
Abstract
Abstract
Background:
Aerosol therapy in preterm infants is challenging, as a very small proportion of the drug deposits in the lungs.
Aim:
Our aim was to compare efficiency of standard devices with newer, more efficient aerosol delivery devices.
Methods:
Using salbutamol as a drug marker, we studied two prototypes of the investigational eFlow® nebulizer for babies (PARI Pharma GmbH), a jet nebulizer (Intersurgical® Cirrus®), and a pressurized metered dose inhaler (pMDI; GSK) with a detergent-coated holding chamber (AeroChamber® MV) in the premature infant nose throat-model (PrINT-model) of a 32-week preterm infant (1,750 g). A filter or an impactor was placed below the infant model's “trachea” to capture the drug dose or particle size, respectively, that would have been deposited in the lung.
Results:
Lung dose (percentage of nominal dose) was 1.5%, 6.8%, and 18.0–20.6% for the jet nebulizer, pMDI-holding chamber, and investigational eFlow nebulizers, respectively (p<0.001). Jet nebulizer residue was 69.4% and 10.7–13.9% for the investigational eFlow nebulizers (p<0.001). Adding an elbow extension between the eFlow and the model significantly lowered lung dose (p<0.001). A breathing pattern with lower tidal volume decreased deposition in the PrINT-model and device residue (p<0.05), but did not decrease lung dose.
Conclusions:
In a model for infant aerosol inhalation, we confirmed low lung dose using jet nebulizers and pMDI-holding chambers, whereas newer, more specialized vibrating membrane devices, designed specifically for use in preterm infants, deliver up to 20 times more drug to the infant's lung.
Introduction
In the case of bronchodilators, low lung deposition in preterm infants might be sufficient, particularly when corrected for body weight. Fok et al. showed that nebulization with standard devices results in a clinical response, 7 but optimal dosage per kilogram of body weight—per nebulizer type—is still unclear. 8 Optimizing nebulizer efficiency might offer new therapeutic options. Use of newer technology has been shown to achieve higher lung delivery efficiency in ventilated macaques (up to >14% with vibrating membrane nebulizers), 9 but thus far this has not been shown in spontaneously breathing infants. In adults, lung deposition with an investigational PARI eFlow® (including a small valved holding chamber) was 38±4.3% (mean±SD) of nebulizer charge. 10
Important factors influencing lung deposition are the particle size produced by the device, mechanical dead space, residual volume, and, for jet nebulizers, flow requirements. Also, a non-tightly fitted face mask greatly reduces drug delivery to the patient.11,12
In this study, we evaluated lung deposition of salbutamol as a drug marker using a standard jet nebulizer (Intersurgical® Cirrus®), a pMDI (GSK) with a detergent-coated holding chamber (AeroChamber® MV), and two vibrating membrane nebulizers (PARI Pharma's investigational eFlow nebulizer prototypes for babies) simulating two clinical conditions by applying different breathing patterns. To facilitate clinical use, two elbow extensions positioned between the model and the eFlow nebulizer were tested.
Methods and Materials
Upper airway model
The premature infant nose throat-model (PrINT-model) is described extensively elsewhere. 13 In short, this upper airway model corresponding to a premature infant of 32-weeks gestational age (1,750 g) was developed from a three-planar magnetic resonance imaging scan. It was constructed using three-dimensional printing and a photopolymer (FullCure® 720) and validated by comparison of total airway volume with a high-resolution computed tomography scan. The model includes the upper airways from the nostrils down to 4 mm below the vocal cords, and the mouth is closed. With a corresponding breathing pattern, the model has proved to be valuable in assessing aerosol delivery. 13
Devices and face masks
A standard jet nebulizer [Intersurgical Cirrus®, Berkshire, UK; 3.5 μm volume median diameter (VMD)] with a bottom-loaded vented infant face mask (Unomedical®) was evaluated and compared with a pMDI (Allen & Hanburys, GSK, Middlesex, UK) with a detergent-coated holding chamber without valve (AeroChamber® MV) and Laerdal® infant mask (unvented). In addition, two vibrating membrane nebulizers were tested, both with a front-loaded PARI SmartMask® Baby mask (vented): the prototype investigational eFlow nebulizers for babies, one with a small (eFlowSR) and one with a large (eFlowLR) reservoir (PARI Pharma GmbH, Munich, Germany; 3.0 μm VMD). The size of the laser-drilled holes in the aerosol generator (vibrating membrane) of the eFlow devices determines the particle size of the aerosol. The investigational nebulizers are designed to have a low residual volume.
The jet nebulizer was run at 6 L/min until at least 30 sec after sputtering commenced. The pMDI canister (Ventolin, 100 μg per actuation) was shaken for 15 sec and attached to the holding chamber after five waste actuations. The ratio of actuation/breaths was 1:10, and actuation cycles were repeated five times [nominal dose (ND) 500 μg]. Between cycles, the canister and actuator were shaken again for 5 sec. The vibrating membrane devices were run continuously until nebulization stopped.
Using the eFlowSR, two different elbows with a corner of 45° and 90° (to optimize the angle between patient and nebulizer to facilitate clinical use) were compared with no elbow.
Experimental setup
Face masks with attached nebulizer were fitted tightly to the PrINT-model using Parafilm® (Brand GmbH, Wertheim, Germany). The vents in the face masks were not covered. The airway model was attached to a modified 22-mm T-piece below the tracheal opening to create an additional dead space of 2.2 mL on top of 1.3 mL dead space from the airway model. Total dead space was 3.5 mL, corresponding to the airway dead space in infants weighing 1,750 g. In setup A (Fig. 1A), a filter was attached to the T-piece to measure lung dose (LD); in setup B (Fig. 1B), the filter was replaced by a Next Generation Impactor™ in order to measure particle size at the tracheal opening of the airway model.

Experimental setup
Both the filter and the impactor setups were performed using a constant flow through the system commonly used in impactor measurements. In all setups, the air flow through the filter and the impactor was kept constant at 15 L/min using a suction device and a mass flow controller (Analyt-MTC, Modell GFC, Müllheim, Germany). This flow was independent from any driving flow of a nebulizer, as the nebulizer was attached to the model and not included in the circuit. Aerosols that were actively inhaled through the airway model entered this constant flow circuit. A zero flow at the tracheal opening of the PrINT-model was balanced by applying a regulated blowing airflow of 15 L/min to the side port of the T-piece (Fig. 1). Humidity and temperature were kept constant at 50% relative humidity (±3%) and 23°C (±1°C). To prevent dripping of collected drug from the upper airways onto the filter, the setup was turned upside down (this was not possible using the jet nebulizer with bottom-loaded face mask and when performing the particle size measurements with impactor for the jet nebulizer and the prototype investigational eFlow nebulizer). The impactor was cooled to prevent evaporation.
Nebulizer, elbow, PrINT-model, modified T-piece, and (lung) filter were washed separately with 22.5 mL of methanol. A total of 2.5 mL of NaOH (0.1 mol/L) was added to each wash, and subsequently absorbance of salbutamol was measured with a spectrophotometric method (Shimadzu UV-1601; Shimadzu, Kyoto, Japan; wavelength 276 nm). All face masks were excluded from drug analysis due to leaching of softeners and colors when washed in methanol, which interfered with the absorbance measurements.
All experiments were repeated six times.
Definitions
Total output rate has been calculated from the weight difference of the nebulizer before and after nebulization. Lung dose (LD) was drug deposition in the filter or impactor including deposition in the T-piece. Drug deposition on the PrINT-model (PD) was determined separately for deposition on the face (FD) and deposition on the inner airways of the model (AD). Inhaled mass (IM) was defined as LD plus PD. Device residue (DR) was determined including deposition in the elbow, as the output of the device was defined as amount of aerosol available for inhalation at the face mask. All values were expressed as a percentage of ND, with ND defined as total amount of drug filled in the device. Values were also calculated as a percentage of emitted dose (ED; total amount of drug exiting the device).
Breathing patterns
Two different breathing patterns were used (Harvard Rodent Ventilator, Model 683, Harvard Apparatus, Holliston, MA): (1) a “high” breathing pattern (HBP) with a tidal volume of 12 mL and a respiratory rate of 80 breaths per minute (bpm) resembling an infant in distress; and (2) a “low” breathing pattern (LBP; tidal volume of 8.75 mL and frequency of 60 bpm), which reflects a physiologic breathing pattern of a quiet infant.
Statistical analysis
DR, LD, and PD were compared using one-way analysis of variance (p<0.05). Subsequently, if significance was present, comparisons were made for each pair of means. As we compared four devices, six pairwise comparisons were made using Bonferroni's correction for multiple testing with significance level p=0.008 (0.05/6), and three pairwise comparisons for the three elbow setups with p=0.017 (0.05/3). Independent-samples t tests were used to compare the difference in deposition variables between the two breathing patterns and deposition in the two elbows.
The correlation between DR and PD or LD was investigated using Pearson's correlation coefficients (SPSS Statistics, 17.0; SPSS, Chicago, IL).
Results
Four aerosol delivery devices
LD was significantly lower for the jet nebulizer [1.5% of ND (0.2), mean (SD)] and pMDI-holding chamber [6.8% (1.0)] compared with the investigational eFlow nebulizers with small and large reservoir: 18.0% (1.7) and 20.6% (1.8), respectively (p<0.001; Fig. 2). In all experiments, higher DR was strongly correlated with lower LD (r=–0.98, p<0.01) and lower PD (r=−0.98, p<0.01). LD and PD were positively correlated (r=0.98, p<0.01). Analysis of all experiments using the ED gave similar results.

LD, DR, and PD for four aerosol devices. IM is PD plus LD. Data represent means + SD and are expressed as a percentage of ND. The HBP was applied. All differences between devices are significant (p<0.001), except differences in PD and DR between eFlowSR and eFlowLR, and the difference in LD is p=0.023.
Breathing patterns
An LBP (reflecting physiological quiet tidal breathing) decreased PD (p<0.05). However, it did not decrease LD (Fig. 3A), and DR was only significantly affected for the jet nebulizer and the membrane nebulizer with elbow (Fig. 3B). Details for deposition as a percentage of the ND are presented in Table 1.

See also Figure 2. Analysis using the ED gave similar results.
Elbow experiments
Adding an elbow extension to the membrane nebulizer did decrease LD (Fig. 4). The corner of 90° in the elbow even further decreased IM compared with the 45° elbow (p<0.001). Deposition in the 45° elbow itself was 13.3% of ND (1.1) versus 15.7% (2.7) in the 90° elbow (p=0.09). The 90° elbow had two small vents, which were closed with Parafilm in three additional runs. This did not have an effect on LD [open 7.3% (1.7) and closed 7.6% (0.7)] and PD [11.2% (1.1) to 12.4% (0.2)].
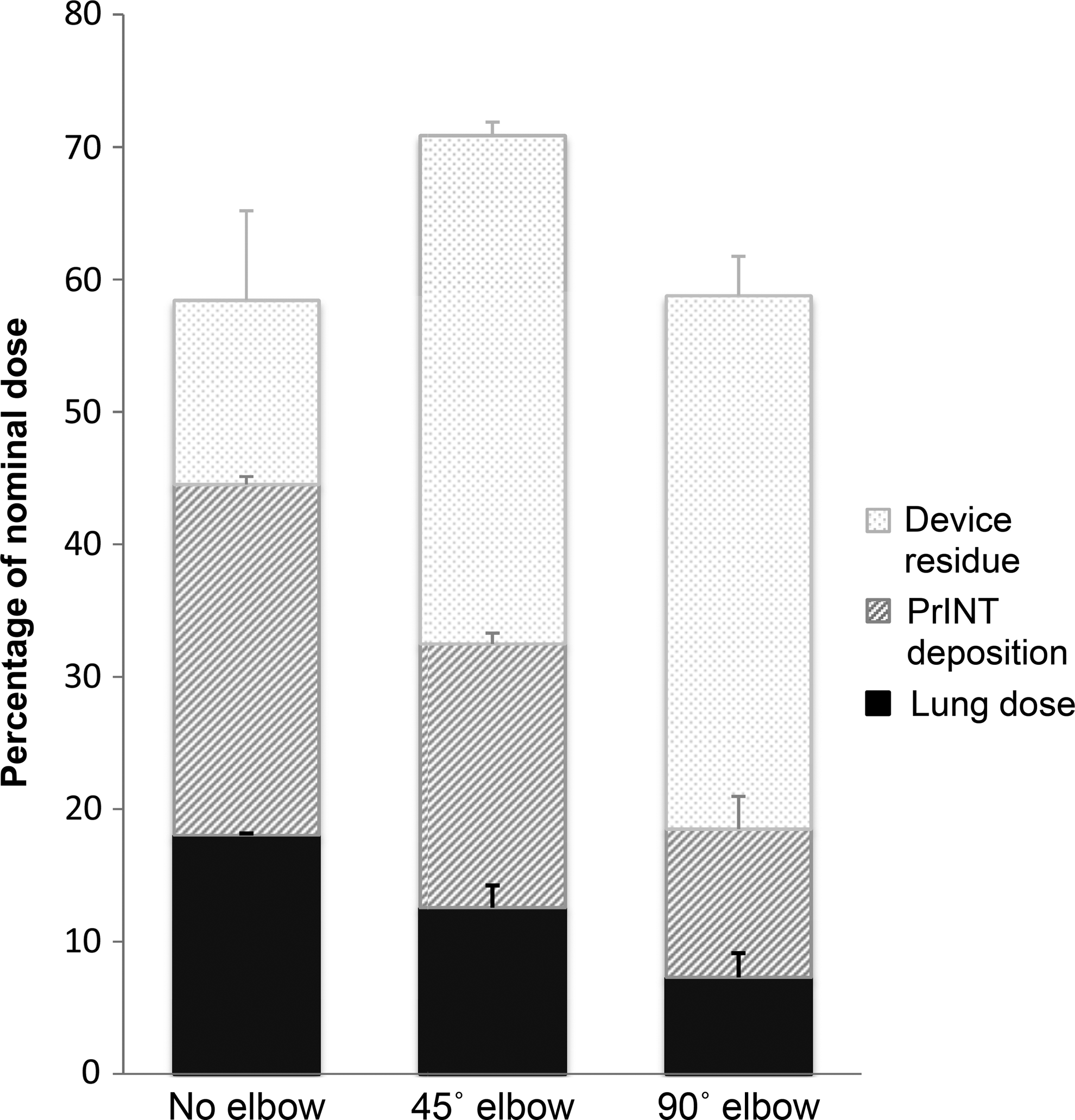
LD, DR, and PD applying two types of elbow extensions attached to the eFlowSR. DR includes residual drug in the elbow. Data represent means + SD and are expressed as a percentage of ND. The HBP was applied. All differences are significant (p<0.001), except DR for elbow 45° and 90°.
Aerosol particle size
The particle size characteristics of the aerosol exiting the infant model (i.e., entering the infant's “lungs”) are summarized for two devices in Table 2.
BP, breathing pattern; GSD, geometric standard deviation; MMAD, mass median aerodynamic diameter; TOR, total output rate.
Face deposition
Between 2.4% and 21.4% of the ED was deposited on the face (FD) of the PrINT-model (Table 1). For the jet nebulizer, the ratio between AD and FD was 1:1. For the eFlow nebulizers, FD was two to four times as much as AD.
Discussion
This study compared several aerosol delivery devices in an upper airway model of a preterm infant. All experiments were done under similar flow, pressure, and humidity settings. Two different breathing patterns were applied, and an adequate amount of dead space was simulated. We found lung deposition was considerably higher for customized vibrating membrane nebulizers (between 18.0% and 20.5% of ND), compared with a commonly used jet nebulizer and pMDI (1.5% and 6.8%, respectively). Previously published in vivo deposition studies of inhaled radiolabeled salbutamol demonstrated lung deposition in spontaneously breathing infants with bronchopulmonary dyplasia ranging from 0.12% to 2.26% for an MDI and from 0.12% to 0.66% for a jet nebulizer. 6 Cumulative urine excretion of nebulized sodium cromoglycate in ex-preterm infants' pulmonary deposition was estimated to be between 0.46% and 0.89% of ND for different nebulizers. 14 In our study, lung deposition using the pMDI and jet nebulizer was comparable, but higher, probably due to optimization of study conditions (i.e., no air leaks in the face mask, no simulation of impaired patient cooperation such as struggling and crying, stable and optimal temperature and humidity conditions).
In vitro models are useful tools in studying aerosol delivery in preterm infants.4,13 They are well correlated to in vivo performance 15 and help minimize radiolabeled aerosol deposition studies in animals and humans, which require special ethical considerations. 16 However, in vitro filter setups tend to overestimate aerosol delivery because of the absolute nature of filters, which cannot simulate possible loss of aerosol during exhalation.
Two important factors that influence aerosol delivery (besides aerosol particle size, ventilating parameters, and patient-related factors) are nebulizer efficiency and aerosol density. Dubus et al. demonstrated that higher nebulizer efficiency is due mainly to the lower residual volume of newer vibrating membrane devices. 9 We confirmed those findings in our study: lower nebulizer residue was strongly correlated with higher lung deposition. Furthermore, less drug residue and reduced ND needed are potentially cost-saving factors, especially if expensive drugs are considered. As an additional benefit, the higher efficiency of vibrating membrane devices was combined with shorter treatment times. The output rate of the investigational eFlowSR was almost double that of the jet nebulizer (238 mg/min vs. 117 mg/min). This might be beneficial particularly in infants and children, where cooperation is essential. It has been suggested that inhaled therapy should be performed during quiet sleep, 17 and the vibrating membrane devices do combine short treatment times with silent operation.
Despite the multiple advantages of the vibrating membrane nebulizers, it must be remembered that the high efficiency of these devices may lead to potential overdosing or other side effects. Currently, it remains unclear if the eight to 10 times higher aerosol deposition on the model's airway, in addition to a higher deposition on the face compared with the jet nebulizer, leads to an increased risk of dose-related adverse effects, depending on the drug being delivered. The setup used in these experiments was not able to answer these questions. For jet nebulizer use in preterm infants, we confirmed that the amount of drug inhaled depends more on its driving flow than on its tidal volume. In our setup, the HBP resulted in a minute ventilation of 790 mL/min when measured at the nostrils, and the LBP in a ventilation of 480 mL/min. The driving flow of the nebulizer was 6 L/min, so at least five-sixths of the aerosolized drug cannot be inhaled in aroused preterm infants with a higher breathing pattern. The LBP simulates quiet tidal breathing in a preterm infant, and here more than 90% of the aerosol is lost through the holes in the mask. For the jet nebulizer, we demonstrated that 70% of the initial dose is left in the reservoir, so theoretically only 3% of the initial dose is available for inhalation (i.e., only 30% exits the nebulizer, and of that only 10% can be inhaled). Smaldone et al. showed that IM (drug delivery at the mouth orifice of a face model of a 2-year-old child) using a jet nebulizer operated at 8 L/min was 50% lower than when the nebulizer was operated at 4 L/min. 12 This reflects the disproportion of minute ventilation and the amount of air in which the aerosol is dispersed (aerosol density). Once inspiratory flow is greater than the driving gas flow, the aerosol is diluted by entrained air. In preterm infants, this effect does not occur, and therefore they inhale a much larger dose in dose per kilogram than adults.18,19
Due to an entirely different operating technique, the pMDI-holding chamber is more effective than the jet nebulizer, but with its higher device (holding chamber) residue, lung deposition is lower than for the vibrating membrane devices. The latter devices operate without a driving flow, but merely create an undiluted cloud of a highly concentrated aerosol in front of the preterm infant's nose, which can be readily inhaled. For the clinical setting, where costs are an important factor, the use of vibrating membrane nebulizers has to be analyzed also by a cost-effect and side-effect analysis. We propose a detailed analysis for different specific clinical settings; in our experiment, we used salbutamol only as a drug marker, and we did not intend to perform any form of cost analysis.
In conclusion, the jet nebulizer and pMDI-holding chamber are less efficient in aerosol delivery compared with newer vibrating membrane devices in an in vitro model of a preterm infant of 32-weeks gestational age. This is due to a high driving flow in relation to the minute ventilation, a higher nebulizer residue, and the technique of a driving flow opposed to an almost standing cloud of a highly concentrated aerosol from a vibrating membrane. A possible clinical consequence of our study might be that, in using the traditional devices, higher doses are needed to get the desired effect. Also, as lung deposition may be reduced in the clinical setting, in vivo clinical studies are necessary to confirm the deposition measurements from vibrating membrane nebulizers shown in this study.
Footnotes
Acknowledgments
Dr. Tiemersma contributed to performing the tests, drafting the manuscript, and reading and approving the final manuscript. Dr. Minocchieri contributed to conceiving the study, performing the tests, coordinating the study, helping to draft the manuscript, and reading and approving the final manuscript. Dr. van Lingen contributed to conceiving the study, helping to draft the manuscript, and reading and approving the final manuscript. Dr. Nelle contributed to conceiving the study, and reading and approving the final manuscript. Dr. Devadason contributed to conceiving the study, coordinating the study, and reading and approving the final manuscript. The authors thank M. Tservistas (PARI Pharma, München, Germany) for technical advice and equipment supplies. Work was performed at Perth Medical Aerosol Research Group, School of Paediatrics and Child Health, University of Western Australia, Princess Margaret Children's Hospital, Perth, Western Australia.
Author Disclosure Statement
Dr. Tiemersma received a grant from the Science Foundation of the Isala Clinics (ZWIK) and the Paediatric and Neonatal Research Fund Zwolle. Dr. Minocchieri received a personal grant from the Swiss National Research Foundation (PBZHP3-123293). Dr. van Lingen, Dr. Nelle, and Dr. Devadason have no conflicts of interest.