
Abstract
Abstract
Background:
Placing a surgical mask on an infected patient (respiratory source control) may offer a health-care worker (HCW) more protection than donning an N95 respirator (receiver protection). This observation was made in an in vitro study that used hard, nondeformable faces, and the lack of proper N95 fit may have accounted for the observed results. In the present study, we test the effects of fit on respiratory source control protection, using a soft, deformable mannequin head.
Methods:
Resusci Anne CPR mannequin heads were placed in a chamber allowing 6 air exchanges/hr (14 cubic feet per minute), to simulate an infected patient (source) and an HCW (receiver). The heads were ventilated with a tidal breathing pattern. The source exhaled radioactive aerosols, and a filter was attached to the receiver to quantify inhaled exposure. N95 respirators and surgical masks were tested on both heads. The degree of protection was expressed by calculating the reduction in exposure expressed as a simulated workplace protection factor (sWPF; the ratio of exposure with mask to exposure without mask) compared statistically using confidence intervals.
Results:
Use of the Resusci Anne heads resulted in improved fit, with higher sWPF than previously reported, for example, for source N95 mask combinations (7,174 vs. 317) as well as receiver (7.53 vs. 1.37). Masks placed on the receiver provided minimal exposure protection (sWPF range 0.99–7.53), except when sealed with Vaseline (sWPF 63.1). Any mask applied to the source mannequin resulted in significant reductions in exposure (sWPF range 214–17,038).
Conclusion:
Improved fit significantly enhanced the effects of source control protection. A Vaseline-sealed N95 respirator on the receiver offered less protection when compared with any mask on the source. Respiratory source control can offer more protection to HCW and potentially decrease the spread of aerosolized infections.
Introduction

Model of source/receiver/environment interaction. Parameters that can be set or measured are shown. Dilution is an effect of the environment on the concentration of produced aerosols. Filtration is a function of mask used and occurs at both the receiver and source. Particles not filtered were deflected by the mask at the source and carried away from the receiver by the environmental flow (6 air exchanges/hr(4)). Breathing pattern was set to simulate adults with tidal breathing.
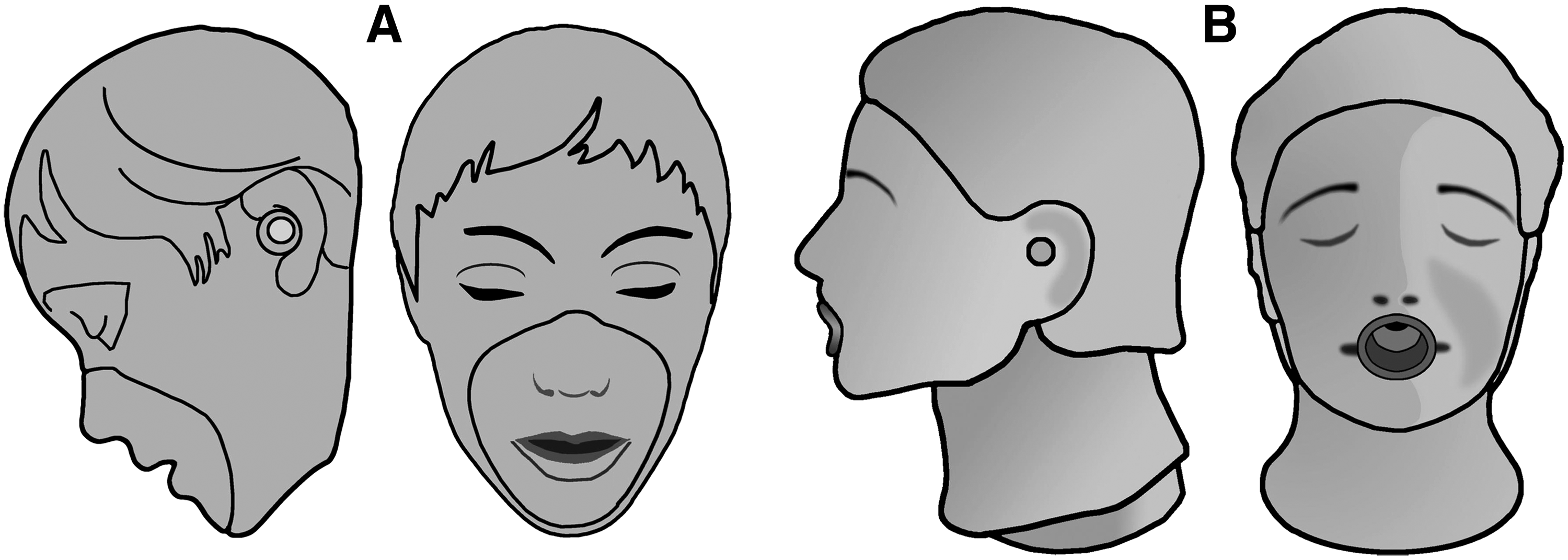
An important concern that arose in the study by Diaz and Smaldone was the face–mask interface. Their mannequin heads were made of a nondeformable, hard plastic and were smaller than the head of a “typical adult” (Fig. 2A; “BRAD” CPR adult mannequin head). Because the effectiveness of the N95 respirator is known to be heavily dependent on fit,(2,3) it is possible that the results were largely a function of the poor fit of the respirators on those particular heads. The current study was designed to examine the role of “mask fit” on the reproducibility of the source control data. We used Resusci Anne CPR mannequin heads (Fig. 2B), which are realistically sized (based on a mold of a real female face), with soft, deformable “skin-textured” faces, to better define the role of fit of the N95 mask in this model, and thus test the validity of the findings of Diaz and Smaldone.(1)
Materials and Methods
A chamber (Fig. 3), connected to a hood through a fixed opening providing 6 air exchanges/hr(4) and measuring 5.2 ft in length×4.9 ft in width×6.2 ft in height, was made to replicate the original enclosure used by Diaz and Smaldone.(1) Two Resusci Anne CPR mannequin heads (no. 310200; Laerdal Medical, Wappingers Falls, NY) were placed in the enclosure, 3 ft apart. Both heads were fitted with standard respiratory tubing measuring 70 mL in volume, connected to the inside orifice of the mouth coupling, and coursed inside the head and out the bottom of the neck to create an airtight connection. Each head was ventilated by a Harvard pump (Harvard Apparatus SN no. A52587; Millis, MA) simulating a tidal breathing pattern (volume of 500 mL, respiratory rate of 15 breaths/min, and duty cycle of 0.5 sec). The source head (mimicking the infected patient) was connected to an AeroTech II nebulizer (three devices used in rotation; Biodex, Shirley, NY) powered by an air tank with a flow of 10 L/min. The nebulizer was filled with 3 mL of 0.9% normal saline labeled with technetium-99m and run to dryness over 10 min, producing radioactive wet aerosols simulating contaminated particles exhaled during tidal breathing. A cylindrical plastic ring was placed in the mouth of the source head to prop the lips open, allowing the aerosols to be exhaled exclusively from the mouth. No modifications were made to the receiver head, which was ventilated through the nose and mouth. To quantify exposure, a filter (model no. 041B0522; PARI, Starnberg, Germany) was attached to end of the airtight connection on the receiver head to capture all inhaled particles.
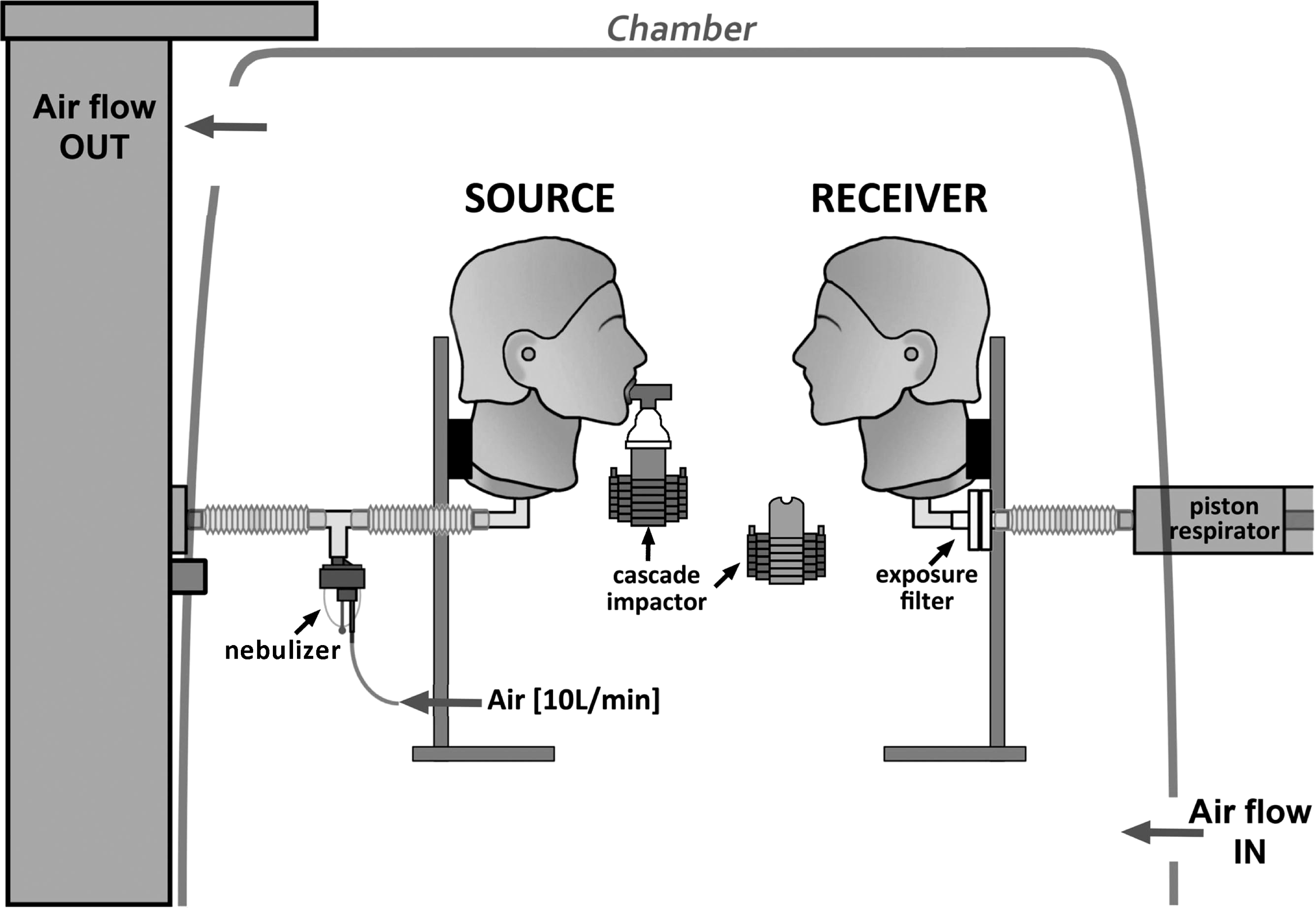
Setup illustrating ventilated mannequin heads 3 feet apart. Source head was connected to an AeroTech II nebulizer and exhaled radioactive aerosols. A filter was attached to the receiver head to capture and quantify inhaled radioactive aerosols. In a separate series of experiments, cascade impactors were used to measure size distribution of expired aerosols at the source and inhaled at the receiver.
In a separate series of experiments (also illustrated in Fig. 3), the aerodynamic distributions of aerosolized particles at the source and near the receiver were measured in triplicate by cascade impaction (Marple 8-stage impactor; Thermo Fischer Scientific, Waltham, MA; 2 L/min flow). The source cascade impactor sampled source aerosols as they were nebulized, whereas the receiver cascade impactor sampled the aerosols that reached the vicinity of the mouth of the receiver.
A NIOSH-approved N95 respirator (model no. 1860S size small; 3M, St. Paul, MN) and an ear loop surgical mask (model no. GCFCXS; Crosstex International Inc., Hauppauge, NY) were used to assess several mask combinations on the source and receiver mannequin heads. Combinations included the following: no mask on either head [maximum exposure (Max Ex)], a surgical mask tightly fit on the source (S-TSM), a surgical mask looped “naturally” around the ears of the source (S-SMnat), an N95 on the source (S-N95), a surgical mask tightly fit on the receiver (R-TSM), a surgical mask looped around the ears of the receiver (R-SMnat), and an N95 on the receiver (R-N95). N95 masks were visually sized to fit the mannequin. To further test fit, additional experiments were performed with the N95 sealed to the face with a bead of Vaseline (soap bubble–tested; S-N95vas, R-N95vas) to evaluate for leaks. We modeled the chamber to mimic a negative-pressure hospital room where air entered the chamber at the entrance and moved in one direction to the exhaust located behind the patient. Smoke tracer experiments were performed within the chamber to visually define ambient air currents. Chamber flow toward the hood was measured using a Balometer (model no. 6200D; Alnor, Huntington Beach, CA) and reported as cubic feet per minute (CFM). The hood extraction was set at 14 CFM and was equivalent to 6 air exchanges/hr for the chamber, to recreate the conditions in the Diaz and Smaldone study.(1) Relative humidity and temperature ranged from 23% to 68% and 20.5°C to 23.2°C, respectively. The mannequin heads were set 3 ft apart to mimic two individuals sitting in a room. A tidal breathing pattern was chosen to represent the most common clinical interaction between two people. The nebulizer chosen created wet aerosols with a representative size distribution of that exhaled by humans during tidal breathing.(5,6)
The first series of experiments were performed without masks on either head to measure Max Ex, which represented the percentage of nebulized particles that traversed the chamber from the source to the receiver and were inhaled after being diluted by mixing with the ambient air inside the chamber. The next series of experiments involved placing N95 and surgical masks on the source. The surgical mask was studied in two configurations, either pulled tightly (stretched) against the face, or looped around the ears in a “natural” configuration, to measure the relative reduction in exposure compared with Max Ex. As outlined in the study by Diaz and Smaldone,(1) these configurations assessed the combined effects of filtration (particles captured by the mask) and deflection (particles not filtered by mask and redirected away from the receiver). The tight surgical mask was previously characterized as being a better deflector.(1) The same mask configurations were also tested on the receiver mannequin head. The latter setup assessed mask filtration on the receiver combined with effects of fit (particles leaking around the masks and inhaled by the receiver). The last set of experiments consisted of sealing the N95 on the source head with a bead of Vaseline around the perimeter of the respirator to enhance fit and eliminate any visible leaks. In these experiments, filtration was the only mechanism of protection.
Aerosol exposure was quantified by measuring radioactivity captured by the receiver filter expressed as a percentage of nebulized activity. Nebulized activity represented the difference between initial nebulizer charge and that remaining after nebulization. Data were corrected for tube losses in the mannequin head by applying a correction factor signifying the part of the nebulized activity that was deposited in the tubing and was therefore not available to the receiver. This factor was defined in a separate experiment in which the activity lost in the tubing within the head (between the nebulizer and the mouth) was measured using a gamma camera interfaced to a computer (Maxi Camera 400, General Electric, Horsholm, Denmark; Power Computing, Model 604/150/D, Austin, TX; NucLear MAC, Version 4.2.2, Scientific Imaging, Inc., Crested Butte, CO). Losses approximated 15.69% of nebulized charge. For each nebulization, the activity nebulized multiplied by (1-0.1569) defined the actual aerosol exhaled by the source for each experiment. Radioactivity captured on filters, masks, or in the cascade impactor was quantified in a calibrated well counter (10 μCi to 10 mCi; Kemble Instruments, Hamden, CT) or a calibrated rate meter (<10 μCi; Ludlum Measurements Inc., Sweetwater, TX).
Statistics
Exposure data and mask filtration were expressed as percentage of nebulized particles [mean±95% confidence intervals (CI)]. Separation of CI defined statistical significance. To compare different effects, exposure and mask filtration were depicted graphically on scatter plots. To allow direct comparison with the original experiments by Diaz and Smaldone,(1) exposure data were expressed as a simulated workplace protection factor (sWPF) defined as the ratio of Max Ex to actual exposure.(7)
Results
Particle distributions and mass median aerodynamic diameters (MMAD) are summarized in Figure 4. Data are plotted as log aerodynamic diameter versus probability with CI. At the source, approximately 90% of the particles were less than 2 μm, with an average MMAD of 0.95 μm (95% CI:±0.119). The MMAD of particles reaching the vicinity of the receiver was 0.69 μm (95% CI:±0.0663).
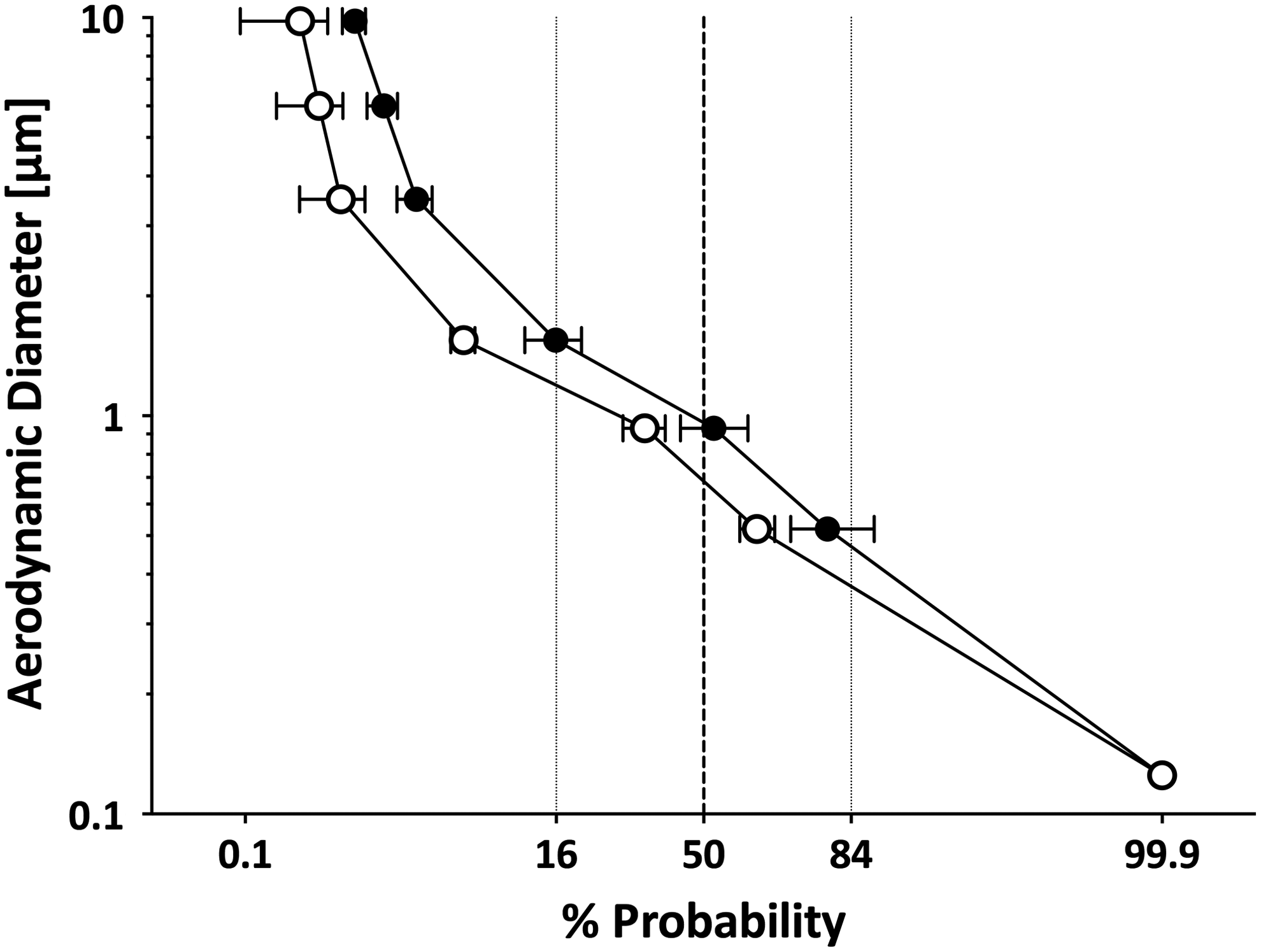
Distribution of radioactivity for all stages of the cascade impactor using the AeroTech II nebulizer, plotted as log particle size versus probability [confidence intervals shown (MMAD±95% CI; n=3)]. Source (closed circles) MMAD=0.95 μm; Receiver (open circles) MMAD=0.69 μm.
Max Ex and exposure data are shown in Figure 5, with the corresponding sWPF for each mask configuration listed in Table 1. Data are separated by the process described in Materials and Methods above, and reported as percentage of nebulized particles. The protective effect of each intervention in reducing exposure is best illustrated by the magnitude of the sWPF.
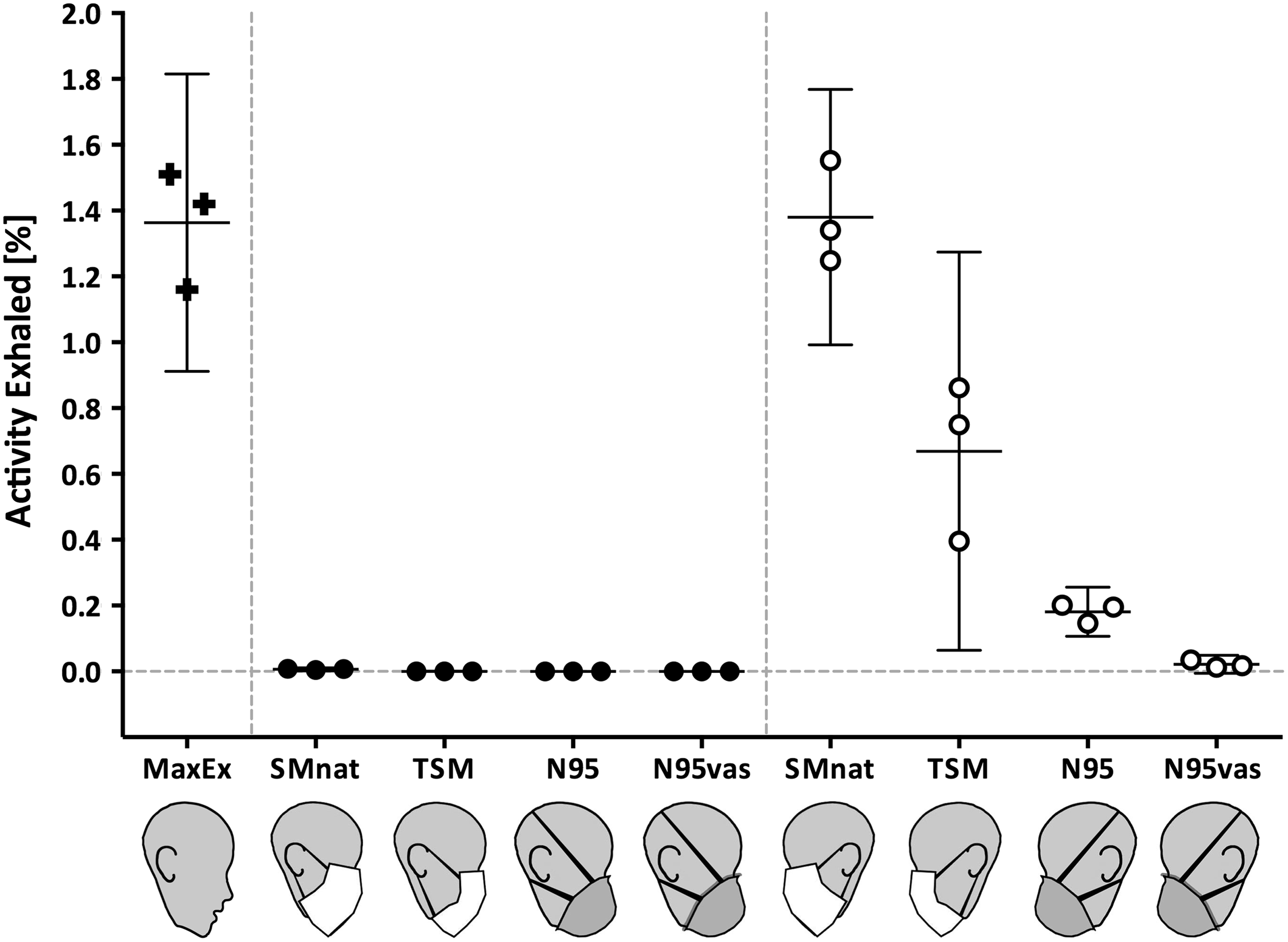
Inhaled mass exposure data, expressed as percentage of nebulized charge±95% CI. Source, heads facing right (closed circles); Receiver, heads facing left (open circles). Placing any mask on Resusci Anne head significantly reduces Receiver exposure. On the Receiver, only Vaseline-sealed N95 respirator provides protection approaching source control.









N, all experiments repeated in replicate; TSM, tightly fit surgical mask; SMnat, surgical mask natural fit; N95vas, N95 sealed to face with Vaseline; CI, confidence intervals; sWPF, simulated workplace protection factor, the ratio of exposure without a mask to exposure with a mask; N/A, not applicable.
Exposure is expressed as a percentage of nebulized particles inhaled by the receiver. Mask filtration is expressed as a percentage of nebulized particles captured by the mask.
Normalized for exposure reaching receiver.
Max Ex averaged 1.363% (95% CI: 0.912–1.81%) of the total activity exhaled, and represents the amount of aerosol inhaled by the receiver as a function of dilution. This was assigned an sWPF of 1, signifying no protection. Applying a surgical mask or N95 respirator to the source resulted in significant reductions in exposure to 0.00637% (95% CI: 0.00163–0.01110%), corresponding to an sWPF of 214 for the S-SMnat, 0.00023% (95% CI: 0.00009–0.00038%) or an sWPF of 5,850 for the S-TSM, and 0.00019% (95% CI: 0.00012–0.00027%) or an sWPF of 7,174 for the S-N95. Conversely, only minimal, insignificant reductions in exposure were measured when a surgical mask or unsealed respirator was placed on the receiver [exposures ranging from 1.38% (95% CI: 0.992–1.77%), sWPF of 0.99 for the R-SMnat, to 0.669% (CI: 0.0641–1.27%), sWPF of 2.04 for the R-TSM, and 0.181% (95% CI: 0.106–0.256) corresponding to an sWPF of 7.53 for the R-N95].
The sealed N95 respirator experiments illustrate the effects of so-called perfect fit (no leaks around the mask). On the source, the S-N95vas provided the highest sWPF, three times greater than the S-N95 without Vaseline (sWPF of 17,038 vs. 7,174, respectively). The only mask on the receiver to provide significant protection was the sealed R-N95vas with sWPF 63.1.
Radioactivity captured by each mask quantified the effectiveness of filtration (Fig. 6). Mask filtration was reported as a percentage of activity exhaled at the source. At the receiver, filtration was expressed as a percentage of Max Ex, that is, normalized for the reduction in aerosols reaching the receiver as a result of environmental dilution. At the source, the N95 filtration averaged 77.06% (95% CI: 73.25–80.88%) in comparison with 37.03% (95% CI: 5.096–68.96%) for the S-TSM and 13.18% (95% CI: 7.476–18.89%) for the S-SMnat. Filtration at the receiver captured an average of 92.28% (95% CI: 37.62–146.9%) for the N95, 48.83% (95% CI: 32.1–65.55%) for the TSM, and 32.68% (95% CI: 22.36–43.01%) for the SMnat. Although, the sealed S-N95vas respirator filtration was similar to the unsealed S-N95 [75.42% (95% CI: 56.86–93.98%)], the sWPF differed significantly. Likewise, the R-N95vas filtered about the same amount of particles as the unsealed R-N95 [91.41% (95% CI: 2.273–180.5%) vs. 92.28% (95% CI: 37.62–146.9%)], but with marked differences in sWPF [the sWPF measurements depend on activity captured on the exposure filter (Fig. 2) and include effects of deflection].
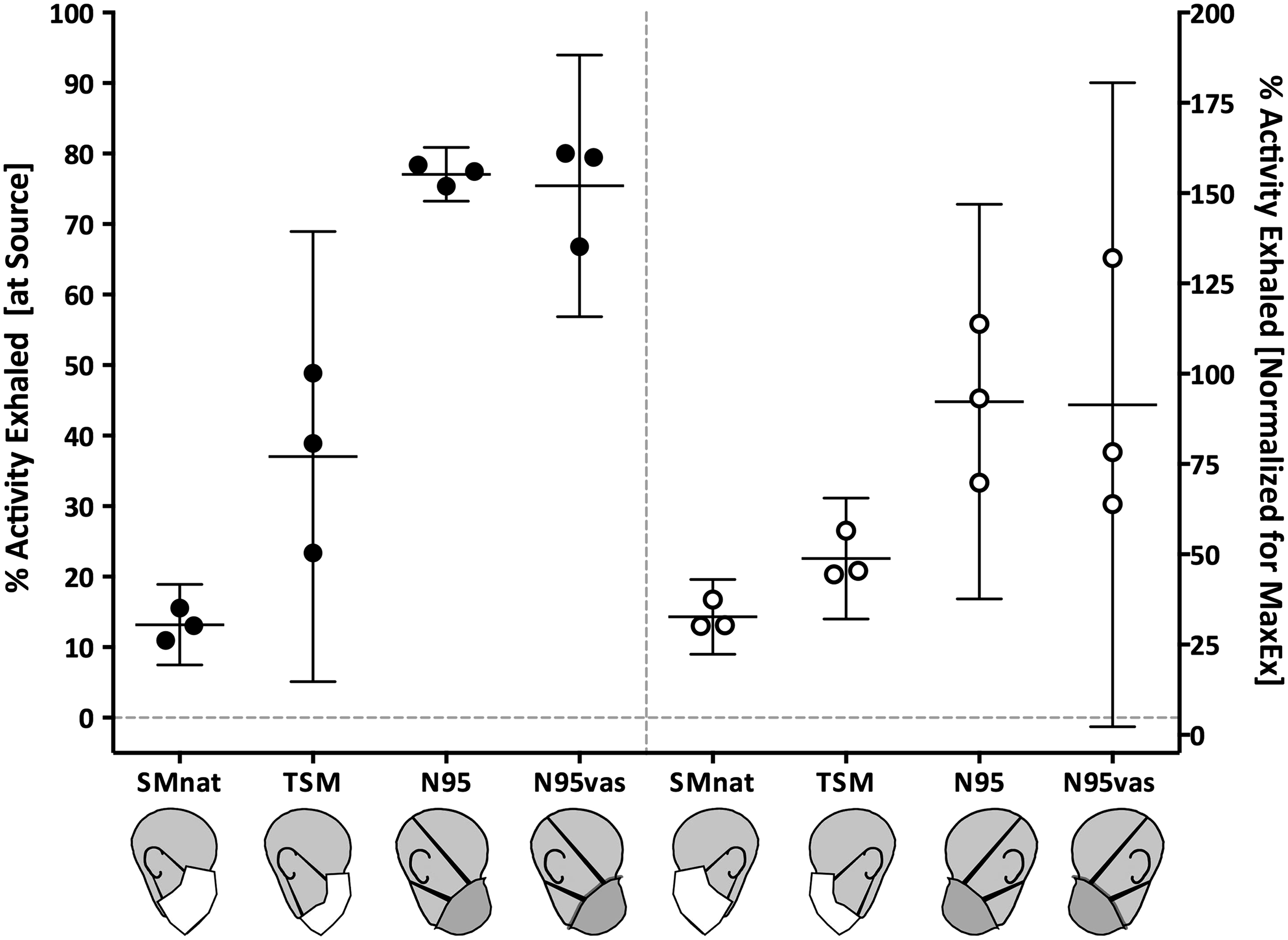
Deposition on mask expressed as a percentage of nebulized charge±95% CI, for the Source [heads facing right (closed circles)]. Receiver mask deposition [heads facing left (open circles)] was normalized for Max Ex, or concentration of aerosols reaching receiver. N95 was superior to surgical mask on both source and receiver.
Discussion
Using the new mannequin heads, we were able to demonstrate that source control protection is in fact a reproducible phenomenon enhanced by better fit of the masks on the face. The results from the present study support the findings of Diaz and Smaldone.(1) Their in vitro study demonstrated that a simple, cheap surgical mask placed on the infected source may be more effective in decreasing exposure than a more expensive N95 respirator sealed to the face of the receiver. Our study confirms their observations using new heads with skin-textured faces. The Resusci Anne CPR mannequin heads allow for a better seal between the N95 and the contours of the face, resulting in comparatively better fit as evidenced by higher sWPF values. For example, Diaz and Smaldone reported an sWPF of 1.37 for the N95 on the receiver (without a Vaseline seal); for the same configuration, we measured an sWPF of 7.5, demonstrating better fit. Because of this, the protection provided by the N95 on the receiver in our study was statistically higher than that provided by the surgical mask on the receiver (Fig. 5). However, rather than favoring use of masks as better filters on the receiver, our results indicate that better fit improves protection via the mask on the source. Protection with better fit on the receiver was significantly increased, but these changes were minimal when compared with the effects of source control. In general, our sWPF for masks placed on the source are much higher than those reported by Diaz and Smaldone.(1) That is because the better fit in our study improved filtration at the source. The significantly greater sWPF measured in our study for the S-TSM and S-N95 are likely due in part to the improved fit, leading to greater filtration at the source. For those two masks, filtration was significantly higher in our study when compared with the original Diaz and Smaldone study (37.03% and 77.06% vs. 14.8% and 35.7%, respectively), especially when considering that the filtration on the S-N95 without Vaseline is equal to the filtration of the Vaseline-sealed N95 on the source (77.06% vs. 75.42%). This observation represents the strongest evidence that the new heads used in our study provided an effective seal with the N95 masks. Despite the similar filtration rates between the Vaseline-sealed N95 and the unsealed N95 masks on the source, the N95vas had a much higher sWPF. This pattern was also observed in the Diaz and Smaldone study. However, in that study, the filtration of the sealed N95 was much higher than that of the unsealed N95 (81% vs. 35.7%), indicating that in fact the N95 did not fit as well on the “Brad” mannequin head.
In our current study, we normalized the filtration at the receiver for Max Ex, the average concentration of particles presented to the receiver with no protection (1.363% of exhaled activity). As a result, we found that the N95 at the receiver did in fact filter approximately 95% of the aerosol, yet the reductions in exposure by source control (mask on the source) were significantly greater than the filtration ability of the N95 in reducing exposure.
Surgical masks were developed to reduce the transmission of respiratory pathogens in the operating room (source control). In contrast, N95 respirators are air-purifying devices that filter aerosolized particles with high efficiency, aiming to reduce the risk of disease acquisition. Despite the difference of purpose, the literature assessing the “protective” value of these masks traditionally focuses on head-to-head comparisons of only the filtration capacity of surgical masks versus N95 respirators (usually confined to studying receiver protection only, with masks glued to the face).(8,9) In concordance with previous studies, whether on the source or the receiver, N95 respirators are more effective as filtering devices (Fig. 6). However, our data demonstrate that the overall protection of the individual by reducing aerosol exposure is more complex than the results of simple filtration protection. Our experimental model, which considers the interaction of both the source and the receiver, demonstrates that other mechanisms of mask protection can be more important than filtration alone. The mask on the source significantly reduces exposure even if the particles are not captured via filtration but are deflected away from the receiver.(1) Figure 1 depicts the complex interplay of protective factors important in the transmission particles between two individuals. These include breathing pattern, environmental airflow, the fit of masks, filtration, deflection of particles, and aerosol distribution. Future studies will attempt to define further the contributions of each of these factors to help delineate better strategies for improving protection to the caregiver and other noninfected individuals exposed to potentially infective aerosols.
Although no in vitro model can guarantee in vivo results, our research attempts to model transmission and quantitatively study factors involved in the control of infectious respiratory diseases. These studies are not possible in vivo. The present article asks important technical questions regarding mask fit and sets the stage for future studies. To assess the importance of fit, we used a single breathing pattern, without variation in minute ventilation under only one environmental condition, whereas in real life, patients with respiratory illness may also cough and sneeze. The flow of air in the chamber mimicked only one form of room ventilation (negative-pressure room). The work of Diaz and Smaldone already established that environmental flow is a key variable that influences protection. These and other variables will be assessed in more detail in future studies.
A comprehensive infection-control program focused on prevention (e.g., vaccination), and respiratory protection is an important part of reducing potentially lethal outcomes from periodic outbreaks of respiratory illnesses that reach epidemic proportions. The large majority of the respiratory protection and transmission literature focuses only on filtration protection of the caregiver (receiver). The data supporting their recommendations are based on in vitro studies with masks glued to mannequin heads, and do not address the interplay of the various variables described in our model including masking the source. Although our study does not “prove” the value of source control, it proves that it is an important factor that should not be ignored. In support of this approach, Dharmadhikari et al. showed that having a patient wear a loose-fitting surgical mask reduced tuberculosis transmission by 56%.(10)
Further studies focused on the complex interaction of an “infected source” and a receiver using either a cough model or situations mimicking increased minute ventilation may be beneficial. As mentioned, caution should be exercised in directly extrapolating conclusions from bench research studies directly to the bedside until appropriate clinical research is conducted.
Footnotes
Acknowledgments
The authors would like to thank Lorraine Morra, BS, for technical assistance.
Author Disclosure Statement
This study was supported in part by Cantel Medical Corp. (Little Falls, NJ). Dr. Mansour has no conflicts of interest. Dr. Smaldone serves as a consultant to Cantel Medical. The State University of New York at Stony Brook owns patents on mask design.