
Abstract
Abstract
Background:
The Tyvaso Inhalation System is a hand-held nebulizer system used to administer treprostinil, an approved therapy for pulmonary arterial hypertension. Our goal was to establish an in vitro method for delivering a standard dose of treprostinil through a ventilator circuit and artificial airway.
Methods:
An AeroTech II jet nebulizer (continuous air flow at 10 L/min; Biodex Medical Systems) was placed in the ventilator circuit with a test lung. Two ventilators were tested, the Dräger Evita 2 Dura (Dräger Medical GmbH) and Avea (CareFusion), without humidity. Delivered dose was defined by capturing radiolabeled particles exiting the endotracheal tube with a filter (Pari) and measuring radioactivity. Particle distributions were measured distal to the endotracheal tube by cascade impaction. We hypothesized that drug delivery would be determined by the number of breaths needed, such that the complete time of inspiration totaled 29 sec (e.g., number of breaths needed=29 sec/TI, where TI is the inspiratory time of an average breath read from the ventilator display).
Results:
Nebulizer output was linear for 6 min, and the standard prescribed target dose of 54 μg (3.1% of full ampule) was delivered in 29 sec. Using our TI algorithm to control delivery, the mean inhaled dose±SD was 72.2±16.5 μg (range 47.2–98.6; n=23). Dräger delivered higher doses than Avea. Effects of mode, breathing pattern, and positive-end expiratory pressures were not significant. The mass median aerodynamic diameter and fine particle fraction were 0.71±0.015 and 0.997±0.0006, respectively.
Conclusions:
Using the algorithm, it was possible to deliver aerosolized treprostinil, at controlled doses, via mechanical ventilation over a wide range of controlled breathing patterns. The conditions of nebulization must be precisely followed (one full ampule per treatment, use of the AeroTech II nebulizer, continuous nebulization using an external flow of 10 L/min, bypass of the humidifier or removal of in-line heat and moisture exchanger, and treatment completed in 6 min or less).
Introduction
Materials and Methods
In vitro model
We have established an in vitro model for measuring aerosol delivery during mechanical ventilation (Fig. 1). Two ventilators, the Dräger Evita 2 Dura (Dräger Medical GmbH, Lübeck, Germany) and Avea (CareFusion, Yorba Linda, CA), were tested. The ventilator was connected via a standard circuit (Hudson RCI, Universal 22mm Ventilator Circuit, Dual Heated Limb; Teleflex Medical, Research Triangle Park, NC) and an 8.0-mm endotracheal tube (Rusch, Teleflex Medical) to a test lung (Michigan Instruments, Grand Rapids, MI). Modes included continuous mechanical ventilation (CMV) with volume control (VC-CMV) and pressure control (PC-CMV) tested at varying pressures, tidal volumes, respiratory rates, inspiratory times, and positive-end expiratory pressures (PEEP) at 21% oxygen. Humidification was not used.
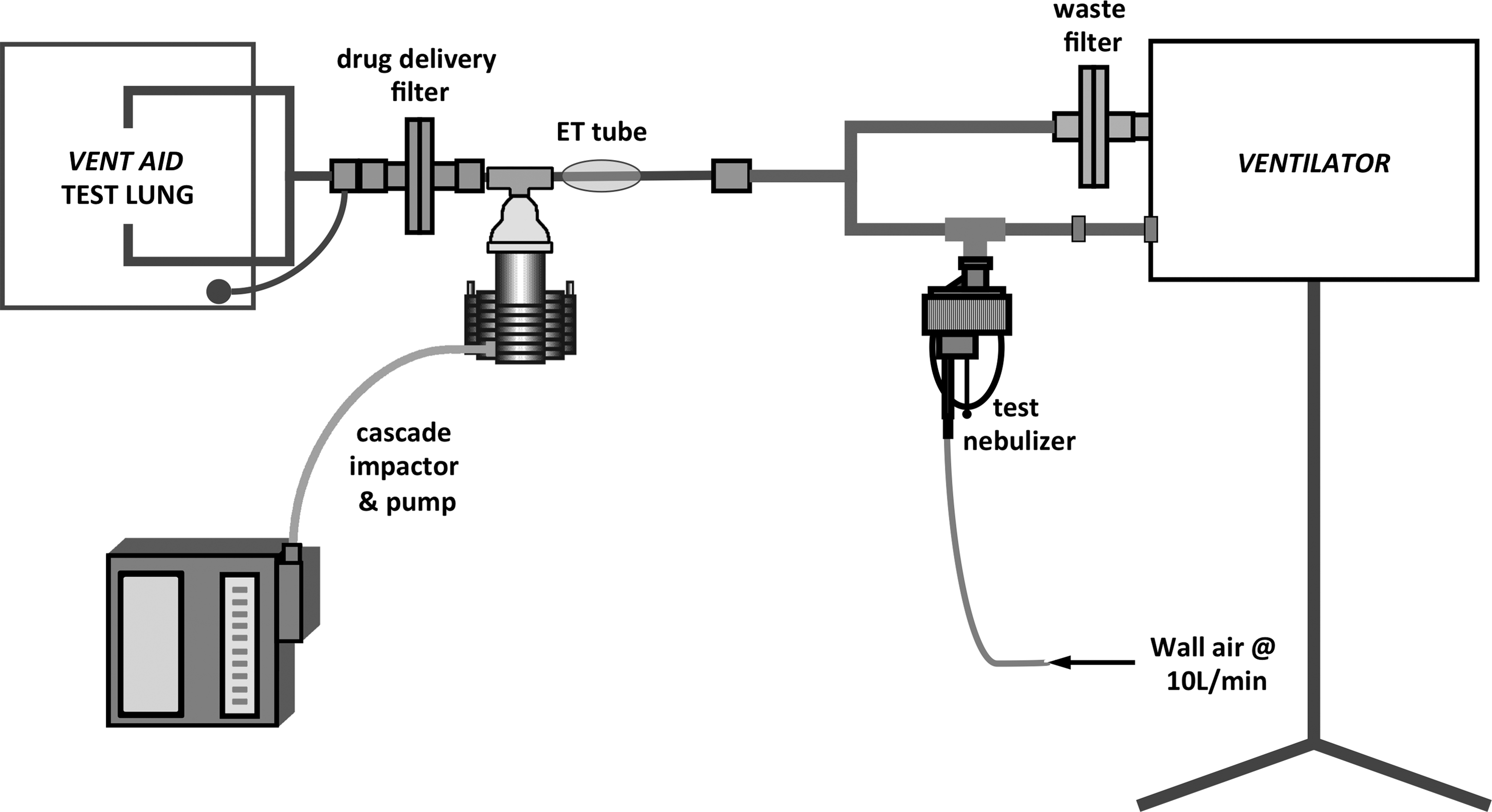
In vitro setup. The AeroTech II nebulizer was placed in the inspiratory line 12 inches proximal to the Y-adapter. The nebulizer was run with a continuous airflow at 10 L/min. The circuit was completed with the ventilator test lung. Radiolabeled particles that passed through the endotracheal tube were captured by the drug delivery filter, and radioactivity was measured in a well counter. In separate experiments, aerodynamic particle distribution was measured via a Marple cascade impactor placed between the endotracheal tube and the filter.
A jet nebulizer (AeroTech II; Biodex Medical Systems, Shirley, NY) was inserted into the inspiratory limb of the circuit in a standard position, 12 inches proximal to the Y-adapter. Test aerosols were captured by a filter (Pari, Starnberg, Germany) placed in the circuit distal to the endotracheal tube. Aerosols captured on this filter represent the delivered dose or particles that would be inhaled by a patient under similar conditions. Our goal was to specify conditions of delivery that would insure that the filter dose would approximate the delivered dose specified in the package insert (54 μg) inspired by a spontaneously breathing patient using the Tyvaso Inhalation System.
Nebulizer formulation and radiolabel assay
Our model uses radioactivity [99m-technetium (99mTc)] to measure drug delivery. Once validated, this method allows rapid measurement of aerosol delivery with a high degree of sensitivity and accuracy.(4,5)
To validate the use of 99mTc for treprostinil, we carried out a series of protocols. To establish a standard curve, three ampules of treprostinil [Tyvaso (0.6 mg/mL)] were combined to a total volume of 8.7 mL (to minimize pipetting errors) and mixed with approximately 10 mCi of 99mTc. Aliquots of radiolabeled treprostinil solution were pipetted into sample tubes containing high-pressure liquid chromatography (HPLC) assay buffer (Cirrus Pharmaceuticals Inc., Durham, NC). Sample volume was varied to create a distribution of samples within the range of the HPLC assay sensitivity (3–180 μg). For the standard-curve experiments, radioactivity was measured in a dose calibrator (Atomlab 100; Biodex Medical Systems), and time was recorded. After decay correction, a predicted amount of treprostinil was determined based on the amount of measured radioactivity in the sample. All samples were analyzed by HPLC at an independent laboratory (Cirrus Pharmaceuticals Inc.).
To measure potential effects of nebulization, several additional protocols were followed. Using the AeroTech II, single ampules (1.74 mg in 2.9 mL) of radiolabeled treprostinil solution were nebulized for 2–3 min. Following nebulization, samples of liquid remaining in the nebulizer were obtained via pipette. This maneuver tested the effects of nebulization on drug concentration and radioactivity within the nebulizer (e.g., whether drug or radiolabel was absorbed onto plastic). Finally, a separate series of nebulizer experiments was performed in which radiolabeled particles were captured by a cascade impactor (Marple 8-stage impactor; Thermo Fischer Scientific, Waltham, MA; 2 L/min flow). The stages of the impactor were washed and all material combined. Although each stage contained drug and radioactivity, all the material was combined, as each stage individually did not contain enough drug to be detectable by our HPLC assay. The combined liquid eluted from the stages was divided and assayed. Radioactivity in the different samples was used to predict the mass of drug from captured aerosol particles.
The nebulizer
Because nebulizer function is variable between brands and models,(6) we chose a single commercially available jet nebulizer (AeroTech II; Biodex Medical Systems) known to provide linear output with reasonable efficiency and predictable particle distribution for other soluble drugs.(4) We used three separate nebulizers in rotation for our experiments.
AeroTech II output
Before ventilator experiments were performed, nebulizer output (radioactivity per minute) was measured. Jet nebulizers require a defined flow of gas to generate aerosol. Commercial ventilators do not come with uniform sources of flow and pressure for nebulizer use, nor do all ventilators provide standardized, controlled breath actuation for nebulizers.(7) Therefore, we set a standard for nebulizer function by using an external flow source to run the nebulizer continuously (compressed air at 10 L/min at 50 psig). Similar gases are available in the hospital from wall air or oxygen. By using an external source with a defined nebulizer, the known variability of nebulizer/ventilator combinations is avoided.
The AeroTech II was filled with one ampule of radiolabeled treprostinil (1.74 mg, the nebulizer charge) and placed in the ventilator circuit with the endotracheal tube and drug delivery filter in place, but without a test lung and the ventilator turned off (Fig. 2). Under these circumstances, the continuous nebulization rate of treprostinil, solely influenced by the nebulizer gas (10 L/min) minus any tube losses, was assessed. The filter was changed every minute, and the cumulative radioactivity on the filters determined drug output over time.

Measuring output of the AeroTech II nebulizer. The nebulizer was filled with one ampule of radiolabeled treprostinil and placed in the ventilator circuit with the endotracheal tube and drug delivery filter in place, but without the test lung. The ventilator was turned off. The darkened tube illustrates the path of generated aerosol in the circuit.
Drug delivery during mechanical ventilation
From the nebulizer output data, we observed that it takes 29 sec of continuous nebulizer operation to deliver the standard 54-μg dose of treprostinil. During mechanical ventilation, aerosol particles are delivered to the patient only during inspiration. During respiratory pause or expiration, aerosol will be blown out of the circuit and wasted. To define aerosol delivery for common ventilator settings, we used the inspiratory time per breath (TI), a parameter readily available on modern commercial ventilators to define the number of breaths required to deliver the dose. The number of breaths necessary to deliver the required dose is calculated by Equation 1:
where TI is the inspiratory time in seconds of an average breath and 29 sec is the amount of time necessary to deliver 54 μg of treprostinil.
In addition to defining performance for the chosen nebulizer, our protocol tested the performance of two ventilators at commonly used adult settings plus a wide range of extreme values to test the limits of our predictive algorithm. Humidification, an unpredictable factor(8,9) known to affect aerosol delivery, was not tested.(10,11) For each experiment, the nebulizer was filled with a 1.74-mg ampule of treprostinil solution mixed with 99mTc and run for the number of breaths calculated from Equation 1 (breaths used by the operator from Equation 1 were rounded to the nearest integer). Although the nebulizer gas triggered the ventilator alarms, there were only small changes in actual tidal volume (confirmed by direct observation of the test lung).
Particle distribution
The AeroTech II was charged with one ampule of treprostinil mixed with a known amount of 99mTc and placed in the ventilator circuit with the cascade impactor (Fig. 1). With the ventilator running, the nebulizer was run for 8 min (Dräger Evita 2 Dura, VC-CMV, tidal volume 500 mL, respiratory rate 15 breaths/min, flow 30 L/min, inspiratory time 1.0 sec, PEEP 0 cmH2O, without humidity). Aerodynamic particle distributions were determined by measuring radioactivity on the stages and plotting the cumulative percentage of radioactivity against the log particle size on probability paper. This experiment was repeated three times.
Statistics
Descriptive statistics were described by means±SD and linear regression. Correlations were tested using Bland-Altman analysis. Group data were compared using 95% confidence intervals (CI). Calculations were performed using GraphPad Prism v6.0 for Mac OS X (GraphPad Software, San Diego, CA).
Results
Nebulizer formulation and radiolabel assay
Figure 3 presents the validation data for the labeled aerosols. The standard curve is shown in Figure 3A. Drug (in micrograms) in each sample was precisely predicted by radioactivity in the samples, as the data are close to the line of identity. Bland-Altman analysis in Figure 3B indicates that data remain close to the mean over the range of samples, except for the highest values. Potential effects of nebulization on the correlation are tested in Figure 3C. Here the linear regression line from Figure 3A is drawn without the data points. Then the data from the nebulized solutions were plotted (from the nebulizer cup post nebulization and the samples from the combined washings of the cascade impactor). All data points are near the line, indicating no systematic effects of mixing with the radiolabel or the nebulizer plastic during nebulization.
Validation of radiolabel; HPLC results compared with radioactivity.
AeroTech II output
Figure 4 shows nebulizer output over time plotted as percent nebulizer charge. Over the first 6 min, the output curve approximates a line represented by the linear regression equation y=0.1216x – 0.4257. Beyond 6 min, the delivery of medication was no longer linear. We found that 54 μg of drug (3.1% of the nebulizer charge) is delivered in 29 sec. This result is the basis for Equation 1, which, with the inspiratory time (TI), defines the total number of breaths needed to deliver 54 μg of drug for a given ventilator setting.

Cumulative nebulizer output expressed as percent nebulizer charge (one ampule of treprostinil) over time. Output over 6 min is approximated by the linear regression equation y=0.1216x – 0.4257 (p<0.0001); the dotted line represents 54 μg, the label dose (3.1% of nebulizer charge) at 29 sec. After 6 min of nebulization, output is no longer linear. Three experiments were performed.
Drug delivery during mechanical ventilation
Drug delivery (±95% CI) is plotted for ventilator type and mode in Figure 5 and listed in Tables 1 and 2. The mean inhaled dose±SD was 72.2±16.5 μg (range 47.2–98.6; n=23). For the Dräger, there was a systematic increase in drug delivery above the target dose. This was significant compared with the Avea. By confidence intervals, there was no significant effect for mode, breathing pattern, or PEEP (see Discussion).

Drug delivery for Dräger and Avea ventilators, volume control and pressure control modes (VC-CMV, PC-CMV±95% CI). The target dose of 54 μg is shown. Delivery for Dräger was significantly higher than that for Avea.
VC, volume control ventilation; f, breaths per min; VT, tidal volume (mL); VTE, exhaled tidal volume (mL); Vi, flow (L/min); Ti, Inspiratory time (sec); PC above PEEP, pressure control level above positive end expiratory pressure (cm H2O); PEEP, positive end expiratory pressure (cm H2O); No. of breaths nebulizer energized, (from eq (1) rounded to nearest integer); Dose delivered (μg of Treprostinil).
PC, pressure control ventilation; f, breaths per min; VT, tidal volume (mL); VTE, exhaled tidal volume (mL); Vi, flow (L/min); Ti, Inspiratory time (sec); PC above PEEP, pressure control level above positive end expiratory pressure (cm H2O); PEEP, positive end expiratory pressure (cm H2O); No. of breaths nebulizer energized, (from eq (1) rounded to nearest integer); Dose delivered (μg of Treprostinil).
Particle distribution
Aerosol distributions are shown for the three nebulizers in Figure 6. Data for the three devices were superimposed and highly reproducible. The mass median aerodynamic diameter (MMAD) and fine particle fraction averaged 0.71±0.015 and 0.997±0.0006, respectively. The mean±SD geometric standard deviation (GSD) was 1.81±0.012.
Cascade impaction data (log particle size vs. probability). The AeroTech II was charged with one ampule of treprostinil and a known amount of 99mTc and run for 8 min (Dräger in VC-CMV mode, tidal volume 500 mL, respiratory rate 15, flow 30 L/min, inspiratory time 1 sec, PEEP 0 cmH2O (n=3).
Discussion
In the intubated patient, drug delivery by aerosol can vary by an order of magnitude if the only instruction from the physician is the dose of drug to be placed in the nebulizer.(10) For treprostinil, this article defines key factors that provide enough practical guidance to the physician to reach a dose that is well within the range of variability seen in the spontaneously breathing patient using the Tyvaso Inhalation System.(12) Table 3 summarizes our algorithm in stepwise form. First, the nebulizer and its conditions of use [placement in the circuit, use of AeroTech II jet nebulizer, no heat and moisture exchanger (HME) in the circuit, or if a humidifier is used it must be bypassed] must be precisely followed; then with those requirements and our formula, it is possible to control delivery over a wide variety of settings, modes, and brands of ventilator. The common variable for all ventilator settings is the inspiratory time (TI), which was used to define the number of breaths needed for controlled delivery.
HME, in-line heat and moisture exchanger; TI, inspiratory time (sec).
It is important to note that our model including Equation 1 will apply only to patients who are not triggering the ventilator. Not all mechanically ventilated patients are ventilated using the CMV mode and, therefore, they may not have a consistent inspiratory time and respiratory rate. Prior to initiating treatment, we recommend that the clinician assess the patient's current minute ventilation and adjust the ventilator parameters to meet the patient's minute ventilation requirement, thus eliminating the patient's need to trigger. The adjusted settings will be used during drug delivery only and are to be returned to the pretreatment settings after dosing is achieved. We recognize that adjusting the ventilator parameters during aerosol therapy is not commonly practiced. However, delivery of this drug requires a precise inspiratory time in order to calculate the number of breaths needed to deliver the standard 54-μg dose of treprostinil. Pressure support ventilation, in which the respiratory rate and inspiratory time are not controlled, is not recommended during aerosol therapy with treprostinil.
Our approach to controlling delivery, although relatively simple, does not include all factors that might affect aerosol therapy. For example, we cannot precisely predict the effects of humidification. The delivery of water vapor in the intubated patient is not well standardized. It can range from no added vapor (e.g., HME, which obviously must be removed during any aerosol delivery) to varying amounts of vapor, depending on the type of humidifier and the ventilator settings.(8–10) It has been well documented for many years that humidification can significantly reduce aerosol delivery.(6,11) This observation has been reported for other drugs(10,13) and, based on all these points, we suggest that the humidifier be bypassed during aerosol treatment. This has been the policy at our institution for many years, and there have been no adverse effects in the presence of beneficial clinical results.(14)
Whereas the data for the Avea were clustered around the target dose, it is clear from Figure 4 that other factors for the Dräger affected delivery. To study this further, we plotted the data against the number of breaths calculated from Equation 1 (Fig. 7). According to our algorithm, drug delivery should be 54 μg. For both ventilators, there was a systematic increase in delivery with breath number, but the effect was significantly greater for the Dräger. Residual aerosol in the inspiratory line between breaths could explain proportional breath-related increases in delivery. The Dräger, which does not use bias flow, may retain a higher fraction of aerosol in the inspiratory line between breaths. The default bias flow of the Avea (2 L/min) may minimize this effect.

Drug delivery versus the number of breaths used for a treatment [filled symbols, Dräger; open symbols, Avea; circles, VC; squares, PC; best fit lines (±95% CI) shown for each ventilator]. Drug delivery tended to increase with the number of breaths. For all experiments, the Dräger delivered significantly more drug (p<0.0001).
Our choice of nebulizer was based on several factors, including our own experience and preference. Other devices may be suitable. However, differences in performance characteristics between devices and the lack of firm nebulizer standards require that studies be repeated with treprostinil for each brand of nebulizer.
In spontaneously breathing patients, the Tyvaso Inhalation System provides up to four doses per day from one ampule. Mechanical ventilation, however, with significant losses per breath during expiration limits the dose to one treatment per ampule, and treatment must be completed within 6 min (before the ampule runs out; Fig. 4).
Our measured particle distributions suggest that the AeroTech II produces smaller particles than the Tyvaso Inhalation System (MMAD reported at 2.0 μm).(15) It is uncertain if some of these differences are methodological, but it is possible that the patterns of deposition in the lungs might be different. Although scintigraphic data for treprostinil deposition in humans is not available, the particle distribution of treprostinil generated by the AeroTech II is within the range expected for lung deposition previously reported in intubated patients.(16)
We have not studied inhaled treprostinil in vivo in intubated patients. However, using a similar model, we have delivered antibiotics to intubated patients with measured clinical effects supporting our approach to therapy.(10,14,17) The present study builds on those studies by providing a formula that moves beyond supervised research by aerosol experts to a clinically relevant algorithm that provides some guidance to a clinician who may, by circumstance, need to administer Tyvaso to a mechanically ventilated patient. Our aim was to provide an innovative in vitro study to use as a model for possible further clinical trials.
Limitations
Conducting an in vitro study and using only one type of nebulizer may be viewed as a limitation. However, as previously stated, the purpose of this study is to provide a platform to guide clinical studies or to further in vitro studies. If a physician wishes to use a different nebulizer, it must be tested and the formulas corrected. To best assess the predictive value of our formula, we tested a wide range of ventilator settings, some of which are not commonly used in clinical practice. For example, in several of the trials, we used settings with tidal volumes of 1,200 mL and in others zero PEEP (ZEEP). The purpose of testing a wide range of settings was to test the limits of our predictions. ZEEP was used to assess the baseline response of the system, and then PEEP levels ranging from 0 to 10 cmH2O were used to confirm that the presence of PEEP did not affect drug delivery. Our clinical algorithm encompasses several factors that may change during aerosol therapy. In addition, the added flow to the system from the nebulizer will trigger high volume alarms. Therefore, we recommend direct observation during treatment by the respiratory therapist.
Footnotes
Acknowledgments
This study was funded in part by United Therapeutics as an investigator-initiated study. The authors thank Lorraine Morra for her assistance in performing the experiments and in the preparation of the manuscript.
Author Disclosure Statement
No conflicts of interest exist for R.P., G.C.S., and A.C. P.S. has received research funding from United Therapeutics for clinical trials.