
Abstract
Abstract
Background:
Few studies on performance comparison of nebulizer systems coupled with a single-limb circuit bilevel ventilator are available. Most of these data compared the aerosol drug delivery for only two different systems. Using an adult lung bench model of noninvasive ventilation, we compared inhaled and lost doses of three nebulizer systems coupled with a single-limb circuit bilevel ventilator, as well as the influence of the nebulizer position.
Method:
Three vibrating mesh nebulizers (Aeroneb® Pro, Aeroneb® Solo, and NIVO®), one jet nebulizer (Sidestream®), and one ultrasonic nebulizer (Servo Ultra Nebulizer 145®) coupled with a bilevel ventilator were tested. They were charged with amikacin solution (500 mg/4 mL) and operated at two different positions: before and after the exhalation port (starting from the lung). The inhaled dose, the expiratory wasted dose, and the estimated lost dose were assessed by the residual gravimetric method.
Results:
The doses varied widely among the nebulizer types and position. When the nebulizer was positioned before the exhalation port, the vibrating mesh nebulizer delivered the highest inhaled dose (p<0.001), the jet nebulizer the highest expiratory wasted dose (p<0.001), and the ultrasonic device the highest total lost dose (p<0.001). When the nebulizer was positioned after the exhalation port, the vibrating mesh nebulizers delivered the highest inhaled (p<0.001) and expiratory wasted doses (p<0.001), and the ultrasonic device the highest total lost dose (p<0.001). The most efficient nebulizers were NIVO and Aeroneb Solo when placed before the exhalation port.
Conclusions:
In a single-limb circuit bilevel ventilator, vibrating mesh nebulizers positioned between the exhalation port and lung model are more efficient for drug delivery compared with jet or ultrasonic nebulizers. In this position, the improved efficiency of vibrating mesh nebulizers was due to an increase in the inhaled dose and a reduction in the exhaled wasted dose compared with placement between the ventilator and the expiratory port. Because of the high total lost dose, the ultrasonic device should not be recommended. Nebulizer placement before the exhalation port increased the inhaled dose and decreased the expiratory wasted dose, except for the jet nebulizer.
Introduction
S
Three different types of nebulizers are commonly used(20,24): jet, ultrasonic, and vibrating mesh nebulizers. Jet nebulizers use a high-speed velocity gas flow to produce aerosol,(23,25) whereas ultrasonic nebulizers generate aerosol by sound waves created by high-frequency vibrations of a piezoelectric crystal.(23,25) Vibrating mesh nebulizers, the most recent devices, produce aerosol by vibrations of a mesh or plate with multiple apertures.(13,26) Aerosol delivery is highly influenced by nebulizer- and drug-related factors (e.g., mechanisms of aerosol production,(13,27–29) performances of the nebulizer,(15,30,31) characteristics of the drug solution(32–35)), as well as ventilator- and circuit-related factors (e.g., the ventilator settings,(36,37) drug loss in the circuit,(38) heat and humidification in the circuit,(32,39) or the nebulizer position(24,40)).
Several studies have shown that the choice of ventilator does not influence the clinical outcomes of NIPPV treatment.(17,18,41) However, some healthcare institutions prefer bilevel ventilators because of their easier handling, lower costs, and higher flexibility compared with other types of ventilators currently available.(41–43) Unlike intensive care unit (ICU) ventilators, bilevel ventilators generally use a single-limb circuit with an integrated exhalation port device.(14,41,44) It forms a continuous leak port and, hence, the loss of nebulized drug in the ambient air can be potentially increased.(40,45,46) Additionally, a breath-synchronized nebulization option that could improve drug delivery by limiting drug loss during exhalation(1,32,47,48) is currently not available on bilevel ventilators.(1,44)
Only a few studies on performance comparison of nebulizer systems coupled with a single-limb circuit bilevel ventilator are available.(42,45,49,50) Most of them compared the aerosol drug delivery between only two different systems. Moreover, the influence of the type of nebulizers on drug loss through an exhalation port was not well studied. Abdelrahim et al.(49) reported that the amount of drug lost from a single-arch exhalation port was significantly higher with a jet nebulizer than with a vibrating mesh device. They also observed that this drug loss was significantly higher than the drug delivery for the jet nebulizer. Concerning the ultrasonic device coupled with a bilevel ventilator, to our knowledge no data are currently available.
A comparison of all nebulizer systems, including an ultrasonic device, under the same conditions can help clinicians to optimize practical recommendations.(7,24,51) Therefore, the aims of this in vitro study are, firstly, to compare inhaled and lost doses of three types of nebulizers coupled with a single-limb circuit bilevel ventilator using adult settings and, secondly, to evaluate the influence of nebulizer position on these doses.
Materials and Methods
Nebulizers and bilevel ventilator
Three types of nebulizers were tested in this study:
• Three vibrating mesh nebulizers: Aeroneb® Pro (VAP), Aeroneb® Solo (VAS), and NIVO® (VAN) (Aerogen, Dangan, Galway, Ireland). They were powered by the Aeroneb® Pro Controller. • One jet nebulizer: Sidestream® (PJN) (Medic-Aid, West Sussex, UK). It was driven with a Porta-Neb® compressor (Philips Respironics, Guildford, UK) providing an air flow rate of 6 L.m–1. • One ultrasonic nebulizer: Servo Ultra Nebulizer 145® (USN) (MAQUET Critical Care AB, Solena, Sweden). It was electrically driven by an ICU ventilator (continuous nebulization mode).
These different nebulizers were coupled with a bilevel ventilator Philips Trilogy® 100 (Philips Respironics, Murrysville, PA) designed for use in home and alternative care sites. This typical turbine-based ventilator was used with an adult single-limb circuit (180 cm length×22 mm diameter) and a passive exhalation port (Whisper Swivel II®; Philips Respironics) placed in-line close to the patient to provide a continuous leak path for exhaled gases. The leak flow through this orifice is proportional to the pressure in the circuit (range from 17 L.m–1 at 5 cm H2O to 40 L.m–1 at 20 cm H2O; according to the Philips Respironics user manual). For the current study, no heating and humidification systems were used.
Experimental model
The test lung (5600i Dual Adult Training/Test Lung; Michigan Instrument Inc., Grand Rapids, MI) is made of dual chambers linked by a rigid metal piece. The first chamber (simulating the respiratory muscles) was connected to an ICU ventilator MAQUET SERVO-i® (MAQUET Critical Care AB), which was set in volume controlled ventilation mode to simulate a spontaneous breathing adult patient with obstructive lung disease [tidal volume=400 mL, respiratory rate=15 breaths/min, I/E ratio=1:3, inspiratory rise time=5% of respiratory cycle time, breath-hold time=5% of respiratory cycle time]. The second chamber (simulating the lungs) was connected to the bilevel ventilator Trilogy100, which was set in Pressure Support mode (spontaneous mode) with an inspiratory positive airway pressure (IPAP) of 20 cm H2O, an expiratory positive airway pressure (EPAP) of 5 cm H2O, a flow trigger sensitivity of 9 L.m–1, an inspiratory cycle-off of 30% of peak inspiratory flow, and an inspiratory rise time set at level 1 (fastest response). The ventilator pressures were adapted from obstructive lung disease patients when bilevel ventilation is initiated during acute exacerbations in clinical practice.(41,52) The flow trigger sensitivity was set to prevent auto-triggering or missed trigger. The positive pressure insufflated by the ICU ventilator into the first chamber (driving chamber) produced a negative pressure in the second chamber (pressurized chamber), which triggered the inspiratory phase of the bilevel ventilator.
Absolute bacterial/viral disposable filters (Air Safety Ltd., Lancashire, UK) were used to collect the different nebulized doses. A first filter (filter 1) was placed between the inlet of the lung model and ventilator circuit to measure the inhaled dose (IND), i.e., the dose that would reach the facemask during the breathing cycle. It was positioned superiorly to the ventilator circuit to prevent contamination by liquid medication resulting from impaction. A second filter (filter 2) was placed in a customized filter holder enclosing the exhalation port completely, as shown in Figure 1. This filter system was specifically designed to collect the amount of drug lost to the atmosphere through the Whisper Swivel II device. This quantity was defined as the expiratory wasted dose (EWD).
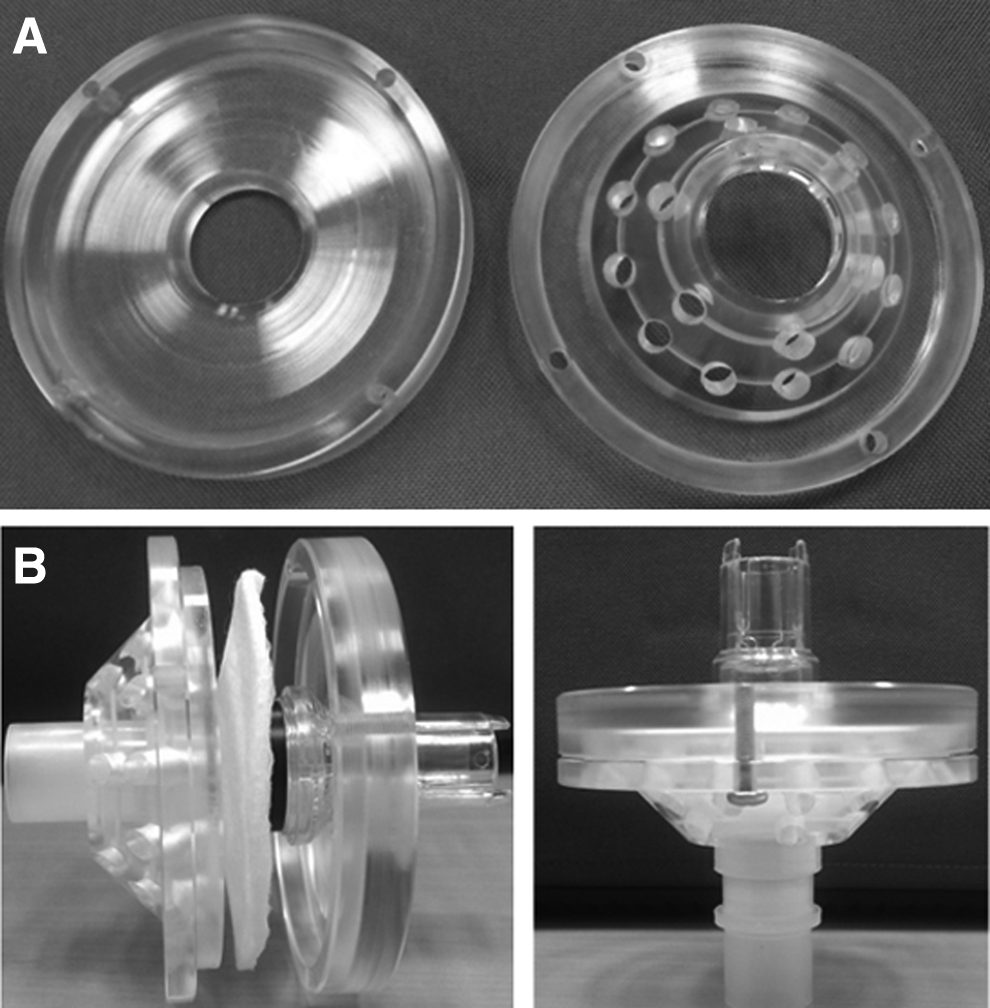
Pictures show our customized filter holder disassembled
Study design
The nebulizers were connected to the ventilator circuit with a standard T-piece connector for the pneumatic nebulizer and with specific adapters (recommended by the manufacturers) for the ultrasonic nebulizer and vibrating mesh devices. Each nebulizer was tested in triplicate (n=3) at two different positions, as shown in Figure 2: a first position between the exhalation port and lung model (prior to the Whisper Swivel II), and a second position between the ventilator and exhalation port (after the Whisper Swivel II).
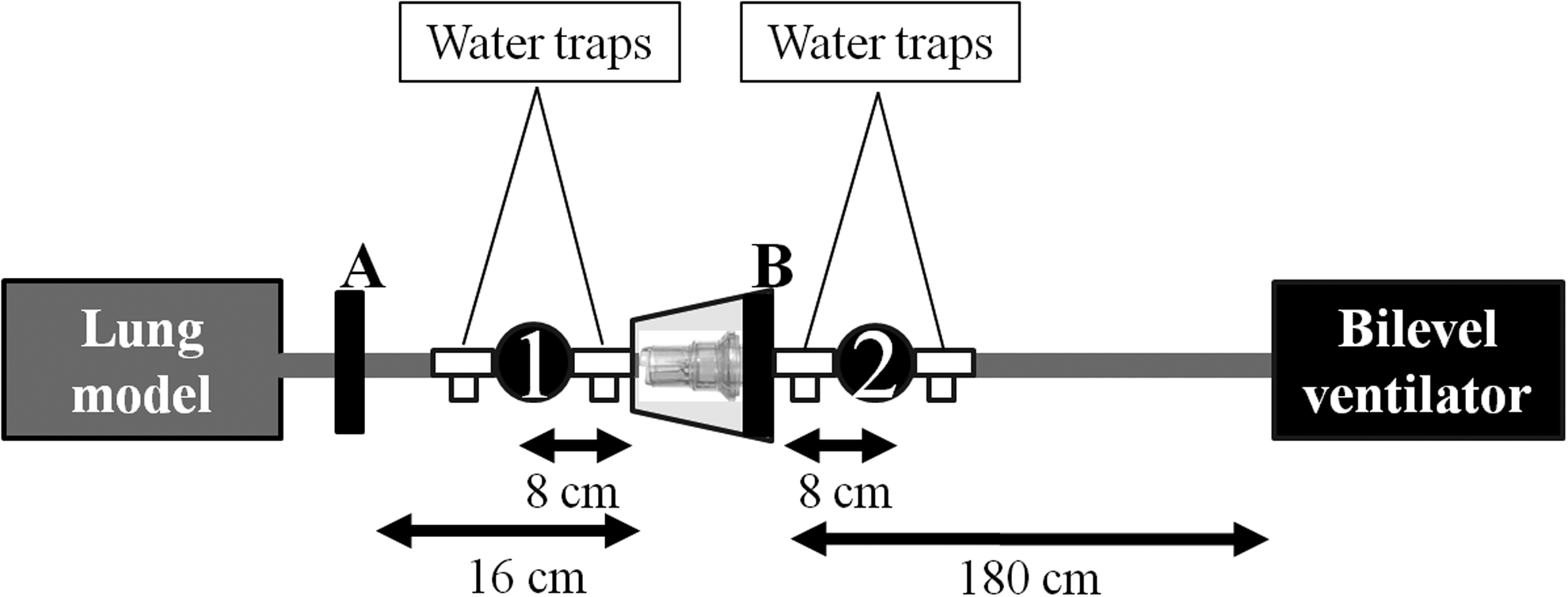
Experimental model with the nebulizer positions. 1: Nebulizer in position between the exhalation port and lung model; 2: nebulizer in position between the ventilator and exhalation port; A: filter measuring the inhaled dose; B: filter measuring the expiratory wasted dose (dose lost through the passive exhalation port).
For each run, a new single-patient use disposable nebulizer (Sidestream, Aeroneb Solo, NIVO), nebulizer cup (Servo Ultra Nebulizer 145), and complete ventilator circuit, including the Whisper Swivel II exhalation port, were used, whereas the multi-patient use reusable nebulizers (Servo Ultra Nebulizer 145 and Aeroneb Pro) and the specific adapters were cleaned and dried after each test according to the manufacturer's instructions. The nebulizations were started 60 sec after the ICU ventilator and the bilevel ventilator were switched on. The nebulizations were considered as finished when there was no visible evidence of nebulization for a period of 30 sec. Ventilator was switched off at least 30 sec after the end of the nebulization time. All the experiments were performed by the same investigators.
Measurements
Each nebulizer was filled with 500 mg of amikacin (Amukin; Bristol-Myers Squibb, Braine-l'Alleud, Belgium) diluted in 4 mL of normal saline.
The mass of amikacin collected on filters during ventilation was quantified using the residual gravimetric method, as described previously by Veccellio et al.(53) The filters were weighed before the test by using a high-precision scale (Mettler AE166; Mettler Instruments, Zurich, Switzerland; 0.0001 g precision). After the nebulization, both filters were dried at ambient room temperature for 24 hr and then weighed again. By subtracting the weight of the filters before and 24 hr after the nebulization, we obtained the inhaled dose (filter 1) and the expiratory wasted dose (filter 2). The relative mass of the amikacin in total solute mass (drug and excipient) of each drug ampoule (1 g/4 mL) used was measured in triplicate. Amikacin solution (100 μL) was placed on a dried filter, which, after 24 hr of drying at ambient room temperature, was weighed again. The relative mass of amikacin was calculated as the ratio between the drug mass deposited on the filter (25 mg) and the difference between the weights of the filters after and before drying (mean±SD: 63.27±0.32%). Inhaled dose and expiratory wasted dose of amikacin were calculated by multiplying the drug mass by the mean relative mass of active compounds. All measurements were performed under the same hygrometric conditions.
The total drug mass lost in the ventilator circuit (including connections, water traps, nebulizer connectors, and tubing) and left in the nebulizer system (residual dose) was estimated by subtracting the inhaled dose and the expiratory wasted dose from the nominal dose of amikacin. This amount of drug was defined as the lost dose (LD). All data were expressed in absolute terms (milligrams) or as percentages of the nominal doses of amikacin.
To evaluate the output performance of the devices, each reservoir was weighed empty, before (filled with amikacin solution), and then after the nebulization. The emitted solution (ES) was defined as the weight of the solution leaving the nebulizer. It was obtained by calculating the difference between the weight of the reservoir before (with the initial charge) and after nebulization. The residual solution (RS) was defined as the solution retained in the nebulizer and was calculated by subtracting the weight of the reservoir empty from the weight of the reservoir after nebulization. Data were expressed in absolute terms (milligrams) or as percentages of the weight of the solution.
Statistical analysis
Results are presented as means±SD. Statistical analysis was performed with the commercially available software Stata (Stata/IC 12.1 for Windows; StataCorp LP, College Station, TX, USA). Statistical differences in inhaled dose, expiratory wasted dose, lost dose, emitted solution, and residual solution between the five models of nebulizers at each position were investigated with one-way analysis of variance. If the test for the homogeneity of variance (Bartlett's test) gave a significant result, the Kruskal-Wallis test was used. When relevant, post-hoc multiple comparisons tests were made using Tukey's test. Paired t tests were performed to assess the differences between the inhaled dose, expiratory wasted dose, and lost dose of each nebulizer at each position. A difference was considered statistically significant when the p value was<0.05.
Results
Influence of nebulizer type on inhaled dose
The inhaled doses for each nebulizer at each position are shown in Table 1. In both positions, there was a significant difference between the nebulizers (p<0.001 at each position).
Means are expressed in absolute terms with SD in parentheses (n=3). IND, inhaled dose; EWD, expiratory wasted dose; LD, lost dose; NomS, nominal solution; ES, emitted solution; RS, residual solution; VAP, Aeroneb Pro; VAS, Aeroneb Solo; VAN, NIVO; PJN, Sidestream; USN, Servo Ultra Nebulizer 145.
In position between the exhalation port and lung model, the inhaled dose was significantly higher with the vibrating mesh nebulizers in comparison with the other devices (p<0.001 for each comparison). No significant difference between the jet and the ultrasonic nebulizers was observed. When we compared the vibrating mesh nebulizers with one another, significant differences were found (p<0.01), except between VAN and VAS.
In position between the ventilator and exhalation port, the vibrating mesh nebulizers and the jet nebulizer delivered significantly higher inhaled dose than the ultrasonic device (p<0.001 for each comparison). Inhaled dose was significantly greater for VAS compared to VAN (p<0.01) and for PJN (p<0.01).
Influence of nebulizer type on expiratory wasted dose
The expiratory wasted doses for the different nebulizers at each position are reported in Table 1. In both positions, there was a significant difference between the nebulizers (p<0.001 at each position).
In position between the exhalation port and lung model, the expiratory wasted dose was significantly higher with the jet nebulizer than with the other nebulizers (p<0.001 for each comparison). VAS and VAP lost significantly more drug through the expiratory port than the ultrasonic device (p<0.001 for each comparison). There was no significant difference between VAN and the ultrasonic device. A significant difference was found between the different vibrating mesh nebulizers (p<0.001), except between VAS and VAP.
In position between the ventilator and exhalation port, the expiratory wasted dose was significantly higher with the vibrating mesh nebulizers than with the other devices (p<0.001 for each comparison) and was similar between the jet nebulizer and the ultrasonic device. There was a statistical difference between VAP and VAS (p<0.01) and VAS and VAN (p<0.01), but no significant difference between VAP and VAN.
Influence of nebulizer type on lost dose
The estimated lost doses for the different nebulizers are reported in Table 1. The results showed a significant difference between the devices (p<0.001 at each position). In both positions, the lost dose was significantly higher with the ultrasonic nebulizer than with the jet or vibrating mesh devices (p<0.001 for each comparison in position between the exhalation port and lung model and p<0.05 for each comparison in position between the ventilator and exhalation port). The amount of drug loss with the jet nebulizer was significantly higher than with the vibrating mesh devices (p<0.001 for each comparison in both positions). When we compared the vibrating mesh nebulizers with one another, significant differences were found in position between the exhalation port and lung model only between VAP and VAS (p<0.01) and VAN and VAS (p<0.05).
Influence of nebulizer type on output performance
Nominal (NomS), emitted (ES), and residual (RS) solutions of the different nebulizers at each position are shown in Table 1. In both positions, only emitted and residual solutions showed a significant difference between devices (p<0.001 at each position).
In position between the exhalation port and lung model, we found significant difference in both emitted and residual solutions between all nebulizers (p<0.01 for each comparison), except between VAS and VAN.
In position between the ventilator and exhalation port, the vibrating mesh nebulizers showed a higher emitted solution than the other devices (p<0.001 for each comparison). The ultrasonic nebulizer produced higher emitted solutions than the jet nebulizer (p<0.001). When we compared the vibrating mesh nebulizers with one another, significant differences were found between VAN and VAP (p<0.05) and between VAS and VAP (p<0.01). Moreover, the residual solution of the ultrasonic nebulizer was significantly lower than for the jet device, whereas the vibrating mesh showed a significantly lower residual solution than the other two devices (p<0.001 for each comparison). No significant difference was found between the three vibrating mesh nebulizers.
Influence of nebulizer position on inhaled dose
Figure 3A shows the inhaled dose for each nebulizer in both positions. In position between the exhalation port and lung model, each nebulizer delivered a higher inhaled dose than in position between the ventilator and exhalation port. The vibrating mesh and the ultrasonic nebulizers delivered approximately 3- to 4.5-fold more drug in position between the exhalation port and lung model than when positioned between the ventilator and exhalation port (p<0.001 for each comparison). The same trend, but in a lower proportion, was observed with the jet device (p<0.05).

Influence of nebulizer position on expiratory wasted dose
Figure 3B shows the expiratory wasted dose for each nebulizer in both positions. The results varied depending on the nebulizer systems. All vibrating mesh nebulizers wasted almost 4- to 20-fold less aerosol through the exhalation port in position between the exhalation port and lung model than in position between the ventilator and exhalation port (p<0.001 for each comparison). The same result was found for the ultrasonic nebulizer with approximately 3-fold less drug lost in position between the exhalation port and lung model (p<0.001). However, an opposite trend was observed for the jet nebulizer, which lost 2-fold more drug in position between the exhalation port and lung model than in position between the ventilator and the exhalation port (p<0.001).
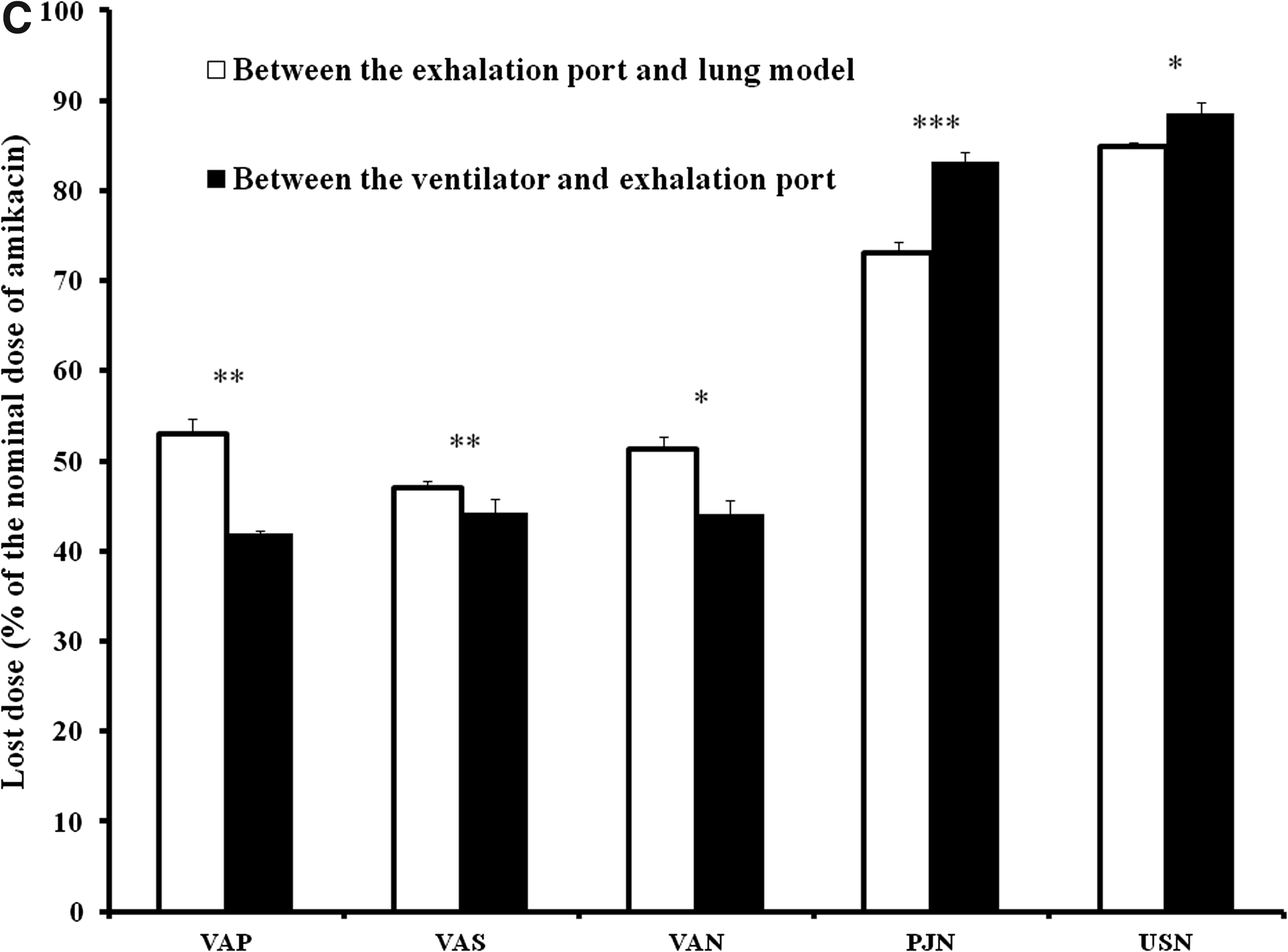
Influence of nebulizer position on lost dose
Figure 3C shows the estimated lost dose for each nebulizer placed in both positions. The ultrasonic device and the jet nebulizer showed opposite results compared with the vibrating mesh nebulizers. The estimated lost dose for the ultrasonic and the jet nebulizers was significantly higher in position between the ventilator and exhalation port than in position between the exhalation port and lung model (p<0.01 and p<0.001 for the ultrasonic and the jet nebulizers, respectively). In contrast, in position between the ventilator and exhalation port, the circuit wasted dose decreased significantly for all the vibrating mesh nebulizers (p<0.001, p<0.05, and p<0.01, for VAP, VAS, and VAN, respectively).
Discussion
To our knowledge, this is the first in vitro study that compares three different types of nebulizer system coupled with a single-limb circuit bilevel ventilator using adult settings. Previous works investigated the influence of nebulizer type and position between vibrating mesh and jet nebulizers,(36,40,45,46,49,50,54) but none evaluated ultrasonic devices. The results of these studies are summarized in Table 2.
Data are means expressed as percentage of the nominal dose of drug (%). IPAP, inspiratory positive airway pressure; EPAP, expiratory positive airway pressure; ND, nominal dose; IND, inhaled dose; EWD, expiratory wasted dose; LD, lost dose; VAN, NIVO; VAS, Aeroneb Solo; VAP, Aeroneb Pro; JN, jet nebulizer; USN, ultrasonic nebulizer; nc, unpublished data; Before, position between the exhalation port and lung model; After, position between the ventilator and exhalation port.
In this study, we showed that there were: (1) significant differences in inhaled and lost doses between nebulizer systems associated to a bilevel ventilator; (2) a significant influence of the nebulizer position on these doses; and (3) significant variability in the inhaled and lost doses between the three vibrating mesh models (see Fig. 4).
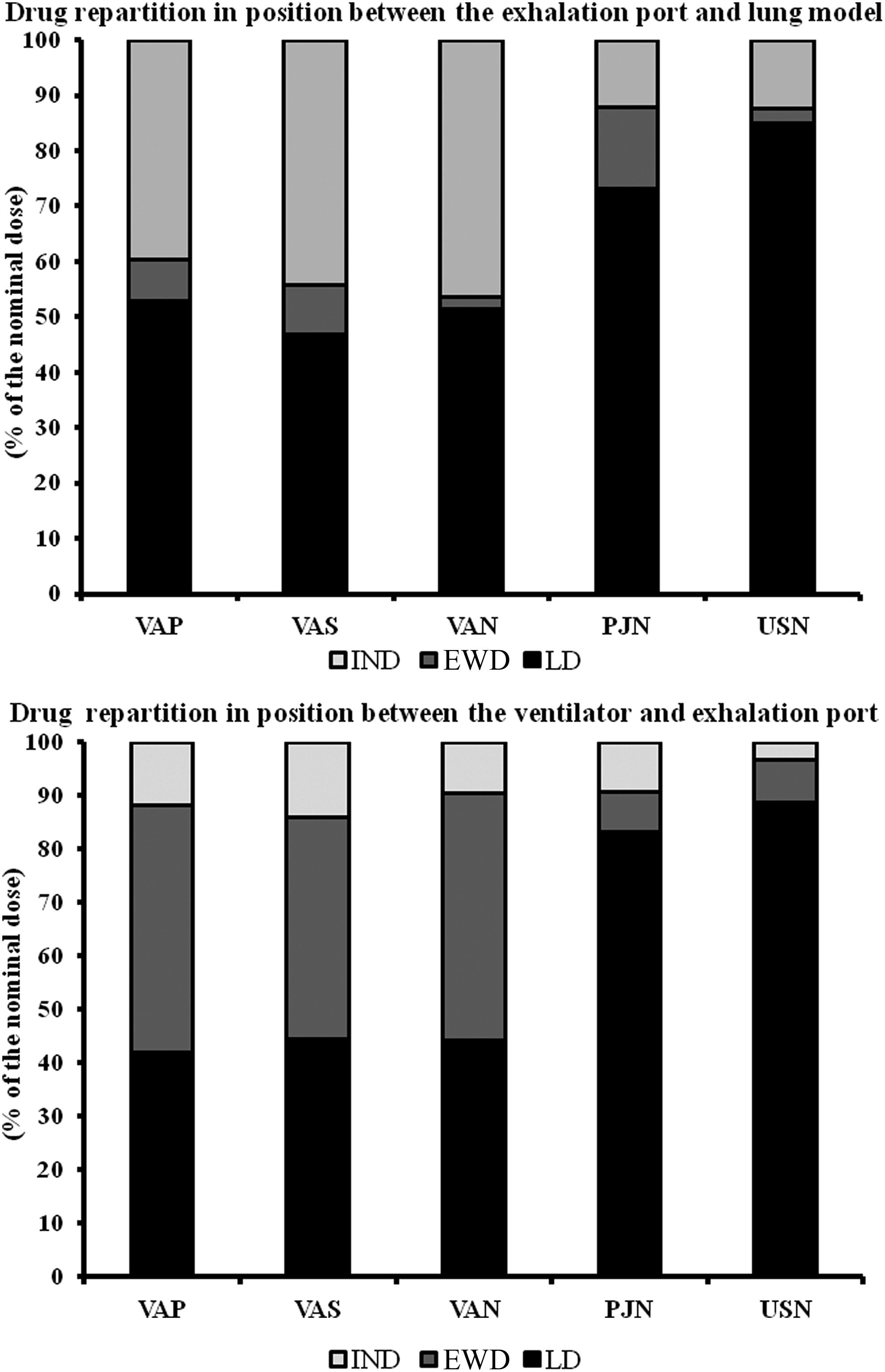
Nebulized drug repartition for the different nebulizers placed in position between the exhalation port and lung model (upper panel) and between the ventilator and exhalation port (lower panel). Means are expressed as percentage of nominal dose of amikacin. IND, inhaled dose; EWD, expiratory wasted dose; LD, lost dose; VAP, Aeroneb Pro; VAS, Aeroneb Solo; VAN, NIVO; PJN, Sidestream; USN, Servo Ultra Nebulizer 145.
When the nebulizers were positioned between the exhalation port and lung model, we observed that the vibrating mesh nebulizers delivered approximately 3-fold more inhaled dose than the other devices. This higher efficiency has been already reported in two previous studies.(49,54) Indeed, Abdelrahim et al.(49) showed that the Aeroneb Pro delivered approximately 2-fold more inhaled dose of terbutaline than the Sidestream. More recently, McPeck et al.(54) found an approximately 4-fold increase in inhaled dose with the NIVO compared with a jet nebulizer at IPAP/EPAP of 15/8 cm H2O. These results are in agreement with our findings, which show that the NIVO delivered higher inhaled dose than the jet nebulizer at IPAP/EPAP of 20/5 cm H2O. The higher efficiency of vibrating mesh devices was also reported in intubated and mechanically ventilated lung models.(19,30,48,55–57) However, it is difficult to extrapolate these findings to spontaneous models using a specific noninvasive ventilator. Indeed, the leak port and the higher turbulence generated by the high gas flow in the single circuit may probably increase drug loss in the environment and inertial impaction in the circuit, and thus affect inhaled drug delivery.(14,15,36,58,59)
We speculate that the differences in the inhaled dose observed between the vibrating mesh nebulizers and the other devices might be due to the output efficiency of the different nebulizer systems.(30,49) As shown previously, the vibrating mesh and ultrasonic devices emitted more solution than jet nebulizers in a position between the exhalation port and lung model.(15,26,56,60,61) At the same time, the inhaled dose, expressed as a percentage of emitted solution, was approximately 2-fold higher with the vibrating mesh than with the jet nebulizer and approximately 3-fold higher than with the ultrasonic device. Despite the ultrasonic device providing approximately 20% more emitted solution than the jet nebulizer, the inhaled dose of both was similar. These results are in contrast with previous studies(12,14,61–63) showing that, during mechanical ventilation, ultrasonic devices had higher inhaled dose than jet nebulizers. In addition, we observed that the ultrasonic nebulizer lost 5.6-fold less expiratory wasted dose than the jet nebulizer. Therefore, we suspected that a greater dose of amikacin was lost in the circuit (including the nebulizer). Indeed, the estimated lost dose was approximately 12% greater than with the jet device. Based on previous findings, several factors including droplet size,(25,57,64) nebulization time,(25) gas flow used to power jet nebulizer, and evaporative water loss(25,64–66) may have contributed to influence the drug loss.
Moreover, when positioned between the expiratory port and lung model, the jet nebulizer had an expiratory wasted dose significantly higher than the vibrating mesh devices. Abdelrahim et al.(49) likewise found the same results with the same nebulizers. However, the difference between both devices was more notable. We speculate that the difference is due in part to several ventilator-related factors(30,39,46) (e.g., higher amount of air leakage with the Whisper Swivel II compared with single-arch exhalation port, high bias flow) and drug-related factors(67) (e.g., higher viscosity of amikacin compared with terbutaline) that affect drug delivery.
Similar to previous findings,(50,68) we found significant performance variability among our vibrating-mesh models. At position between the exhalation port and lung model, the inhaled dose with the Aeroneb Solo and NIVO was significantly higher than with the Aeroneb Pro. One potential explanation is the low residual volume of the Aeroneb Solo and NIVO. The conical shape of both devices seems to allow a better emitted solution through the nebulizer system. Indeed, we reported, respectively, 2.8-fold and 2.4-fold lower residual volume than for the Aeroneb Pro. Another potential explanation is that Aeroneb Solo and NIVO (disposable nebulizers) were changed after each run, whereas Aeroneb Pro (reusable nebulizer) was reused after it was cleaned and dried according to the manufacturer's instructions. A problem of aperture obstruction(69) associated with the use of high-viscosity drug(67,70) could have affected the performance of the Aeroneb Pro and led to the high variability of its emitted solution. However, our findings differ from those of White et al.(50) who found approximately 2-fold higher inhaled dose with the NIVO than with the Aeroneb Solo during simulated pediatric noninvasive ventilation (NIV). The difference with our results may be explained by two reasons. Firstly, we placed both nebulizers at position between the exhalation port and lung model, whereas White et al.(50) positioned the NIVO between the exhalation port and mask and the Aeroneb Solo between the ventilator and exhalation port. Secondly, unlike our model, they used a heated humidification system. These factors could have increased drug loss, and thus affected inhaled dose delivered with Aeroneb Solo.(24,48)
Similar to some previous studies,(36,45,49) we found the highest inhaled dose when all types of nebulizer were positioned between the exhalation port and lung model. However, Calvert et al.(40) reported higher inhaled dose with a jet nebulizer placed between the ventilator and exhalation port. We speculate that this difference may be due to the fact that Calvert et al.(40) interrupted the nebulization after 5 min. In our study, all nebulizers were operated until the end of aerosol generation (no visible evidence of nebulization) with a higher nebulization time for the jet nebulizer (mean=21±1.6 min). The evaporation of the solvent over time could have led to an increase in the concentration of drug solution in the reservoir(24,71,72) and, hence, the viscosity that further reduces drug nebulization.(73,74) Moreover, Calvert et al.(40) maximized drug delivery by using a longer inspiratory time and lower flow rate(36,75) (high I/E ratio, high tidal volume, and low respiratory rate).
In their study, Abdelrahim et al.(49) reported that the amount of drug expelled through the exhalation port with a jet nebulizer and Aeroneb Pro was greater when the devices were positioned between the ventilator and exhalation port. Our data confirmed their findings regarding the Aeroneb Pro, but differ regarding the jet nebulizer. This difference may be explained by several factors: (1) The high level of IPAP set in regard to the type of exhalation port (Whisper Swivel II versus single-arch exhalation port): the leak through the Whisper Swivel II being proportional to pressure, high-level pressure may have increased drug loss in the environment.(46) (2) The ventilator characteristics (Philips Trilogy 100 versus Nippy 2): the high level of bias flow may have increased the clearance rate of aerosol.(30) (3) The physical properties of the nebulized drug (amikacin versus terbutaline): the high viscosity of amikacin may have affected the nebulizer mechanism and thus reduced output rate.(70) Moreover, our results showed that the expiratory wasted dose with the vibrating mesh nebulizers was highly influenced by their position. Indeed, the drug lost through the exhalation port increased by more than 33% when the nebulizers were placed between the ventilator and the exhalation port compared with position between the exhalation port and lung model. At the same time, the amount of drug lost in the circuit (including the nebulizer) decreased by 21%, 5.6%, and 14% with Aeroneb Pro, Aeroneb Solo, and NIVO, respectively.
These results raise the question of the relevance of positioning vibrating mesh nebulizers between the ventilator and exhalation port. Indeed, these devices lost their advantage of higher drug delivery compared with the jet nebulizer. Moreover, when placed between the ventilator and exhalation port, the vibrating mesh nebulizers produced higher expiratory wasted dose, which would increase environmental exposure to drug. However, these results may be due to the fact that our settings maximized drug delivery (high-output nebulizers, dry circuit, high level of IPAP, and low level of EPAP) during NIV using a Whisper Swivel II that increases aerosol loss with high inspiratory pressure.(46) Thus, it is difficult to extrapolate from these findings to other settings and types of exhalation port.
Some limitations should be considered when interpreting the results of our study. Firstly, we used single ventilator settings and breathing parameters, and only one type of exhalation port. These configurations do not fully reflect all the possible clinical situations. Therefore, we cannot comment on the effects of changes in IPAP/EPAP levels, breathing characteristics, and the influence of other types of exhalation port, including interface with an integrated leak port, on aerosol delivery. Secondly, we did not use a humidifier because it is an important factor affecting aerosol delivery.(14,39) Hence, the results may not be extrapolated to NIV with heated humidifier. Thirdly, the inhaled drug collected on filters represents the inhaled dose and not the lung deposition that contributes in part to the clinical response to nebulization. Fourthly, the efficiency of aerosol delivery may be affected by the properties of the drug solution and the nebulizer brands tested.(33,70) The results may not be applied to the same nebulizers used with other medications or to other nebulizers.(31,70)
In conclusion, with a bilevel ventilator including a single-limb circuit with a Whisper Swivel II exhalation port, the vibrating mesh nebulizers deliver a higher amount of amikacin than jet and ultrasonic nebulizers irrespective of their position in the circuit. However, to decrease the amount of lost dose, especially through the leak port with the vibrating mesh nebulizers and in the circuit with the jet and ultrasonic devices, we recommend the placement of nebulizers between the patient and exhalation port. Our findings on the expiratory wasted dose raise the question of whether a breath-synchronized nebulization option may influence the inhaled dose during NIV, especially with the vibrating mesh nebulizers.
Due to their low performance compared with mesh nebulizers, we do not recommend using ultrasonic devices with a single-limb circuit bilevel ventilator.
The results of this study suggest that, with different types of nebulizers, an appropriate position should be carefully chosen to ensure optimal clinical efficacy and reduce aerosol loss in the environment, especially when toxic or expensive drugs are nebulized. However, additional research should be performed to determine if these in vitro results are clinically relevant.
Footnotes
Acknowledgments
Special thanks are given to Miss Eveline Frei for her assistance in manuscript writing and to Mr. Bernard Landry and Ian Mantripp for revising the manuscript.
Author Disclosure Statement
The authors declare there are no conflicts of interest.