can be assumed to be independent of temperature with lower velocities and incompressible flow. 14 The DPI represents the simplest system to model with the added assumptions of one-way coupling between the particle and gas phases. However, accurate modeling of the turbulent flow is required to adequately capture particle dispersion and deposition. Details of simulating each inhaler inlet condition are provided below with frequent references to previous studies by our group. The CFD model and numerical methods for simulating transport and deposition within the MT models are then presented.
For the MDI, inlet air and formulation flows were prescribed as mass flow rates over time. Based on literature values, the expected spray time of the MDI was 0.25 sec 29 and occurred once fully developed flow through the system at 30 L/min was established. To estimate initial conditions of the spray, isentropic flow through the nozzle was considered. The formulation exiting the nozzle was assumed to be at the HFA 134a boiling point for atmospheric pressure and traveling at sonic velocity (i.e., choked flow conditions). Conservation of mass was used to estimate an approximate density of the slurry exiting the nozzle. The thermodynamic pressure at the nozzle exit was determined from the ideal gas law and found to be 127.0 kPa based on HFA 134a properties. This very high static pressure at the nozzle exit experiences a sudden expansion as it adjusts to atmospheric conditions, which can further accelerate the flow, create significant droplet inertia and breakup, and induce high shear stresses in the flow field. Simulation of the expanding gas propellant was assumed to be sufficient to incorporate the effect of the droplet phase on the air flow. Previous applications of this assumption have resulted in good agreement between CFD predictions and in vitro experimental results.22,30
For the Respimat, the previous study of Longest and Hindle 14 indicated that two-way coupling occurred near the spray nozzle inlet. Two-way coupling occurs when the particle phase is sufficiently dense such that it affects heat, mass, and momentum transfer in the continuous phase. Longest and Hindle 14 previously demonstrated that two-way coupling with the Respimat inhaler could be approximated by applying an equivalent inlet air velocity (of 15 m/sec) to the spray nozzle orifice, which has a diameter of 500 μm. This previously developed approach was found to match both the penetration velocity and deposition characteristics of the Respimat aerosol, which is formed by colliding two microjets of high-velocity liquid at an angle, and was applied in the current study. An additional assumption with the Respimat device was the use of rectangular air inlets instead of inlets with rounded corners (Fig. 2). Considering the 1.5-sec firing time of the Respimat inhaler, steady-state conditions were assumed as a reasonable approximation.
The Novolizer device forms an aerosol by passing air over a metered mass of powder, with the initial aerosol passing through a cyclone impactor and then exiting the inhaler through a 6-mm diameter inlet to the MT. The MT inlet is located in the middle of an oval 20×25 mm mouthpiece, which serves to maintain an open mouth position when using the inhaler. The numerical model of the Novolizer consists of this oval geometry with a central 6-mm air jet entering the MT and neglects jet swirl that may be present with this device. Because the air jet enters the MT throughout the inhalation period (∼3 sec), steady-state conditions were again assumed in the numerical model.
To address the complex flow conditions of the multiple inhalers, a low Reynolds number (LRN) k-ω turbulence model was selected. This model has previously been well tested and found to provide good estimates of aerosol transport and deposition in upper airway geometries.31,32 To evaluate the variable temperature and specific concentration fields in the MT-TB model, interconnected relations governing the transport of heat and mass (HFA 134a) were also included. These governing equations were previously presented in detail by Longest et al. 33 In addition to the monodisperse particle deposition studies indicated above, the LRN k-ω approach has also been shown to provide good estimates of transport and deposition for pharmaceutical aerosols generated with a DPI 26 and spray devices including an MDI and SMIs.14,22
A Lagrangian particle tracking model was used to determine the trajectories of individual particles, turbulent dispersion, evaporation, and deposition. This model was implemented using a previously developed combination of a commercial code (Fluent 12; ANSYS, Inc., Canonsburg, PA) and user functions. User routines were used to better model near-wall conditions and to simulate aerosol deposition in the complex three-dimensional multiscale flow field. Previous studies have shown that the isotropic turbulence approximation, which is assumed with the LRN k-ω model, can overpredict aerosol deposition. As a result, a user routine was employed to account for anisotropic near-wall turbulence, as previously described by Longest et al. 33
Droplet and particle initial conditions were set to best match the physics of each inhaler system. For the MDI, particles were initialized at sonic velocity in the HFA 134a propellant (152 m/sec) with a spray angle of 35° over the 250-μm spray orifice. With the Respimat, Longest and Hindle 14 previously determined that an initial droplet velocity of 25 m/sec, spray angle of 20°, and droplets initialized over a 500-μm spray nozzle inlet were appropriate based on the plume penetration characteristics reported by Hochrainer et al. 29 For the DPIs, particles were initialized over the 6-mm jet inlet with a blunt concentration profile, and particle velocities were set to match the local fluid conditions.
Considering the MDI, determining the initial size of the aerosol is challenging. The propellant evaporates very rapidly from the droplets, making a determination of the initial size very difficult. Instead, a size distribution for the Proventil HFA 134a MDI was implemented from the previous study of Cheng et al. 28 with a final dried mass median aerodynamic diameter (MMAD) of 2.2 μm based on impactor testing in an Andersen Cascade Impactor. Evaporation of the MDI droplets is an extremely complex phenomenon involving the vaporization of both propellant and semivolatiles (ethanol) in the presence of surfactant. Longest et al. 30 previously demonstrated that MDI deposition could be accurately simulated with a CFD model by initializing the spray with the final dried polydisperse size distribution and simulating the transport of these solid drug particles. This dried particle approach is implemented in the current MDI simulations for the Proventil suspension, and the quality of this assumption will be evaluated based on comparisons with in vitro measurements of drug deposition.
For the Respimat aerosol, the size distribution was based on the previous measurements of Longest and Hindle. 14 In brief, a laser diffraction system (Spraytec; Malvern Instruments Inc., Southborough, MA) was implemented to determine the size distribution of the aerosol as it exited the Respimat spray nozzle. To assess the size distribution in a relatively stable section of the aerosol plume, the center of the laser was positioned 1.5 cm away from the spray nozzle unit, and 30 L/min of co-flow air was pulled around the nozzle during size analysis.
Aerosol size distributions for the Salbulin and drug-only Novolizer were based on the experimental measurements reported in this study. Hygroscopic growth of the DPI aerosol was excluded to match the in vitro test conditions and is not expected to be large in the upper airways.
To determine the deposition of drug mass for the polydisperse aerosols considered, an equal number of particles were simulated in each of the size bins of the aerosol characterization device. Deposition fractions for each size bin were then combined with the initial polydisperse distribution of the aerosol in order to determine the correct deposition of drug mass. Simulations of polydisperse aerosol deposition from pharmaceutical inhalers are discussed further by Longest et al. 33 For the Novolizer simulations, approximately 36,000 total particles were injected under steady-state conditions. With the Respimat, steady-state simulations of droplet deposition were resolved with 52,000 initial droplets. Simulations of the MDI required a transient solution due to the spray burst of propellant release. 12 As a result, 240,000 droplets were modeled to resolve both the polydisperse aerosol and transient solution.
In performing the CFD simulations, previously established best practices were implemented. All transport equations were discretized to be at least second-order accurate. The computational mesh was constructed in Gambit 2.4 (ANSYS, Inc.) and consisted entirely of hexahedral elements, which provide a higher quality solution than commonly used tetrahedral grids. Grid convergence based on maximum velocity and deposited drug mass was established for approximately 300,000–500,000 control volumes. Characteristic mesh sizes near the MDI spray nozzle and MT wall boundaries were 0.005 mm and 0.1 mm in the wall-normal direction, respectively.
Results
Effect of insertion angle on in vitro deposition
Tables 1 and 2 show the effect of inhaler insertion angle on the in vitro aerosol deposition from the Salbulin Novolizer DPI and drug-only Novolizer DPI, respectively. All drug recoveries for the Novolizer were more than 90% of the nominal dose. Device retention differed significantly between the two formulations (Student's t test, p<0.05) using the Novolizer. For the Salbulin formulation, device retention was low, about 4%; however, there was high MT deposition. In contrast, using the drug-only formulation, about 25% of the dose was retained in the device, and this was accompanied by lower MT deposition. For the Salbulin formulation, one-way ANOVA analysis showed no significant difference in device, MT, TB, and TLD deposition using the different insertion angles (p>0.05). The lowest and highest MT depositions for the Salbulin formulation were observed at +20° and −20°, respectively, with the nominal absolute insignificant difference of 4.18%. In contrast, for the drug-only Novolizer DPI, there was a significant effect of insertion angle on the MT and TLD deposition (one-way ANOVA, p<0.0001). More specifically, there were significant increases in MT deposition when the Novolizer was inserted at the −20° and −10° compared with 0° (Tukey's HSD). However, when the DPI was inserted at +10° and +20°, there was no significant change in MT deposition compared with horizontal. For the drug-only Novolizer DPI, the lowest and highest MT deposition was observed at +10° and −20° insertion angles, respectively, with a significant absolute difference of 8.79%.
Data are presented as the means (SD) for n=5.
Data are presented as the means (SD) for n=5.
MT model was connected directly to the filter; the TB region and Plexiglas chamber were excluded from the setup.
p<0.05, significant effect of insertion angle on MT and TLD deposition (one-way ANOVA).
p<0.05, significant effect of insertion angle on MT and TLD deposition compared with 0° (post hoc Tukey HSD).
Table 3 shows the effect of inhaler insertion angle on the in vitro aerosol deposition from the Proventil HFA MDI. In this case, the drug recoveries were all more than 95% of the nominal dose. Device retention on the MDI (actuator and mouthpiece) was about 15% of the dose and was not affected by insertion angle. MT deposition was lower for the Proventil MDI compared with the Salbulin Novolizer DPI for all insertion angles (Student's t test, p<0.05). However, there was a significant effect of insertion angle with the MDI on the MT and TLD deposition. Post hoc analysis revealed a significant increase in MT deposition for the −10° and −20° insertion angles compared with 0°. This trend was similar to the results observed for the drug-only Novolizer DPI. In the case of Proventil HFA MDI, the lowest and highest percent MT depositions were observed at +10° and −20° interface angles, respectively, with a significant absolute difference of 11.34%.
Data are presented as the means (SD) for n=5.
TB deposition was below the limit of quantification (below 1% of the nominal dose).
p<0.05, significant effect of insertion angle on MT and TLD deposition (one-way ANOVA).
p<0.05, significant effect of insertion angle on MT and TLD deposition compared with 0° (post hoc Tukey HSD).
Table 4 shows the effect of inhaler insertion angle on the in vitro aerosol deposition from the Respimat SMI. Drug deposition in the device and MT was less than 30% of the recovered dose, which resulted in a high pulmonary fraction compared with the MDI and DPI. There was no significant change in percent deposition in any region with change in Respimat SMI insertion angle (one-way ANOVA, p>0.05). The lowest and highest MT depositions for Respimat were observed at −10° and +10°, respectively, with the nonsignificant absolute difference of just 2.47%.
Data are presented as the means (SD) for n=5.
Initial particle size distributions
Initial particle size distributions for the Salbulin Novolizer and drug-only Novolizer DPIs are provided in Figure 3 based on cascade impactor testing. As described, the DPI formulation combinations were actuated with a square waveform profile and a flow rate of 75 L/min. The MMAD values for the Salbulin and drug-only formulations with the Novolizer were calculated to be 1.96 μm and 2.44 μm, respectively, excluding the preseparator fraction and based on midpoint diameters. As expected, the carrier-based Salbulin formulation has much higher drug loss in the preseparator, which is represented in Figure 3 as the particle size fraction at 12 μm.

Aerosol size distributions based on drug mass as a function of NGI midpoint diameters for each stage with the Salbulin Novolizer DPI and drug-only Novolizer DPI. Aerosols from the Novolizer were sized at a flow rate of 75 L/min and a square waveform. The MMADs of the Salbulin and drug-only Novolizer aerosols were 1.96 and 2.44 μm, respectively.
CFD analysis of insertion angle effects
Velocity fields in terms of vectors and speed contours sampled at the geometric midplane of the MT model are presented in Figure 4 for the three inhalers at the angles of −20° and +20°. In all cases, a jet of gas flow is observed to exit the inhaler mouthpiece and interact with the walls of the MT geometry. For the DPI, the jet arises from the relatively small 6-mm orifice inlet. With the spray inhalers, the jet is created by evaporation of the propellant and entrained air for the MDI or the mouthpiece configuration for the Respimat SMI. As expected, negative angles clearly create jet interactions with the tongue region, and positive angles cause jet interaction with the top of the mouth and throat (in the region of the soft pallet). Based on jet-velocity vector magnitudes, strong jet interactions are observed with the walls of the MT geometry for the DPI and MDI systems. In contrast, the reduced velocities of the Respimat SMI mitigate interaction between the jet of air entering the MT and the wall boundaries. For all cases, significant recirculation is observed to occur in the midplane, which reduces the cross-sectional area available for downstream flow and increases the potential for particle impaction with the walls. These recirculation regions appear to be enhanced due to the positive and negative angles of the inhalers.
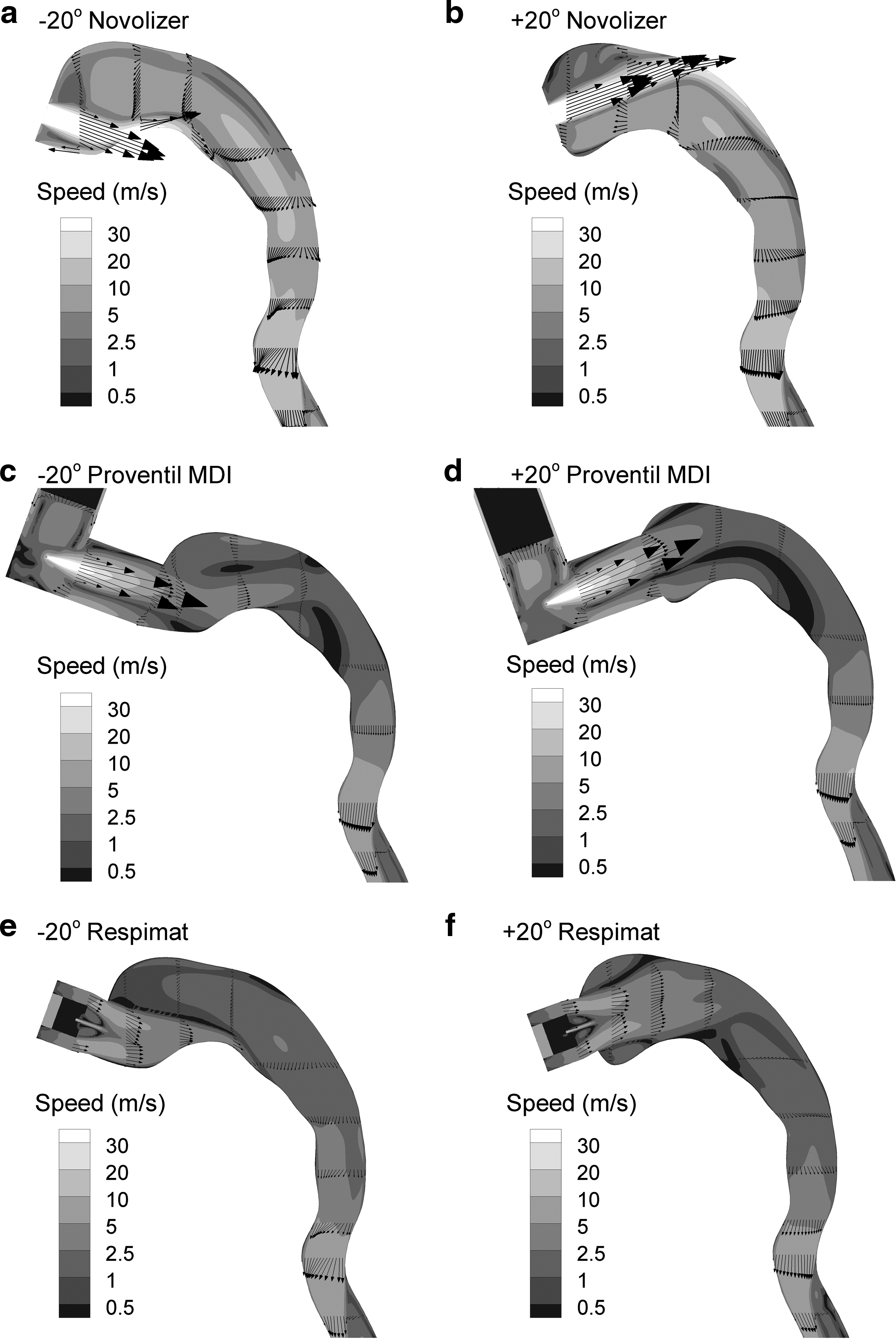
Velocity vectors and contours of velocity magnitude for the
Predicted particle deposition locations are illustrated in Figure 5 based on the CFD model for the three inhalers at −20° and +20°. In all cases, increased deposition is observed to shift from the tongue region for negative inhaler angles to the top of the throat for positive angles, as expected. This shift is qualitatively observed to be most significant for the MDI, which also had the highest change in MT deposition as a function of inhaler angle based on the experiments. In contrast, relatively little difference in local deposition is observed with the Respimat SMI for the two angle cases considered. Therefore, the inhaler angle has the largest effect on local deposition for the inhalers with the strongest jet velocities (MDI and DPI) and relatively little effect as jet velocity is reduced, as with the Respimat SMI. Furthermore, increased deposition with negative angles (compared with the positive angle cases) appears to be associated with increased local deposition on the tongue.
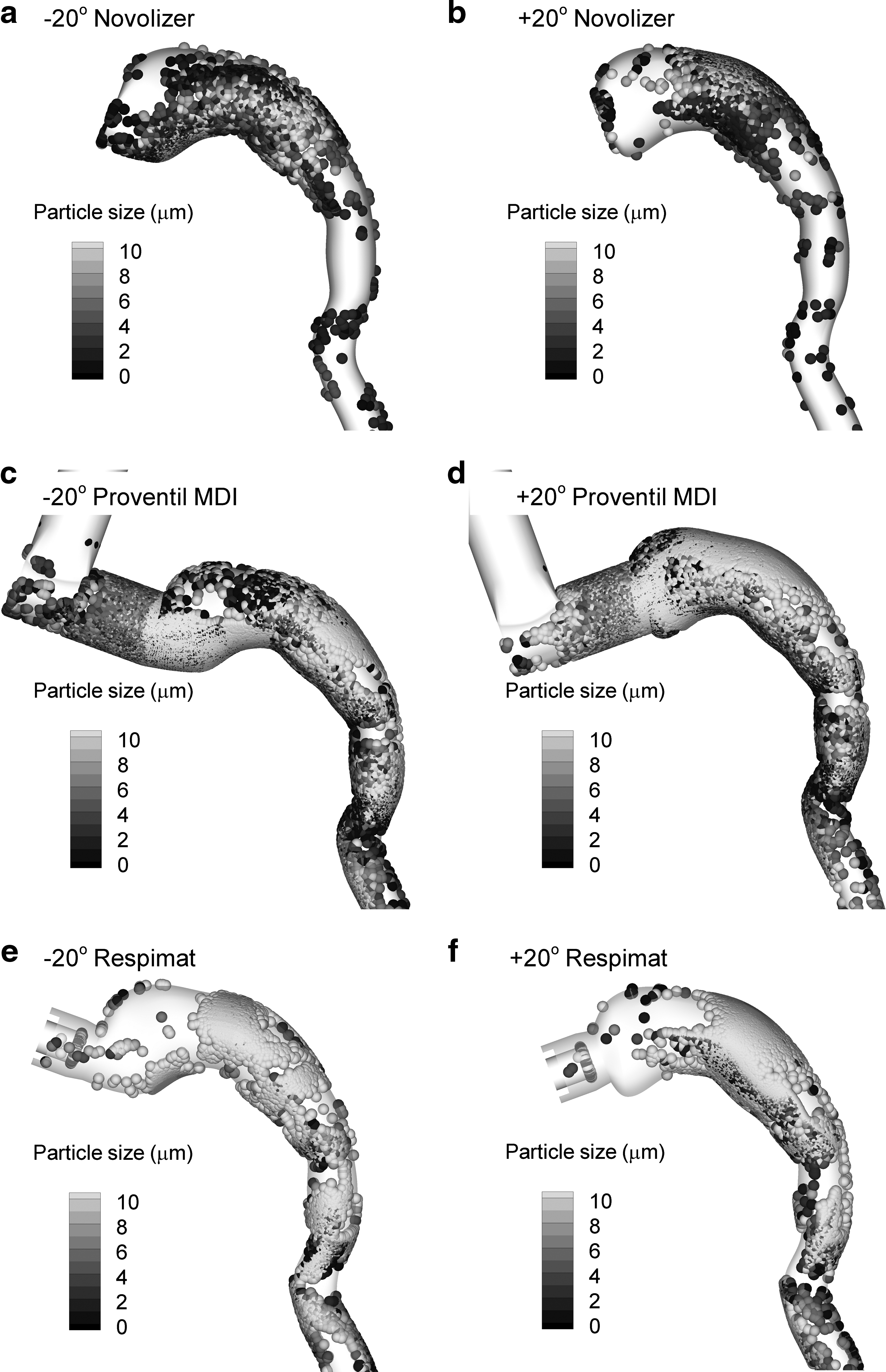
Locations of simulated polydisperse aerosol deposition for the
A comparison between the in vitro results and CFD predictions of MT deposition fraction for all inhalers evaluated at the extreme angles of −20° and +20° is illustrated in Figure 6. In general, the CFD model matches the mean deposition fractions from the experiments in each case along with the trend in reduced MT deposition for positive angles relatively well. Reasons for the somewhat higher CFD values compared with the experiments in some cases are presented in the Discussion.

Comparison of MT deposition fractions between the in vitro experiments and CFD results for the angle cases of −20° and +20° with each inhaler.
Effect of insertion angle on aerosol size distribution exiting the MT
Figure 7A compares the mass fraction of albuterol sulfate deposited in the MT and impactor from the drug-only Novolizer DPI inserted at −20° and +10° angles, which represent the maximum and minimum extremes of MT deposition for this inhaler. In this setup, the MT was connected directly to the preseparator leading to the NGI. There was a significant difference in percent deposition at impactor stages 2, 3, 4, and 5 (Student's t test, p<0.05) between these two insertion angles. Figure 7B depicts the percent differences in the impactor deposition (percent delivered dose) between +10° and −20° angles shown in Figure 7A, which were calculated from

Comparison of cases −20° and +10° for the drug-only Novolizer DPI in terms of
Differences in impactor deposition were found to be particle size dependent (Figure 7B); % difference increased with increase in particle size (for NGI stages S7 to S2), indicating a change in the impaction deposition with change in angle.
Discussion
In this study, the effect of inhaler insertion angle on in vitro drug deposition in an airway model was investigated. The airway model was evaluated using both experimental and CFD techniques to gain further insight into the critical factors controlling MT deposition for a DPI, MDI, and SMI. Results of the CFD simulations for the four inhalers considered were generally consistent with the experimental results and provided insight into the changes in deposition fraction associated with inhaler insertion angle.
Based on the results of this study, it is observed that aerosol momentum is the key parameter that determines the degree to which inhaler angle will affect deposition. Momentum is the product of velocity and mass and is directly proportional to the probability of aerosol deposition by inertial impaction. That is, higher momentum systems have higher inertial impaction based on Newton's second law. As an approximation of momentum for aerosols in the MT region, the speed of an air or gas jet from an inhaler as the jet approaches a boundary provides an estimate of velocity. The initial MMAD of the droplets and particles considered provides a direct association with aerosol mass. High-momentum systems have high inertia, which reduces the ability of the aerosol to change direction at sites where it encounters a boundary. Based on CFD observations, inhaler angle can affect deposition at the wall boundaries of the tongue and on the upper portion of the throat. Reduced deposition associated with positive angles in this study occurs because the longer travel distances to the top of the throat allow for reduced velocities and more time for the aerosol to change direction before impaction occurs. Based on momentum, systems with higher jet velocities entering the MT and larger MMADs are expected to be more sensitive to inhaler insertion angle. Reducing either jet velocity or particle size decreases system momentum and, hence, will decrease impaction and the effect of inhaler angle on deposition in the MT.
The observation that increased momentum increases the effect of inhaler angle on MT deposition is supported by Figure 7B. This figure illustrates that as aerosol size increases from stage 7 (0.29–0.48 μm) to stage 2 (3.97–7.15 μm), the percent difference in aerosol deposition associated with inhaler angle increases, almost exponentially. However, this direct relationship appears to have a limit. It is interesting that as size is increased beyond stage 2, inhaler angle has a diminished effect on deposition. This drop-off occurs because, after the aerosol reaches a critical size, the ability of the aerosol to pass through the MT region is reduced regardless of inhaler angle. Therefore, increasing the aerosol size results in an increase in momentum and associated increase in angle effect up to a point. This relationship is then limited by the aerosol size that cannot effectively pass through the MT geometry.
Significant effects of inhaler angle on MT deposition were observed for both the Proventil HFA MDI and drug-only Novolizer DPI. In contrast, the Salbulin Novolizer DPI and Respimat SMI showed no significant effect of inhaler angle on variability in MT deposition. These findings are consistent with the expectation that systems with high aerosol momentum will be more sensitive to inhaler angle effects. For the Proventil MDI, spray velocity is maximum among the systems considered (Fig. 4). The MDI aerosol is either larger than with the other inhalers (before evaporation) or a consistent size with the DPIs (∼2 μm). Therefore, the Proventil MDI is predicted to have the highest momentum and, therefore, the largest effect of inhaler angle on deposition, as observed in vitro. In contrast, the Respimat SMI is predicted to have the lowest momentum of the systems considered. This is evident from the low velocities observed in Figure 4. The Respimat has a relatively large MMAD compared with the other inhalers (5.3 μm); however, the large reduction in jet velocity creates the lowest momentum system of the three inhalers considered. This observation is consistent with the in vitro finding that the Respimat inhaler had a negligible association between insertion angle and MT deposition.
Considering the Novolizer, it is interesting that the drug-only formulation was affected by angle, whereas the Salbulin formulation was not. In both systems, the flow field and jet velocities entering the MT and interacting with the top of the throat and tongue are the same. Differences in momentum of the aerosol are then controlled by the aerosol size. Excluding the preseparator drug fraction, the drug-only formulation has the larger MMAD of the two DPI cases (2.44 vs. 1.96 μm) resulting in a higher momentum system. Therefore, it is reasonable that the drug-only Novolizer DPI would be more affected by inhaler angle, as demonstrated in vitro. Furthermore, it is expected that the significant fraction of large particles from the Salbulin formulation is associated with decreasing the sensitivity of this inhaler to insertion angle. Based on Figure 3, approximately 47.2% of the Salbulin formulation is deposited in the preseparator, and likely represents agglomerated drug and lactose particles (where the lactose carrier has an MMAD of approximately 60 μm). These large particles deposit in the MT regardless of the inhaler angle and, therefore, diminish the effect of inhaler angle on deposition fraction. It is concluded that the Salbulin formulation is less affected by insertion angle, and this reduced sensitivity is partly associated with drug remaining on large lactose carriers and high MT deposition. These observations imply that new drug-only formulations with DPIs may be more sensitive to variations in insertion angle. However, the high MT deposition values associated with the Salbulin Novolizer DPI may not be the best solution for reducing sensitivity to inlet angle. Reducing the size of the drug-only formulation and the associated aerosol momentum, potentially by using less cohesive formulations, will likely reduce the observed insertion angle effect.
CFD analysis revealed that inserting each of the three inhalers in a downward directed position (–20° case) results in additional aerosol deposition on the tongue (Fig. 5a, c, and e), whereas inserting the inhalers in an upward-directed position results in more deposition on the back of the throat (Fig. 5b, d, and f). It is interesting that for all inhalers being studied, change in MT drug deposition due to orientation change was not always accompanied by a corresponding change in the TB deposition. Also, changing the angles from +10° to +20° did not significantly change MT deposition for any of the inhalers.
Limitations of the current study relative to in vivo conditions include a static MT geometry and single tongue position, use of a single characteristic MT model, and steady-state or square-wave simulated breath profiles. It was assumed that the angle of the devices in the range of −20° to +20° did not influence the initial size distributions of the aerosols. This assumption is supported in part by similar depositions in the devices at different angles based on the in vitro experiments (Tables 1–4). It is also noted that these results are based on only one characteristic flow rate for each device. For the CFD model, assumptions of steady flow and no droplet evaporation with the Respimat inhaler may be responsible for overpredicting deposition fractions. Reasons for overpredicting the particle deposition of the drug-only Novolizer aerosol are not clear; however, one possible explanation is the difficulty in estimating the size fraction of the aerosol that deposits in the inhaler connections and preseparator during the in vitro sizing experiments.
Previous studies in this series have emphasized the need to consider a range of MT-TB geometries and correct inhalation waveforms to predict in vivo measured intersubject variability for a single DPI 23 and in vivo mean drug delivery for a range of DPIs. 34 The effect of transient inhalation waveforms on MT and TB deposition has also been emphasized in previous studies for DPIs 26 and MDIs. 30 In the current study, the focus was to implement the previously developed MT-TB geometry to assess the effect of inhaler insertion angles. To better isolate the effect of insertion angle and to simplify the experiments, a single mean MT geometry was implemented and a steady-state (MDI and Respimat) or square-wave (DPI) inhalation condition was used. Implementation of steady-state or square-wave inhalation profiles is beneficial, because the initial aerosol size can be measured with cascade impaction and then implemented in the CFD model. Realistic transient inhalation profiles may influence the MT deposition and lung delivery of the inhalers considered in this study. However, transient inhalation is not expected to largely influence the results of this study in terms of evaluating the relative effects of inhaler insertion angle on MT deposition and TLD.
Factors affecting MT deposition and lung delivery of an aerosol can be categorized as parameters that can and cannot be controlled by the patient. The previous study of Delvadia et al. 23 indicated that airway size combined with characteristic inhalation resulted in lung delivery that varied by a factor of 4 in some cases for a high-quality DPI device. Similarly, the type of inhaler prescribed by the physician can influence lung delivery of the aerosol or TB delivery by a factor of approximately 2.30,34 In contrast, Longest et al. 30 previously showed that correct versus incorrect inhalation waveforms with DPI and MDI inhalers influenced lung delivery by a relative difference of approximately 30%. Similarly, the patient-controlled factor of inhaler angle considered in this study produced relative differences of 30% MT deposition in some cases. Based on these studies with in vitro models, it appears that patient-controlled factors often have a less significant impact on lung delivery of a drug compared with many factors that are beyond the patient's control. However, factors that can be controlled by patient education, such as correct inhalation and inhaler angle, can help to reduce intersubject variability for size groupings of individuals and improve the performance of specific inhalers. Quantifying the effects of insertion angle across a range of inhalers can also help to make patient instructions as simple as possible. For example, results of this study indicate that instructions for correct inhaler angle may not be needed for some inhalers.
It is expected from this study that, for some inhalers, the correct inhaler orientation can reduce not only intersubject but also intrasubject variability. In this regard, it is important to recognize that inhaling at the optimal flow rate alone does not produce the maximum lung dose, and it is equally important to educate the patients about the correct way to hold the inhaler during inhalation for some devices. This finding is of significance given the fact that most patients do not appreciate the need for holding the inhaler at correct orientation. The CFD model highlighted significant differences in deposition locations (tongue vs. back of the throat). Large depositions on the tongue or back of the throat may have implications for taste perception and tissue irritation. Results of this study demonstrate that doses on the tongue and back of the throat, and associated side effects, can be controlled with simple angle changes of the inhaler.
Conclusions
Changing the angle at which an inhaler is inserted into the mouth may have significant effects on aerosol behavior within the MT region, but deposition is only affected for some inhalers with specific formulations. The magnitude of inhaler orientation effects on MT deposition is clearly dependent on aerosol momentum, i.e., stronger effects when the product of jet velocity entering the airways and aerosol size is relatively high. The magnitude of the orientation effect for DPIs can also be formulation-dependent. For example, use of adhesive formulations (course lactose+micronized drug) may make DPIs less susceptible to the orientation effect compared with the use of drug only formulations. This study demonstrated that inhaling at the optimal flow rate alone does not warrant the maximum lung dose, and it is equally important to educate patients about the correct way to hold certain inhalers during use. Our future studies will focus on assessment of other variables such as mouthpiece insertion depth, variable head orientation, and tongue position on regional aerosol drug deposition.
Footnotes
Acknowledgments
Assistance with constructing the MT geometries to accept inhalers at different angles and the composite MT-TB geometry from Geng Tian and Ross Walenga (VCU School of Engineering) is gratefully acknowledged.
Author Disclosure Statement
The authors are faculty and students of Virginia Commonwealth University. The work was supported in part by funds from the Medical College of Virginia Foundation. Supplies and inhalers were purchased from commercial sources. No conflicts of interest exist.