
Abstract
Abstract
Background:
Improved inhalation device/drug combinations are necessary to advance inhaled antibiotic therapy in cystic fibrosis (CF). Previously, for a novel drug/inhaler combination, equivalent lung deposition was demonstrated; here, we investigated its safety and pharmacokinetics.
Methods:
In a randomized, open-labeled, multicenter, active controlled, parallel 28-day study, we compared a new tobramycin formulation (T100 PARI, 150 mg/1.5 mL) nebulized with a drug-specific PARI eFlow® nebulizer and TOBI® (300 mg/5 mL) nebulized with a PARI LC PLUS® nebulizer in 78 CF patients.
Results:
Noninferiority of the primary endpoint peak plasma tobramycin concentrations and the secondary endpoint area under the concentration time curves in plasma were observed. Sputum concentrations exceeded expected minimum inhibitory concentrations of Pseudomonas aeruginosa and were the same across both treatment groups, as were tolerability and safety. The nebulization time (4.6 vs. 16.1 min) was much shorter for the new drug/device combination.
Conclusion:
Inhaled therapy with T100 PARI delivered by an investigational eFlow offers a patient treatment time benefit and comparable safety and pharmacokinetics.
Introduction
I
Long nebulization times of up to 2×20 min per day are the major disadvantage of current inhaled tobramycin therapy. Significantly shorter inhalation times can be achieved using more efficient inhalation devices such as the eFlow® system in combination with more concentrated tobramycin and smaller liquid medication volumes. In a previous in vitro aerosol characterization study, we evaluated comparable respirable doses nebulizing tobramycin in the standard application (TOBI, 300 mg/5 mL, PARI LC PLUS powered by a PulmoAide® compressor) compared with a more concentrated tobramycin solution using a smaller volume in a customized drug-specific electronic PARI eFlow nebulizer, as used in previous clinical studies.(10) The new tobramycin formulation T100 PARI (150 mg/1.5 mL) nebulized with a drug-specific eFlow provided a respirable dose of 70.4±3.4 mg in comparison with 55.4±2.3 mg for the standard TOBI (300 mg/5 mL) nebulized with the PARI LC PLUS. The substantially higher drug delivery rate of 22.8 mg/min with the eFlow and T100 PARI versus 7.0 mg/min with the PARI LC PLUS and TOBI provided a significant reduction in mean nebulization time from 15 to 4 min, while increasing the respirable fraction (percent droplet mass below 5 μm) from 54.7% to 70.4%. Additionally, a deposition study using radioactively labeled tobramycin solutions demonstrated equivalent total lung deposition and distribution of TOBI (300 mg/5 mL) nebulized with the PARI LC PLUS [45.4 mg; 95% confidence interval (CI), 39.3–51.6] compared with the new formulation of T100 PARI (150 mg/1.5 mL) nebulized with the drug-specific PARI eFlow (46.0 mg; 95% CI, 40.3–51.7).(11)
The objectives of this study were to determine the pharmacokinetics of T100 PARI in patients with CF by assessing the tobramycin sputum concentrations and to provide safety information by investigating tobramycin peak plasma (Cmax) and area under the plasma concentration time curve (AUC). Lastly, tolerability of T100 PARI (150 mg/1.5 mL) nebulized with the optimized eFlow configuration was compared with that of the standard treatment regime using TOBI (300 mg/5 mL) delivered via a PARI LC PLUS nebulizer for 28 days, in order to detect any possible adverse reactions with more efficient inhalation of tobramycin.
Materials and Methods
Patient characteristics and study design
CF patients were eligible to participate in this study if they were able to perform spirometry with an FEV1 at least 40% of predicted in a stable clinical condition at least 1 month prior to screening and provided documented P. aeruginosa sputum or throat cultures within 6 months prior to screening or at least two consecutive positive P. aeruginosa cultures within the previous year. CF was diagnosed by sweat chloride levels greater than 60 mEq/L or carrying two disease-causing genetic mutations of the CF transmembrane conductance regulator.
After screening, the patients were randomized to two treatment groups: the T100 PARI/eFlow group and the TOBI/PARI LC PLUS group (Fig. 1). Randomization was based on randomization lists created in an automated fashion with the method of permuted blocks and a block size of four. Study medication was inhaled twice daily as add-on therapy to existing medications. Neither inhaled antibiotics other than the study medication nor other antipseudomonal antibiotics by any route were allowed within 7 days before and during the trial. Macrolide therapy initiated more than 6 weeks prior to study initiation was allowed.
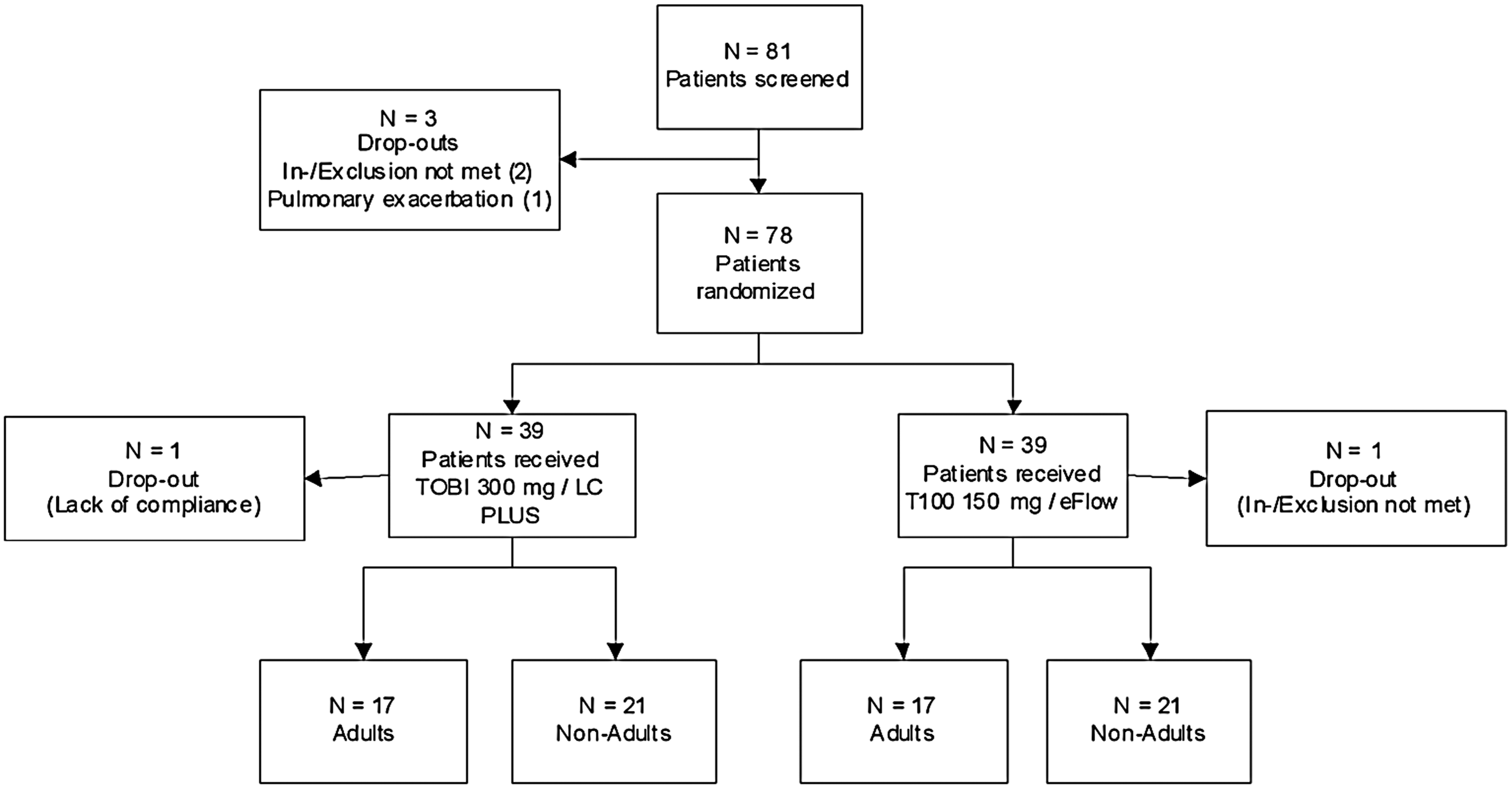
Distribution of patients to treatment groups. Screened: N=81; three screening failures not receiving medication. Randomized: N=78; intention to treat population; one patient (T100) excluded because did not meet in-/exclusion criteria and never received medication; one patient (TOBI) excluded due to lack of compliance. Analyzed: N=76; per protocol population.
The primary endpoint of the study was the tobramycin Cmax plasma level after 7 days of twice daily inhalation (steady state) to evaluate potential safety differences between the two treatment groups. The secondary endpoint was tobramycin plasma AUC after 7 days to further evaluate safety. The tobramycin levels in sputum were also measured to compare the potential efficacy of the tobramycin at the site of infection between the groups.
Procedure
After a 7-day washout phase, the patients were treated twice daily with their assigned medication and devices for 28 consecutive days. Blood and sputum samples were taken on days 1 (Visit 2), 7 (Visit 3), and 28 (Visit 4) (Fig. 2). Plasma sampled on Visits 2 and 4 was used to determine tobramycin trough levels. When receiving medication, the patients were trained in the study centers how to handle, clean, and correctly use the devices. At each visit, spirometry before inhalation and 30 min post inhalation was performed. At Visits 2, 3, and 4, tobramycin concentration was determined in sputum 10 min after inhalation. At Visit 3, tobramycin concentration was measured in plasma before and after inhalation as described below. Adverse events (AEs) were recorded at each visit; an audiology test was performed at each visit as well as a targeted physical examination. Visit 4 was the last treatment day and the end of the trial for those patients who completed the study as planned.

Study design. Green represents the screening period, blue the washout period, orange the treatment period, and yellow the safety follow-up period. V1–V4, Visit 1 to Visit 4. Color images available online at www.liebertpub.com/jamp
Determination of tobramycin concentration in plasma and sputum
At Visit 3, blood samples were taken 15–30 min before inhalation (trough level) and 0.5, 1, 1.5, 2, 3, 4, 6, and 8 hr after inhalation for pharmacokinetic (PK) analyses. At Visits 2 and 4, blood samples were taken 15–30 min before inhalation to determine tobramycin trough levels. Heparin plasma was stored below −18°C until final analysis. Sputum was sampled 10 min after the inhalation at Visits 2, 3, and 4 after the subject had rinsed the mouth carefully, and stored below −18°C until final analysis. Analysis of tobramycin concentration was done by reverse-phase HPLC-MS/MS after electrospray ionization. The method was validated in human plasma and human saliva and was calibrated for a range between 50 μg/L and 5,024 μg/L for plasma, and between 500 μg/L and 50,000 μg/L for saliva.
Lung function measurements
Lung function tests were standardized and performed according to the recommendations of the European Committee from Coal and Steel.(12)
Adverse events
Attention was given to bronchospasm (defined as a fall in FEV1 of more than 15% at 30 min after the end of inhalation), dyspnea, voice alteration, tinnitus, and deterioration of lung function (defined as a decline of FEV1 of more than 15% from pre- to posttreatment).
Statistical methods
The data are given as means±SD. The primary analysis was based on a noninferiority setting with the assumption that T100 PARI/eFlow does not differ from TOBI/PARI LC PLUS peak concentrations (Cmax) by more than 30%. The selection of the 30% range was chosen in acknowledgement of the EMA Guideline on the Investigation of Bioequivalence (CPMP/EWP/QWP/1401/98 Rev. 1/Corr**) considering that this guideline does apply for immediate-release formulations only. The local p values for the noninferiority hypotheses were based on one-sided t tests in applying the F test for the contrast of group differences obtained from the ANOVA model. The one-sided test was chosen to show noninferiority T100 PARI/eFlow versus TOBI/PARI LC PLUS. The corresponding 90% CI values are given, which correspond to a one-sided 5% significance test. All analyses were done by the statistical software package SAS version 9.1. The statistical model was fitted by the SAS procedure MIXED. Tolerability and safety endpoints were assessed by descriptive statistics.
Inhalation devices
For inhalation of TOBI, the PARI LC PLUS jet nebulizer was used, because this nebulizer was used for approval of TOBI. T100 PARI tobramycin solution was nebulized with a customized drug-specific eFlow nebulizer using vibrating membrane technology (PARI Pharma GmbH, Starnberg, Germany). The nebulizer was adjusted to produce droplets of optimal size and high delivery rate. The mean mass median aerodynamic diameter of the T100 PARI tobramycin solution nebulized with the drug-specific eFlow was 3.6 μm versus 4.5 μm with TOBI/PARI LC PLUS as determined by Anderson Cascade Impactor measurements. The drug delivery rate with T100 PARI/eFlow was three times higher than that with TOBI/PARI LC PLUS according to in vitro testing (PARI Pharma internal investigations).
Results
Patient demographics
Patients' mean age was 20.3±8.9 years (mean±SD). The non-adults were 13.7±2.8 years old, and the adults 28.1±7.1 years old. Age differences between the groups were in the±1 year range. Gender distribution of the groups was comparable, with 19 males in the T100 PARI/eFlow group (n=39) and 20 males in the TOBI/PARI LC PLUS group (n=39).
At Visit 1, no significant differences in lung function were detected between the two treatment groups. In the T100 PARI/eFlow group, the mean FEV1 percent predicted at Visit 1 was 73.5±18.8, and in the TOBI group it was 75.1±21.5.
Tobramycin plasma PK data and sputum levels
The primary analysis was based on a noninferiority setting with the assumption that peak concentrations Cmax do not differ by more than 30% in the T100 PARI/eFlow patients compared with the TOBI/PARI LC PLUS group. The analysis of the secondary endpoint plasma AUC was conducted in the same manner. The systemic mean Cmax levels as well as the mean AUC concentrations of the T100 PARI/eFlow group were lower than those in the TOBI/PARI LC PLUS group, and nebulization time was shorter, as shown in Table 1. However, despite the statistically significant difference regarding Cmax and AUC, the noninferiority level of ±30% was achieved for all age groups with the exception of adults, as can be seen from the overlapping CI values.
Data are given as means±90% CI. Statistical analysis was performed using ANOVA model, one-tailed t test.
Sputum tobramycin levels were numerically higher in the T100 PARI/eFlow group compared with the TOBI/PARI LC PLUS group. The same pattern appeared in the adult and non-adult subgroups (see Table 1). There were no significant differences between the groups, most probably due to the well-known high inter- and intrapatient sputum variability.
Tobramycin plasma trough levels
Trough levels at Visit 3 (day 7) were similar in the T100 PARI/eFlow group compared with the TOBI/PARI LC PLUS group [all patients (means±SD): 204.2±205.5 vs. 155.7±113.0 μg/L; p=0.897]. The same pattern was found in the adult and in the non-adult subgroups.
Trough levels at Visit 4 (day 28) were not different between the TOBI/PARI LC PLUS group compared with the T100 PARI/eFlow group (all patients: 177.2±236.2 vs. 149.1±143.7 μg/L; p=0.274). The same pattern was found in the adult and in the non-adult subgroups. Mean trough plasma levels were approximately one tenth of the recommended maximum aminoglycoside trough plasma level after oral application (less than 2 μg/mL) in each group.(6,13)
All PK analyses were performed in two age strata, i.e., non-adults and adults. There were no qualitative or clinically relevant differences between these age groups. Analyses of center effects indicated that the data were not influenced by specific centers.
Ratio of tobramycin plasma/sputum concentrations
Calculations of tobramycin concentrations in plasma and sputum on day 7 revealed ratios of 0.050% and 0.073% for the T100 PARI/eFlow and the TOBI/PARI LC PLUS groups, respectively, in the overall study population. Similar ratios were found in the age subgroups (see Table 1).
Adverse events
In this study, a total of 246 AEs were reported. Numerically, the incidence of experiencing AEs was lower in the T100 PARI/eFlow group than in the TOBI/PARI LC PLUS group (103 vs. 143; see Table 2), but it was not statistically significant. Across all events, 147 (59.8%) events were categorized as mild, 75 (30.5%) as moderate, and 24 (9.8%) as severe in intensity. Severe AEs were less frequent in the T100 PARI/eFlow group (7/103; 6.8%) compared with the TOBI/PARI LC PLUS group (17/143; 11.9%).
N, number of events.
Of the 246 AEs, 179 (72.8%) were considered unrelated to the study medication, whereas 67 (27.2%) were assumed related and thus qualified as adverse drug reactions. In the study group (T100 PARI/eFlow), 26 of 103 AEs (25.2%) were considered related to therapy; in the reference group (TOBI/PARI LC PLUS), these were 41/143 AEs (28.7%).
In the system-organ class “ear and labyrinth,” there were more AEs in the T100 PARI/eFlow group compared with the reference group (10 vs. 2). The difference was caused by cases of external ear pain (T100: n=2, not related; TOBI: n=0), impaired hearing (T100: n=4, 3 related; TOBI: n=0), and tinnitus (T100: n=3, not related; TOBI: n=1, not related).
All events resolved by the end of the study. There were considerably fewer respiratory disorders in the study group than in the reference group (60 vs. 110; i.e., −45%). This difference was mainly caused by more cases of cough (30 vs. 51), dysphonia (12 vs. 19), dyspnea (6 vs. 14), and increased bronchial secretion of partially increased viscosity (4 vs. 7; all for T100 vs. TOBI, respectively).
Overall, AEs were more frequent in the adult population, with 56–57% of patients reporting AEs between the visits compared with 29–45% in the non-adults.
Decline of FEV1
At Visit 2, the mean decline in FEV1 was 1.77±6.49% in the overall patient population when pre- and postinhalation values were compared. In the non-adults, the decline in the T100 PARI/eFlow group exceeded marginally the decline in the TOBI/PARI LC PLUS group (2.08±5.55 vs. 1.65±7.88%, p=0.846) and vice versa in the adult population (1.43±6.28 vs. 1.87±6.44%, p=0.873). Both differences were not statistically significant.
FEV1 changes from pre- to postinhalation were slightly smaller at Visit 3, with an average decline of 0.51±5.81% in the overall patient population. In both age groups, the decline was less in the T100 PARI/eFlow group. In the adult population, FEV1 showed an increase of 0.96±6.81% in the T100 PARI/eFlow group and a decline of 1.01±4.21% in the TOBI/PARI LC PLUS group.
At Visit 4, overall FEV1 changes were negligible (–0.10±5.42% overall), and differences between groups were not statistically significant. Generally, values obtained tended to improve in both groups between Visits 2 and 3 and remained stable through Visit 4.
Discussion
This PK study fulfilled its primary objective and confirmed that T100 PARI/eFlow did not increase systemic tobramycin exposure compared with the reference product TOBI/PARI LC PLUS. Overall, the PK data from this study are applicable to a general population with CF. They show that nebulization time was significantly reduced to approximately one third in the T100 PARI/eFlow group compared with the reference group (TOBI/PARI LC PLUS), whereas systemic exposure to tobramycin was not increased and sputum concentrations were maintained approximately identical. The systemic exposure finding was important with regards to safety, because aminoglycosides possess various systemic toxicities, the most important being irreversible ototoxicity, particularly in children.
The PK of inhaled tobramycin in CF patients is well characterized. In 2002, Geller et al.(6) published the results of a PK study performed with TOBI/PARI LC PLUS, which showed that the administration of tobramycin, 300 mg bid, in a 28-day off/28-day on regimen produced low plasma tobramycin concentrations, reducing the potential for systemic toxicity, but providing high sputum concentrations ensuring efficacious antibiotic drug concentrations at the site of infection. The results of PK analyses of our study confirmed the observations made by Geller et al.(6) A low ratio of serum to sputum tobramycin concentration, as reported, is the most important factor to enable therapeutic efficacy while respecting safety considerations, but is in contrast to the primary definition of bioequivalence for oral and systemic drug products according to current regulatory definitions (EMA Guideline on the Investigation of Bioequivalence, CPMP/EWP/QWP/1401/98 Rev. 1/Corr**). Usually equivalent blood plasma levels (Cmax, Tmax, and AUC) are required to prove bioequivalence. However, a bioequivalent therapeutic effect in the airways requires that the same drug dose will be administered and equally deposited and distributed to the target site, whereas the drug concentration in blood and plasma reflects a safety aspect. As aminoglycosides diffuse poorly across lipid membranes and into the bronchial secretions, and their distribution is restricted mainly to the extracellular fluid, high parenteral drug concentrations are required to exceed microbial breakpoints greater than approximately 16 μg/mL.(14) Using the inhalation route, a tobramycin sputum concentration of approximately 2.5 mg/g could be achieved, thus exceeding by approximately 150-fold the minimal inhibitory concentration (MIC) of tobramycin for P. aeruginosa. High targeted tobramycin sputum concentrations can be obtained upon inhalation, and this route of administration allows reduction of systemic tobramycin concentrations that potentially cause nephro- and ototoxic side effects, particularly in children.(15)
Overall, pulmonary delivery of 150 mg of tobramycin (loaded dose) nebulized with a drug-specific eFlow (T100 PARI/eFlow) was at least equivalent, if not superior, to the present standard regimen (TOBI/PARI LC PLUS). Specifically, for T100 PARI/eFlow, despite the lower tobramycin loaded dose (–50%) and substantially decreased nebulization time (approximately −70%), tobramycin sputum concentrations were similar to those of standard TOBI/PARI LC PLUS.
Of interest is the comparison of our PK data with those published by others for TOBI/PARI LC PLUS and Bramitob®/PARI LC PLUS (Table 3). Mean plasma tobramycin peak concentrations (Cmax) for TOBI/PARI LC PLUS based on plasma sampling were reported in the range of 0.95 μg/mL in the study by Geller et al.,(6) 1.3 μg/mL by Hubert et al.,(16) and 1.65 μg/mL for TOBI/PARI LC PLUS in this study, whereas Cmax for Bramitob was only 0.68 μg/mL. It should be noted that these data for TOBI as well as for Bramitob must be considered with caution, because only a single-point plasma measurement was performed 1 hr post inhalation, and Cmax was not determined from PK curves as in this study (Table 3). The variability of other PK studies performed with tobramycin and different nebulizer systems is also of interest for the interpretation of the results in this PK study. In the study by Newhouse et al.,(17) healthy volunteers inhaled radiolabeled TOBI (300 mg/5 mL) via a PARI LC PLUS. The AUC was 2.1 μg·hr/mL and Cmax was 0.28 μg/mL, which may be consistent with the low lung deposition rate (5%). In comparison, Touw et al. reported Cmax values of 1.2 μg/mL in CF patients after inhalation of 600 mg of tobramycin nebulized via a WISO SENIOR ultrasonic nebulizer.(18)
BLQ, below limit of quantification; CI, 90% confidence interval; n, number of included patients; ND, not determined; SD, standard deviation.
Brand name and mL/fill volume.
Mean values, single time point measure of tobramycin plasma levels 1 hr after inhalation.
Mean values, single time point measure of tobramycin sputum levels 10 min after inhalation.
Minimum – maximum.
Standard deviation.
90% confidence interval.
The TOBI/PARI LC PLUS mean sputum level of 2,272 μg/g in our study was higher than those found by other investigators. Geller et al.(6) reported 1,237 μg/g and Eisenberg et al.(19) 687 μg/g for TOBI (300 mg/5 mL) nebulized by the PARI LC PLUS, which was similar to the observed sputum concentration of 695 μg/g for Bramitob/PARI LC PLUS published by Lenoir et al.(20) (Table 3). Sputum concentration was 769 μg/g for the PARI LC PLUS in the study of Hubert et al.,(16) but 1,572 μg/g for the eFlow rapid. Mean sputum concentrations in our study were on average higher for both TOBI/PARI LC PLUS and T100 PARI delivered via a drug-specific eFlow nebulizer (2,272 and 2,598 μg/g, respectively). In general, there is a very high variability of tobramycin concentration in sputum, and this is most likely the result of different recoveries from sputum samples, variable inhalation and deposition patterns, variability of airway obstruction and anatomy with age and disease, mucus plugging, as well as individual sputum production. In addition, a direct comparison of PK data from different studies may lead to erratic conclusions due to different study designs, methods, and intervals of sampling, including analytical methodology. The high variability aspects as outlined above for tobramycin sputum levels also apply to plasma serum levels. Hence, bioequivalence criteria derived from oral drug products defining an interval of, e.g., ±30% of the mean median values as bioequivalent are hardly applicable for inhaled drugs, particularly in CF patients. So far, the ongoing discussions on bioequivalence criteria for inhaled products are focusing on inhaled steroids, β-agonist, and anticholinergic drugs in patients suffering from “stable” asthma and chronic obstructive pulmonary disease (COPD). However, it must be considered in this context that the health status of CF patients is much more variable, and common bioequivalence criteria of PK studies therefore are hardly applicable. Regardless, the new concentrated tobramycin formulation T100 PARI administered by the drug-specific eFlow nebulizer generated tobramycin sputum concentrations of approximately 150-fold the MIC of P. aeruginosa. Due to tobramycin's low influx potential, only 0.050% of the antibiotic drug was detected in the blood circulation of the patients, making the new drug/device combination an attractive alternative to systemic administrations known to bear a higher risk for undesired ototoxic and nephrotoxic side effects.
In conclusion, noninferiority based on a maximum 30% difference for Cmax and AUC could be observed at day 7 for T100 PARI/eFlow compared with TOBI/PARI LC PLUS and in all age groups with the exception of adults. Maximum tobramycin plasma concentrations of both treatment arms were well below accepted safety thresholds for systemic tobramycin application.(6,13) Sputum concentrations of tobramycin greatly exceeded expected minimum inhibitory concentrations of P. aeruginosa and were similar across both treatment groups. Data from this study were supported by an equivalent lung deposition of 46.0 versus 45.4 mg for both groups assessed previously.(11) Inhaled therapy with T100 PARI/eFlow offers a patient benefit due to much shorter nebulization time (mean 4.6 vs. 16.1 min) with a similar rate of side effects, a comparable safety profile, and an equivalent lung deposition. This may contribute to improved drug adherence of CF patients and, finally, therapeutic efficacy.
Footnotes
Acknowledgments
The medical devices (eFlow, PARI LC PLUS), the investigational medicinal product (T100 PARI), and the reference product (TOBI) were provided by PARI Pharma GmbH (Starnberg, Germany). In addition, the company granted financial support for all analyses. Inamed GmbH (Gauting, Germany) was the clinical research organization (CRO) of this study, and the support of A. Ameal-Godoy and T. Hunger is acknowledged.
M.G. received honoraria for presentations sponsored by Novartis, Germany, Vertex, Germany, and PARI Pharma GmbH, Germany; he also received grants from the Mukoviszidose e.V. Germany and the North American Cystic Fibrosis Foundation for other studies in CF patients. M.K. received honoraria for presentations sponsored by Novartis, Germany and Forest, Germany. H.M. received honoraria for presentations sponsored by Chiesi Farmaceutici, SpA, Italy; he also has been Principal Investigator or Coordinating Investigator in the clinical trials sponsored by Chiesi Farmaceutici, SpA, Italy or PARI Pharma GmbH. The identification number of this study is EudraCT 2005-004103-10.
Author Disclosure Statement
M.G., C.E., H.M., and M.K. declare that no conflict of interest exists. G.B. is an employee of PARI Pharma GmbH (Graefelfing, Germany). O.D. is an employee of PARI Pharma. J.S. was formerly director of clinical development of PARI Pharma. He has no conflict of interest and is an independent consultant of Phaidon Healthcare GmbH (Munich, Germany). M.Ke. was formerly chief scientific officer of PARI Pharma and has no conflict of interest. He is now an independent consultant of Keller Pharmaconsult (Munich, Germany).
Study Centers
The following list shows the study centers where this work was conducted, along with the names of the lead researchers:
• Matthias Griese, Dr. von Haunersches Kinderspital, Ludwig Maximilians University, Munich, Germany • Albrecht Tacke, Helios Kinderklinik Berlin-Buch, Germany • Joachim Günther Bargon, St. Elizabethen Krankenhaus-Frankfurt, Germany • Rainald Fischer, Klinik der Innenstadt LMU-Munich, Germany • Helmut Teschler, Klinik Essen-Heidhausen, Germany • Manfred Ballmann, Kinderklinik Hannover, Germany • Lutz Nährlich, Kinderklinik Erlangen, Germany • Frank-Michael Müller, Kinderklinik Uni Heidelberg, Germany • Halina Batura-Gabryel, Clinic of Physiopneumology Medical Academy, Poland • Maria Trawinska-Bartnicka, Children's Hospital - Specialist Healthcare Unit on Mother and Child, Gdansk, Poland • Andrzei Milanowski, Institute of Mother and Child, Centre of Diagnostics and CF Treatment, Warszawa, Poland • Henryk Mazurek, Clinic of Bronchology and CF, Institute of Tuberculosis and Lungs Diseases, Rabka, Poland • Felix Ratjen, Hospital of Sick Children, Toronto, Canada • Elisabeth Trullis, St. Michael's Hospital, Toronto, Canada