
Abstract
Abstract
Background:
A peak inspiratory flow rate (PIFR) of <60 L/min against the internal resistance (resist) of a dry powder inhaler (DPI) may limit the ability of a patient with chronic obstructive pulmonary disease (COPD) to achieve bronchodilation. The hypothesis was that lung function would be higher with a beta-agonist inhaled via nebulization compared with dry powder in patients with COPD who exhibit a PIFRresist of <60 L/min against the Diskus®.
Methods:
This study was randomized, single-blind, and crossover with spirometry and inspiratory capacity (IC) measured at 15, 30, and 120 min post treatment. The efficacy of arformoterol aerosol solution (15 μg/2 mL) via nebulizer was compared with salmeterol dry powder (50 μg) via Diskus. The primary outcome was the change in lung function from baseline at 2 hr as these two inhaled beta-agonists have the similar peak bronchodilator effect as measured by forced expiratory volume in 1 sec (FEV1).
Results:
Twenty patients (15 females/5 males) with postalbuterol FEV1 of 0.83±0.31 L (38±12% predicted) and PIFRresist of 53±5 L/min completed the study. At 15 min, improvements in FEV1, forced vital capacity (FVC), and IC were significantly higher with arformoterol than with salmeterol. At 2 hr, changes in FVC and IC, but not FEV1, were significantly higher with arformoterol. At visit 3, patient preference was similar for salmeterol Diskus (n=8) and arformoterol solution (n=7), whereas five patients reported no preference.
Conclusions:
At peak effect (2 hr), volume responses were greater with arfomoterol via nebulizer compared with dry powder salmeterol in patients with COPD who had a PIFRresist of <60 L/min. Bronchodilator therapy via nebulization should be considered in patients with COPD who have a suboptimal PIFRresist against a particular DPI.
Introduction
A
Alternative approaches to using a DPI for bronchodilation are inhaling an aerosol solution from a nebulizer and using a metered-dose inhaler (MDI) with a spacer.(1) In randomized controlled trials, patients with moderate to severe COPD show similar improvements in FEV1 at 2 hr with a long-acting beta-agonist delivered by MDI (salmeterol) or DPI (formoterol) and by nebulization (arformoterol/formoterol).(7–10) Although PIFRresist was not measured in these study patients, their baseline characteristics do not fit the clinical phenotype—female gender, shorter stature, and reduced values for forced vital capacity (FVC) and inspiratory capacity (IC) as percent predicted—of patients with COPD who exhibit a suboptimal PIFRresist (<60 L/min) against the simulated resistance of the Diskus.(6)
The objective of this study was to compare the acute changes in lung function with the recommended initial fast and hard inhalation of a beta-agonist bronchodilator from a DPI (salmeterol Diskus) with the tidal breathing of aerosol solution delivered via nebulization (arformoterol) in patients with COPD who have a PIFRresist of <60 L/min against the Diskus. The rationale for such investigation is that patients with a suboptimal PIFRresist may be “at risk” for not being able to completely inhale a dry powder bronchodilator into the lower respiratory tract.(3,11) Salmeterol dry powder was selected for comparison because: (1) it is a widely used beta-agonist in the Diskus; (2) the Diskus has a lower internal resistance than formoterol Turbuhaler®(2,3,11,12); and (3) patients with moderate-severe COPD and presumed optimal PIFRresist (>60 L/min) show similar peak FEV1 responses at 2 hr after inhaling salmeterol via MDI and arformoterol via nebulizer.(9,10) The hypothesis of our study is that lung function measured at 2 hr post dose would be greater with a beta-agonist bronchodilator delivered by nebulization than with inhalation from a DPI in patients with COPD who exhibit a PIFRresist of <60 L/min.
Materials and Methods
Study subjects
Inclusion criteria were: diagnosis of COPD(13); at least 10 pack-year history of cigarette smoking; age ≥60 years; current or previous use of the Diskus DPI (salmeterol or salmeterol/fluticasone); and PIFR of <60 L/min using the In-check DIAL® against the simulated resistance of the Diskus. Exclusion criteria were: inability to understand verbal instructions; any concomitant disease that might interfere with study procedures; unstable clinical disease; and inability to withhold short- and long-acting bronchodilators on the days of testing. Eligible patients were recruited after they completed pulmonary function tests at our institution.
Study design
This randomized, open-label, single-blind, crossover study was performed between July 2011 and October 2012. The protocol was approved by the Committee for the Protection of Human Subjects at Dartmouth College (#22812). The study was registered with ClinicalTrials.gov: NCT01391559. All patients signed the appropriate consent form. Patients participated in three visits, each 2–3 days apart. Testing procedures at these visits are described in Table 1. At visit 2, patients were randomized to the study medication. The pulmonary function technician who collected patient data at visits 2 and 3 was blinded to the study medication. All patients held short-acting bronchodilators for 4 hr and long-acting bronchodilators for 12 hr (if used twice daily) and 24 hr (if used once daily) prior to visits 2 and 3.
Methods
The In-Check DIAL (Clement Clerke International Ltd., Harlow, UK) was used to measure PIFR against the simulated internal resistance of the Diskus. According to the manufacturer, the In-Check DIAL is accurate within±10% or±10 L/min, whichever is greater. The test–retest reliability of PIFRresist was excellent in 45 patients with advanced COPD.(6) At visit 1, spirometry, IC, and diffusing capacity (NSpire HD3000; Nspire Health Inc., Longmont, CO) were measured using standard techniques.(14,15) Values were expressed as percentages of predicted values.(16,17) At visits 2 and 3, patients performed spirometry and IC maneuvers at baseline and 15, 30, and 120 min after completing inhalation of 50 μg of salmeterol from the Diskus or 15 μg of arformoterol solution administered by the UP-MIST nebulizer (Hospitak REF 3952-E; Birkerod, Denmark) using compressed gas.
Analysis
The primary outcome was the change in lung function (FEV1, FVC, and IC) at 2 hr after inhalation of the study medication compared with baseline. The secondary outcome was patient preference for salmeterol Diskus or arformoterol solution via nebulizer. Paired t tests were used to compare these outcomes at equivalent time periods. Results are presented as means±standard deviation (SD) values. A p≤0.05 was considered significant.
Results
Enrollment, allocation, follow-up, and analysis of patients are shown in Figure 1. Descriptive characteristics of the 15 female and five male patients with COPD are shown in Table 2. All patients had a PIFRresist of <60 L/min at visit 1 (53±5 L/min). The duration of COPD diagnosis was 8.7±4.3 years, and smoking history was 50.8±22.0 pack-years. For patients currently using the Diskus DPI, four reported that the medication improved their breathing difficulty, whereas five were unsure. For patients who previously used the Diskus, one patient reported that the medication improved her breathing difficulty, five reported no benefit, and five patients were unsure.
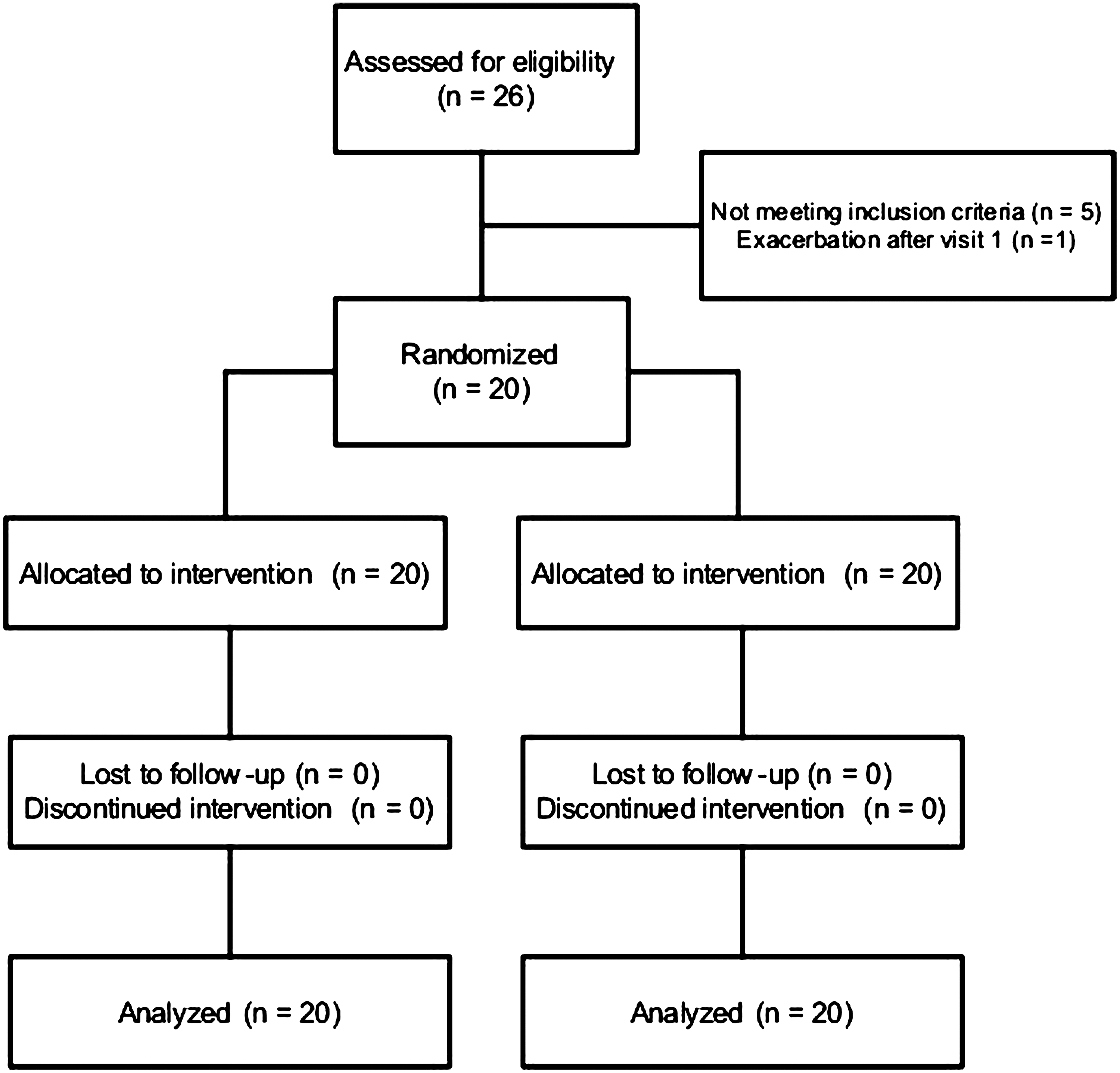
Enrollment, allocation, follow-up, and analysis of patients. The figure shows that 20 patients completed testing with each arm of treatment (arformoterol and salmeterol). Based on randomization, 10 patients received arformoterol first, and 10 patients received salmeterol first. Subjects then crossed over to the other therapy.
BD, bronchodilator; FEV1, forced expiratory volume in 1 sec; FVC, forced vital capacity; IC, inspiratory capacity; SAC BDI, self-administered computerized baseline dyspnea index.(30)
Data were obtained at visit 1. Three patients had stage II disease, 10 patients had stage III disease, and seven had grade IV disease.(29) Medications for COPD included: short-acting beta-agonist (n=20); long-acting beta-agonist (n=9); anticholinergic (n=18); inhaled corticosteroid (n=14); and theophylline (n=1).
There were no significant differences in lung function at baseline between visits 2 and 3. Baseline FEV1 at visit 2 was 0.72±0.30 L (33±11% predicted) and at visit 3 was 0.71±0.29 L (33±11% predicted) (p=0.37). Changes in lung function from baseline with the study medications are displayed in Table 3. At 15 min, improvements in all three measures of lung function were significantly greater with arformoterol compared with salmeterol. At 2 hr, the changes in FVC and IC, but not FEV1, were significantly higher with arformoterol (Table 3 and Figs. 2–4). Eight patients preferred salmeterol Diskus, seven patients preferred arformoterol solution, and five patients had no preference.
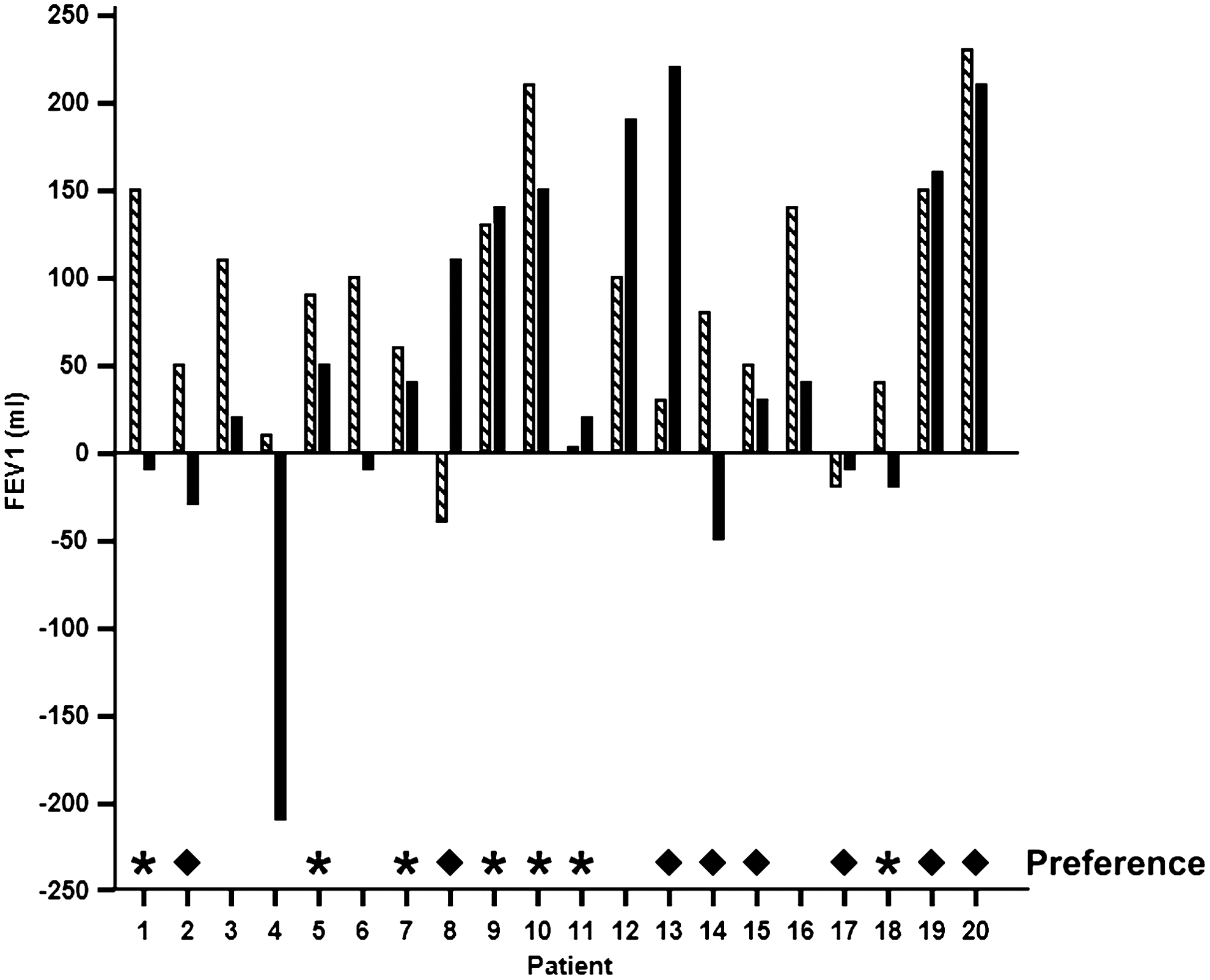
Individual changes in forced expiratory volume in 1 sec (FEV1) at 2 hr compared with baseline. Hatched bars, arformoterol; solid bars, salmeterol. For the group, p=0.17. *Patient preference for arformoterol; ♦patient preference for salmeterol. Five patients did not have a preference.
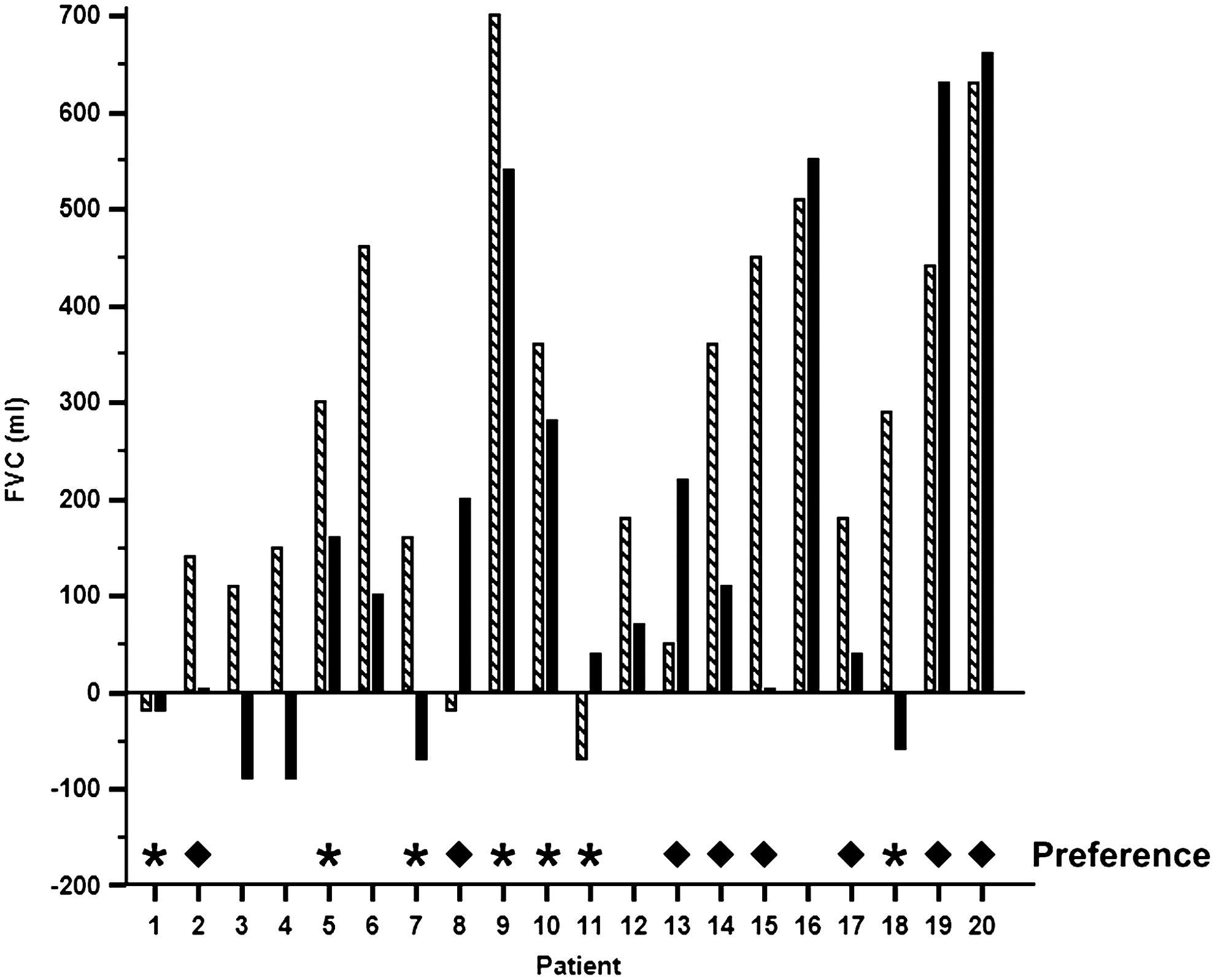
Individual changes in forced vital capacity (FVC) at 2 hr compared with baseline. Hatched bars, arformoterol; solid bars, salmeterol. For the group, p=0.02. *Patient preference for arformoterol; ♦patient preference for salmeterol. Five patients did not have a preference.
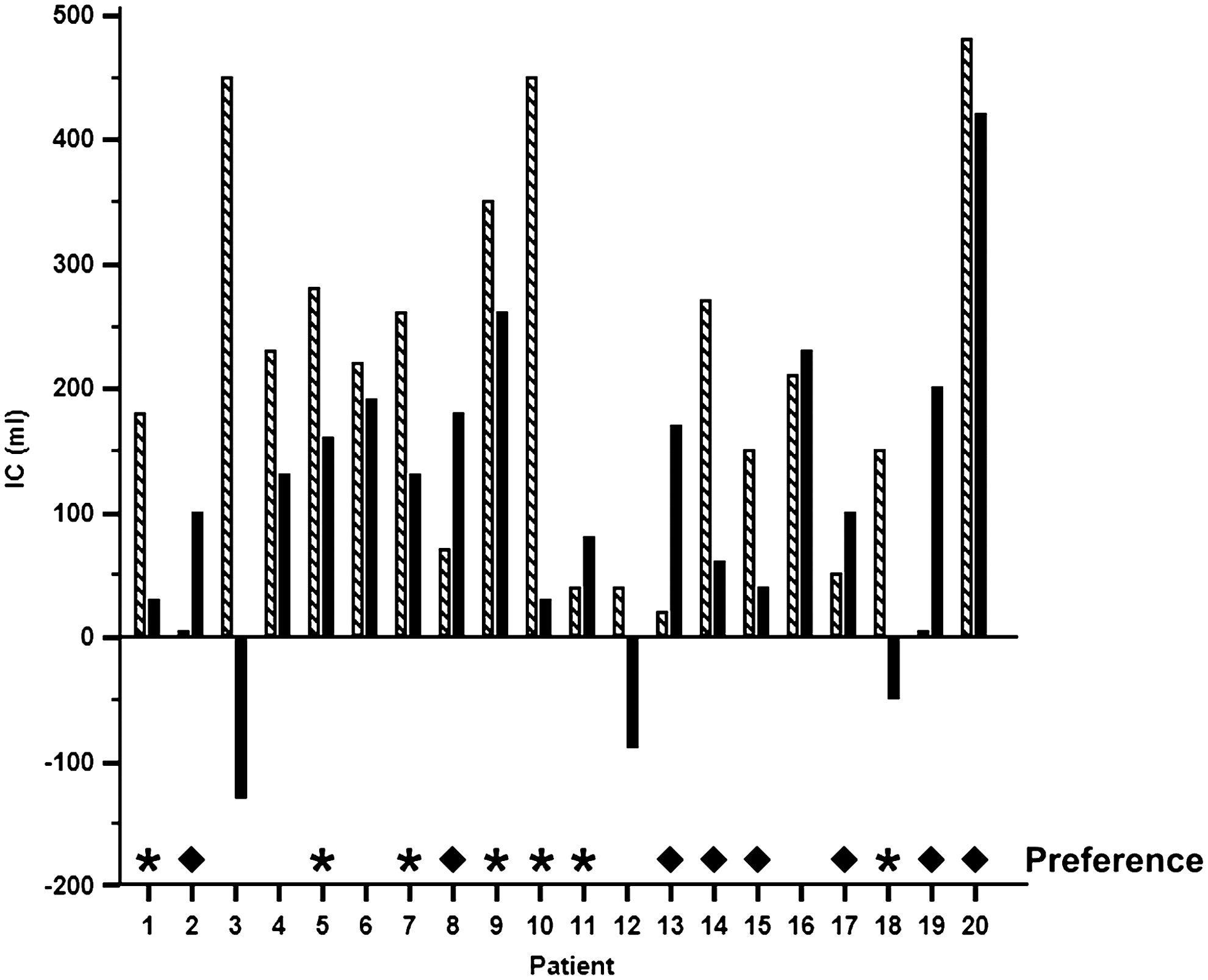
Individual changes in inspiratory capacity (IC) at 2 hr compared with baseline. Hatched bars, arformoterol; solid bars, salmeterol. For the group, p=0.05. *Patient preference for arformoterol; ♦patient preference for salmeterol. Five patients did not have a preference.
Δ, difference compared with baseline values; FEV1, forced expiratory volume in 1 sec; FVC, forced vital capacity; IC, inspiratory capacity.
Numbers in parentheses are percent change from baseline.
Discussion
The major findings of this study of 20 patients with COPD who had a suboptimal PIFRresist against the Diskus were: (1) for peak bronchodilator effect at 2 hr, the increases in FVC and IC, but not FEV1, were greater for arformoterol compared with salmeterol; and (2) patient preference was similar for arformoterol and salmeterol.
It is important to consider baseline characteristics of our patients in interpreting the results. As an inclusion criterion, all patients had a PIFR of <60 L/min against the simulated resistance of the Diskus. Patients were predominantly female (75%), had a low diffusing capacity (47±16% predicted), and reported substantial breathlessness with activities of daily living (self-administered computerized baseline dyspnea index=4.7±1.6). The predominance of females in our study was likely a result of women having lower absolute values for lung function compared with men, and the requirement of a threshold value for PIFRresist. Nineteen of the 20 patients in our study had a diffusing capacity below the lower limit of normal, consistent with the emphysema phenotype of COPD.
Standard and approved doses of salmeterol Diskus (50 μg) and arformoterol solution (15 μg) were evaluated in this study. We considered that these doses were appropriate for comparison based on results of two previous randomized controlled trials in which salmeterol via MDI (42 μg) and arformoterol solution (15 μg) demonstrated similar peak bronchodilator effect for FEV1.(9,10) Neither FVC nor IC results were reported in these trials.(9,10) Furthermore, the dose of salmeterol delivered by MDI (42 μg), which was discontinued in December 2007 because of its chlorofluorocarbon propellant, is equivalent to the dose delivered by Diskus (50 μg).
The responses in lung function were highly variable among individuals as shown in Figures 2–4. The significantly greater improvements in lung function at 15 min with arformoterol are consistent with a more rapid onset of action than with salmeterol.(9) Although the mean differences in FEV1 between arformoterol and salmeterol were similar at 15 min (33 mL) and 2 hr (32 mL), statistical comparison showed no difference for FEV1 at 2 hr between medications. This may be due in part to response variability as evident by the high SD with salmeterol therapy at 2 hr. In contrast, the increases in FVC and IC at 2 hr were significantly greater with arformoterol than with salmeterol. These results support the hypothesis of the study, and are consistent with previous studies that demonstrate bronchodilator responsiveness is more common for FVC than FEV1 in patients with severe emphysema.(18,19)
To our knowledge, this study is the first to compare the bronchodilator effects of inhaling similar beta-agonists via DPI and via nebulization in a unique COPD population who had a suboptimal PIFRresist. As a result, these patients may not be able to completely inhale a dry powder bronchodilator into their lower respiratory tract. The DPI and nebulizer delivery systems require different inhalational maneuvers. A deep and hard inhalation is recommended to overcome the internal resistance of a DPI in order to deaggregate the powder formulation into fine particles, whereas tidal breathing is recommended for inhalation of aerosol solution in a nebulizer.(1) We did not investigate the mechanism for greater improvement in lung function with arformoterol, but consider it likely that the nebulized aerosol arformoterol achieved deeper penetration into the lower respiratory tract than dry powder salmeterol in our patients with a suboptimal PIFRresist. However, imaging studies using radiolabeled tracer material attached to the medication would be required to demonstrate this effect.(20,21)
Although we did not measure residual volume (RV) and functional residual capacity (FRC) in our patients, the reduced values for FVC and IC at baseline suggest that our patients had air trapping and hyperinflation. Improvements in FVC and IC are considered to be markers of changes in RV and FRC, respectively, after bronchodilator administration.(19,22) Newton and colleagues(23) showed substantial increases in both FVC and IC after inhalation of albuterol in hyperinflated patients with COPD even though only a minority of patients had improvements in FEV1. Although it is unknown whether the improvements in FVC and IC with arformoterol would be sufficient for our patients with PIFR of <60 L/min to experience clinical benefit, previous studies in patients with COPD have demonstrated significant improvements in dyspnea ratings with arformoterol after 3 and 6 months.(8,10)
There are limitations to our study. First, the study was single-blind as the patient was aware which medication was administered at each test visit, although the technician collecting the outcome data was not informed of medication assignment. A double-blind condition would have been preferred to avoid potential bias. However, a placebo Diskus identical in appearance to salmeterol was not available. Second, we compared salmeterol Diskus rather than formoterol Turbuhaler with nebulized arformoterol solution, because the Diskus is a widely used DPI and has a lower internal resistance than the Turbuhaler.(2,3,11,24) In theory, a lower internal resistance, as exists with the Diskus DPI, would minimize any possible limitations of a suboptimal PIFRresist. Third, this study was performed in 20 patients, and a larger number of participants would be required to exclude a type II error. Fourth, single doses of bronchodilators were administered, and multiple doses over a longer study period with assessment of clinical outcomes would be relevant.(25)
In 2001, a European Respiratory Society task force suggested that future research is needed to identify which patients with COPD “might benefit (or not benefit) from nebulized therapy using clinically relevant assessment systems.”(26) This task force proposed optimizing the patient's inhalational technique with a DPI, and if the patient does not experience subjective benefit, then switching to nebulized therapy.(26) This approach is used commonly in clinical practice. Present guidelines and statements on the management of stable COPD do not recommend any objective measure as to when to prescribe nebulized bronchodilator therapy.(13,27–29)
Our study is the first to prospectively examine whether using a threshold of PIFRresist of <60 L/min against a specific DPI is a useful criterion for when to use a nebulizer to deliver bronchodilator medications. Our results should be interpreted with caution until supported by a prospective and double-blind study with a larger number of patients. A 1–2-week randomized controlled trial comparing dry powder and nebulized bronchodilators is needed in patients with COPD who exhibit a suboptimal PIFRresist to further address the question, “When should nebulized bronchodilator therapy be prescribed for patients with COPD?”
Footnotes
Acknowledgments
Dr. Mahler developed the research protocol, supervised data collection, reviewed the analysis, and prepared the manuscript. Dr. Mahler is the guarantor of the manuscript and takes responsibility for the integrity of the data and the accuracy of data analysis. Ms. Waterman assisted in the development of the research protocol, collected data, performed statistical analysis, and reviewed the manuscript. Mr. Ward assisted in the development of the research protocol, collected data, and reviewed the manuscript. Dr. Gifford reviewed and revised the research protocol, performed statistical analysis, and reviewed the manuscript. Sunovion Pharmaceuticals Inc. provided a grant for this investigator-initiated investigation to the Clinical Trials Office at Dartmouth-Hitchcock Medical Center, but had no role in the conduct of the study, data analysis, or manuscript preparation/review.
Author Disclosure Statement
Dr. Mahler serves as a consultant to Boehringer Ingelheim, Forest, GlaxoSmithKline, Novartis, and Sunovion, and serves on advisory boards of Forest, GlaxoSmithKline, Merck, Novartis, Pearl, and Sunovion. The Clinical Trials Office at Dartmouth-Hitchcock Medical Center has received grant support from Boehringer Ingelheim, GlaxoSmithKline, Novartis, and Sunovion for which Dr. Mahler was the principal investigator. Ms. Waterman, Mr. Ward, and Dr. Gifford have no conflicts of interest.