
Abstract
Abstract
Background:
MAP0004 is an investigational orally inhaled dihydroergotamine (DHE) delivered via a TEMPO® metered dose inhaler that was effective in the acute treatment of migraine in a large Phase 3 trial. Rapid and consistent absorption of DHE is important for efficacy in the acute treatment of migraine.
Methods:
The pharmacokinetic parameters from four recent clinical studies, with doses including the proposed clinical dose of 1.0 mg nominal (0.65 mg emitted) MAP0004, were assessed for the consistency and speed of absorption of DHE.
Results:
Across these studies, MAP0004 administration resulted in rapid DHE absorption, with a median time of maximum concentration (Cmax) of approximately 10 min. The Cmax and area under the curve from time zero to 2 hr associated with the MAP0004 1.0 mg nominal dose were also similar between the three studies with this dose. Cmax values after 1.0 mg MAP0004 administration were consistently lower than for 1.0 mg intravenous DHE administration, and Cmax appeared to correlate with incidence of nausea. In these studies, DHE absorption through the lung was fast, consistent, and not associated with any unique tolerability issues for this route of administration.
Conclusions:
These results provide evidence of the consistency of absorption that can be achieved with the use of an appropriate metered dose inhaler, which may translate into a predictable therapeutic response.
Introduction
In addition, receptor binding and function assays have been performed to determine which receptors were activated at varying concentrations of DHE and its primary metabolite, 8′-hydroxydihydroergotamine (8′-OH-DHE). The receptor-binding profile of MAP0004 suggests that systemic DHE concentrations attained after MAP0004 dosing are sufficient to trigger anti-migraine receptors to the same degree as after intravenous (IV) dosing, while likely minimizing the activation of receptors responsible for the adverse event profile characteristic of IV DHE (nausea, dizziness, cardiovascular effects, and potential fibrotic effects).5,6
The four studies presented here are: (1) a study in smokers and nonsmokers to assess the impact of smoking on MAP0004 pharmacokinetics(7); (2) a study of the effect of MAP0004 on pulmonary arterial pressure over 4 hr with administration at 0 and 2 hr (submitted for publication); (3) a study of the potential for a drug–drug interaction of MAP0004 with a potent CYP3A4 inhibitor(8); and (4) a thorough QT study at a supratherapeutic dose of 3.0 mg of MAP0004. The first three studies were performed at the MAP0004 proposed nominal dose of 1.0 mg and included 1.0 mg of IV DHE for comparison, because this is the approved IV dose for the acute treatment of migraine.
In addition to these four studies, two previous studies of MAP0004 with PK data have already been published: an initial Phase I single ascending dose study that was conducted in healthy volunteers, the majority of whom were male,(9) and a study in subjects with asthma.(10) The results from these two previously published studies are not discussed here. In the four studies presented in this article, which were conducted as part of the MAP0004 clinical development program, subjects were selected to be demographically similar to the population intended to use the product. The pharmacodynamics results, including tolerability, have been reported previously(7,8) or have been submitted for publication. The assessment of the pooled data from these studies provides a more comprehensive overview of the consistency of systemic exposure. As the efficacy and adverse events following DHE administration are presumably a function of systemic DHE concentration, consistency of achieving plasma concentrations is an important consideration.
Methods and Materials
All studies reported here were conducted in accordance with Good Clinical Practice and the ethical principles of medical research involving human subjects of the Declaration of Helsinki.
Study drugs and devices
MAP0004 was manufactured under the direction of MAP Pharmaceuticals. Dihydroergotamine mesylate for injection (IV DHE) was supplied by Bedford Laboratories as a single-use vial containing 1 mg in 1 mL of a clear colorless sterile solution. One milligram of IV DHE was used as a comparator in the studies described, because it is the approved IV dosage for the acute treatment of migraine.
Study subjects
The subjects in these studies were in good health and were nonsmokers other than the smokers in the smoking/nonsmoking study. In the smoking/nonsmoking study, the smokers were currently smoking at least 10 cigarettes/day for at least 1 year with a positive urinary cotinine result at screening. All subjects were trained to properly use the TEMPO inhaler.
Subjects were eligible for these studies if they were between the ages of 18 and 45. Women had to be either sterile or practicing an adequate form of contraception. Women who were pregnant or breastfeeding or were planning a pregnancy during the study were excluded.
All subjects had to have stable cardiac status with normal rhythm (or arrhythmia deemed clinically insignificant on an electrocardiogram), a resting heart rate between 40 and 100 beats per minute, and a QTc interval using Fredericia's and Individualization correction methods not greater than 450 msec.
A history of coronary artery disease (CAD), or risk factors for CAD (such as hypertension, hyperlipidemia, family history of premature CAD, or diabetes mellitus), were reasons for exclusion. A history of cerebral vascular incident, transient ischemic attacks, or seizures was also grounds for exclusion. A history of bronchospasm with any inhaled medication or other inhaled substance, such as chlorofluorocarbon or hydrofluoroalkane propellants, was grounds for exclusion. A history of concurrent illness that required hospitalization within 30 days prior to screening or a history of unstable psychiatric illness requiring medication or hospitalization in the previous year was an additional reason for study exclusion.
Subjects were ineligible if they had a contraindication to DHE, a history of hemiplegic or basilar migraine, a diagnosis of cancer (other than noninvasive skin cancer) in the last 5 years, a known allergy or sensitivity to study drugs or their formulations, clinically significant liver or kidney disease, a history of chronic pulmonary disease, or if they had major surgery, vascular surgery, or sepsis during the previous 6 months.
In order to remain in the studies, subjects needed to maintain good health during the studies and were required to provide consent to participate.
Study designs
Table 1 summarizes the study designs and the PK parameters determined in each.
Note: M=male; F=female.
AUC0–t is defined as AUC0–48, AUC0–4, AUC0–48, and AUC0–36 where the sample period is 48, 4, 48, and 36 hr, respectively.
Referred to as smoker/nonsmoker study.
Referred to as PASP study.
Referred to as DDI study.
Referred to as TQT study.
Effect of smoking (smoker/nonsmoker study)
The primary objective of this study was to compare DHE pharmacokinetics following oral inhalation and IV administration in smokers and nonsmokers. The clinical significance of any differences between smokers and nonsmokers in tolerability of MAP0004 was also evaluated. This was a single-dose, open-label, two-period crossover study (in two sequences) comparing MAP0004 (1.0 mg nominal dose) to 1.0 mg IV DHE in smokers and nonsmokers. Blood samples were collected to 48 hr post dose, and plasma samples were analyzed to determine concentrations of DHE and the 8′-OH-DHE metabolite. Forty-seven healthy adults were enrolled (24 nonsmokers and 23 smokers).
Acute effects on pulmonary arterial pressure (PASP study)
The primary objective of this study was to compare the acute effect of DHE administered via oral inhalation and IV DHE on pulmonary arterial systolic pressure (PASP) as determined by echocardiography. Additional objectives were to assess the pharmacokinetics of DHE and its metabolites and to compare the pharmacokinetics and pharmacodynamics of repeat MAP0004 dosing, given as two 1.0 mg doses (at time 0 and 2 hr), to a single 1.0 mg IV dose given at time 0.
This was a single-dose, double-blind (double-dummy), three-period crossover study comparing MAP0004 (1.0 mg nominal dose) to 1.0 mg IV DHE to placebo in healthy volunteers. At each treatment visit, the study drug was administered followed by 2 hr of study assessments, and then the sequence of events was repeated a second time for a total of 4 hr. The first dose at time 0 included inhalation administration (MAP0004 or placebo inhaler) and IV (over 1 min) administration (1.0 mg IV DHE or IV placebo). The second dose at 2 hr included only inhaled administration (MAP0004 or placebo inhaler). Serial blood samples were collected during the entire 4-hr interval, and plasma samples were analyzed to determine the DHE and 8′-OH-DHE metabolite concentrations. Twenty-four healthy adults enrolled in the study.
Impact of potent CYP3A4 inhibitor on DHE pharmacokinetics (DDI study)
The primary objective of this study was to assess the potential for a potent CYP450 3A4 inhibitor (ketoconazole) to affect DHE metabolism following MAP0004 administration. This was a single-dose, open label, three-period sequential study comparing MAP0004 (1.0 mg nominal dose) alone to a single dose of MAP0004 1.0 mg following 4 days of ketoconazole oral dosing at 400 mg once a day and 1.0 mg IV DHE. Seven to 11 days after coadministration of MAP0004 with ketoconazole, IV DHE was administered. A blood sample was obtained prior to each dose, and serial blood samples were collected for 48 hr post dose to determine DHE and 8′-OH-DHE concentrations. Twenty-four healthy adults enrolled in the study.
Thorough QT study (TQT study)
The primary objective of this study was to compare the acute effect of a supratherapeutic (3.0 mg) dose of MAP0004, moxifloxacin 400 mg, and placebo on the QT interval corrected by Fredericia's and Individualization methods. The secondary objectives were to assess the tolerability of the supratherapeutic (three times the 1.0 mg intended dose) dose, to assess DHE systemic exposure at 3.0 mg and to assess any relationship between the DHE plasma concentrations and changes in corrected QT interval.
This was a single-dose, double-blind, three-period crossover study comparing a supratherapeutic dose of MAP0004 (3.0 mg nominal) to moxifloxacin 400 mg to placebo. Subjects were given 3.0 mg MAP0004 or placebo and oral moxifloxacin or placebo at each visit. At each visit, a predose blood sample and postdose serial blood collections to 36 hr were obtained for the determination of plasma DHE and 8′-OH-DHE concentrations. Fifty-four healthy adults (34 female, 20 male) were randomized in this three-period, six-sequence, crossover study.
Assay
A sensitive and specific assay for plasma DHE and its metabolites was developed. The assay was developed, conducted, validated, and reported by the analytical laboratories of Simbec Research Limited (Merthyr Tydfil, UK).
The assay method used high-performance liquid chromatography in conjunction with tandem mass spectrometry (LC-MS/MS) for the determination of plasma DHE and 8′-OH-DHE metabolite concentrations. The lower limit of quantitation of the assay was 10 pg/mL for DHE and 20 pg/mL for 8′-OH-DHE. Some plasma samples were also analyzed to determine if any of the minor putative metabolites, i.e., 8′,10′-dihydroxydihydroergotamine, dihydrolysergic acid amide, and dihydrolysergic acid, were being formed in vivo.
The linear range of the DHE assay was from 10 to 5,000 pg/mL with a percent coefficient of variation (CV%) of 53. Accuracy was estimated to be 94.6% to 95.5%, with an imprecision of less than or equal to 11.5%. The recovery from plasma was 85.0% (CV% of 2.1). This assay is more sensitive than previous methodologies based on HPLC with fluorometric detection.(11)
Bioanalytical stability studies were of sufficient scope and duration, and results of sufficient stability, to assure that the concentration values determined for samples collected during the development program for PK analysis were valid for all conditions experienced. Incurred Sample Reanalysis was completed on the TQT study samples, and the results were found to be acceptable.
PK analysis methodology
The PK parameters were derived from plasma concentrations of DHE and the 8′-OH-DHE metabolite using standard noncompartmental analysis methods(12) utilizing the software WinNonlin version 5.2 (Pharsight Corp., Sunnyvale, CA). Subjects who did not have evaluable PK data or who were statistical outliers were excluded from analysis. Outliers were defined as subjects with biologically improbable low or high exposure that was also outside the 95% confidence intervals (CIs) around the mean of other subjects. The PK parameters calculated for all four studies were maximum concentration (Cmax), time of Cmax (Tmax), area under the curve (AUC) from time zero to 2 hr (AUC0–2hr), and AUC from time zero to the last point of blood collection (AUC0–t); AUC zero to infinity (AUCinf) was calculated for the studies with at least 36 hr of blood sample collection. The half-life was determined using log-linear regression on the terminal portion of the concentration–time curve. For intravenously administered DHE, systemic clearance (CL) and the volume of distribution (Vd) were also determined.
AUC0–2hr was evaluated because this AUC interval could be determined for every study, including the PASP study, where a second dose was administered at 2 hr. In addition, DHE exposure in the first 2 hr following dosing is thought to be critical for pain relief and may be related to the side-effect profile.
The absolute bioavailability (F) of MAP0004 was determined relative to IV DHE. Bioavailability was calculated for both the nominal (the amount of drug discharged from the metering valve) MAP0004 dose of 1.0 mg and the emitted (the amount of drug discharged from the mouthpiece) dose, approximately 65% of the nominal dose.
Dose proportionality was assessed between the 1.0 mg and 3.0 mg dose levels by normalization of Cmax and AUC to 1.0 mg followed by t test comparison. Normalization of the 3.0 mg data was done by dividing Cmax and AUC by 3.
Statistical analysis
Statistical comparisons of Cmax and AUC0–2hr across studies for assessment of consistency in exposure was performed via analysis of variance using the software GraphPad Prism version 5.04 (GraphPad Software, Inc., La Jolla, CA). Post-hoc pairwise comparisons were done using Tukey's multiple comparison test. The same software was used to compare dose-adjusted Cmax and AUC between the 1.0 mg and 3.0 mg dose levels via t test.
Results
Subject disposition
A total of 149 subjects were enrolled in the four studies. All 149 received MAP0004. Six subjects either did not have evaluable PK data or were excluded as statistical outliers (five nonevaluable in the PASP study and one outlier in the DDI study(8)). Thus, MAP0004 PK data were obtained for a total of 143 subjects. For the 1.0 mg MAP0004 dose, PK data from a total of 66 nonsmoking subjects who received MAP0004 without co-administration of another drug were obtained.
Of the 149 enrolled subjects, 88 also received 1.0 mg IV DHE; 84 were evaluable for pharmacokinetics and four outliers were not included. PK data from a total of 62 nonsmoking subjects who received 1.0 mg IV DHE were obtained.
Subject demographics
Of the 149 subjects enrolled in the four clinical studies reported here, 97 were female (65.1%) and 52 were male (34.9%). The ages of the subjects ranged from 19 to 45 years, their body weights ranged from 48.3 to 112.4 kg, and their body mass index (BMI) ranged from 19.3 to 36.6 kg/m2. Two subjects self-identified as American Indian or Alaskan native (1.3%), 6 as Asian (4.0%), 17 as black or African American (11.4%), 1 as black/white (0.7%), 1 as native Hawaiian or other Pacific islander (0.7%), and 122 as white (81.9%).
Pharmacokinetics of DHE and 8′-OH-DHE following MAP0004 and IV DHE
The PK parameters for MAP0004 at nominal doses of 1.0 mg and 3.0 mg are presented in Table 2 along with parameters for IV DHE 1.0 mg. Parameters for the 8′-OH-DHE metabolite following MAP0004 and IV DHE administration are presented in Table 3. Table 4 summarizes combined data from the three studies with 1.0 mg MAP0004 administration. This table also summarizes the data from the TQT study after normalization from the dose of 3.0 mg to 1.0 mg.
N, geometric mean (CV%). Median for Tmax.
AUC0–t is AUC0–2, AUC0–4, AUC0–36, and AUC0–48, for t of 2, 4, 36, and 48 hr, respectively.
F=bioavailability based on nominal dose.
F=bioavailability based on emitted dose, which was approximately 65% of nominal dose.
AUC2–4 hr.
N, geometric mean (CV%). Median for Tmax.
AUC0–t is AUC0–2, AUC0–36, and AUC0–48, for t of 2, 36, and 48 hr, respectively.
Percent of parent exposure based on Cmax.
Percent of parent exposure based on AUC0–t.
AUC0–t is AUC0–2hr.
Data from 24 and 24 subjects in the smoking study, 19 and 18 subjects in the PASP study, and 23 and 20 subjects in the DDI study for inhaled and IV, respectively.
Also shown are data from 54 subjects in the TQT study who were given 3 mg orally inhaled MAP0004. Cmax and AUC values for these 54 subjects were normalized to a dose of 1 mg for comparison.
Effect of smoking (smoker/nonsmoker study)
The results for this study showed significantly lower plasma DHE and 8′-OH-DHE metabolite concentrations in smokers compared with nonsmokers after MAP0004 administration. The MAP0004 Cmax was 2,551 pg/mL in nonsmokers and 1,282 pg/mL in smokers. The AUC0–inf was 4,516 pg.hr/mL in nonsmokers and 3,393 pg.hr/mL in smokers, a 25% reduction. Bioavailability in nonsmokers was 0.37 and 0.57 based on nominal and emitted dose, and was 0.29 and 0.45 in smokers. Half-life was similar between the two groups (14.5 and 16.1 hr for nonsmokers and smokers, respectively).
Acute effects on pulmonary arterial pressure (PASP study)
The PK parameters observed in this study were similar to those in previous studies. The MAP0004 Cmax after the first 1 mg nominal dose was 2,357 pg/mL and 2,609 pg/mL after the second dose at 2 hr. The Tmax was 12 min for the first MAP0004 dose and 10 min for the second dose at 2 hr. The AUC0–2hr averaged 1,234 pg.hr/mL for the first dose and 1,513 pg.hr/mL for the second dose. Because blood was collected for only 4 hr, calculation of half-life and other PK parameters was not performed.
Impact of potent CYP3A4 inhibitor on DHE pharmacokinetics (DDI study)
The results demonstrated that there was little or no effect of ketoconazole on DHE exposure following MAP0004 administration. The AUC0–inf increased from 3,784 pg.hr/ml to 4,323 pg.hr/ml following ketoconazole co-administration with MAP0004. This increase was not statistically or clinically significant. There was no effect on Cmax (2,583 vs. 2,495 pg/mL) or half-life (13.5 vs. 11.2 hr).
The 8′-OH-DHE metabolite exposure increased with ketoconazole, and the increase was statistically significant compared with MAP0004 administered without ketoconazole. The 8′-OH-DHE Cmax increased by 15% (from 69 to 80 pg/mL), and the AUCinf increased by 248%. However, such low metabolite plasma concentrations following ketoconazole co-administration are unlikely to produce any pharmacologic effect.
The absolute bioavailability of MAP0004 DHE alone was 0.38 (nominal dose) and 0.58 (emitted dose). The absolute bioavailability of MAP0004 co-administered with ketoconazole was 0.46 (nominal) and 0.71 (emitted). This increase in bioavailability is consistent with the small increase in exposure observed with ketoconazole inhibition.
Thorough QT study (TQT study)
The Cmax associated with the 3.0 mg MAP0004 dose (8,757 pg/mL) was approximately 3.8 times that observed at the 1.0 mg nominal dose. The AUC0–inf averaged 13,464 pg.hr/mL and was 3.0 to 3.6 times that of the 1.0 mg nominal dose. The 8′-OH-DHE metabolite Cmax was 183 pg/mL, which was approximately three times that observed after the 1.0 mg nominal dose. The MAP0004 DHE Tmax and half-life values were similar to those observed in previous studies.
Comparison across studies
The DHE concentration–time profiles over the first 2 hr after 1.0 mg of MAP0004 or DHE IV are shown in Figure 1A on a semilog scale and in Figure 1B on a linear scale. Also plotted is the concentration profile for the TQT study after dose normalization to 1.0 mg. For inhaled administration, the results were similar for all three studies that used 1.0 mg MAP0004, with Cmax of greater than 2,000 pg/mL being seen in less than 0.25 hr and mean concentrations at subsequent time points also being similar. The consistency in exposure following 1.0 mg MAP0004 is demonstrated in Figure 2, which shows box plots of Cmax (Fig. 2A) and AUC0–2hr (Fig. 2B) across three studies (PASP study, DDI study, and nonsmokers in the smoker/nonsmoker study). Also shown are the data from the TQT study after dose normalization to 1.0 mg.
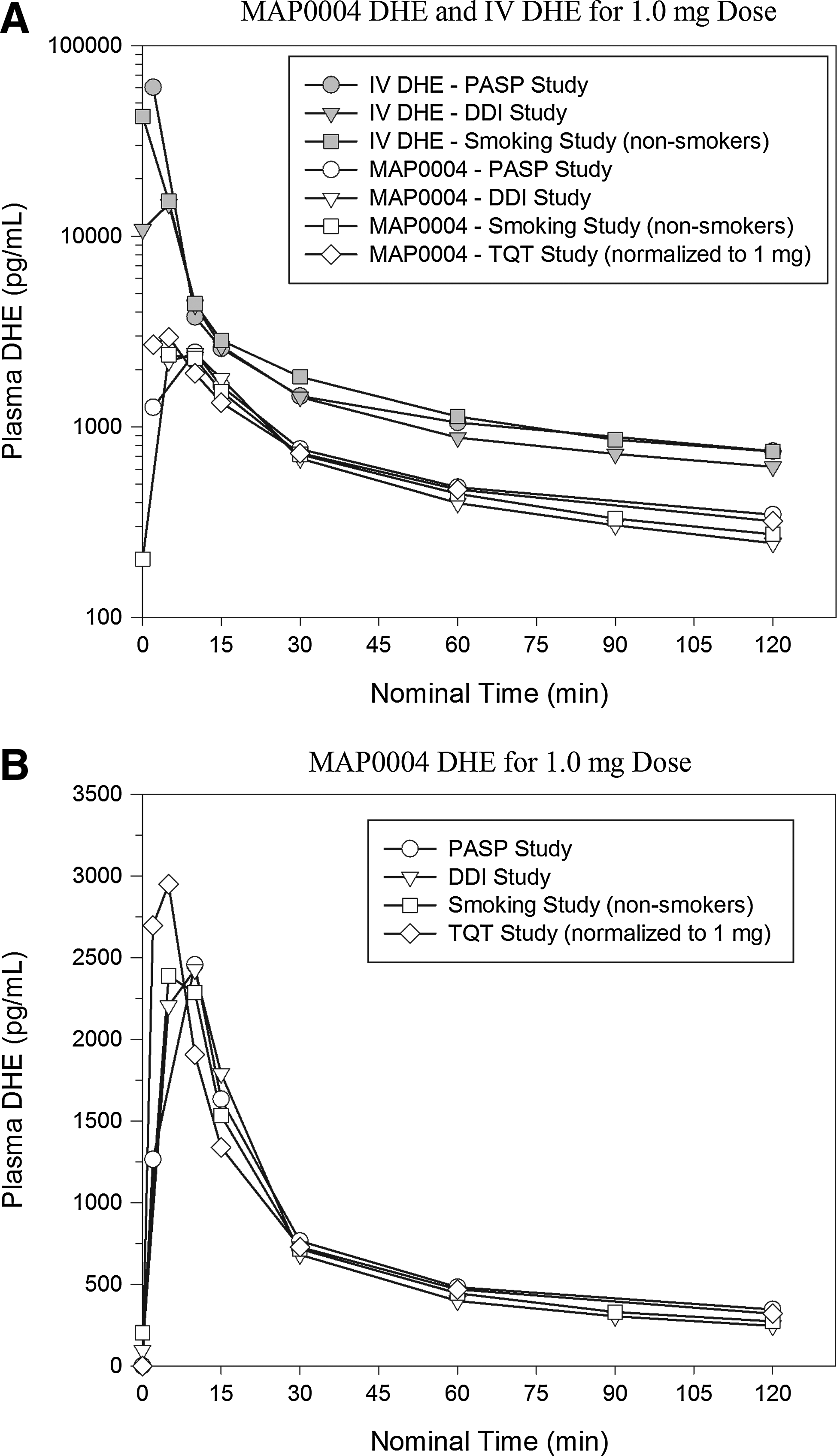
Concentration–time profiles of geometric mean DHE following 1.0 mg dose from MAP0004 oral inhalation or IV (1 min). The graphs include the concentration-time profile from the TQT study for which the concentrations were normalized from 3 mg to 1 mg.

DHE plasma Cmax
An analysis of variance did not show a difference in either parameter across the three studies done at 1 mg (p values of 0.4390 for Cmax and 0.4932 for AUC0–2hr) or across the three studies at 1 mg plus the dose-normalized TQT data (p values of 0.2975 for Cmax and 0.5383 for AUC0–2hr).
An unpaired t test showed no difference in either Cmax or AUC0–2hr between the pooled data from the three studies at 1.0 mg dose versus the TQT study after dose normalization (p values of 0.0692 for Cmax and 0.9055 for AUC0–2hr). This indicates dose proportionality across the range of doses from 1.0 to 3.0 mg. It should be noted that although Cmax for dose-normalized TQT was higher than that for the pooled Cmax for 1.0 mg (3,068±963 pg/mL for TQT vs. 2,720±1,088 pg/mL for 1.0 mg in Table 4), this difference was not statistically significant.
Summarized across studies, 1.0 mg MAP0004 resulted in a Cmax for the 8′-OH-DHE metabolite averaging 71 pg/mL (geometric mean) and ranging from 34 to 200 pg/mL (Table 4). This average is significantly lower than after 1.0 mg IV DHE, for which Cmax averaged 296 pg/mL and ranged from 23 to 884 pg/mL. The half-life for the 8′-OH-DHE metabolite following 1.0 mg MAP0004 averaged 12.9 hr without ketoconazole in the DDI study and was shortened by co-administration with ketoconazole to 9.4 hr (Table 3).
In vitro/in vivo comparison
The aerodynamic particle size distribution of MAP0004 delivered from the TEMPO inhaler was characterized by cascade impaction at 28.3 L/min, and the resulting fine particle dose (FPD) of less than 5 μm was compared with the Cmax values measured in vivo. The FPD represents the mass of drug that has the greatest probability of bypassing the larynx and impacting within the airways, where it can then be absorbed into the systemic circulation. The FPD and resulting Cmax for three separate manufactured lots of the MAP0004 are shown in Table 5. Across the four studies evaluated in this analysis, there is very strong dose-to-dose consistency as demonstrated by the quantified FPD for each lot of manufactured material. This in turn translates into a consistent Cmax, as highlighted by a calculated coefficient of variation of less than 50% in each of the four studies. The strong dose-to-dose consistency from the TEMPO inhaler is a key contributor to the consistent Cmax observed with MAP0004.
Nonsmokers only.
Cmax after the first dose of MAP0004.
Pre-ketoconazole treatment.
TQT study 3.0 mg dose, normalized to 1.0 mg for comparison.
Discussion
Comparison of MAP0004 data presented here with data from the IV route of DHE administration is discussed in this section. The discussion is organized according to the standard ADME processes for drug absorption and disposition (distribution, metabolism, and excretion).
Absorption
MAP0004 is rapidly absorbed, as shown by a median Tmax of 0.167 hr (10 min) ranging from 0.067 hr to 0.250 hr (4 to 15 min) for the 1.0 mg dose (Tables 2 and 4). The bioavailability of 1.0 mg MAP0004 was 0.37 for nonsmokers in the smoker/nonsmoker study and 0.38 for subjects in the DDI study (absent ketoconazole administration) based on the nominal dose, or 0.57 and 0.58 based on the emitted dose, respectively.
The observed differences in DHE exposure between smokers and nonsmokers following MAP0004 administration may be due to reduced pulmonary absorption in the smoker population. Smokers have been shown to have reduced aerosol penetration to the small airways and more central airway deposition, which may result in lower absorption of inhaled DHE into the bloodstream.(13)
The reported increased production of sputum in smokers may be another explanation for the reduced absorption of orally inhaled DHE in this population. Airway absorption and bioavailability of inhaled corticosteroids have been shown to be lower in subjects with chronic obstructive pulmonary disease (COPD), with a larger fraction of inhaled drug expectorated in the sputum of COPD subjects.(14)
Metabolism
Four DHE metabolites have been identified in human plasma following oral administration.(15,16) The major metabolite, 8′-OH-DHE, exhibits affinity equivalent to its parent for adrenergic and 5-hydroxytryptamine receptors and demonstrates equivalent potency in several venoconstrictor activity models, in vivo and in vitro.(15) In quantitative PK characterization, 8′,10′-dihydroxydihydroergotamine and dihydrolysergic acid metabolites were below the lower limit of quantitation. Dihydrolysergic acid amide was present only at low levels (approximately 25 pg/mL).
Following 1.0 mg MAP0004 administration, the relative exposure, based on Cmax, for the 8′-OH-DHE metabolite compared with the parent DHE was 2.37% (nonsmokers in the smoker/nonsmoker study) and 2.68% (subjects in the DDI study not receiving ketoconazole) (Table 3). The 8′-OH-DHE metabolite AUC0–48hr averaged 5.78% and 6.37% that of parent for the nonsmokers in the smoker study and in the DDI study, respectively. For smokers, the metabolite Cmax and AUC0–48hr averaged 2.93% and 8.53% compared with DHE. In the DDI study, following ketoconazole administration, the metabolite Cmax was 3.19% that of parent, but AUC0–48hr increased to 20.6% relative to parent. Although ketoconazole clearly had an impact on 8′-OH-DHE levels, the increase in parent exposure was not clinically significant, and the increase in metabolite exposure was likely too low to achieve a pharmacological effect.
Following 1.0 mg IV DHE, the 8′-OH-DHE metabolite Cmax relative to DHE was 0.46% and 0.66% for smokers and nonsmokers in the smoker/nonsmoker study, respectively, and 1.20% for the DDI study. The metabolite AUC0–48hr was 4.26% (smokers), 4.65% (nonsmokers), and 5.72% (DDI study).
Half-life
The plasma concentration versus time profiles for MAP0004 and IV DHE from the three studies at 1.0 mg showed evidence of biexponential or perhaps triexponential decline with time (Fig. 1). This figure also shows the profile for the dose-normalized concentrations from the TQT study.
The half-life for DHE following 1.0 mg MAP0004 averaged 16.1 hr (smokers), 14.5 hr (nonsmokers), and 13.5 hr (subjects in the DDI study not receiving ketoconazole) (Table 2). The co-administration of ketoconazole with MAP0004 did not impact half-life (11.2 hr). The half-life after 3.0 mg MAP0004 was similar at 11.7 hr. The half-life following IV DHE was 13.3 hr (smokers), 12.4 hr (nonsmokers), and 11.1 hr (in the DDI study).
The half-life for the 8′-OH-DHE metabolite following 1.0 mg MAP0004 averaged 12.9 hr without ketoconazole in the DDI study and was shortened by co-administration with ketoconazole to 9.4 hr (Table 3). Administration of 3.0 mg MAP0004 in the TQT study did not alter the metabolite half-life (10.9 hr). Following IV DHE, the metabolite half-life averaged 13.9 and 10.7 hr in smokers and nonsmokers, respectively, and 12.4 hr in the DDI study. Thus, the metabolite half-life after either a 1.0 mg or 3.0 mg MAP0004 or 1.0 mg IV DHE dose was about the same as the parent half-life, indicating formation rate limited kinetics.
Comparison of Cmax for MAP0004 versus IV DHE
In comparison with DHE delivery by the IV route, MAP0004 1.0 mg produced peak concentrations (Cmax) that were approximately 20 times lower than after IV administration. As shown in Table 4, the Cmax following 1.0 mg MAP0004 averaged across three studies resulted in a geometric mean of 2,507 pg/mL (arithmetic mean of 2,720±1,088 pg/mL) with a CV% of 40.0. In contrast, the Cmax for IV administration of 1.0 mg was 54,189±34,970 (geometric mean of 44,106 pg/mL). The variability for IV DHE was high compared with that for MAP0004 (CV% of 64.5).
As reported by Shrewsbury et al.(9) and later Jividen,(5) the incidence of nausea increases in subjects with higher Cmax values. The incidence of nausea in a recently completed MAP0004 Phase 3 trial(17) was 5.2%, which is a lower incidence than was reported in a large efficacy trial that utilized subcutaneous administration.(18)
Consistency in DHE exposure following MAP0004
It is important to avoid large variations in DHE exposure that may lead to tolerability issues, if the exposure is too high, and efficacy issues, if the exposure is too low. The optimal plasma concentration boundaries have not yet been identified, but the incidence of nausea has been reported to be plasma concentration–related. The 3.0 mg supratherapeutic MAP0004 dose in the TQT study produced a higher incidence of nausea than observed after a 1.0 mg MAP0004 dose, reflecting that nausea may be related directly to increased DHE exposure level. Therefore, increased variability in exposure following a given DHE dose might produce a higher risk of nausea, for example.
Consistent exposure from the TEMPO inhaler might have been predicted by the in vitro characteristics. The FPD and Cmax for three separate lots of the product are shown in Table 5. The consistent FPD values correlate with the consistent Cmax values and verify an association between the in vitro performance of the TEMPO inhaler and the in vivo PK characteristics. This consistent exposure following MAP0004 administration is an important attribute that may contribute to consistent therapeutic effect.
The similarity in the PK parameters observed in the three clinical studies at 1.0 mg dosing provide evidence that exposure following MAP0004 administration via the TEMPO inhaler was consistently reproducible. This is shown by comparison of Cmax and AUC values across studies, as summarized in Table 4. The CV% for Cmax was 40% for 1.0 mg MAP0004 as compared with CV% of 65% for 1.0 mg IV DHE. However, the CV% for AUC0–2hr was similar, 37.4% for MAP0004 versus 43.6% for IV DHE. The 95% CIs are also shown in Table 4 and do not overlap between MAP0004 and IV DHE for either Cmax, AUCinf, or AUC0–2hr. The 95% CI for Cmax following 1.0 mg MAP0004 was 2,453 pg/mL to 2,988 pg/mL compared with 45,308 pg/mL to 63,069 pg/mL for 1.0 mg IV DHE. The range in Cmax for 1.0 mg MAP0004 was from 791 to 6,803 pg/mL compared with the 1.0 mg IV DHE range from 10,579 to 183,399 pg/mL.
Pharmacokinetics/pharmacodynamics: onset of efficacy in relation to pharmacokinetics
In a pivotal study, pain relief following MAP0004 1.0 mg was rapid in many subjects,(17) which was consistent with the rapid absorption demonstrated by the Tmax between 4 and 15 min. Exposure in the first 2 hr is likely important to pain relief and justifies the emphasis on Cmax and early AUC (AUC0–2hr). AUC0–2hr is predictive of AUCinf as was demonstrated by good fit to a linear regression (data not shown). On average, AUC0–2hr was 32% of AUCinf.
Conclusions
In these four PK studies, MAP0004 administration resulted in rapid and consistent exposure to DHE. The 1.0 mg nominal dose resulted in mean Cmax and AUC0–2hr values that were not statistically different across these four recent studies. The intersubject variability in Cmax was 40% (CV%) for MAP0004 as compared with 65% for IV DHE. The consistency of absorption may be important in the therapeutic use of the product.
Footnotes
Acknowledgments
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors. The studies reported here were funded entirely by MAP Pharmaceuticals, Inc. TEMPO® is a registered trademark of MAP Pharmaceuticals, Inc.
Author Disclosure Statement
No conflicts of interest exist. D. Kellerman, S. Borland, and S. Kori are full-time employees of MAP Pharmaceuticals. A. Forst and D. Combs are currently paid pharmacokinetic consultants for MAP Pharmaceuticals.