
Abstract
Abstract
Purpose:
A new approach to delivering high doses of dry powder medicaments to the lung is presented. The Orbital® dry powder device is designed to deliver high doses of drugs to the respiratory tract in a single dosing unit, via multiple inhalation maneuvers, overcoming the need to prime or insert multiple capsules.
Methods:
The Orbital was tested in its prototype configuration and compared with a conventional RS01 capsule device. Three formulations were evaluated: 200 mg of spray-dried ciprofloxacin formulation for respiratory infection, 200 mg of spray-dried mannitol formulation for mucus clearance, and 100, 200, and 400 mg of co-spray-dried 1:8 formulations containing ciprofloxacin and mannitol as combination therapy. The systems were evaluated in terms of physicochemical properties and tested using a multistage liquid impinger at 60 L/min. Emptying rates were evaluated, and the aerosolization performance compared with 10 capsules used sequentially in the RS01.
Results and Discussion:
The systems were different in terms of morphology, thermal response, moisture sorption, and stability; however, they had similar sizes when measured by laser diffraction, making them suitable for comparison in the Orbital and RS01 devices. The aerosolization performance from the Orbital device and RS01 was dependent on the formulation type; however, the fine particle fraction (FPF) produced by the Orbital device was higher than that by the RS01. The FPFs for ciprofloxacin, mannitol, and co-spray-dried formulation were 67.1±1.8, 47.1±2.2, and 42.0±1.8, respectively. For the Orbital, 90% of the loaded dose was delivered within 10 inhalation maneuvers, with the profile being dependent on the formulation type.
Conclusion:
The Orbital provides a means of delivering high doses of medicine to the respiratory tract through multiple breath maneuvers after a single actuation. This approach will allow the delivery of a wide range of high-payload formulations (>100 mg) for the treatment of a variety of lung disorders. To date, no such passive device exists that meets these crucial criteria.
Introduction
D
Although these devices are suited to deliver low-dose molecules, such as β2-agonists and corticosteroids (microgram quantities), they lack the capacity to deliver higher-dose medicaments such as antibiotics,(3) phospholipids,(4,5) or mucociliary clearance enhancers(6,7) (milligram quantities).
For example, the only currently marketed inhalation antibiotic DPI is Novartis's TOBI Podhaler® with a 112-mg dose. This formulation has been shown to be well tolerated in patients with cystic fibrosis(8); however, the product requires the patient to actuate and inhale four separate capsules of 28 mg each. For treatment of mucus obstruction, Pharmaxis has developed Bronchitol®, a 400-mg inhaled dry powder formulation.(9) However, again this requires the inhalation of 40-mg mannitol aliquots from 10 capsules using a conventional DPI.
Ultimately, the “load-prime-inhale-empty-load-prime…” routine for higher-dose inhaled formulations is time consuming and thus may result in poor patient compliance in the long term, precluding these products from use outside niche disease indications.(10,11)
One of the rate-limiting steps in the realization of high-dose inhalation therapy is in the device itself. Best intentions aside, the majority of companies working in this space have modified existing capsule inhaler DPI technology to incorporate engineered drug microparticulate systems, rather than building the device from the ground up, focusing on the required dose. Examples where devices have been designed specifically for higher doses include the pressurized aerosol dry-powder delivery (PADD) device, developed by Britannia Pharma, for the delivery of 250 mg of surfactant therapy.(4) This device was shown to be capable of delivering highly cohesive mixtures of dipalmatidylphosphatidylcholine and unsaturated phosphatidylglycerol (7:3 ratio) with fine particle fractions (FPFs) in excess of 30%. Unlike regular DPIs, the PADD was classified as an active device and required an 8–14-bar disposable power source. In the passive DPI devices field, there is still nothing commercially available to meet these dose requirements, although devices such as the Twincer® may be capable of reaching the low end (∼50 mg) of these dose regimes.(12)
The most immediate application of high-dose inhalation therapy is in the promotion of mucociliary clearance and treatment of local lung infection. Respiratory infection is the number one cause of death worldwide,(13) usually a consequence, albeit terminal, of other disease state, like chronic obstructive pulmonary disease and cancer, and results in bacterial or viral colonization in the lungs with associated hypermucosal secretion. Current therapies require multiple dosing via oral or intravenous medication,(14) with limited treatment options being available to the medical practitioner. Antibiotics and mucociliary clearance agents need to be delivered as “high-dose” medicaments (up to 400 mg),(6,15–19) and thus an approach to achieving this in a single unit dose would be advantageous.
Here, the authors present a new approach to delivering high-dose inhalation medicines via a passive (breath-actuated), premetered multi-inhalation dry powder device (Orbital®) (Fig. 1). This new device allows the administration of high drug doses of up to 400 mg, with multiple inhalation maneuvers. The Orbital device is a single-use, disposable unit containing a “puck” that holds up to 400 mg of drug powder. After actuation, by pushing the puck into the deagglomeration chamber, the patient inhales as he or she would do a normal DPI device and the drug powder is forced, centrifugally, out through one (or multiple) orifices in the puck, into the deagglomeration chamber, where the rotating puck classifies the powder into an inhalable size before it is delivered into the respiratory tract. A key innovative step in the Orbital design is the puck orifice that acts as the rate-limit step for release of powder. Thus, it becomes possible for the patient to inhale a fixed dose over a series of inhalation maneuvers rather than receiving a single 400-mg bolus.
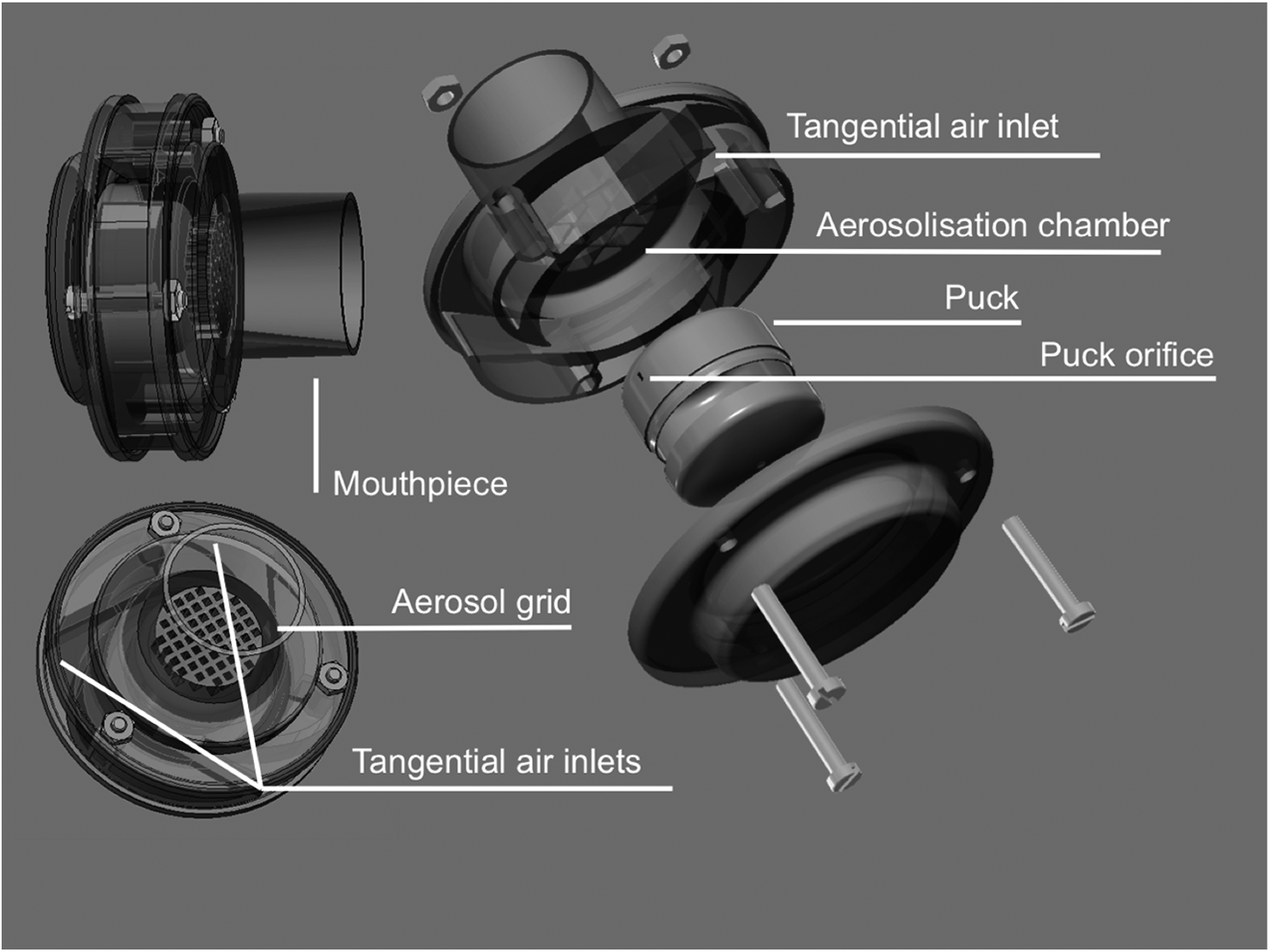
Diagram of the Orbital DPI device.
To assess the performance of the Orbital, three drug particulate systems were engineered and studied: mannitol, the antibiotic ciprofloxacin, and a formulation containing ciprofloxacin co-spray-dried with mannitol in a 1:8 ratio. This third formulation was designed to study the potential of delivering co-engineered microparticles for treatment of local infection while simultaneously enhancing mucociliary clearance. This specific ratio was chosen because a current clinical trial underway by Bayer Ltd. is evaluating a 32.5-mg dose of ciprofloxacin incorporated into a 50-mg PulmoSphere® powder delivery system(20,21); a 1:8 ratio ciprofloxacin-HCl:mannitol used here would be equivalent to a ciprofloxacin dose of 22.5–45 mg, when delivered with high doses of mannitol (∼200–400 mg), as used in Bronchitol for cystic fibrosis.
The inhalation particle systems were characterized in terms of their physicochemical properties and were evaluated for aerosol performance using the Orbital and compared with a commercially available capsule-based DPI (RS01®).
Materials and Methods
Materials
Ciprofloxacin hydrochloride (referred to as ciprofloxacin hereafter) was obtained from MP Biomedicals (Sydney, Australia). Mannitol (Pearlitol® 160C) was obtained from Roquette (Lestrem, France). Experiments were conducted using high-purity water (18.2 MΩ.cm, MilliQ; Merck Millipore, Billerica, MA). All solvents were of analytical grade from Thermo Fisher Scientific (Sydney, Australia). Sodium phosphate monobasic dihydrate was purchased from Sigma Aldrich (Sydney, Australia). The RS01 and Orbital DPI devices (Fig. 1) were supplied by Pharmaxis Ltd. (Sydney, Australia).
Construction and operation of the inhaler devices
The prototype Orbital device (Fig. 1) consists of three parts that can be stacked and assembled together by the operator. The drug is contained in a transparent, sealed plastic cylindrical cup, named the “puck,” with a hole located on the side to allow powder emission. The ratio of the diameter of the discharge hole to that of the dosing puck can be varied to control the residence time for the powder in the puck, and the efficiency by which particles are retained. In this study, the aerosol efficiency of the standard prototype configuration, with one hole (1.01-mm diameter), was evaluated.
The puck has a dose capacity ranging from 100 mg up to 400 mg, depending on the density of the powder. The puck is placed in the center compartment of the device. Upon inhalation, air is drawn in through the three tangential air channels positioned around the diameter of the device where the puck is located. The large flow of circulatory air through the powder compartment causes the puck to rotate, resulting in particle emission, subsequent puck-particle-wall collisions, and powder aerosolization.
In comparison, the RS01 is a single-dose commercial passive device used for the delivery of many proprietary inhalation formulations (i.e., Bronchitol and Aridol, both Pharmaxis Ltd.). It uses size 3 hydroxypropylmethylcellulose (HPMC) or gelatin capsules as a dose delivery system. The capsule is placed in the appropriate loading chamber located at the base of the device, and then pierced using one metal pin located on either side of the chamber. Upon patient inhalation, the powder is then drawn from the capsule through the device at a steady flow rate via a tangential flow rate. The RS01 is advantageous because of its compact size and simplicity of use. Depending on powder density, the size 3 capsules can usually hold a maximum amount of ∼30 mg of dry powder per capsule.
Production of the model inhalation particle systems
Ciprofloxacin, mannitol, and a combination of ciprofloxacin and mannitol in a ratio of 1:8 w/w were dissolved in water to obtain a concentration of 10 mg/mL for all three samples. Each solution was sonicated for 3 min and filtered using 0.45-μm filters. The solutions were spray-dried using a BÜCHI B290 spray dryer (Flawil, Switzerland) in an open-loop configuration with the following settings: inlet temperature of 160±2°C, outlet temperature of 75±2°C, feed rate of 6%, aspiration pressure of 800 kPa, and aspiration rate of 47.6 m3/hr. The resultant spray-dried powders were collected and stored in a desiccator at room temperature prior to use.
Physicochemical characterization of the model inhalation particle systems
Electron microscopy
Each powder was deposited on carbon adhesive-coated aluminum stubs and sputter coated with gold (thickness 10 nm) at an electric potential of 25 mA for 2 min, under argon gas. The morphological examination of each powder was conducted at high vacuum using a Zeiss Ultra Plus scanning electron microscope (Sydney, Australia) at 3 keV.
Particle size analysis
Particle size distribution of each spray-dried sample was determined by laser diffraction (Mastersizer 3000; Malvern, Worcestershire, UK) using a dry dispersion unit (Aero S). Measurements were performed by placing 200 mg of each sample in the feeder under a dispersion pressure of 4 bar, a flow rate of 40 L/min, and a feed height of 2.5 mm. Samples were measured using a refractive index of 1.52 determined using a refractometer (Thermo Spectronic 334610; Thermo Fisher Scientific, Waltham, MA). Experiments were performed in triplicate.
X-ray powder analysis
A D5000 Siemans X-ray powder diffractometer (Karlsruhe, Germany) was used to study the crystallinity of the powders. The operating conditions were: temperature of 25°C, diffraction 2θ angle of 5–40°, step time of 1 sec, and step size of 0.04°.
Differential scanning calorimetry (DSC)
The thermal response of each powder to a temperature ramp was investigated using DSC. Approximately 5 mg of each sample was placed in a sealed 40-μL aluminum crucible and scanned using a Mettler Toledo DSC 1 (Melbourne, Australia) between 40°C and 400°C at a heating rate of 10°C/min. Exothermic and endothermic peak temperatures, onset temperature, and heat of enthalpy (ΔH) were determined using STARe software V.9.0x.
Dynamic vapor sorption (DVS)
The moisture sorption behavior of each sample was studied using a DVS-Intrinsic (Surface Measurement Systems, Alperton, Middlesex, UK). Samples (∼10 mg) were weighed into metal pans and exposed to a continuous flow (270 mL/min) of nitrogen carrier gas, from 0% to 90% relative humidity (RH) (at 25°C), at 10% RH increments for two cycles. Equilibrium moisture content at each humidity step was determined by a mass rate (dm/dt) of 0.002% min–1.
Chromatographic assay methodology for drug assay quantification
Ciprofloxacin and mannitol were analyzed using two validated high-performance liquid chromatography (HPLC) methods using a Shimadzu ULPC system equipped with LC20AD Liquid chromatograph, SPD 20A UV detector, RID 10A refractive index detector, SIL 20A Autosampler, DGU 20A degassing unit, and CTO 20A column oven with Lab Solutions software (Shimadzu, Sydney, Australia).
For the ciprofloxacin, the UV detector was set at 275 nm, and a reverse-phase stationary column Nova-Pak C18 (3.9×150 mm i.d.; Waters, Milford, MA) was used with an injection volume of 100 μL and a flow rate of 1 mL/min. The column oven was set at 24°C, and a mixture of methanol:water (30:70 v/v) with 0.1 M sodium phosphate monobasic dihydrate, adjusted to pH 3.35 with phosphoric acid, was used as the mobile phase. A calibration curve was constructed using standard solutions of ciprofloxacin in the range of 0.1 to 50 μg/mL (R2=0.9999). The retention time of ciprofloxacin was ∼3.4 min. For the quantification of mannitol, the refractive index detector was used. Samples were injected into the HPLC system onto a Resolve C-18 column (5 μm, 150×3.9 mm; Waters) with deionized water as the mobile phase. The HPLC was set to a flow rate of 1 mL/min and injection volume of 100 μL, resulting in a retention time of 4 min. Linearity was obtained with concentrations ranging from 0.05 to 10 mg/mL (R2=0.9999). The retention time of mannitol was 1.6 min. In vitro aerosol mass deposition of ciprofloxacin and mannitol microparticulates was measured using their respective HPLC methods, whereas the co-spray-dried system was analyzed using the ciprofloxacin method, because it had higher sensitivity and ciprofloxacin was the smaller component.
Comparison of drug aerosolization efficiency from the Orbital and RS01 devices
The in vitro aerosolization properties of each formulation were determined using a Multi-Stage Liquid Impinger (MSLI; Westech, Bedfordshire, UK). Although not accepted by the U.S. Food and Drug Administration for DPIs,(22) the MSLI (USP Apparatus 4) was deemed the most suitable impactor methodology, because previous studies have shown the failure of Anderson (USP Apparatus 3) and Next Generation (USP Apparatus 5) impactors using the doses studied here.(7,23)
In general, stages 1 to 4 of the MSLI were filled with 20 mL of water, and a cellulose filter (A/E glass; Pall Corp., Port Washington, NY) was placed on stage 5. The flow rate through the MSLI was set to 60 L/min using a flow meter (TSI, Shoreview, MN). As described by the European Pharmacopoeia,(33) under these conditions the effective cutoff diameters for MSLI stages 1 to 4 are 6.8, 3.1, 1.7, and 0.26 μm, respectively, with stage 5 as a terminal filter.
Evaluation of the three formulations was conducted using both the Orbital device and RS01. A total dose of 200 mg was chosen to compare the two devices. For the RS01 (Resistance RS01=0.018–0.023 kPa1/2/L min–1), this dose consisted of 10×20 mg (±0.5 mg) capsules, whereas for the Orbital device (Resistance Orbital without puck=0.039 kPa1/2/L min–1), single pucks were filled with 200 mg (±2 mg).
Specifically, for the RS01, 10×size 3 HPMC capsules (CAPSUGEL, Bella Vista, NSW, Australia) were loaded with 20±0.5 mg of powder. Single capsules were inserted into the device, and this was fitted to the MSLI induction port using an adaptor, primed, and tested at a flow rate of 60 L/min for 4 sec, set using a calibrated mass flow controller (Model 4040; TSI Instruments, Singapore). The RS01 device was then removed, the capsule stored for analysis, and a second capsule inserted before repeating this procedure for 10 consecutive capsules to achieve a total dose of 200 mg. After all 10 capsules were tested, samples from each stage of the MSLI were collected, diluted to an appropriate volume with mobile phase for chemical analysis, and assayed using HPLC. Similarly, the induction port, filter stage, capsules, and device were washed into separate volumetric flasks, diluted, and tested using HPLC. This procedure was repeated in triplicate for each powder.
For the Orbital device, 200±2 mg of powder was weighed into the puck, which was then sealed and placed into the Orbital's aerosolization chamber. The device was weighed, placed into the induction port of the MSLI, and then tested at 60 L/min for 4 sec. After testing, the Orbital device was reweighed and the delivered mass calculated from the weight difference. The Orbital was then retested in the MSLI and the process repeated for a maximum of 20 times or until the weight difference between the two recorded values was 2 mg or less (i.e., 1%). At the end of the testing protocol, the Orbital was disassembled and the puck and orbital components washed separately for HPLC analysis, along with the MSLI stages and induction port as described previously.
In addition, the co-spray-dried formulation, containing 1:8 ciprofloxacin:mannitol was tested across a range of doses (100, 200, and 400 mg total puck fill weights) to evaluate the influence of target delivered dose on aerosolization performance in the Orbital.
The MSLI and device recovery data from HPLC analysis were processed to report device and MSLI stage deposition, total loaded dose (LD=induction port, MSLI stages, and device components), emitted dose (ED=induction port and MSLI stages), fine particle dose (FPD; defined as particles with an aerodynamic diameter≤6.8 μm; i.e., stage 3 filter), and FPF (i.e., FPD/LD×100). Additionally, the cumulative mass data collected across the MSLI stages were treated using log-probability analysis to produce mass median aerodymanic diameter (MMAD) values and geometric standard deviations (GSDs).
Statistical analysis
Data were analyzed using one-way analysis of variance (ANOVA) followed by the Tukey's post hoc test. Differences were considered statistically significant at a level of p<0.05.
Results and Discussion
Physicochemical characterization of the model inhalation particle systems
To suitably evaluate the Orbital DPI device, three high-dose formulations were chosen, namely: (1) an antibiotic powder to reduce respiratory infection; (2) a mannitol powder to enhance mucociliary clearance; and (3) a novel co-spray-dried formulation of the two with a view to simultaneously treat infection and enhance mucus clearance in patients with lung infections, like chronic obstructive pulmonary disease or cystic fibrosis. To study the Orbital device, however, each of the engineered powders had to first be characterized in terms of their physicochemical properties.
Electron microscopy
Electron micrographs of the spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles are shown in Figure 2A, B, and C, respectively. All particles had spherical morphology; however, the ciprofloxacin particles presented a dimpled surface morphology similar to that reported in a previous study.(24) In comparison, the morphology of spray-dried mannitol was smooth with characteristic submicrometer crystal formation across the surface.(24) This observation was similar to those of previous studies where mannitol particles were produced from aqueous solutions at a slightly lower inlet temperature of 120°C.(24,25) The co-spray-dried formulation presented a surface morphology similar to that of mannitol, but the surface appeared smoother. Such observations suggest that the overall particle morphology was dictated mostly by the presence of mannitol that was present in larger quantities, with the ciprofloxacin accumulating most probably at the interface, as a smooth amorphous layer. Ciprofloxacin hydrochloride is soluble in water (30 mg/mL),(26) whereas mannitol is freely soluble.(27) Furthermore, mannitol has a lower molecular weight (182.2) than ciprofloxacin hydrochloride (367.8). Subsequently, it is hypothesized that ciprofloxacin would accumulate at the air–liquid interface during the spray-drying process due to its higher molecular weight and relative lipophilicity.

Scanning electron microscopy images of
Particle size analysis
The particle sizes of the spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles are shown in Figure 3. In general, all powders had size distributions suitable for inhalation drug delivery,(28) with the ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol powders presenting median volume diameters of 2.7±0.1 μm, 3.4±0.2 μm, and 2.9±0.1 μm, respectively.
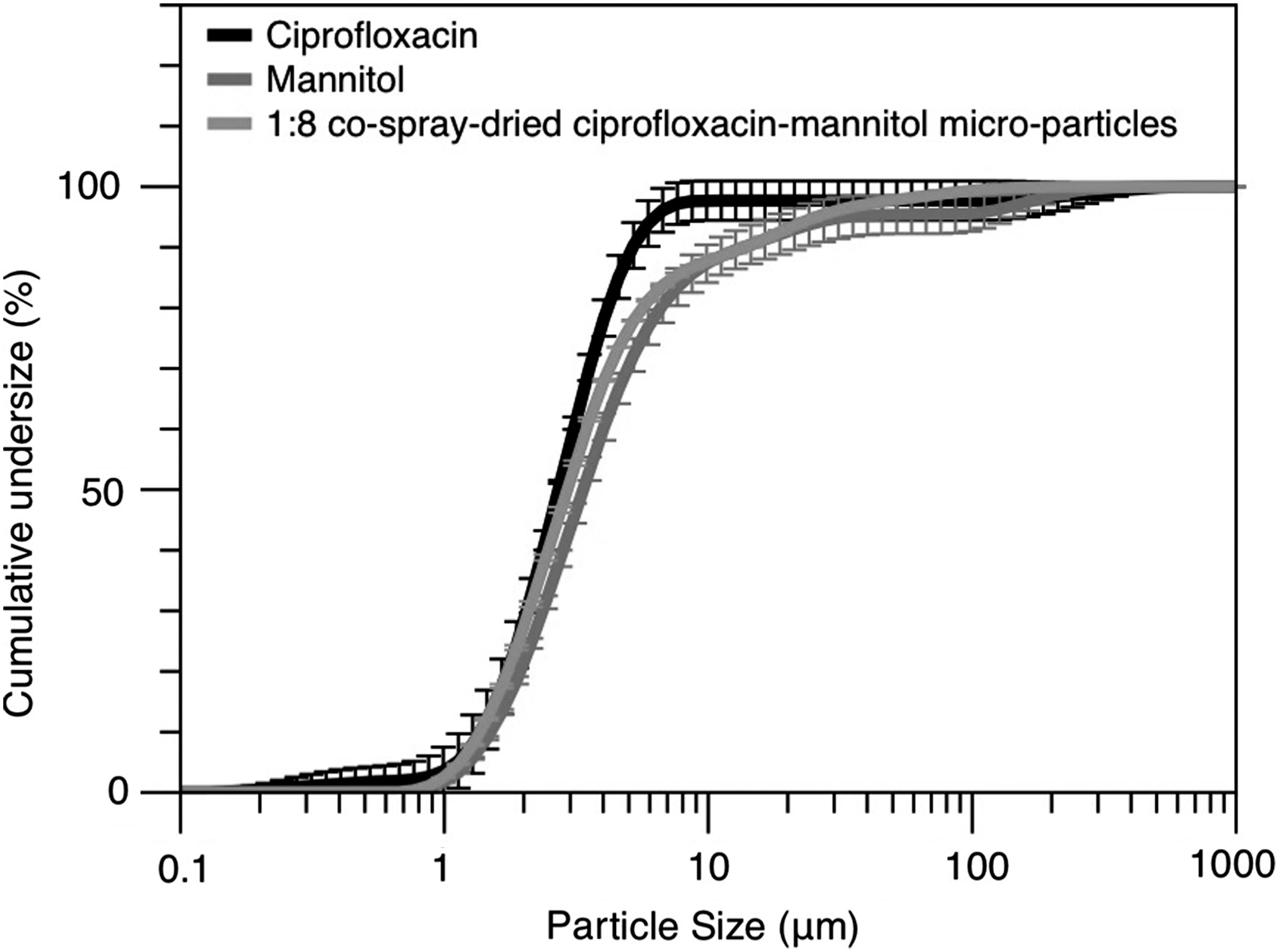
Particle size distributions of the spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles.
X-ray powder diffraction analysis
The X-ray powder diffraction patterns for spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles are shown in Figure 4. In general, the diffraction pattern for the ciprofloxacin microparticles showed a single diffuse halo, representative of a predominantly amorphous structure. Such observations are in good agreement with previous studies of aqueous spray-dried ciprofloxacin.(24,29) In comparison, the diffraction pattern for the spray-dried mannitol microparticles had sharp peaks characteristic of ordered crystal structure. D-Mannitol has three polymorphic forms: α, β, and δ.(30) In general, the diffraction patterns for the raw diffractogram of spray-dried mannitol showed specific peaks corresponding to the α form with peaks at 9.6, 13.8, and 17.3.(31) Additionally, a small peak was observed at 14.7 corresponding to the relative intense peak observed in the β form.(31) Such observations suggest the spray-dried mannitol to be a mixture of both α and β forms. In comparison, the co-spray-dried formulation containing 1:8 ciprofloxacin:mannitol only showed peaks that were attributed to the α form. The lack of new peaks in this spray-dried sample suggests that ciprofloxacin remains in the amorphous state in this system.
X-ray powder diffraction of the spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles.
Differential scanning calorimetry
The DSC thermograms of spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles are shown in Figure 5. In general, the spray-dried ciprofloxacin microparticles exhibited an exothermic peak at 179.5°C, which can be attributed to an amorphous-crystalline phase transition, followed by an endothermic peak of melting at ∼323°C, followed by decomposition.(24) In comparison, the spray-dried mannitol microparticles exhibited an endothermic peak at 165.6°C, which could be attributed to melting of the crystalline form.(32) Such observations support the X-ray powder diffraction data.

DSC thermograms of spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles.
The 1:8 co-spray-dried ciprofloxacin:mannitol microparticles exhibited a DSC profile similar to that of the spray-dried mannitol. This observation is expected, because the co-spray-dried particulate system contained 89% mannitol. Furthermore, it is likely that the endothermic melt would cosolubilize any amorphous ciprofloxacin present in the sample, thus removing any exothermic crystallization phenomena.
DVS studies
The moisture isotherms for spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles are shown in Figure 6. In general, the moisture sorption rank order was: ciprofloxacin>co-spray-dried>mannitol. Specifically, the ciprofloxacin microparticles had a large hysteresis between the sorption and desorption cycles. During the first sorption cycle, an increase in mass of ∼11% was observed, between 0 and 60% RH, before water was expelled at 70% RH, indicating an amorphous-crystalline transition. The mass loss on desorption did not return to 0% but rather 4%, indicating that significant water was retained in the crystallized sample. In comparison, the mannitol microparticles indicated a stable, fully reversible, moisture sorption isotherm with a maximum moisture uptake of 0.3% at 90% RH. The 1:8 co-spray-dried ciprofloxacin:mannitol microparticles had a moisture sorption profile similar to that of the mannitol alone, because the particles consisted of 89% mannitol; however, the maximum moisture sorption was higher (1.9% at 90% RH), and a water retention mass of 0.2% upon drying did indicate possible crystallization of the ciprofloxacin component at elevated humidities.
Moisture sorption isotherms of sorption (●) and desorption (■) of spray-dried (– –) ciprofloxacin, (……) mannitol, and (–––) co-spray-dried ciprofloxacin:mannitol microparticles.
In general, the physicochemical analysis of the three particle systems indicated them to be of suitable size for DPI delivery; however, they were very different in terms of structure and stability. Ciprofloxacin was predominately amorphous and thus less stable than mannitol, whereas the co-spray-dried particle had many features representative of the mannitol alone. Thus, the three inhalation particle systems provide relative extremes in terms of powder properties for study in the Orbital device.
Comparison of drug aerosolization efficiency from the Orbital and RS01 devices
The in vitro aerosol performances of spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles after aerosolization from both the Orbital and RS01 are shown in Figure 7A, B, and C, respectively. MSLI data are represented as the percentage stage deposition of three runs (±standard deviation) after multiple actuations of 200 mg from the Orbital or 10×20-mg capsules from the RS01. The behavior of these three particulate systems in the Orbital and RS01 are discussed below.

In vitro aerosol deposition profile across the device and MSLI stages of the spray-dried
Spray-dried ciprofloxacin microparticles
Significant differences were observed when comparing the in vitro aerosol profiles of spray-dried ciprofloxacin microparticles from the Orbital versus RS01 (Fig. 7A). The FPF of spray-dried ciprofloxacin microparticles when delivered using the RS01 was 46.5±2.6% and 67.1±1.8% when using the Orbital; mass balance was above 95% for both devices. The higher FPF for the Orbital DPI, when compared with the RS01, could be attributed to a shift of drug deposition from stage 1 to stage 3 filter, suggesting that the Orbital device was more efficient at deagglomerating the spray-dried ciprofloxacin. The ciprofloxacin powder being amorphous is more cohesive, and the higher FPF with the Orbital means the device has higher dispersion efficiency than the RS01. This concurs with the lack of difference in FPF between the two inhalers dispersing the less cohesive powders (mannitol and mannitol:ciprofloxacin). This was reflected in a significant decrease in the MMAD, from 3.3±0.11 μm for the RS01 to 3.0±0.03 μm for the Orbital DPI (no change in GSD was observed between the two DPIs, with Orbital and RS01 presenting values of 1.7±0.01 and 1.6±0.01, respectively). Total device retention for the spray-dried ciprofloxacin microparticles in the Orbital and RS01 was similar (3.0±0.6% and 3.2±1.1%, respectively); however, this mass retention was primarily attributed to the puck in the Orbital and capsule retention in the RS01.
Spray-dried mannitol microparticles
The in vitro MSLI stage deposition data for 200 mg of spray-dried mannitol microparticle aerosolization from the Orbital and RS01 are shown in Figure 7B. In general, the FPF from both the Orbital and RS01 was less than for the ciprofloxacin microparticles, but the Orbital produced significantly higher FPF values (47.1±2.2%) than the RS01 (43.8±0.7%). This was also reflected in the MMAD values for mannitol where the Orbital presented a MMAD of 4.2±0.2 μm compared with the 5.1±0.3 μm for the RS01. As with the ciprofloxacin formulation, no significant difference in GSD was observed between the two devices (2.0±0.0 and 2.2±0.4 for the Orbital and RS01, respectively). The higher GSD in the mannitol microparticle system when compared with the ciprofloxacin is most likely attributed to the wider spread in intrinsic particle size data for spray-dried mannitol as presented in Figure 3. Device retention for mannitol in the two devices was 3.5±0.3% and 4.2±0.5% for the Orbital and RS01, respectively.
1:8 co-spray-dried ciprofloxacin:mannitol microparticles
The in vitro MSLI stage deposition data for 200 mg of 1:8 co-spray-dried ciprofloxacin:mannitol microparticles aerosolized from the Orbital and RS01 devices are shown in Figure 7C. In general, no significant differences in the stage deposition were observed between the two devices, and mass balance was>90%. The FPFs of the Orbital and RS01 devices were 42±1.8% and 38.4±2%, respectively, and no differences were seen in either MMAD (Orbital, 4.0±0.27 μm; RS01, 3.8±0.07 μm) or GSD (Orbital, 1.9±0.1; RS01, 2.1±0.02). Interestingly, the FPF in the 1:8 co-spray-dried ciprofloxacin:mannitol microparticle formulations was lower than for the ciprofloxacin or mannitol spray-dried systems.
Delivery efficiency of the Orbital DPI via multiple inhalation maneuvers
Compared with conventional capsule-based DPIs that require multiple-capsule use for high-dose therapy, the Orbital operates by containing a fixed dose in the puck that can be taken through multiple inhalation maneuvers. This approach ensures the patient receives the total dose under manageable sequential breaths. When the patient observes that the puck is empty, he or she disposes of the device and receives a “new” DPI when a new dose of medicament is required. As multiple breaths are required to empty the device, it is important to consider the rate of device emptying as a function of shot number. The puck emptying rate for 200 mg of spray-dried ciprofloxacin, mannitol, or 1:8 co-spray-dried ciprofloxacin:mannitol microparticles from the Orbital as a function of inhalation number (60 L/min, 4 sec) is shown in Figure 8.

Puck emptying rate as a function of experimental MSLI inhalation number for 200 mg loaded mass of the spray-dried ciprofloxacin, mannitol, and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles.
From analysis of the ciprofloxacin emptying rate, it can be seen that ∼50% of the dose (100 mg) is released in five consecutive inhalations, with 100% drug released in 12 inhalations. Interestingly, analysis of the emptying rate for the ciprofloxacin microparticles indicates puck emptying to be linear. Regression analysis of normalized mass data indicated an R2 of 0.98 with emptying coefficient of −8.65% mass per shot. In comparison, the emptying profile for the mannitol and 1:8 co-spray-dried ciprofloxacin:mannitol microparticles followed an exponential form with R2 values of 0.97 and 0.99, respectively. Such observations suggest that the emptying kinetics is dependent on the powder type. The amorphous ciprofloxacin system tends to be more cohesive than the mannitol, as reflected by the high stage 1 deposition data when using the RS01. Subsequently, the puck hole becomes the rate-limiting step for aerosolizing this powder, with a finite amount of powder being aliquoted into the main chamber per puck rotation. Over a 4-sec period, this approximates to 8% of the loaded mass per shot, when studying a 200-mg formulation. In comparison, the mannitol and co-spray-dried particulate systems are predominately crystalline and have lower cohesion. Thus, the ability for powder to exit through the puck orifice becomes dependent on the remaining mass in the puck at each rotation. To study this phenomenon, as well as test the tolerances of the Orbital to a range of doses, the aerosolization efficiency of the 1:8 co-spray-dried ciprofloxacin:mannitol microparticles was tested using the MSLI over a range of loaded doses from 100 to 400 mg.
Influence of loaded drug mass in puck on the efficiency of the Orbital DPI
To evaluate the influence of loaded puck size (i.e., target dose), 100, 200, and 400 mg of the 1:8 co-spray-dried ciprofloxacin:mannitol microparticles were loaded into Orbital pucks and tested using the same protocol as for the previous studies. MSLI data and puck emptying rates are shown in Figure 9A and B, respectively. In general, analysis of the FPF as a function of loaded puck mass suggested no significant difference in FPF with values of 42.8±1%, 42.0±1.8%, and 38.8±2% being observed for 100, 200, and 400 mg, respectively. Such observations suggest that the efficiency of the Orbital device in powder aerosolization is independent of loaded dose. Analysis of the puck emptying rate indicated that the rates were similar for all doses, following an exponential decrease in mass with respect to shot “inhalation” number, further supporting the mass dependency theory with respect to this particulate system. To highlight the reproducibility and exponential nature of puck emptying for the co-spray-dried system, the data for all loaded doses are plotted on a log-normal scale in Figure 10. Linear regression indicated the emptying profiles to be similar with R2 values>0.99. Such observations suggest that dead volume and loaded mass do not significantly influence the dynamics of emptying and aerosolization efficiency.

Comparison of

Emptying rates for 100, 200, and 400 mg puck fill weights of 1:8 ciprofloxacin:mannitol spray-dried microparticles from the Orbital device plotted on a log-normal scale. R2>0.99.
Conclusions
To date, no device has been reported that can efficiently (and passively) deliver high doses of inhalation medicine to the lung without repeat actuation, priming, or capsule loading. Here, we have shown the Orbital device to be capable of delivering 100–400 mg of powder with equivalent or higher efficiency than 10 capsules from a commercially available RS01 device. Furthermore, we have shown the device to be capable of delivering both amorphous, crystalline and co-spray dried powder systems. Ultimately, this approach will lead to improved ease of use and better patient compliance and open up the possibilities of delivering a wide range of high-dose medicaments that are currently not available for inhalation.
Footnotes
Acknowledgments
This research was supported under Australian Research Council's Linkage Projects funding scheme (project no. LP100100451). Associate Professor Young is the recipient of an Australian Research Council Future Fellowship (project no. FT110100996). Associate Professor Traini is the recipient of an Australian Research Council Future Fellowship (project no. FT12010063). We also thank Eric Zhu and Jesslynn Ooi for assistance with DSC and scanning electron microscopy.
Author Disclosure Statement
Authors Young, Traini, and Chan are chief investigators on an ARC Linkage Project (LP100100451) of which Pharmaxis is a partner organization. Authors Crapper and Phillips are employees of Pharmaxis PLC.