
Abstract
Abstract
Background:
Respiratory tract deposition of air pollution particles is a key to their adverse health effects. This study was aimed to determine the size-resolved deposition fraction (DF) of sooty wood smoke particles in the lungs of healthy subjects. The type of wood smoke investigated is typical for household air pollution from solid fuels, which is among the largest environmental health problems globally.
Methods:
Twelve healthy volunteers inhaled diluted wood smoke from incomplete soot-rich combustion in a common wood stove. The DF of smoke particles (10–500 nm) was measured during three 15-min exposures in each subject during spontaneous breathing. Lung function was measured using standard spirometry.
Results:
The total DFs by particle number concentration were 0.34±0.08. This can be compared with DFs of 0.21–0.23 in healthy subjects during previous experiments with wood pellet combustion. For particle mass, the total DFs found in this study were 0.22±0.06. DF and breathing frequency were negatively correlated as expected from model calculations (p<0.01).
Conclusions:
The DF of the investigated sooty wood smoke particles was higher than for previously investigated particles generated during more efficient combustion of biomass. Together with toxicological studies, which have indicated that incomplete biomass combustion particles rich in soot and polycyclic aromatic hydrocarbons (PAHs) are especially harmful, these data highlight the health risks of inadequate wood combustion.
Introduction
A
Biomass combustion for heating and cooking is a major source of air pollution globally. During the winter season, wood smoke from heating residences is a significant contributor to airborne particulate matter (PM) in central and northern Europe, as well as the US, Canada and many other countries.(5,6) A growing body of studies has now confirmed exposure to wood smoke to be associated with asthma, chronic obstructive pulmonary disease, acute lower respiratory infection, and tuberculosis.(7–11) In developing countries, large populations burn biomass for cooking and heating in simple fireplaces often in confined spaces. This results in extensive exposure concentrations and increased incidence of respiratory illness such as COPD. This has attracted considerable attention from the WHO and other authorities as a major health problem.(12) Recent controlled human wood smoke exposure studies have provided additional insights into the airway oxidative, inflammatory and systemic effects.(13–16)
Since the combustion conditions for biomass burning can vary substantially in terms of fuel type, air supply, temperature, and category of stoves and boilers, the physico-chemical characteristics of the wood smoke PM also show large differences.(17) Not surprisingly, systematic research with in vitro models performed by various research groups has resulted in considerably different toxicological capacity and mechanisms for biomass combustion PM.(18–20) This is also the case in experimental exposure chamber studies with wood smoke in human subjects.(21) As a consequence, it is important not to consider wood and other biomass smoke as an entity, but as a heterogeneous group of aerosol pollutants with varying characteristics and abilities to affect human health.
Deposition of air pollution particles in the lungs is one of the crucial factors behind their ability to cause adverse health effects. We have recently demonstrated that the deposition varies substantially between particles from different combustion sources, depending on the size distribution and chemistry of the particles. Considerable differences in deposition have been shown between particles from high- and low-temperature combustion of wood pellets, traffic, and diesel engine exhaust.(22,23)
We have previously reported on the respiratory tract deposition of particles emitted from combustion of wood pellets in a residential pellet burner under two conditions: low temperature (incomplete) and efficient (complete) combustion. 22 However, no study has so far investigated the deposition of particles emitted from traditional batchwise log wood combustion in wood stoves or other fireplaces, which is the most relevant exposure situation both for ambient and indoor air exposures.
The objective of this study was to investigate the respiratory tract deposition in healthy subjects of typical fresh wood smoke particles under incomplete soot-rich combustion conditions in a standard wood stove.
Materials and Methods
Subjects
Twelve healthy volunteers were included: 5 women and 7 men, never smokers, mean age 24±3 years (Table 1). Standard lung function tests were performed according to the guidelines of the American Thoracic Society(24) using a spirometer (Jaeger MSC spirometer, Germany) (Table 1). The study was approved by the regional ethical review board and performed in accordance with the Declaration of Helsinki. All the subjects gave their written informed consent.
Data are expressed as means (SD). BMI, body mass index (kg/m2); FEV1, forced expiratory volume in 1 s; VC, vital capacity; VT, tidal volume; RR, respiratory rate; MV, minute ventilation.
Study design
Subjects inhaled wood stove smoke through a mouthpiece from a 15.3 m3 exposure chamber with an air exchange rate of around 3 times per hour. Mouthpiece breathing may potentially affect the breathing pattern, but was not possible to circumvent without introducing other uncertainties in the measurements.(25) Deposition of wood smoke particles was measured during three 15-minute exposure sessions for each subject. Before the sessions, a test measurement was carried out in order to allow the subjects to adjust to the equipment and be comfortable.
Aerosol generation and characterization
Wood smoke was generated using a common Nordic wood stove (chimney stove) applying a firing procedure that aimed for incomplete combustion conditions with soot-dominated particle emissions. Batches of two birch logs (∼1.1 kg each time) were inserted approximately every 40 min, giving a fuel load of 7–8 kW. In addition, the fire was disturbed two to three times during a batch either by adding some extra fuel (i.e., a small wood log) or by reducing the air supply momentarily. This procedure caused occasions with high burn-rate air-starved combustion conditions, presumably generating a soot-rich aerosol emission, in accordance with a previously reported human exposure campaign in the same project.(21) The varying combustion conditions were maintained with average O2 and CO levels of 8.7% and 3500 ppm, respectively. The average 10–90 percentiles were 4.9 and 14.6 for O2, and 1000 and 5900 ppm for CO. Several occasions with high CO levels, in excess of 15,000 ppm, occurred in connection with low excess oxygen (<3%) conditions.
In previous studies, it had been illustrated that this kind of combustion with high burn rate of wood is associated with increased fine particle emissions with high soot and polycyclic aromatic hydrocarbon (PAH) emissions.(26–28) Within the scope of the larger human exposure campaign, the chemical composition of the particles in the chamber during similar combustion conditions were characterized with respect to organic and elemental (soot) carbon, PAH (total and species) and inorganic salt fraction, as described in more detail by Unosson et al.(21) In the present study, the fine particle mobility number size distribution and concentration were measured by a scanning mobility particle sizer (SMPS), as described in more detail below.
Respiratory tract deposition measurements
The set-up used for the respiratory tract deposition measurements has been described previously(29,30) and follows general experimental guidelines.(31) In summary, subjects wearing a nose clip breathed wood smoke through a mouthpiece while sitting in a relaxed position. Wood smoke was drawn from the exposure chamber for inhalation, while exhaled smoke was directed into a 2 dm3 stainless steel container open to atmosphere. The container for exhaled air was heated to approximately 37°C to avoid condensation of water vapor.
The particle concentrations in the inhaled and exhaled air respectively were measured with a scanning mobility particle sizer (SMPS, design: Lund University) consisting of a differential mobility analyzer (DMA, 28 cm long Vienna type) and a condensation particle counter (TSI Inc., model 3010). The SMPS measures the particle number size distribution in the range of 10–500 nm, classified according to the particle mobility diameter. This is also the appropriate equivalent diameter for this application, since diffusion is the dominating deposition mechanism in the respiratory tract for particles below 500 nm.(31) Scan time was set to 90 sec (both up and down scan). The first 90 sec of data from each exposure session were discarded to ensure complete mixing of the aerosol in the lungs. The aerosol was dried to below 20% relative humidity before measurement.
Fresh wood smoke particles are generally a mixture of agglomerated soot particles and hygroscopic salt particles that may change in size when exposed to high relative humidity.(32,33) A particle size shift between the inhaled and exhaled samples due to the elevated humidity in the lungs may cause errors in the measured respiratory tract deposition.(29,31) To minimize such errors, the aerosol sampled from the inhaled air was humidified to 90% relative humidity and subsequently dried. Thereby, the inhaled and exhaled size distributions were comparable.
Deposition fraction and dose rate
The size-dependent deposition fraction, DF (dme), was assessed from the general equation
where Cin and Cex are the measured inhaled and exhaled particle concentrations, respectively. The mobility equivalent diameter, dme, is used for particle size determinations in this research. As discussed elsewhere, this is the most relevant diameter measure in the diffusion-dominated size regime (approximately <700 nm for particles with an effective density similar to wood smoke).(31) The calculated DF was corrected for particle losses in the instrument between inhaled and exhaled sampling points and for mouthpiece dead space.(34,35)
Estimations of the surface area and mass of the deposited particles were based on the measured mobility number size distribution and measurements of the particle effective densities, according to principles previously outlined by Löndahl et al.(22) and Rissler et al.(23) Characterization of the effective density was carried out by an aerosol particle mass analyzer (APM, model 3600, Kanomax, Japan) as described by McMurry et al.(36) and more specifically by Rissler et al.(37) Based on these data, particles <60 nm in diameter were assumed to have a near spherical shape and a particle effective density of ∼1.2 g cm−3. Particles larger than 60 nm were of agglomerate shape, and thus the density decreased with increasing size. A power-law function with the exponent −0.52 (corresponding to a mass-mobility exponent of 2.48) was fitted to the measured effective densities. For instance, the density was 0.93 g cm−3 for 100 nm particles and 0.46 g cm−3 for 400 nm.
The surface area was estimated from the mobility number size distribution assuming both spherical particles and agglomerates consisting of 50 nm primary particles with negligible contact area.(23) However, the calculated surface area is of limited value for wood smoke particles since they contain a substantial fraction of alkali salts and other material that will dissolve after deposition. Therefore, the assumption of spherical particle shape was used in the analysis, if nothing else is stated.
The total deposition fraction (TDF) was calculated from the size-dependent deposition fraction and the particle size distributions by number, surface area, and mass.
22
The measured deposited dose rate (particles/hour) was determined from the total deposition fraction, TDF, inhaled volume flow, Q, and inhaled particle concentration:
Dose rates were estimated for a supposed exposure concentration, Cin, of 1 μg/m3. Subject specific values of deposition fractions and inhaled volume flows were used.
Statistical analysis
All data, lung function tests, and particle deposition fractions, were normally distributed and are therefore reported as means±standard deviation (SD) unless otherwise stated. Pearson correlation test was used for associations between DF and lung function parameters and breathing pattern. All data were analyzed using SPSS, version 21 for Windows (IBM® SPSS® Statistics 21, Chicago, IL, USA).
Results
Wood smoke particles
The wood smoke aerosol varied over time depending on combustion conditions. The total particle concentrations, derived from the measured size distribution and effective density, were 78,700±78,000 cm−3 by number, 3700±1800 mm3/m2 by surface area, and 81±35 μg/m3 by mass (Fig. 1). If assuming agglomerated particles, the surface area was 8200±3500 mm3/m2. For reasons previously explained, the surface area calculated for spherical particles was used in the proceeding analysis. The mass concentration measured by the TEOM was 132±26 μg/m3. The higher mass measured by the TEOM, compared to the value calculated from the size distribution measurement, is explained by a larger size range for this instrument (<1 μm, see also Fig. 1) and possibly a different instrumental response to peaks in the wood smoke emissions.

Size distribution of the wood smoke particles by number and mass (mean value for the exposure sessions). For the number size distribution, the 10th–90th percentiles are shown for the 15-minute long exposure sessions. The mass distribution (solid line) is calculated from the number distribution and the measured effective density.
The size distribution was clearly bimodal (Fig. 1). Fitting two log normal functions to the distribution results in count mean diameters (CMD) of 45 and 149 nm, geometric standard deviations (σg) of 1.88 and 1.61 and relative number concentrations of 64% and 36% for each mode, respectively.
The variation in particle concentrations was due to fluctuations between efficient and incomplete soot-rich combustion, as is typical for this type of wood smoke. The chemical characterization of the PM in the chamber during similar combustion conditions using the same stove and fuel, showed that the carbonaceous matter was dominated by soot with an elemental carbon (EC) to total carbon (TC) ratio of 0.72±0.08 as given in Unosson et al.(21) Further, from analysis of the components in the wood smoke, it was estimated that the total PM consisted of 38% soot, 24% organics, and the remainder presumably alkali salts (a correction factor was used to convert the organic carbon (OC) content to total organic PM and EC to soot PM mass concentration).(21)
Respiratory tract deposition
The deposition fraction (DF) of wood smoke particles generally decreased with increasing particle size in the studied interval (10–500 nm) (Fig. 2). The total deposition fraction (TDF) of wood smoke particles was 0.34±0.08 by number, 0.22±0.06 by surface area, and 0.22±0.06 by mass (Table 2). The surface area and mass were dominated by the larger particles, for which the DF was low and hence also the TDF. A significant part of the mass and surface area of the wood smoke particles was found at larger sizes than the measured range of 10–500 nm (Fig. 1) and thus, the TDF of the entire distribution is probably higher than that in the measured size interval due to the increasing deposition fraction at larger sizes. The TDF by number correlated positively with tidal volume (r=0.65, p=0.02) and negatively with respiratory rate (r=−0.84, p=0.0006) as could be expected from theoretical deposition models (Fig.3).
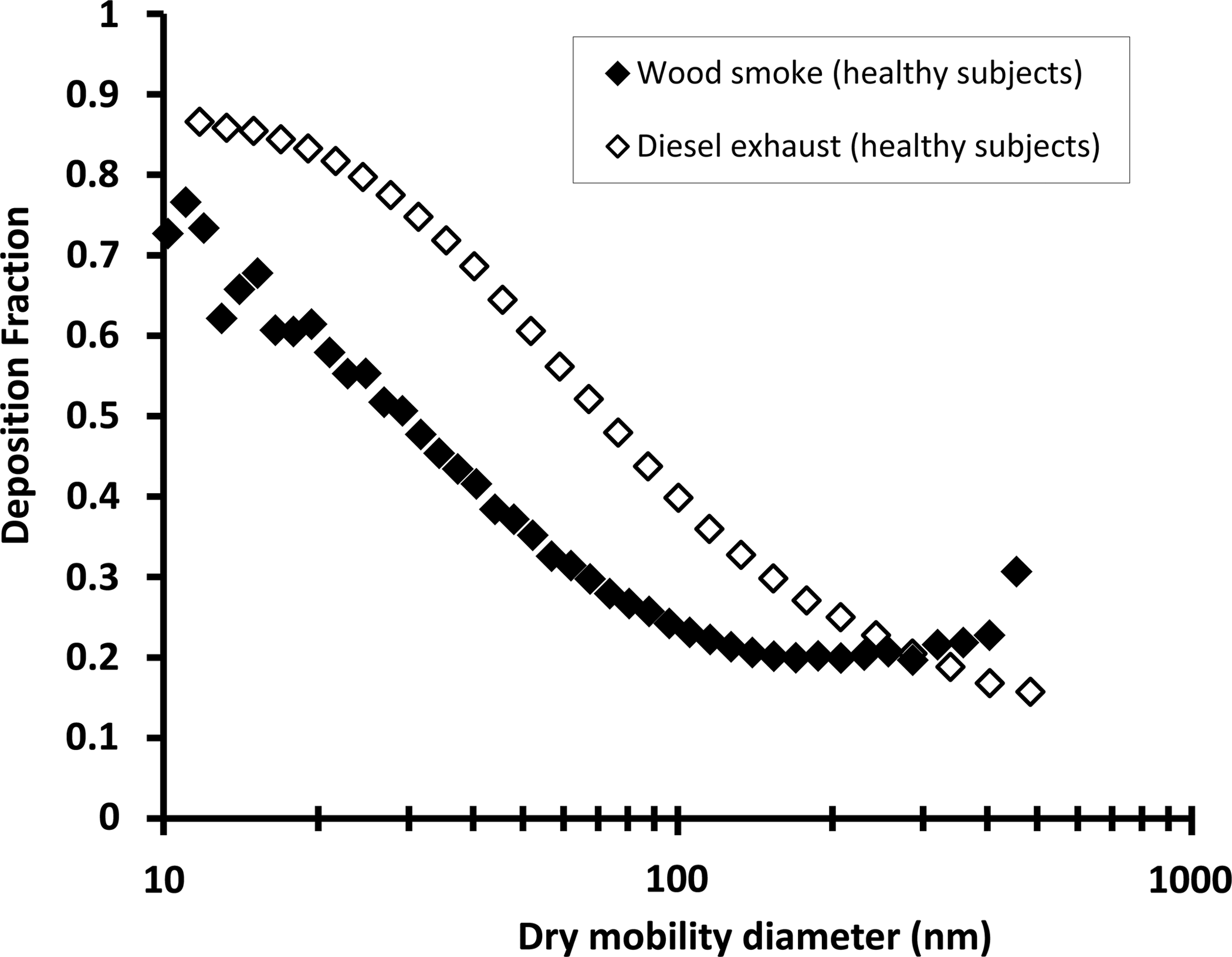
Deposition fractions (DF) of wood smoke particles for healthy subjects. Experimental data for DF of diesel exhaust particles are shown for comparison (Rissler, et al. 23 ).

Correlation between total deposition fraction (TDF) by number and respiratory rate (min−1) (r=−0.611, p=0.009).
Deposited dose rates (particles/hour) are shown in Table 3. Tidal volume was positively correlated with dose rate by number (r=0.88, p=0.0001), surface area (r=0.74, p=0.005) and mass concentration (r=0.71, p=0.009). There was also a significant correlation between minute ventilation and dose rate by number (r=0.67, p=0.018), surface area (r=0.62, p=0.03) and mass concentration (r=0.59, p=0.04), as seen in Figure 4.

Correlation between dose rate (number per hour) and minute ventilation (MV) (r=0.67, p=0.018).
Parameterization of data
In order to facilitate comparison and implementation of data, a parameterization of the measured deposition fractions of particles from different sources, published here and previously,(22,23,38) was carried out based on a double exponential equation:
where dme is the particle mobility diameter in μm and the values of A, B, C, and D are constants specific for each studied aerosol. The equation is not based on theory for particle deposition, but was chosen for its simplicity and good correlation with experimental data. Table 4 shows fitting parameters for the deposition fractions, their valid size intervals and correlations between modeled and measured data.(22,23,38,39)
To facilitate comparison of experimental data, a double exponential equation was fitted to the average size-dependent deposition fractions measured for various aerosols during normal breathing for healthy adults and COPD subjects (see Materials and Method section). The equation is
r=Pearson correlation coefficient for the fitted equation compared to the measured values, Löndahl et al.(46)
Discussion
In the present study, the respiratory tract deposition of incomplete soot-rich wood smoke was investigated. This type of smoke is highly relevant since this is a common method for burning wood worldwide. The aerosol is comparable to “household air pollution from solid fuels,” which has been highlighted as the largest air pollution problem globally from a health perspective.(12) In vitro studies have even shown that wood smoke particles generated from incomplete combustion were more toxic and induced higher inflammatory responses compared with more efficient biomass combustion(20,40) and diesel exhaust particles.(41,42) We have recently demonstrated, by an experimental exposure study, that this soot-rich wood smoke combustion caused an acute increase in arterial stiffness in human subjects—a finding that has been linked with adverse long-term health effects.(21,43)
Air pollution, both particles and gases that deposit in the respiratory tract, can elicit a plethora of oxidative and pro-inflammatory events leading to adverse health effects.(13,15) Particle respiratory deposition has been little studied in contrast to particle concentrations in ambient air, which are continuously recorded at a large number of sites worldwide. Since the deposited particle fraction and also the relative toxicity may vary considerably between sources, knowledge of the actual deposition is an important factor to identify for air pollution particles from different relevant scenarios.
Characteristics of the wood smoke
The particle size distribution for the investigated wood smoke was bimodal. This is consistent with a smaller mode of alkali salt particles from complete combustion that dominates numerically, together with a mode of larger soot particles.(18,27) The bimodal distribution is most probably a consequence of both varying combustion conditions at different parts of the fuel in the stove and changes in combustion efficiency over time.
The vast majority of the numbers of particles emitted from the current sooty wood log combustion had a dry mobility size distribution peak that was smaller than for the previously studied pellet combustion, both during the efficient (alkali salt dominated) and low-temperature (organics dominated) wood pellet combustion.(22) This increased the total deposited fraction and deposited dose, since the DF increased with decreasing size in this size range.
Experimental technique
The currently employed technique was developed by the investigators as a reliable and accurate means to determine deposition in human subjects with high precision.(29) However, the presently studied wood smoke aerosol was challenging from an experimental point of view.(31) The particle concentration varied rapidly over time due to the changing combustion conditions that are typical for this type of burning. In addition, the particles were highly agglomerated with hygroscopic material that is likely to cause a restructuring during exposure to high relative humidity. The exposure time was long compared to previous studies with the present technique in order to minimize errors from concentration variations. It was also necessary to remove periods of data when the combustion emissions were peaking. To avoid errors in DF from particle restructuring, the aerosol was humidified and dried before sampling. In real life, subjects vary their ventilation between nasal and mouth breathing, whereas the present investigation was limited to mouth breathing. For aerosol particles in the studied size range, there is no major difference in deposition between relaxed oral and nasal breathing. According to the Multiple-Path Particle Dosimetry Model (MPPD V2.1, Applied Research Associates Inc.), the DF could be expected to be about 0.04±0.02 higher during relaxed nasal breathing for wood smoke. For small (<20 nm) non-hygroscopic particles, nose breathing may increase the DF by 0.07–0.1.
Deposition of wood stove smoke
As shown in Figure 5, the investigated sooty wood smoke has a DF that closely matches the data previously obtained for particles from low-temperature incomplete wood pellet combustion. Meanwhile, for most of the studied size range, the DF for biomass combustion was low compared with diesel exhaust particles.
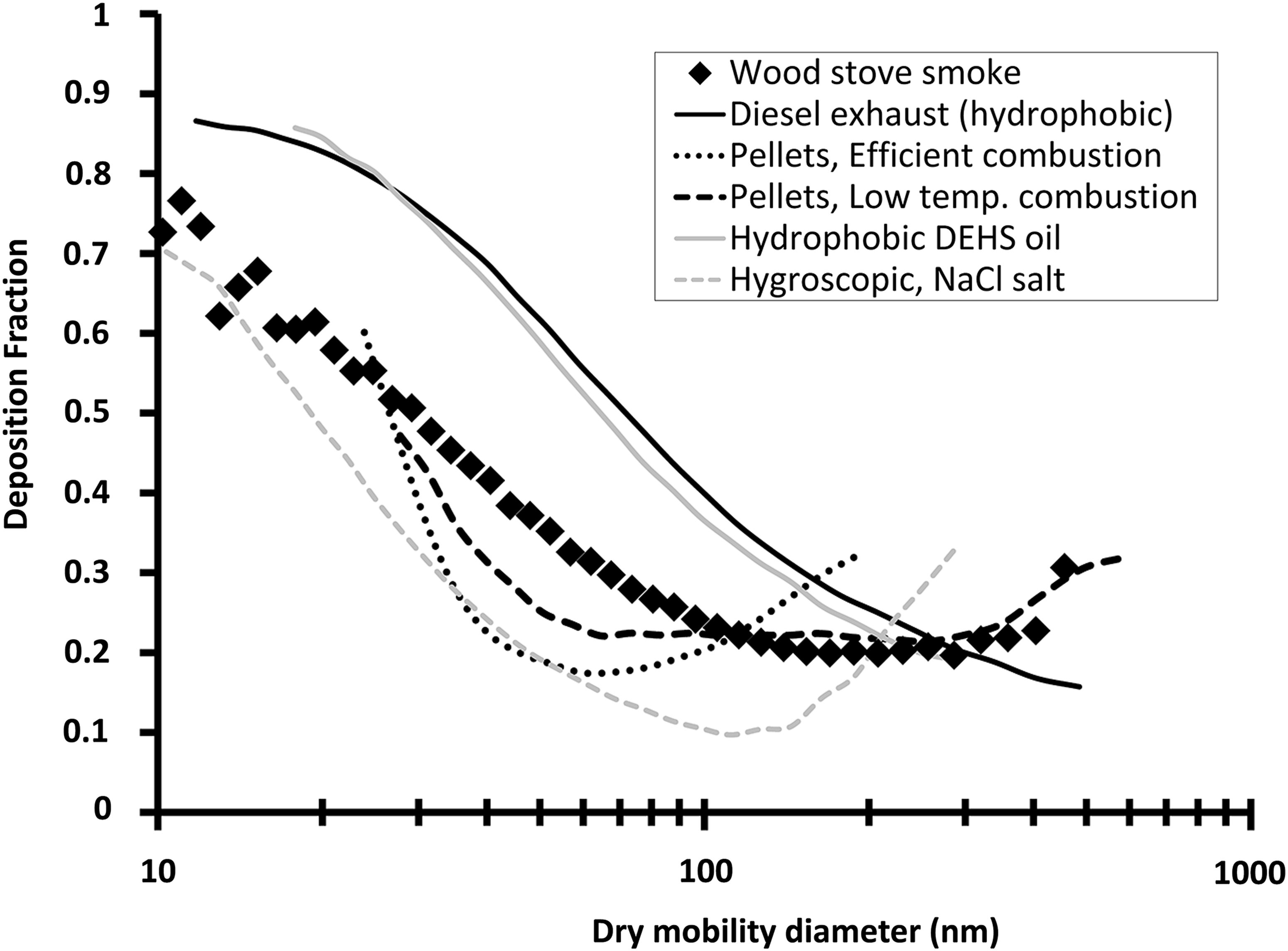
The DF of wood smoke particles could be explained by their physical and chemical properties. DF depends on several factors, such as particle size, chemical compositions and hygroscopicity. The smaller particles contained a substantial fraction of alkali salts, which are water soluble. These particles will grow by uptake of water in the respiratory tract, where the relative humidity is about 99.5%. The growth decreases their diffusivity and, hence, also their probability to deposit. For instance, a dry hygroscopic 50 nm particle may grow to a size of 150 nm and therefore have a substantially decreased probability to deposit. On the other hand, the larger particles consisted mainly of soot, which is hydrophobic. These deposited to a lesser extent than the smaller particles because they had a size for which the DF is low.(18,45)
The measurements indicate a somewhat higher DF of the largest wood smoke particles (>300 nm) compared to completely hydrophobic particles (Figs. 2 and 5). This may very well be explained by a small fraction of hygroscopic material also on the large wood smoke particles. In this size range, particle growth will increase the DF since deposition by gravitational settling and impaction increases with particle size for large particles. A higher effective density of the biomass combustion particles may possibly also have contributed to the difference in the DF for the largest sizes. For instance, the effective density of 400 nm particles was 0.46 g cm−3 for the wood smoke and 0.25 g cm−3 for the previously studied diesel exhaust (during transient engine running conditions).(23) A higher effective density increases deposition by gravitational settling and impaction.(31)
DF was around 0.3 by number, corresponding to around 0.2 by mass. Although this is a somewhat lower DF than for some other aerosols, such as diesel exhaust particles, it is sufficient to cause considerable adverse health effects.
The DF correlated positively with tidal volume and inversely with respiratory rate. The relationship between DF and respiratory rate was expected to be negative, since under high respiratory rate the inhaled particles spend less time within the lungs. The opposite would be expected concerning the tidal volume: large tidal volumes (i.e., deep breaths) were associated with low respiratory rate (r=−0.77, p=0.004 for the healthy group). Minute ventilation (MV) was correlated neither with respiratory rate nor with DF. This is consistent with previous data showing that the DF remains almost constant irrespective of level of exercise.(46) However, the MV correlated positively with the dose rate because of the increasing inhaled volume. A higher dose rate during heavy breathing is expected.(47,48)
Comparison with other aerosols
The total deposition fraction (TDF) by number for the sooty wood smoke studied in the present campaign was higher than for previously reported data for both efficient and incomplete (low-temp) wood pellet combustion, while surface area and mass were relatively similar (Table 2). In comparison, diesel exhaust and traffic-related particles have shown substantially higher TDFs for all aspects. For instance, diesel engine exhaust generated during idling conditions resulted in twice as high TDFs by particle number.(39) Exhaust particles from engines are generally hydrophobic due to the high fuel content of organic hydrocarbons, which results in less water uptake in the human airways and a higher probability to deposit by diffusion compared to the more hygroscopic biomass combustion particles.
The total measured deposited dose rate (particles/hour), with exposure concentrations normalized to a PM exposure of 1 μg/m3, is higher for the currently studied wood smoke compared with the two previously studied pellet combustion cases, whereas the diesel exhaust and traffic-related particles had even higher dose rate by number, surface area, and mass, as seen in Table 3.
The particles in the emissions from the residential wood pellet boiler that we previously investigated were generated under different combustion conditions compared to the present study, thus generating PM composed almost completely of alkali salts in one case and of organic material (mainly pyrolysis products) in the other. The present investigation therefore adds information on a type of ultrafine wood smoke particles that are soot and PAH rich, and which have not previously been examined. This biomass aerosol is the first to be identified to be able to induce adverse cardiovascular effects in humans.(49)
In a study by Kristensson et al.,(50) the Multiple Path Particle Dosimetry (MPPD) Model was used to estimate the respiratory tract deposition of wood smoke and traffic-related particles in ambient air in a town in Sweden. The modeled DF, based on direct measurements of ambient particle size distributions and hygroscopic properties, was in general agreement with the experimental data obtained in this study.
Conclusions
The fraction of particles deposited in the respiratory tract upon inhalation depends on the chemical and physical characteristics of the particles. This study presents the first experimental data on the deposition of soot-rich particle emissions from a traditional wood stove—a very common type of aerosol worldwide. The particles in the size range of 10–500 nm had a relatively low deposition probability in the respiratory system compared to hydrophobic particles such as diesel soot,(23) but similar or slightly higher than particles from a wood pellet burner.(22) The result is in accordance with theory, mainly through factors such as particle size and particle water uptake in the lungs. Further research should address particle deposition in groups of subjects with COPD and asthma with a wide range of severity and different phenotypes, in order to improve the understanding of health effects related to biomass exposure.
Footnotes
Acknowledgments
The following organizations are gratefully acknowledged for financial support: The EU ERA-NET Bioenergy Program (project BIOHEALTH), The Swedish Research Council (Project 621-2011-3560), The Swedish Heart Lung Foundation, and Västerbotten County Council Spearhead Research Grant.
Author Disclosure Statement
The authors declare that there are no conflicts of interests.