
Abstract
Abstract
Background:
The incorrect handling of Diskus inhalers in Chinese patients with chronic obstructive pulmonary disease (COPD) is not well documented.
Objective:
The present study was conducted to evaluate in detail the handling errors related to the Diskus device, and to elucidate the importance of educating COPD patients on the proper use of the device.
Methods:
A total of 384 COPD patients from a pulmonary clinic in China over a period of 5 years were included in the study. The compliance of COPD patients to the 13 discrete steps of Diskus usage were scored and analyzed by three measures: (1) On day 0, patients were given only a package insert on Diskus, and the handling error rate was assessed. Then the patients were given instruction on the 13-step Diskus procedure until they could demonstrate the proper technique. (2) On days 1, 2, and 3, the observation group was continuously educated on a 13-step procedure, and the percentage of patients who scored 100% for each step was recorded. The control group had no such training. (3) On days 10, 20, and 30, the percentage of all subjects correctly performing the Diskus 13-step inhalation procedure was assessed.
Results:
Incorrect handling techniques on Diskus usage were widely distributed among Chinese COPD patients. Step 8 (“Inhale forcefully from the beginning, slowly, deeply, and uniformly during the inspiratory phase until the lungs are full”) was the most commonly mishandled step (93.8%). The total score and individual step scores of the patients from the observation group were significantly improved during 3-day continuous education. There was also a significantly higher percentage of correctly performed steps in the observation group than in the control group upon assessment on day 10 (96.24% vs. 85.63%, respectively; p<0.01), day 20 (97.31% vs. 86.09%, respectively; p<0.01), and day 30 (98.19% vs. 87.39%, respectively; p<0.01).
Conclusion:
Handling errors of the Diskus 13-step inhalation procedure were commonly observed in Chinese COPD patients. Continuous educational interventions and regular supervision by health-care providers are therefore crucial for the optimum use of the Diskus inhaler.
Introduction
C
Several observation studies have compared incorrect handling practices among MDI and various DPI devices.(12) However, the incorrect handling of Diskus in COPD patients has not been well studied. The prevalence of Diskus errors among COPD patients and other related details were investigated, and the effect of continuous patient education and regular supervision on Diskus usage was assessed.
Materials and Methods
Subjects
Randomized and cross-sectional evaluations based on prospective observational were conducted at the pulmonary clinic of the 88th Hospital of the Chinese People's Liberation Army (PLA) in Tai'an. Data were collected from January 2007 to January 2012. We recruited 384 adult subjects with COPD (mean age, 64 years; Table 1). Subjects were included in the study according to the following criteria: (1) a clinical history and diagnosis of COPD [history of smoking; symptoms such as breathlessness, chronic cough, increased sputum production, wheezing, and chest tightness; frequent and exacerbated chest infections; postbronchodilator and pulmonary function tests with forced expiratory volume in 1 sec (FEV1)/force vital capacity<70%]; (2) a need for medication by inhalation; and (3) previous use of other inhalers but with no prior experience with the Advair Diskus DPI. Patients who had used the Advair Diskus DPI for over a week and those who had received instruction on Diskus inhaler use during the preceding week were excluded from the study. All subjects were outpatients with stable condition and only mild to moderate airway obstruction. Lung function testing was not included in the study protocol. To minimize selection bias, the special clinic office and the investigators were instructed to collect and enroll eligible patients daily. The study was fully explained to all subjects, and informed written consent was obtained from the participants. None of the patients refused to participate in the survey. The study was approved by the Human Ethics Committee of the 88th Hospital of the Chinese PLA. The approved protocol was not altered during the study.
COPD, chronic obstructive pulmonary disease; LABA, long-acting β2-agonists; LTRA, cysteinyl leukotriene receptor antagonist (montelukast) (p.o.); mMRC, modified British Medical Research Council; NS, not significant; Y/N, yes/no.
According to the self-compiled part of the questionnaire.
According to the investigator-filled part of the questionnaire. Other bronchodilators: terbutaline sulfate aerosol (inhalation), or sustained-release theophylline (p.o.).
Study design
The manufacturer's instructions on Diskus use, previous publications on the optimal technique for inhalation,(19–22) and our own previous observations were used to formulate the 13 essential steps for handling the Diskus inhaler (Table 2). Incorrect handling of Diskus was defined as the incorrect performance of any of these predefined steps (including the critical errors; Table 2).
All data are presented as the percentage of subjects performing the incorrect step compared to the total number of observations.
Critical errors.
9.9%.
79.9%.
All the investigators were trained by the same pulmonary doctor who educated the subjects. The investigators received instructions on the Diskus 13-step inhalation procedure and were given follow-up instruction until they were well acquainted with the Diskus device and its proper handling, such that they could perform the evaluation procedure (i.e., on the proper handling of Diskus and on how to score each step of the process). The incorrect handling of the essential steps was subjectively reported, as in similar previous studies.(23)
A questionnaire on patient demographics and a checklist of the essential steps were completed by the investigators during patient assessment. Potential factors that could be associated with incorrect handling were noted; these factors included the age, sex, primary diagnosis, and educational level of the patient. Any unscheduled medical intervention for their respiratory disease within the previous year was noted. Such interventions included emergency room visits, hospital admission, antimicrobial treatment, or corticosteroid tablet intake. Given that these data were collected retrospectively, the use of health-care resources by the patients could not be controlled by the investigators.
The model (or placebo) inhalers used for the handling study were provided by GlaxoSmithKline (China). Each placebo inhaler was completely identical to the Advair Diskus DPI except that it did not contain any active drug. To avoid exhausting the patients with continuous puffing, a long investigation time was allotted for each patient. The study was divided into three parts (Fig. 1). For the first phase, the 384 enrolled COPD patients were asked to use a placebo Diskus inhaler by self-administration under the simultaneous observation of two investigators. Patients were asked to use Diskus as though they were at home. First, each patient was given only the four-step package insert of the Diskus device without additional explanation. The patients were then requested to demonstrate their technique of using the Diskus inhaler with three continuous puffs (at 10-min intervals). The handling errors were recorded independently by the investigators on separate observation sheets (see Table 2). Then the 384 COPD patients were randomly assigned during the second phase into two groups: the observation group (O-group) or the control group (C-group). The number of patients was distributed equally among the two groups, which were not interchangeable. Patients from both groups were formally given verbal instruction on the 13-step Diskus handling procedure with practical demonstrations using a placebo Diskus inhaler. The subjects were trained until they could demonstrate the proper technique (this day was set as the baseline, day 0). The patients were then prescribed to use the Diskus inhaler device therapy (at two daily inhalations) beginning the following day (day 1). The O-group patients were evaluated from day 1 to day 3 by the same investigators. The average number of steps correctly performed and the percentage of patients scoring 100% for each step during the 3 days were compared (Table 3). Handling errors committed by the patients in this group during the 3 days were corrected by the investigators. By contrast, the C-group had no such training as the control group. For the third phase, the subjects were requested to demonstrate Diskus usage in the outpatient clinic room on days 10, 20, and 30, and the handling technique was reevaluated by the same investigators (Table 4). Each patient was instructed to make only three puffs with a 10-min interval for each puff.

Flow diagram of the study design.
Puff twice daily, only assess second puff.
NA, not applicable; NS, not significant; S, significant.
The average correct handling scores of the O-group on days 10, 20, and 30 were 96.24%, 97.31%, and 98.19%, respectively. The average correct handling scores of the C-group on days 10, 20, and 30 were 85.63%, 86.09%, and 87.39%, respectively.
Handling scores
The preliminary analysis concerned the errors made with the proposed 13 steps. The analysis focused on the critical errors (described in Table 2) that are likely to make aerosol therapy useless, according to the literature.(2) The are 13 distinct inhalation steps or maneuvers for Diskus; however, from the second use onwards, only 12 steps are required because the device does not need to be unwrapped repeatedly. The percentage of handling errors for each step was defined as the number of subjects who incorrectly performed a certain step divided by the total number of subjects (i.e., 0% implies that all steps were correctly performed, whereas 100% indicates that none of the subjects correctly performed the step). Incorrect handling that could reduce or negate dose delivery was defined as a critical handling error (indicated by superscript “a” in Table 2). The possibility that an incorrect step would lead to a missing dose could not be determined, because a placebo Diskus inhaler was used during initial educated performance.
Statistical analysis
Descriptive analysis was conducted on the demographics and patient characteristics. To compare demographics and disease characteristics between the O-groups and C-groups, the two-sample t test was used when the data were normally distributed; otherwise the Mann-Whitney test was used. Also, an overall performance score based on all steps combined was calculated. Unless stated otherwise, age, level of education, and COPD diagnosis were included as fixed-effect variables in both models. Data are presented as the mean±standard error unless otherwise specified. A p value of<0.05 for a two-tailed test was considered as statistically significant. Analysis was performed with statistics software (Stata 12, www.stata.com).
Results
A total of 384 subjects (257 males and 127 females) completed the evaluation interview and were enrolled in the study. Some of the demographic and clinical characteristics of the patients are presented in Table 1. The mean age of the participants was 64 years (range, 47–81 years), and 66 patients (17.2%) were ≥75 years old. The duration of affliction with COPD varied from 2 to 34 years. A total of 249 patients (64.8%) had high school education or higher. None of the recruited subjects were previously educated by a health-care provider on the proper technique of Diskus inhalation (Table 1). Moreover, there were no significant statistical and clinical difference between the O-group and the C-group. A third of the subjects had been educated on MDI usage by health-care providers. In the present study, respiratory doctors provided all the instruction for the inhalation technique. The modified British Medical Research Council (mMRC) Dyspnea Scale measures the odds of incorrect handling after adjusting for age, sex, and educational level. The odds ratio (OR) for incorrect handling was 6.4 for scale 3 of mMRC (95% confidence interval, 1.71–11.09), as compared with scale 2 and scale 0–1.
During the initial assessment with the four-step inhalation technique in the Diskus leaflet, the percentage of subjects performing each step incorrectly was based on their third puff (Table 2). Incorrect handling was frequent and widely distributed among the users of Diskus, as compared with the proposed 13-step procedure. According to our arbitrary criteria, at least one essential error for Diskus was observed in 100% of users, with 93.8% making at least one critical error. On average, 60–70% of the 13-step procedure was incorrectly performed. By contrast, 90% of the critical handling errors, on average, were made for the 13 steps. Step 8 was incorrectly performed by 93.8% of the subjects, which was the highest error rate among the 13 steps. Steps 6, 7, and 10 were incorrectly performed by >60% of the subjects, whereas steps 4 and 5 were incorrectly performed by 40–50%. All the other steps (steps 1, 2, 9, 11, 12, and 13) were incorrectly performed by <25% of the subjects (Fig. 2).
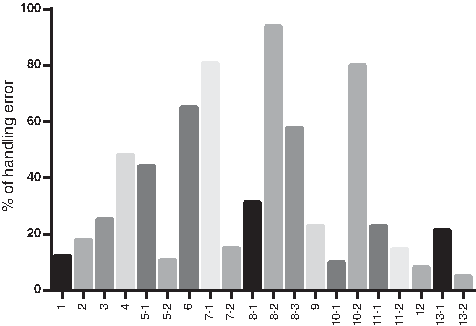
Incorrect handling of 13-step Diskus inhalation procedure (% of handling error: 0=no incorrect handling, 100=all steps performed incorrectly).
The average correct performance of all inhalation steps for the O-group is shown in Table 3. The total score and the scores for the individual steps of the O-group patients were significantly improved after the 3-day continuous education. Statistical analysis was not performed because of the absence of a control group.
The correct handling on days 10, 20, and 30 were compared between the O-group and the C-group. All the subjects from the O-group had significantly improved their rate of correct inhalation during the 3-day period (Table 4). Patients who were continuously checked for 3 days to master the prescribed inhaler practice during follow-up visits had a lower risk of inhalation errors when using Diskus (OR, 0.91±0.18; p<0.01). The average correct handling scores of the O-group on days 10, 20, and 30 were 96.24%, 97.31%, and 98.19%, respectively. However, the handling at every step had not significantly improved in the C-group (Fig. 3). The correct handling of the O-group was significantly higher than that of the C-group in steps 3–8, step 10, and step 11 (p<0.01). The total number of subjects with critical errors was high during the initial Diskus handling (about 93.8%), but this was considerably decreased by day 10 to approximately 7.5%.

Subjects in each group correctly performing on days 10, 20, and 30.
Discussion
Approximately 4–94% of patients using DPIs do not use the devices correctly, and 25% have never been trained to use an inhaler.(7,24,25) The results showed that the frequency of handling errors (critical and noncritical) is high among COPD patients who were given only the Diskus device leaflet as the instruction. The provision of a device leaflet seems insufficient for preventing handling errors. Only a few of the patients were able to correctly perform all of the steps correctly. This frequently occurring type of critical error in DPI usage is a critical factor that determines the treatment effectiveness.(26) These critical errors could result in the complete failure of dose application and need to be considered during patient evaluation. The critical errors in Diskus usage may be related to a specific feature in the Diskus device or to the detailed instructions in the package insert. In the present study, frequent errors were observed among most of the subjects.
The incorrect handling of steps 1 and 2 causes the dry powder to be incorrectly positioned in the mouthpiece, thereby decreasing the inhaled dose that reaches the lungs. Incorrect handling of step 3 causes the dry powder dose to fall from the device when the mouthpiece is held downwards. Incorrect handling of step 4 produces excess humidity in the mouthpiece with the clumping and blowing of the dry powder out of the device, thereby resulting in the suboptimal delivery of the medication. Incorrect handling of step 5 produces an insufficient inhalation force and shorter inhalation time. Moreover, forced exhalation of the residual volume before inhalation is not recommended, because it may lead to the temporary collapse of airway. The incorrect handling of step 6 creates a bent and narrow airway that obstructs the inhalation of the dry powder. The incorrect handling of step 7 causes dose blockage by the tooth, tongue, and palatine uvula in the initial path of the mouth, thereby reducing the forced inspiratory volume.
The complex and controversial handling of step 8 involves several mechanical principles: (1) The forceful inhalation from the beginning deagglomerates the powder formulation into more efficient small “respirable” particles.(27,28) (2) Extremely high velocity of inhalation tends to cause the aerosol to be deposited in the upper airway instead of moving around the bend of the throat,(29,30) whereas a slower flow minimizes oropharyngeal and upper airway deposition while enhancing distal delivery and deposition.(31–34) In vitro studies indicate that the Diskus inhaler deagglomerates and delivers a consistent fine particle dose at flow rates of 28 and 60 L/min.(13,14) Adult patients with obstructive lung disease and severely compromised lung function (with 20–30% of the predicted mean FEV1) were reported to achieve a mean peak inspiratory flow of 82.4 L/min (range, 46.1–115.3 L/min) using the Diskus device.(35) Patients with COPD may be expected to receive an adequate dose of the drug with slow, deep, and uniform inhalations using a Diskus inhaler, thereby achieving maximal performance. However, extremely slow inhalation has often been described as inhaler mishandling.(36–38) For Diskus, the lowest effective inspiratory flow is 30 L/min. (3) Inhalation should not be prematurely stopped, nor should patients inhale twice or more during the inspiratory phase of the breathing cycle. Some patients with moderate and severe COPD have weak inspiration flow and usually encounter this problem.
Incorrect handling of step 9 produces an excessively humid condition that may create agglomerated residues that adhere to the inner wall of the mouthpiece. Step 10 is intended to allow for the sedimentation of drug particles in the small airways of lung, as well as to increase the amount of inhaled drug particles deposited in the peripheral and lower airways during the breath-hold residence time.(39–42) Incorrect handling of step 11 may disturb and partially exhale the drug deposited in the lung. This step may similarly produce a condition of excess humidity in the mouthpiece, as in step 4. The purpose of closing the Diskus in step 12 is to prevent dust and humidity from accumulating in the mouthpiece reservoir. Incorrect handling of step 13 increases the risk of developing an oropharyngeal candidiasis infection, and the systemic absorption of the swallowed drug. Inhalation through the nose was reported in 2% of the subjects in a previous study,(43) although this error in COPD patients using Diskus was not observed in our study.
Our choice of critical errors was based on the literature.(2) However, these errors were assigned in an arbitrary manner and deserve further discussion. The literature does not identify any conditions that cause patients to become predisposed to inhaler misuse. The mishandling of Diskus may be due to several factors. Patients who did not learn about Diskus usage from a prescribing physician or pharmacist may find self-learning insufficient, thereby leading to defective or incorrect usage. Differences in the handling technique are inevitable, given the different educational levels, ages, and other patient characteristics, even when all patients received the same instructions. DPIs are complex devices, and inhalation involves several steps that may prevent their proper use among patients who are aged or have lower levels of education. Moreover, patients who suffer from dyspnea have more difficulty in performing controlled inhalation or holding their breath for a long period of time. Cognitive decline implies that more complex maneuvers may be challenging for elderly patients. These patients quickly forget the correct technique.(3,44,45) Patients who were able to demonstrate proper technique in the clinic may still ineffectively use the device during routine use, and some may randomly modify the technique even after instruction. Incorrect inhaler use has also been associated with patients having executive dysfunction, which affects planning and sequencing.(46) Health-care providers might feel responsible for instructing their patients on Diskus usage; they may not be acquainted with proper Diskus handling or they may be unaware of optimal device usage. Their inaction is a primary cause of the handling errors.
The results of this study demonstrate the importance of educating and training patients by health-care providers on the proper Diskus usage. Proper inhaler technique warrants continuous education, assessment, and regular supervision by a competent health-care provider. Health-care providers should effectively implement three significant procedures:
(1) Assessment. The increasing consensus is that successful clinical outcomes are determined by the choice of an appropriate inhaler device as much as by the drugs that are used in the device.(47) Therefore, health-care providers must first evaluate if the Diskus device is suitable for prescription to a patient, and if the patient can and will correctly use the device. The recommendation of a Diskus device should consider the level of understanding, personality, and economic position of the COPD patient to achieve cost-effectiveness, meet patient preference, and attain high compliance. (2) Education. The subjects were educated by repeated demonstrations until they could consistently perform the proper technique during consultation. Several studies indicated that such training has to be performed periodically; without follow-up, patients tend to eventually slip back into old habits.(48) During training, the critical handling errors need to be carefully monitored by the health-care provider, because errors in these steps may reduce dose delivery and the therapeutic outcome.(49,50) Proper training and education on Diskus use for each patient will be a powerful means to mitigate the handling error risks in Diskus usage. (3) Supervision. Health-care providers are responsible for regularly checking patients for the proper inhaler technique, and reviewing the compliance to the treatment regimen during each follow-up visit; they should also provide numerous recommendations to ensure that the patient understands how to effectively use the inhaler.(51) The health-care provider must essentially aim to establish a feedback mechanism (asking for regimen adherence and giving automated reminders) to monitor patient compliance, to facilitate patient self-education, and to ensure the correct inhalation by patients.
This study has several limitations. First, we did not measure the effect of mishandling on drug deposition or on the resulting pharmacologic effect. Second, we did not assess the relevance of these findings on the long-term use of the Diskus device.
Conclusion
Handling errors on the Advair Diskus 13-step procedure were widely observed among Chinese COPD patients. The provision of appropriate training and device education by health-care providers is a critical factor in ensuring that patients receive the appropriate medication using a Diskus device. Furthermore, the continuous educational intervention and regular supervision of Diskus usage could minimize handling errors among patients with COPD.
Footnotes
Acknowledgments
HDL and GGZ conceived and designed the study. YYC and HZ collected the data. ZRZ and XXD analyzed the data. HDL and ZRZ helped to draft the manuscript. All of the authors read and approved the final manuscript.
Author Disclosure Statement
The authors declare that there are no conflicts of interest.