
Abstract
Abstract
Background:
Open-vent jet nebulizers are frequently used to promote drug deposition in the lung, but their clinical efficacy and indications are not clear. Our study compared lung deposition of amikacin using two different configurations of a jet nebulizer (Sidestream®): one vented (N1) and one unvented with a corrugated piece of tubing (N2).
Methods:
In vitro nebulizer performance was assessed by laser diffraction and filtering. Lung delivery was evaluated by scintigraphy in baboons as a child model, and by amikacin urinary drug concentration in seven healthy spontaneously breathing volunteers. Subjects were randomly assigned to the two nebulizer systems (N1 and N2).
Results and conclusions:
In vitro results showed a higher efficiency of N2 than N1 in terms of lung deposition prediction (95±3 mg vs. 70±0 mg; p<0.0001). Radioactivity deposition in the baboons' lungs was lower with N1 than with N2 (1.8% vs. 4.7% of nebulizer charge; p<0.05). The total daily amount of amikacin urinary excretion was lower with N1 than with N2 (29.5 mg vs. 40.1 mg; p<0.01). Conversely, in vivo drug output rate was higher with N1 than with N2 (3.1 mg/min vs. 2.2 mg/min; p<0.05). Using a corrugated piece of tubing with standard jet nebulizers delivers higher doses to the lungs than open-vent jet nebulizers. The open-vent jet nebulizer might be recommended for rapid administration of a lower dose to the lungs and the standard jet nebulizer with corrugated piece of tubing for a higher dose in the lungs.
Introduction
The choice of nebulizer depends on many factors, including the amount of drug to be delivered to the lungs, the duration of nebulization, particle size distribution [mass median aerodynamic diameter (MMAD)], drug wastage, and cost.
Jet nebulizers are widely used due to their low cost, and the different types have been extensively described in the literature.(2,3) Traditional constant-output nebulizers produce constant aerosol rates throughout the respiratory cycle, with considerable wastage during expiration,(4) which decreases their efficiency.(5) They are indicated for the administration of bronchodilators, which are known to have a therapeutic threshold effect.(6) Breath-enhanced jet nebulizers increase the drug administration(4,7) by generating more aerosol during inspiration than expiration. They are therefore used when the therapeutic effect is drug amount–dependent, as in the case of antibiotics. Breath-actuated devices only deliver drugs during inspiration, which thus reduces drug wastage. They are indicated for expensive drugs and also for toxic drugs in order to avoid their dissemination in the environment. Another type of jet nebulizer, the open-vent system,(7) is frequently used. This system includes an inlet vent that draws air into the nebulizer, increasing the amount of drug aerosol produced for inhalation by the patient and the rate of nebulizer output.(8) Theoretically, this would lead to shorter nebulization time.(7) If the extra vent is blocked, a similar amount of drug would leave the nebulizer and be inhaled, but over a much longer period.(4,7) In the literature, open-vent devices are classified either as traditional constant-output nebulizers(9,10) or as breath-enhanced nebulizers.(11,12) Among the commercially available jet nebulizers, the Sidestream® vented jet nebulizer is widely used and has been extensively studied. The Sidestream jet nebulizer was originally commercialized with a mouthpiece or an adult or pediatric face mask. We have found several commercially available sets with a mouthpiece coupled with different T-piece models directly connected to the reservoir, some blocking and others allowing the extra vent. A recent study found that a modified unvented Sidestream coupled with an extension increased amikacin lung dose deposition in healthy subjects.(13) More recently, the same modified unvented Sidestream showed an increase in inhaled and pulmonary dose of amikacin compared with a Sidestream vented jet nebulizer in a spontaneously breathing tracheostomized patient model.(14)
However, there is a lack of information about the indications of these vented nebulizers compared with traditional ones. Moreover, the efficacy of the active Venturi system, driven by the patient's inspiratory flow, is debatable in patients, notably children, whose inspiratory flows are insufficient to drive it.
The aim of this study was to compare the performance of an unvented jet nebulizer combined with a corrugated piece of tubing with that of its vented version under various conditions of use. First, an in vitro measurement was performed to predict nebulizer efficiency; second, a scintigraphic deposition study measurement was performed on baboons as a pediatric patient model; and finally, an in vivo study in healthy human adults was performed to evaluate lung deposition.
Materials and Methods
Nebulizers
A well-known validated jet nebulizer (Sidestream; Philips-Respironics, Pittsburgh, PA) was used with two different configurations: connected to a T-piece (18F; Medic-Aid, Pagham, UK) allowing the extra vent (N1), and connected to a T-piece (22M; Medic-Aid) blocking the extra vent combined with a 110-mL corrugated tube connected to the expiratory (N2) (Fig. 1). A nonvalved mouthpiece connected to the T-piece was used as the interface for in vitro and human studies and a nonvalved face mask connected to the T-piece was used as the interface for the animal study. Nebulizers were operated with a compressor (Porta-Neb®, driving gas flow 7 L/min; Medic-Aid).

The two jet nebulizer systems (Sidestream): one with a T-piece allowing the extra vent (N1), and one with a T-piece blocking the extra vent and a 110-mL corrugated tube connected to the expiratory side (N2). Grey arrows, aerosol; black arrows, additional air; white arrow, air compressor.
In vitro measurement
Particle size distribution was measured by laser diffraction (Mastersizer-X; Malvern Instruments Ltd., Malvern, Worcestershire, UK) following the protocol described by Majoral and colleagues.(15) MMAD and respirable fraction (RF%), defined as the fraction of particles between 1 μm and 5 μm, were carried out using Mastersizer-X software.
The inhaled mass was assessed by the residual gravimetric method(16) using a lung model (5600i Dual Adult Training/Test Lung; Michigan Instrument Inc., Grand Rapids, MI). Nebulizers were filled with 4 mL of 125 mg/mL amikacin solution. The solution was nebulized until 1 min after the appearance of the sputtering point for the two Sidestream configurations. A filter was interposed between the lung model and the nebulizer to calculate the inhaled mass. A second filter was placed at the distal end of the T-piece for N1 and the corrugated tube for N2 to measure the aerosol lost at the expiratory way as far as possible. The settings of the lung model were as follows: frequency, 15/min; tidal volume, 600 mL; inspiratory pause, 10%; and inspiration/expiration ratio, 33%. The residual volume was defined as the volume of the solution trapped in the reservoir at the end of the nebulization. It was calculated by subtracting the weight of the dry nebulizer from the weight of the nebulizer with the residual solution at the end of the nebulization corrected by the liquid density. The respirable mass was defined as the mass of drug available for the lungs and was estimated by multiplying the inhaled mass by the respirable fraction. Inhaled and respirable mass were expressed as percentage of the nominal mass of amikacin. The rate of respirable mass was expressed as the respirable mass divided by the duration of the nebulization. Expiratory leakage was defined as the mass of drug lost during the expiratory phase and deposited on the expiratory filter.
In vivo scintigraphy deposition study in baboons
After approval of the local Ethics Committee of the University of Tours, three healthy baboons weighing 9 to 12 kg were installed on a special chair under anesthesia administered via an intramuscular injection of xylazine (1 mg/kg) and ketamine (5 mg/kg). The baboon breathing parameters were determined using a pneumotach (Dyn'R, Muret, France) without the nebulizer system. Tidal volume, breathing rate, and inspiratory/expiratory ratio were measured at 54±9 mL, 35±7 breaths/min, and 0.69±0.09, respectively. They were then kept awake while aerosol was administered through a face mask. Each baboon inhaled an aerosol produced by the two different nebulizer systems described above (N1 and N2). The solution was nebulized until 1 min after the appearance of the sputtering point for the two Sidestream configurations. The order of nebulization was randomized for each baboon, resulting in 12 inhalations. 99mTc-DTPA (Pentacis®; CIS Bio International, Gif-sur-Yvette, France) was used to label the amikacin (500 mg) solution resulting in 74 MBq/4 mL. Immediately after aerosol delivery, the animals and the circuit components were scanned using a gamma camera (e.cam; Siemens, Munich, Germany). The amount of 99mTc-DTPA deposited in the lungs was determined from the digitized images, taking into account attenuation coefficients derived from lung perfusion imaging of each baboon using pertechnetate-macroaggregated albumin. The total lung surface was determined from the pertechnetate-macroaggregated albumin scan. The amount deposited in the extrathoracic region (stomach+mouth) was calculated by applying the attenuation coefficient. The amount of radioactivity remaining in the nebulizer was determined using static acquisition imaging without attenuation coefficient. Aerosol leakage was calculated by the difference between the nebulizer charge and the residual activity and the deposited activity in the baboon. Corrections for the physical decay of 99mTc were made on all measurements.
Kinetic study in human adults
After approval by our Institutional Ethics Committee (Commission d'Ethique Biomédicale Hospitalo-Facultaire, Université Catholique de Louvain; 2008/16MAI/139), we recruited seven nonsmoking healthy male volunteers (mean age=24.3±4.6 years) who gave their written informed consent. Each volunteer performed a spirometry test following ATS/ERS guidelines,(17) and data were expressed as a percentage of predicted value (Table 1).(18) The subjects did not receive any aminoglycoside during the month prior to the experiments. All subjects declared that they were not allergic to aminoglycosides.
FVC, forced vital capacity; FEV1, forced expiratory volume in 1 sec; % pred, percentage of the predicted value.
Results are expressed as means±SD.
Subjects were randomly assigned to the two nebulizer systems (N1 and N2) in a two-way crossover design. A washout period of 48 hr was observed between each nebulization. Participants were requested to empty their bladder before nebulization. They inhaled the aerosol under spontaneous breathing in a sitting position, wearing a noseclip. During nebulization, tidal volume (Vt; mL), respiratory rate (RR; min–1) and minute ventilation (VE; mL min–1) were continuously monitored by inductance plethysmography (Medical Electronic Construction, MEC, Brussels, Belgium). The Spirometer was calibrated before each measurement using a 3 L±0.4% calibration pump (CareFusion, Höchberg, Germany) connected to the flow sensor. Inductive plethysmograph was calibrated following the method of Konno and Mead.(19) The solution was nebulized until 1 min after the appearance of the sputtering point for the two Sidestream configurations.
Urine was collected immediately before and for 24 hr following nebulization. Micturition time and volume were recorded. Urine aliquots were stored at 4°C until further analysis. Urinary amikacin concentration was assessed by fluorescent polarization immunoassay (Abbott Laboratories, Abbott Park, IL). The total amount of amikacin excreted in the urine after nebulization (Cu max) reflecting lung deposition was calculated using JMP software (SAS Institute, Cary, NC) using the Michaelis-Menten kinetic model.(20) The Cu max was expressed in percentage of the nominal mass of amikacin.
After complete nebulization, the residual concentration of amikacin was measured in the reservoir.
Statistical analysis
Results are presented as means±SD, and the coefficient of variation (SD/mean×100) was used to express data variability. For in vitro data, a Student's t test was used with 0.05 as a threshold p value. For in vivo data of baboons and human adults, the significance of the differences between devices was assessed using a paired t test.
Results
Prediction of deposition
The unvented jet nebulizer increased the inhaled (29.8±1% vs. 17.6±0.2% of the nominal mass of amikacin; p<0.0001) and respirable (19±0.6% vs. 14±0% of the nominal mass of amikacin; p<0.0001) fraction of the nominal mass of amikacin compared with the vented device (Fig. 2A and B) and decreased aerosol leakage (21.2±0.8% vs. 38.4±0.4% of the nominal mass of amikacin; p<0.0001) (Fig. 2C). The duration of nebulization (15±0 min vs. 9±0 min) and the MMAD (3.8±0.1 μm vs. 3.3±0.4 μm) were significantly higher (p<0.001) with the unvented device. The rate of respirable mass was higher with the vented device (7±0 mg/min vs. 6±0 mg/min; p<0.001) (Fig. 2D). The residual volume was not significantly different between the two nebulizers (28.8±1.3% vs. 31.7±1.8% of the nominal solution for N1 and N2, respectively).

Comparison of in vitro data obtained during nebulization with open-vent (N1) and standard (N2) jet nebulizers (Sidestream). Results are expressed as means±SD. ***p<0.001; ****p<0.0001.
Deposition study in baboons
There was higher pulmonary activity (4.6±3.1% vs. 1.0±0.4 %; p=0.026) and drug output rate (0.27±0.20%/min vs. 0.12±0.06%/min; p=0.056) with the standard nebulizer than with the open-vent jet nebulizer (Fig. 3). The nebulizer residual activity showed no statistical difference between nebulizers (52±9% vs. 58±4% for N1 and N2, respectively; p=0.17), but there was significantly higher aerosol leakage with the vented nebulizer (45.6±9.6% vs. 33.6±4.2%; p=0.015). Duration of nebulization was reduced by a factor of 2 using the vented nebulizer (9±2 min vs. 20±5 min; p=0.001).
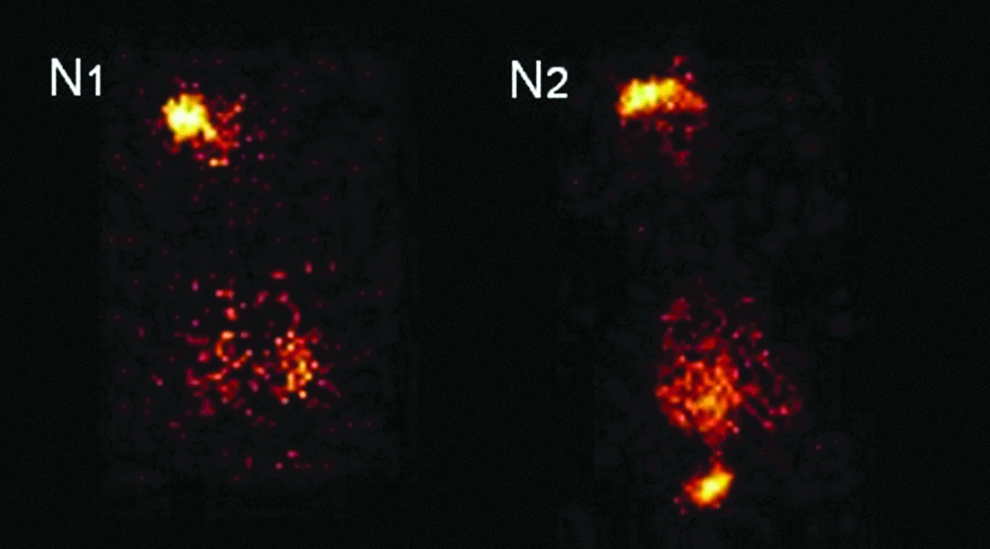
Scintigraphy images obtained with baboons inhaling amikacin aerosol nebulized with open-vent (N1) and standard (N2) jet nebulizers (Sidestream).
Kinetic study in human adults
Tidal volume, minute ventilation, and respiratory rate were similar for the two devices (Table 2; p>0.08). There was no difference in the residual concentration of amikacin (in the reservoir) between the two nebulizers (205.9±15.2 mg/mL vs. 211.0±15.3 mg/mL for N1 and N2, respectively; p=0.61).
Vt, tidal volume; RR, respiratory rate; VE, minute ventilation.
Results are expressed as means±SD, with the coefficient of variation in parentheses.
The total daily amount of urinary amikacin excretion (Cu max) was significantly higher with the unvented nebulizer (8.0±1.4% vs. 5.9±1.8% of the nominal mass of amikacin; p<0.02) (Fig. 4A). Again, duration of nebulization was shorter with the vented than unvented nebulizer (9.5±0.7 min vs. 18.1±1.4 min). Drug output rate was significantly higher with the vented nebulizer (3.1±1 mg/min vs. 2.2±0.4 mg/min) (Fig. 4B). The half-life and elimination constant (Ke) were similar for the two devices (p=0.64 and p=0.37, respectively).

Descriptive plot of pharmacological data obtained after nebulization with open-vent (N 1) and standard (N 2) jet nebulizers (Sidestream). Results are plotted for each subject; horizontal lines represent mean values. Cu max, total daily amount of urinary amikacin excretion. *p<0.05.
Discussion
Our study showed higher predicted lung deposition with the traditional unvented jet nebulizer than with an open-vent system on bench testing, in a model of children and in healthy adults. The difference in deposition was greatest in the animal model.
Our results confirm that nebulization time is shorter with the vented than with the unvented jet nebulizer.(4) They also confirm that the vented system significantly affects the particle size distribution of the aerosol.(4) As previously shown for drug output rate in a comparison of breath-enhanced and unvented jet nebulizers,(4) our results showed a significant increase in lung drug output rate with the vented jet nebulizer for healthy adults. In contrast to studies showing that the amount of drug delivered is higher with a breath-enhanced than with an unvented jet nebulizer,(4,10) the present study found an increase of 37% in urinary drug excretion with the unvented Sidestream (8.0% of the nominal dose) compared with the vented Sidestream (5.9% of the nominal dose). This increase can be explained by various factors, including the increase in inhaled dose with the unvented nebulizer and the increase in aerosol leakage with the vented one observed in our in vitro results. The vented nebulizer functions like the breath-enhanced jet nebulizer during the inhalation phase, but it does not reduce aerosol production during the exhalation phase, resulting in greater aerosol leakage. Open-vent nebulizers do not work as well as breath-enhanced jet nebulizers. Furthermore, the corrugated tube used with the unvented jet nebulizer could also increase the difference in terms of aerosol leakage between the vented and unvented devices.(13)
The baboons were chosen for scintigraphic study as a model of pediatric patients (9–12 kg). Despite substantial differences between the airways of primates and humans,(21) the primate is considered to be a relevant model for predicting deposition in the human lung. The morphology of our baboons corresponded to normal-weight infants between 9 and 24 months. There was a marked decrease in pulmonary drug deposition (77%) in the baboons with the open-vent jet nebulizer compared with deposition with the standard jet nebulizer coupled with a corrugated piece of tubing (1.2% vs. 4.6% of the nebulizer charge for the open vent and the standard jet nebulizer, respectively). Furthermore, we observed a highly significant reduction in lung deposition (80%) between the healthy adult population and the child model with the same open-vent Sidestream device (1.0% vs. 5.4% of the nominal dose for the baboons and the adults, respectively). A smaller decrease (35%) was observed with the standard jet nebulizer (4.6% of the nebulizer charge vs. 7.3% of the nominal dose for the baboons and the human adults, respectively). The decreases observed with the open-vent jet nebulizer could be partly explained by the low inspiratory flow of the baboons, reducing the nebulizer drug output, as it has been showed that the drug output is inspiratory flow–dependent with the open-vent jet nebulizer.(22) Furthermore, the use of the corrugated tube with the standard jet nebulizer probably helped reduce expiratory drug wastage,(13,14) thus explaining the increase of drug deposition with the standard jet nebulizer. Some anatomical and physiological factors could also help explain the striking decrease observed in the baboons compared with the healthy adults. The differences between airway geometry between infants and adults could explain the fact that, for the same MMAD, the respirable fraction of an adult is greater than that of an infant, and that the deposition in upper airways is greater in infants than in adults.(23) The main difference between our baboon model and the normal circumstances of nebulization in infants is that our baboons had normal airways and lungs. As deposition may differ between a healthy animal model and infants with pulmonary diseases, further clinical studies are required with infants.
Preliminary to the kinetic study in the human adult, data were collected to evaluate the “CO2 rebreathing” with the use of the 110-mL corrugated piece of tubing. Theorically, with a gas flow of 7 L/min through the nebulizer, all the expired CO2 is cleared from the dead space. However, we verified this in a preliminary setting where one healthy subject was breathing through the different Sidestream configurations (with and without the 110-mL corrugated piece of tubing) while the partial pressure of CO2 was recorded using a Sidestream capnograph. The inspired pressure of CO2 remained undetectable or close to 1 mmHg.
The study in humans was conducted with healthy subjects. This may lead to a more even aerosol distribution than in patients with lung disease, and makes it easier to compare devices. As considerable differences in lung properties and breathing pattern can be observed in pathological conditions, further investigations in relation to specific disease groups are required.
This study demonstrates that the two Sidestream devices had particular strengths and weaknesses in a sample of healthy adults. In terms of rapid drug delivery, a factor that could shorten treatment duration and improve patients' adherence to therapy,(24) the open-vent Sidestream appears to be superior to the unvented system with a piece of corrugated tubing. The rate of output is greater with the open-vent than with the unvented jet nebulizer. In terms of maximizing drug delivery—an important factor if the drug is very expensive or if the patient needs to receive a high dose—the unvented jet nebulizer with a piece of corrugated tubing allows greater lung deposition. Observations are slightly different with the primate model, which showed a higher rate of output and lung deposition with the unvented jet nebulizer. Our data also confirm our primary hypothesis that the inspiratory flow in infants is insufficient to drive the Venturi system.
Our study has a number of limitations. First, in the bench study, we studied only one adult breathing pattern. Second, we studied only one drug and two configurations of the same nebulizer. Finally, we did not study patients and did not look at the clinical outcomes. Future studies should address the clinical outcomes on patients and the role of other variables, such as new-generation nebulizers, other drugs, and other breathing patterns. However, we believe that our work provides relevant information running against some current teaching about these devices. From this study, we can conclude that standard jet nebulizers with a piece of corrugated tubing may be preferred when administering higher doses in the lungs (e.g., for antibiotics) and open-vent jet nebulizers might be recommended for drugs that need to be administered to the lungs rapidly but in lower doses (e.g., bronchodilatators).
Footnotes
Acknowledgments
This work was supported by the Belgian Fonds National de la Recherche Scientifique (grant no. 3.4529.10). The authors thank Mrs. Stéphanie Asta for dosing urinary amikacin.
Author Disclosure Statement
L. Pitance, G. Reychler, T. Leal, G. Liistro, H. Reychler, J. Montharu, and P. Diot have no conflicts of interest to declare. L. Vecellio is employed by la Diffusion Technique Française.