
Abstract
Abstract
Background:
Early studies have found better clinical efficiency when a nebulizer was used with noninvasive positive pressure ventilation (NPPV), compared with spontaneous breathing without NPPV. However, very limited research addressed factors that might affect aerosol delivery. This study aimed to investigate the influence of exhalation valves and nebulizer positions on aerosol delivery during NPPV.
Methods:
We determined the efficiency of aerosol delivery in patients receiving NPPV with a lung model that simulates spontaneous breathing. Single-arch exhalation port, plateau exhalation valve, and whisper swivel were chosen as exhalation valves under different levels of inspiratory and expiratory pressures. A nebulizer was filled with 1 mL of 0.5% albuterol solution in 3 mL of normal saline, driven with 8 L/min oxygen, and placed at either a proximal position in the ventilator circuit (near the ventilator outlet, where humidifiers are usually connected) or a distal position in the ventilator circuit (between exhalation valve and lung model connection). Albuterol was collected by filters and then measured by ultraviolet spectrophotometry. The velocities of gas flow were also measured at different nebulizer positions.
Results:
Significant differences in the gas flow velocity were shown between proximal and distal positions of the breathing circuit under four combinations of inspiratory and expiratory pressure levels (15/5, 15/10, 25/5, and 25/10 cmH2O) (p<0.05). When the nebulizer was positioned distally, the single-arch exhalation port had the highest aerosol delivery, and the whisper swivel had the lowest aerosol delivery (p<0.05). When the nebulizer was placed proximally, the single-arch exhalation port had lower efficiency of aerosol delivery than the whisper swivel and plateau exhalation valve (p<0.05). In addition, higher inspiratory pressure was associated with increased aerosol delivery (p<0.05). The influence of expiratory pressure on aerosol delivery appeared too complex to predict.
Conclusions:
The type of exhalation valve and the position of the nebulizer in the ventilator circuit have a significant influence on the efficiency of aerosol delivery during NPPV. As a result, with different exhalation valves, an appropriate nebulizer position should be carefully chosen, and the inhaled dose should be adjusted after accurate prediction of aerosol delivery to ensure optimal clinical efficacy.
Introduction
C
Unfortunately, many factors can compromise aerosol delivery during NPPV and eventually decrease the clinical curative effect,(9,10) and very few studies so far have addressed these possible influencing factors. In particular, the single-limb breathing circuit of ventilators designed for NPPV requires selective use of specific exhalation valves. Different types of the valve were shown to be associated with varied amounts of air leakage for which the ventilator compensates accordingly.(11) Therefore, use of different types of exhalation valves will give rise to variable airflow rates in the ventilator circuit proximal and distal to the exhalation valves, with the potential to influence aerosol delivery. However, no study has been conducted in relation to the influence of exhalation valves and nebulizer positions on aerosol delivery during NPPV. In the present experiment, we simulated the aerosol therapy with NPPV in vitro in order to explore such influences. Our hypothesis was that aerosol delivery during NPPV is affected by the types of exhalation valve and nebulizer positions; thus, with different exhalation valves, a suitable nebulizer position should be taken into consideration to achieve better aerosol delivery.
Materials and Methods
Lung model simulating spontaneous breathing
As shown in Figure 1, a ventilator (PB840; Puritan Bennett, Overland, KS) was connected to a chamber (as a drive chamber) of the Michigan dual-chamber lung (Adult TTL 1600; MI Instruments, Grand Rapids, MI). A noninvasive ventilator (synchrony; Respironics, Murrysville, PA) was connected to the other chamber used as a test chamber through a 180-cm breathing circuit (312107; Respironics) without humidifier. Rhythmical changes in the driver chamber volume that simulated spontaneous breathing were transduced to the test chamber through a tight junction metal rod. The drive chamber was used to trigger the noninvasive ventilator during early inspiration. Compliance of the dual-chamber Michigan lung was set to 0.05 L/cmH2O, and resistance to the lung model was set with a parabolic airway resistor (5 cmH2O L–1 sec–1, Pneuflo resistor Rp5; MI Instruments) with a resistance of 4.3 cmH2O L–1 sec–1 at a flow rate of 60 L/min.
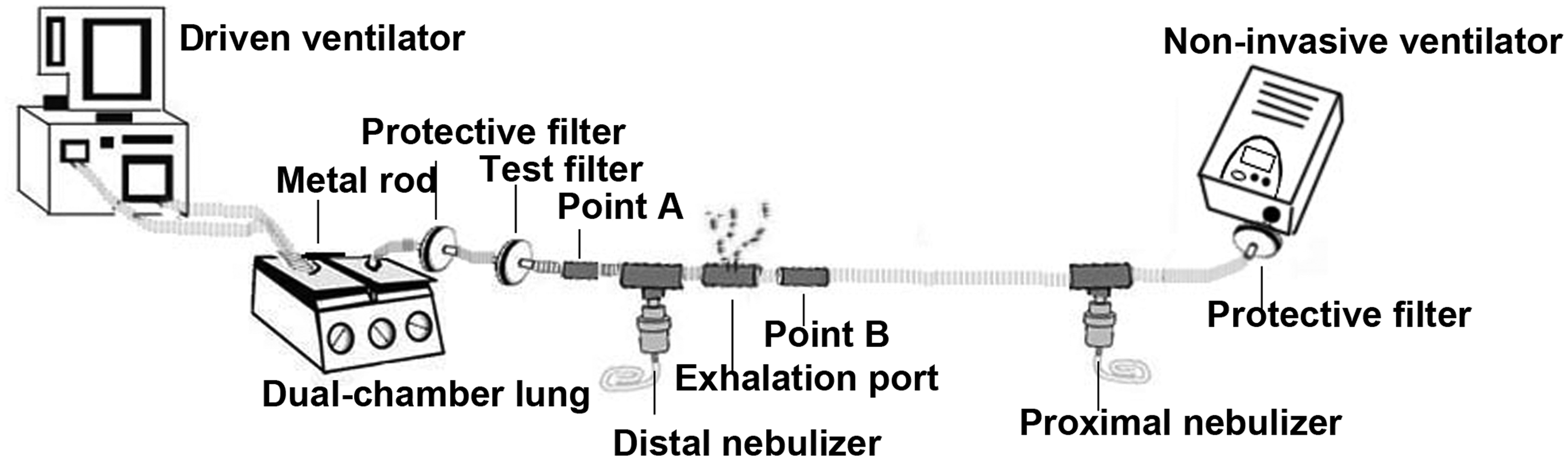
Schematic diagram of experimental procedures.
Experimental settings
The PB840 ventilator was set in the volume control mode (tidal volume, 500 mL; peak flow rate, 50 L/min; waveform, square-wave; respiratory rate, 20 beats/min), whereas the noninvasive ventilator was set in the spontaneous breathing mode with a pressure rising slope of 3. For all experiments, the positive end-expiratory pressure (PEEP) level of the PB840 ventilator was maintained equal to the expiratory pressure of noninvasive ventilator to ensure simultaneous triggering. The experimental settings varied in the following aspects: (1) The inspiratory pressure and expiratory pressure were 15/5, 25/5, 15/10, and 25/10 cmH2O, respectively. (2) The tested exhalation valves included single-arch exhalation port (Respironics), plateau exhalation valve (Respironics), and whisper swivel (Respironics), as shown in Figure 2. (3) The nebulizer positions were proximal (near the ventilator outlet, where humidifiers are usually connected) or distal (between exhalation valve and lung model connection). The distances between the nebulizer and test filter were 15 cm and 195 cm for distal and proximal positions, respectively. In the proximal position, the nebulizer was placed at a distance of 25 cm from the ventilator outlet.
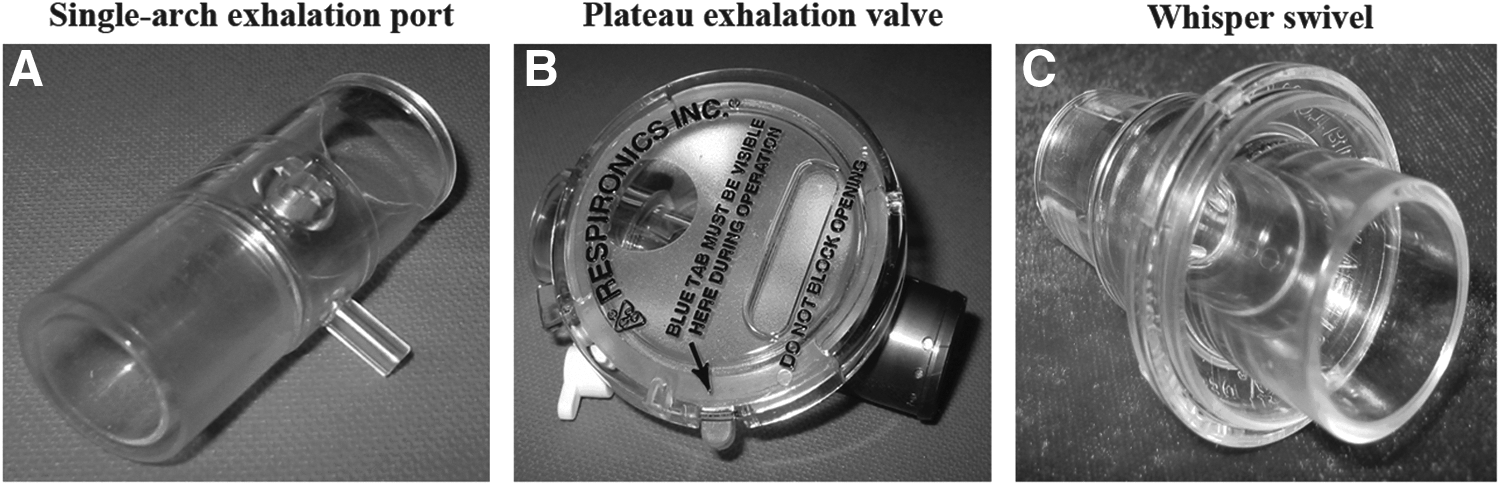
Images of the exhalation ports used.
A 1-mL solution of 0.5% albuterol was diluted with 3 mL of normal saline in a small-volume jet nebulizer (SVN; 1884; Teleflex, Mexico). The nebulizer was driven with oxygen from a wall outlet (50 psi) by using a flow meter (The Pacific Medical, Taiwan) at 8 L/min. The experiment was repeated five times under each experimental setting, and the SVN was disposed after a single use. The aerosol particles were collected by a disposable filter (REF19212; Teleflex Medical, Malaysia) placed at the entrance of the lung model. The nebulizer was maintained in the vertical position, and aerosol was delivered without tapping the nebulizer. Nebulization time was monitored by using a stopwatch, and was defined as the time from the start of nebulization to the beginning of the inconsistent aerosol output.
Aerosol measurement
Following each nebulization, 10 mL of normal saline was used to wash the aerosol collected on the filter. The filter was shaken by using a vortex oscillator (XW-80A; West Shanghai, China) for 1 min to ensure that the aerosol mixed well with the normal saline. Subsequently, the light absorption of the washout solution was measured with a spectrophotometer DU Series 500 (Beckman Instruments, Fullerton, CA) by using a 1-mL quartz cuvette at a wavelength of 276 nm. The amount of albuterol captured on the filter was calculated from the absorption–concentration standard curve generated by plotting light absorption as a function of albuterol concentration. There was a linear relationship between absorption and concentration of albuterol between 0 and 0.1 mg/mL, with a slope of 0.1426 (r2=0.99).
Two filters were placed in series to test the filter's ability to trap aerosol, and albuterol could be completely collected in the first filter, but no albuterol was detected on the second filter. The specificity of our analytic technique was tested by nebulization of saline, with which we found zero light absorption. We also rinsed filters capturing a known amount of albuterol in normal saline for different durations, and found that all albuterol was detected when the filter was shaken in normal saline for 1 min.
Breathing circuit pressure and flow rate measurement
The gas flow analyzer (VT PLUS; Fluke Biomedical, Everett, WA) is an instrument with special modes designed for testing ventilators. When connected in series to different positions of the breathing circuit, the monitor of this analyzer will display the gas pressure and flow at any given position.
The analyzer was connected in series to the breathing circuit at position B to the exhalation valve (see Fig. 1). The connection distal to the exhalation valve was completely occluded and not connected to the test chamber. The noninvasive ventilator was set for continuous positive airway pressures (CPAP) of 5, 10, 15, and 20 cmH2O. The air leakage with each type of exhalation valve was measured at different pressure levels. With this analyzer connected to point A and then to point B, the airflow in the breathing circuit at the near end and far end of different exhalation valves was measured, respectively, under four combinations of inspiratory and expiratory pressure levels (15/5, 25/5, 15/10, and 25/10 cmH2O). We also recorded the peak inspiratory flow rate, peak expiratory flow rate, basic flow rate, inspiratory pressure, and expiratory pressure in five breathing cycles, and meanwhile observed the occurrence of autotriggering or missed triggers.
Statistical analysis
The amount of delivered albuterol was expressed in relative terms and as a percentage of the nominal dose, defined as the loaded dose of albuterol (5 mg) in the nebulizer cup. Measurement data were expressed as means±standard deviation. Multiway analysis of variance was applied to compare the influences of different factors (types of exhalation valve, inspiratory pressure, expiratory pressure, and nebulizer position) on aerosol delivery. The least significant differences method was used for post hoc comparisons when the main effects were significant. The paired t test was used for the comparison of the airflows at the near end and far end of the exhalation valve (points A and B) in the breathing circuit. All statistical analysis was performed using commercially available software (SPSS version 13.0; SPSS, Chicago, IL). Statistical significance was set at p<0.05.
Results
The amounts of air leakage with different types of exhalation valve are shown in Figure 3. Owing to its unique design, the plateau exhalation valve presented with an apparently constant amount of air leakage at different pressure levels (24.01±0.68 L/min). In contrast, the amount of air leakage with the single-arch exhalation port increased from 13.85±0.32 L/min to 28.93±0.57 L/min as the pressure increased from 5 cmH2O to 20 cmH2O; these changes in air leakage were greatest for the whisper swivel, increasing from 20.26±0.41 L/min to 45.63±0.71 L/min. At point A, there were no significant differences in the airflow magnitude between the different types of exhalation valve at the same pressure level (p>0.05). However, at point B and at the same pressure level, the whisper swivel and the plateau exhalation valve were associated with significantly higher flow rates, including peak inspiratory/expiratory flow rate and base flow rate, compared with the single-arch exhalation port (Table 1).
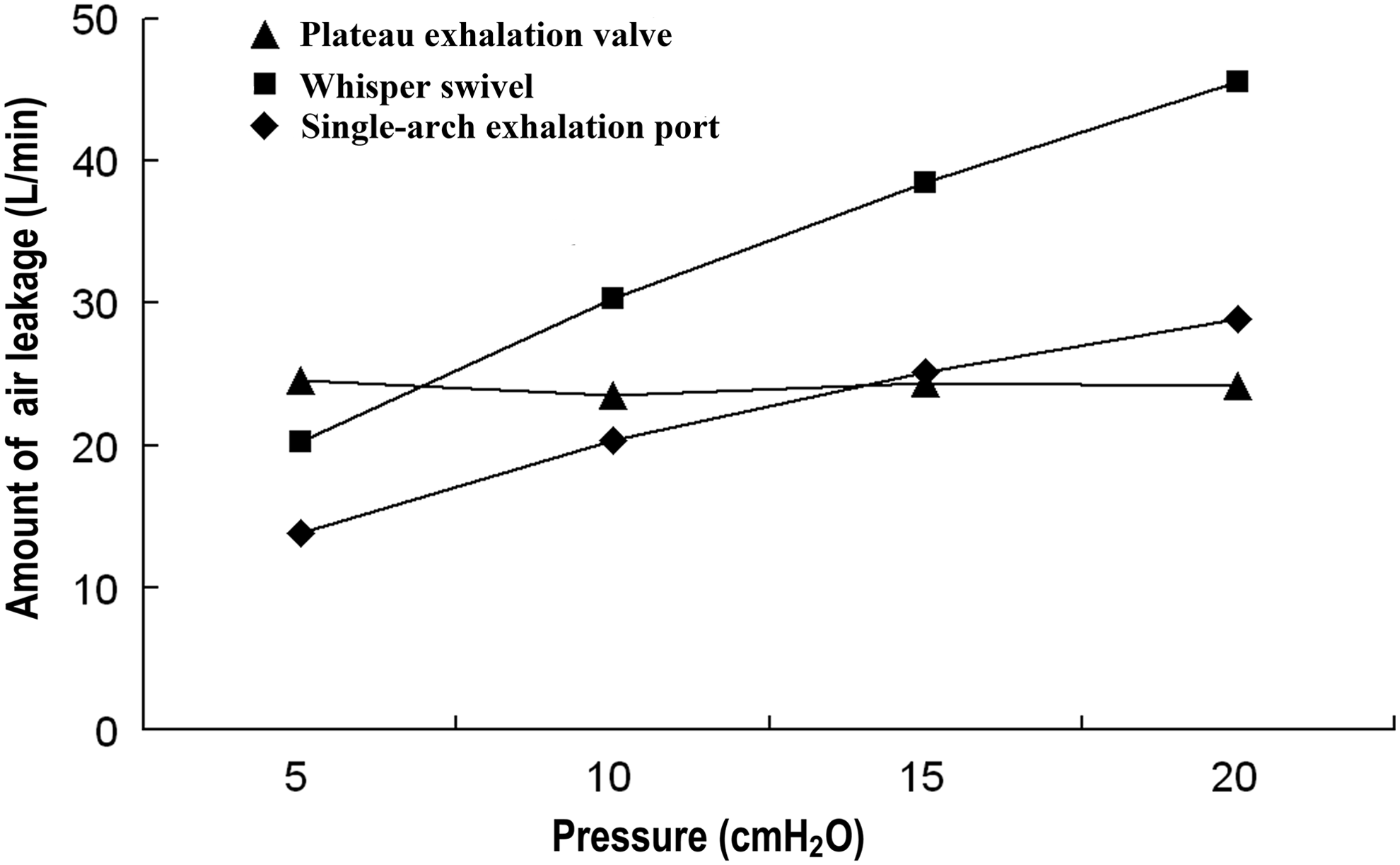
Amounts of air leakage with different exhalation valves.
PEF, peak expiratory flow; PIF, peak inspiratory flow.
The mean nebulization time was 9.7±1.1 min. The use of a nebulizer was found to have minimal impacts on the function of the noninvasive ventilator, as reflected by the proximity between the preset and measured inspiratory pressures at point A (25.00 vs. 25.14±0.51 cmH2O, 15.00 vs. 15.21±0.34 cmH2O) and between those of expiratory pressures at point B (5.00 vs. 5.14±0.37 cmH2O, and 10.00 vs. 10.11±0.43 cmH2O), respectively. Autotriggering or missed triggers were not observed.
The mean aerosol delivery varied from 15.99±0.54% to 28.22±1.59% of the nominal albuterol dose. Types of exhalation valves, inspiratory pressures, expiratory pressures, and nebulizer positions showed significant effects (all p<0.01) on aerosol delivery (Table 2).
Under a variety of pressure levels, different types of exhalation valve were associated with a significant difference between aerosol delivery at the distal position and at the proximal position. In the presence of the single-arch exhalation port (Fig. 4A), aerosol delivery at the distal position was greater than that at the proximal position with the expiratory pressure set at 5 cmH2O (p<0.05), but the opposite was true with the expiratory pressure set at 10 cmH2O (p<0.05). In the presence of the plateau exhalation valve or the whisper swivel (Fig. 4B and C), aerosol delivery at the proximal position was greater than at the distal position under all four combinations of pressure levels (15/5, 25/5, 15/10, and 25/10 cmH2O) (all p<0.05).
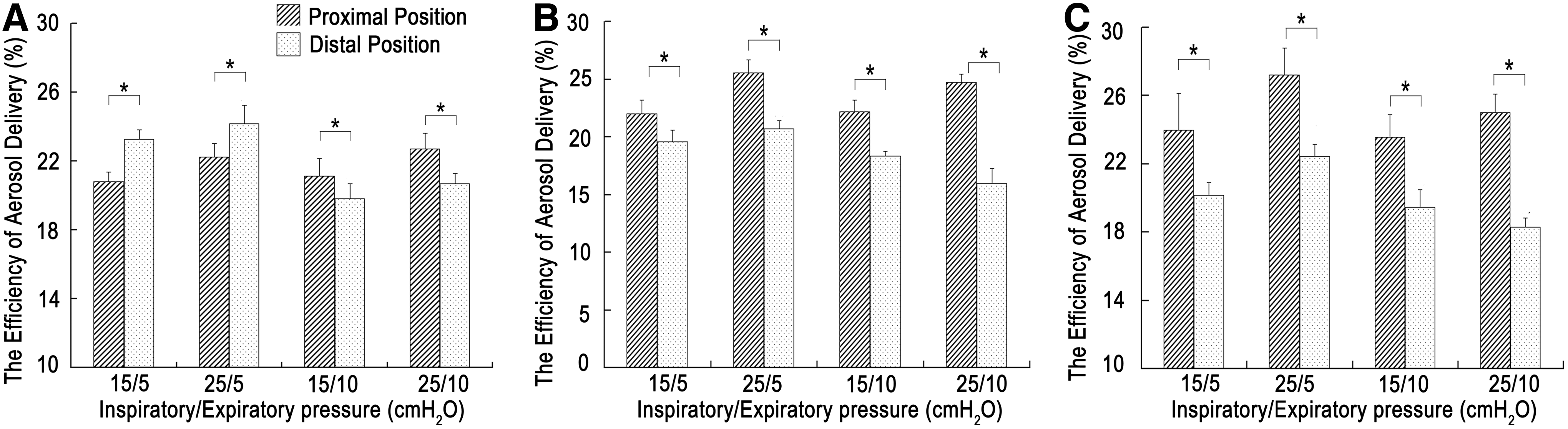
Efficiency of aerosol delivery with different exhalation valves at different nebulization positions:
At the distal position, the single-arch exhalation port had the highest aerosol delivery under all inspiratory/expiratory pressures (Fig. 5A), followed by the plateau exhalation valve and the whisper swivel (p<0.05). The aerosol delivery increased with higher inspiratory pressure (p<0.05), but was inversely correlated with the expiratory pressure (p<0.05). These trends were observed with all three exhalation valves. At the proximal position (Fig. 5B), the plateau exhalation valve had the highest aerosol delivery, followed by the whisper swivel and the single-arch exhalation port except at the pressure level of 25/10 cmH2O (p<0.05). The aerosol delivery with the plateau exhalation valve was significantly greater than that with the whisper swivel except at the pressure level of 25/10 cmH2O (p<0.05). Whereas higher inspiratory pressure was associated with increased aerosol delivery (p<0.05), the influences of expiratory pressure on aerosol delivery were too complex to predict.
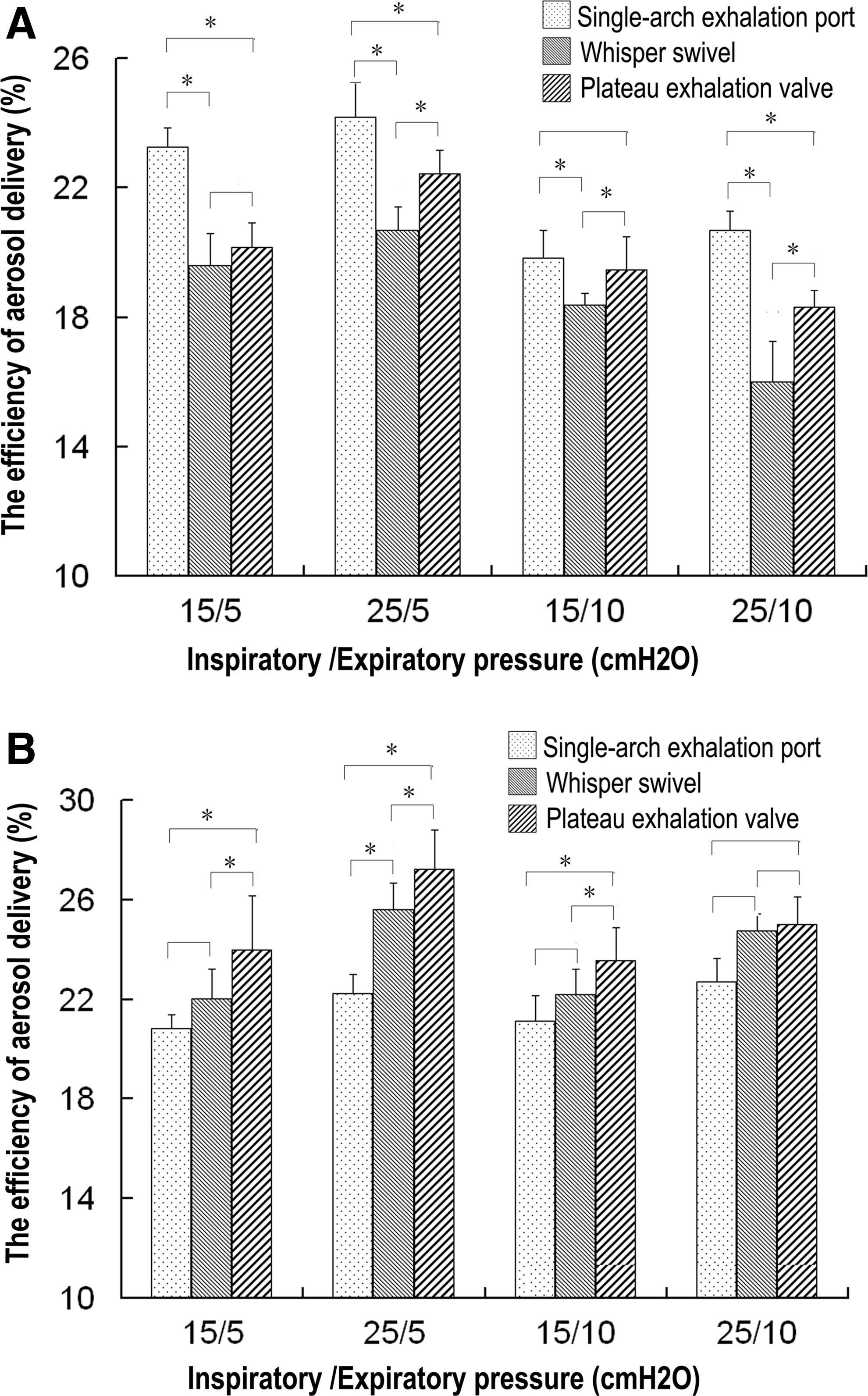
Efficiency of aerosol delivery at different nebulizer positions with different exhalation valves:
Discussion
Early studies demonstrated that lung deposition of aerosols was 10% in patients receiving conventional nebulization, but only 1% to 3% in patients receiving nebulization while on invasive mechanical ventilation.(12) CPAP has also been shown to significantly reduce the total aerosol delivery to the face mask from 1.52% to 0.37% of the initial nebulizer charge.(13) Therefore, it was acceptably a common practice to suspend ventilation when aerosol inhalation of bronchodilators was to be given to patients on NPPV. Further understanding of the factors influencing aerosol delivery and advances in nebulization techniques have led to increased lung deposition of aerosols.(14) A group of recent studies in vitro or in vivo have found better aerosol delivery, aerosol deposition in the lungs, and clinical efficiency with inhalation therapy when the nebulizer was used with NPPV ongoing but not interrupted.(5–8,15) In addition, the relatively widespread use of NPPV in patients at a critical stage of their condition, particularly in those with hypoxemia or acute dyspnea, suggests the preferable option to continue rather than suspend NPPV when inhaled bronchodilators are being given. Research into the factors influencing aerosol delivery during NPPV should considerably improve therapeutic efficacy and patient outcome.
So far, studies on the factors influencing aerosol delivery during invasive mechanical ventilation have found that ventilation mode, tidal volume, respiratory rate, inspiratory waveform, humidification, position, and type of nebulizer device may affect aerosol delivery.(16) Currently, ventilators specially designed for NPPV have become the first choice for noninvasive mechanical ventilation, although critical care ventilators were used in most of the early studies of NPPV. Owing to the unique characteristics of NPPV therapy, the factors influencing aerosol delivery revealed in invasive ventilation might not apply or can be even more complex in noninvasive ventilation. A noninvasive ventilator has a single-limb circuit connecting the ventilator to the face mask. An air leak is incorporated in the circuit or the mask to allow exhaled gases to escape, while the ventilator will compensate for the corresponding air leakage in case of intentional air leakage. The present study found that, for any exhalation valve, the larger the amount of air leakage, the higher the compensation flow rate of the ventilator, as well as the flow rate at point B in the corresponding breathing circuit. However, because point A of the breathing circuit was distal to the exhalation valve, the magnitude of airflow was related only to the preset parameters, such as inspiratory pressure, expiratory pressure, airway resistance, and compliance of the lung model, but not to the amount of air leakage of the exhalation valve. Therefore, the position of a nebulizer (proximal or distal to the exhalation valve) may give rise to a significant difference in aerosol delivery.
With a distally positioned nebulizer (equivalent to point A), aerosols are driven to the patient directly by the inspiratory pressure during the inspiratory phase. More aerosols would be delivered with higher inspiratory pressure and longer inspiratory time. In the early expiratory phase, as most of the aerosol-containing exhaled gas will be discharged from the exhalation valve, the larger the amount of air leakage from the exhalation valve, the greater the aerosol loss. When the flow rate of the exhaled gas is greater than the amount of air leakage from the exhalation valve, part of the gas containing aerosols would flow back to the near end. The rate of backflow is associated with the inspiratory and expiratory pressures. Given a higher inspiratory pressure and a lower expiratory pressure, the corresponding tidal volume would be higher, resulting in more backflow as well as more storage of aerosols in the breathing circuit for delivery during the next breath. In the late expiratory phase, due to the expiratory pressure, continuous airflows will move to the far end and be discharged from the exhalation valve. Meanwhile, higher expiratory pressure causes more air leakage from the exhalation valve and more discharge of aerosols previously stored in the breathing circuit. As such, aerosol delivery with a distally positioned nebulizer would be highest when the single-arch exhalation port is used, followed in order by the plateau exhalation valve and the whisper swivel. For any given exhalation valve, aerosol delivery would be higher with higher inspiratory pressure and lower expiratory pressure.
With a proximally positioned nebulizer (equivalent to point B), varied amounts of air leakage from different types of exhalation valve may result in changing airflows at point B even under the same pressure, and thereby more complex factors could interfere with the efficiency of aerosol delivery. In contrast to the plateau exhalation valve, which was associated with a relatively constant amount of air leakage at different pressure levels owing to its special design, the amount of air leakage for other types of valve was highest at low pressure level (almost <7 cmH2O). During NPPV, the breathing circuit was at a relatively low pressure level for most of time, because (1) the inspiratory time was usually shorter than the expiratory time, (2) it takes time for pressure to rise, and (3) a high-pressure level usually lasts for a shorter duration than the low pressure level. Therefore, in general, the actual total amount of air leakage may be largest with the plateau exhalation valve, followed by the whisper swivel and then the single-arch exhalation port. Consistent with this logic, the larger the amount of air leakage, the more aerosol-containing air discharged from the exhalation valve during the inspiratory and expiratory phases, and hence, in theory, a greater decline in aerosol delivery. Surprisingly, our study found that the measured aerosol delivery was highest with the plateau exhalation valve, followed by the whisper swivel and then the single-arch exhalation port. These findings should probably be explained by the much greater amount of aerosols propelled to the patient end (Fig. 1) at a higher airflow rate at point B, along with the increased air leakage, especially at the start of the inspiratory phase.
Currently, four types of exhalation valve are available for use in clinical practice, including the single-arch exhalation port, the plateau exhalation valve, the whisper swivel, and the mask valve (leak port incorporated in the mask). In a previous study, the efficiency of aerosol delivery during NPPV using a mask valve was noted to fall by 50%.(17) Although this type of exhalation valve was not investigated in our experiment, we speculated that a mask valve could have rendered the least aerosol delivery. This study has found that different types of exhalation valve have a significant impact on aerosol delivery. The purpose of this study, however, was not to provide data for the clinical selection of exhalation valves. By contrast, we think that exhalation valves should be chosen mainly according to rebreathing, costs, and clinical availability. For example, the plateau exhalation valve can minimize rebreathing and be preferred for patients with hypercapnia, but be used for several times at the expense of costs.(18) The single-arch exhalation port is popularly used because of its availability and that it is usually integrated in the disposable breathing, but at the expense of noise and rebreathing. The whisper swivel has a wider application, especially in patients with domiciliary NPPV who do not have to purchase an extra exhalation valve, and the advantage of silence.
The present study found that when the single-arch exhalation port was applied and the expiratory pressure was set to 5 cmH2O, aerosol delivery at the proximal position was lower than at the distal position; when the plateau exhalation valve and the whisper swivel were applied, aerosol delivery at the proximal position was greater than at the distal position under all pressures. Thus, with different exhalation valves, a suitable nebulizer position should be taken into consideration to achieve the best aerosol delivery. A proper exhalation valve and a proper pressure level should be determined according to the specific conditions of a given patient. Different exhalation valves should be used with different nebulizer positioning. These findings are very practical in the clinic to optimize aerosol delivery during NPPV.
Although optimal humidification of the inhaled gas could improve patient comfort, and facilitate successful application of NPPV, it should be acceptable to suspend humidification during nebulization for several minutes.(19) Most noninvasive ventilators designed for NPPV, like the one in our study, deliver ambient air whose humidity depends on ambient temperature and humidity. Furthermore, the inspired air is also humidified during its passage through the nose, unlike that in invasive mechanical ventilation. In view of previous findings that drug deposition in the lower respiratory tract from nebulizers was reduced by 40% or more in a humidified compared with a dry circuit,(20) we did not use a humidifier in our study. Another major reason for not using a humidifier was that the proximal nebulizer position in our study was the humidifier position near the ventilator outlet, but not the “real” proximal nebulizer position (ventilator outlet) in previous studies. We believed that a certain, considerable amount of aerosols being stored within the breathing circuit at the near end and far end of the nebulizer may act like a nebulization spacer and may increase aerosol delivery; in addition, the reflux of more aerosols to the internal space of the ventilator would be avoided when the “new” proximal nebulizer position was used. Calvert et al. reported better aerosol delivery with a nebulizer placed between the leak port and ventilator than one placed between the leak port and face mask,(21) which was opposite to the findings of Abdelrahim and colleagues.(22) One most probable cause is that Calvert placed the nebulizer at a longer distance away from the leak port than Abdelrahim, and this maneuver could have reduced aerosol loss during exhalation. To attain possible higher aerosol delivery, we chose a new nebulizer position (where a humidifier would be connected) at a longer distance away from the leak port than the position used by Calvert.
This in vitro study has several limitations. A complete breathing circuit for NPPV should also include the interfaces, such as nasal masks, full-face or oronasal masks, and mouthpieces; however, we did not address the effect of interfaces on aerosol delivery in this study. Despite no significant difference regarding the bronchodilator effects between patients using masks and mouthpieces in classical nebulization (without simultaneous NPPV),(23) we hypothesized that the dead space of interfaces during NPPV might affect the aerosol delivery. In addition, the clinical efficacy of aerosol inhalation is based on the lung deposition of aerosols, which is largely affected by aerosol delivery and the diameter of aerosol particles. Recent studies on invasive mechanical ventilation found that the faster the airflow, the larger the aerosol particles, and hence more deposition in the breathing circuit and less deposition in the lungs.(24,25) Thus, we also hypothesized that exhalation valves and nebulizer positions may affect the diameter of aerosol particles. Further studies are warranted to clarify these hypotheses and to validate our experimental data in a clinical perspective.
Conclusions
In summary, the air leakage during NPPV makes it complicated to analyze the factors influencing aerosol delivery. We found that the type of exhalation valve and position of the nebulizer in the ventilator circuit have a significant influence on the efficiency of aerosol delivery during NPPV. As a result, with different exhalation valves, an appropriate nebulizer position should be carefully chosen, and the inhaled dose should be adjusted after accurate prediction of aerosol delivery to ensure optimal clinical efficacy.
Footnotes
Acknowledgments
This work was supported by the National Key Technology R&D Program of the 12th National Five-Year Development Plan (2012BAI05B01). Special thanks are given to Prof. Guangqiao Zeng, MD (State Key Laboratory of Respiratory Disease, Guangzhou Medical University) for his assistance in medical writing.
Author Disclosure Statement
The authors declare that they have no competing interests.