
Abstract
Abstract
Background:
In cystic fibrosis (CF) patients, inhalation of alpha1-proteinase inhibitor (A1-PI) can prevent or slow down persistent infections and reduce the massive ongoing inflammation and excessive levels of NE that destroy the airway epithelium, leading to progressive loss of pulmonary function and death. It is essential for an efficient treatment with inhaled A1-PI that an adequate and reproducible dose is deposited within all regions of the lung. The I-neb AAD System provides two inhalation modes: the Target Inhalation Mode (TIM) and the Tidal Breathing Mode (TBM). Both were compared in this study for their efficiency to deliver A1-PI to the lungs.
Methods:
This was a randomized, open label, cross-over study to investigate the lung deposition of A1-PI in 6 healthy subjects (HS) and 15 CF subjects. The primary endpoint was to evaluate the total lung deposition relative to filling dose of A1-PI inhalation solution using the I-neb AAD System in TIM and in TBM. The main secondary endpoints were extra-thoracic deposition, exhaled drug fraction, nebulizer residue, C/P ratio, and variance of pixel counts. Additional exploratory endpoints were total treatment time and the inhalation time. Radiolabeling was performed considering GMP using a commercially available sterile labeling kit. Radiolabeling was validated using NGI data acquired by gamma scintillation and UV spectrometry.
Results and Conclusions:
The intrapulmonary deposition (mean ± SD) in CF subjects was 47.0% ± 6.6% and 46.7% ± 10.3% in TIM and TBM, respectively, and in healthy subjects, 50.0% ± 6.7% and 54.8% ± 7.0% in TIM and TBM, respectively. TIM resulted in an approximately 40% lower treatment time (HS 6.4 min vs. 10.3 min, CF 5.3 min vs. 10.7 min) and less extra-thoracic deposition compared to TBM, and showed a higher residue of drug in the nebulizer, compared to TBM. In both groups, inhalation of a single dose of 77 mg of A1-PI was efficient, safe, and well tolerated using TIM and TBM.
Introduction
T
Nearly 65% of adults and 20% of children with CF have moderate to severe lung disease.(1) Although disease of the pancreas, liver, intestine, and vas deferens is present in subjects with CF before birth, the lung appears to be normal at birth. Defective Cl- re-absorption in the lung leads to desiccated airway secretions by drawing sodium out of the airways, with water following passively. Desiccated secretions interfere with mucociliary clearance and trap bacteria in an environment that is well suited to colonization by distinctive microbial pathogens.(2)
The ensuing lung infection and inflammation recruits and activates neutrophils that ultimately release neutrophil elastase (NE). Normal levels of endogenous antiprotease are rapidly overwhelmed by an excess of NE in the CF lung. In addition, NE stimulates the production of pro-inflammatory mediators and cleaves complement receptors and immunoglobulin G, crippling host defense mechanisms against further bacterial colonization in the lung.(3) Infection becomes persistent, and the massive ongoing inflammation and excessive levels of NE destroy the airway epithelium, leading to the progressive loss of pulmonary function and death.
Inhalation of A1-PI could prevent or slow down this process. Berger et al. showed a dose-related increase in elastase inhibition and in the mean concentration of elastase-A1-PI complex by administering three doses (100, 200, and 350 mg) by inhalation twice daily for 4 weeks in 26 CF patients.(4) Vogelmeier et al. showed double baseline values of A1-PI in the epithelial lining fluid of healthy subjects and anti NE activity up to 36 hours.(5) All the above-mentioned studies showed good tolerability of inhaled A1-PI and reported no serious adverse events (SAEs) and little adverse events (AEs). In addition, Kerem et al. conducted a study in which the drug was well tolerated when inhaled daily for 28 days.(6) Also, a study conducted by CSL with their study product with doses of either 77 mg (69 mg active protein), 175 mg (158 mg active protein), or up to 350 mg (315 mg active protein) or placebo showed no clinically significant findings on any of the safety parameters. No SAEs occurred for the 18 subjects.
It is essential for an efficient treatment with A1-PI that an adequate and reproducible fraction of the dose loaded into the nebulizer device is deposited within all of the lung regions. It was shown by McElvaney(7) that a concentration >8 μM of A1-PI in the lung epithelial lining fluid will result in suppression of neutrophil elastase and restoration of previous anti-neutrophil elastase capacity. In subsequent trials it was shown that approximately 20–40 mg of A1-PI must be delivered to the lung in order to achieve the desired concentration of at least 8 μM.(8)
In this study, the deposition of A1-PI in the lungs and extra-thoracic airways of healthy subjects and subjects with CF was assessed after inhalation with the I-neb AAD System (Phillips Respironics, Respiratory Drug Delivery (UK) Ltd.) for two inhalation modes: the Target Inhalation Mode (TIM) and the Tidal Breathing Mode (TBM). Inspiratory profiles with the I-neb AAD System were determined.
Nikander et al.(9) described the operating principles of the two inhalation modes in detail and can be summarized as followed: TIM (Target Inhalation Mode) was developed to provide the patient with an optimal target time for a slow and deep inhalation. The TIM mouthpiece is designed with an inhalation valve to restrict the inspiratory flow to a slow and deep inspiration at ∼15 L/min. When the inhalation target time is reached, a vibrator signals the end of inhalation. The TIM algorithm will adapt to the subject's inspiratory capacity by increasing the inhalation target time after each inhalation past the target. The goal is to guide the patient to extend the length of the inhalation target time to ∼80% of the forced vital capacity (FVC). When the patient has reached the optimal inhalation target time, the algorithm will adjust it to meet the patient's efforts on each inspiration.
TBM (Tidal Breathing Mode) was developed to adapt to the patients natural breathing. The TBM algorithm continuously records the patient's breathing pattern, and continuously predicts the length of the patient's next inhalation. Aerosol is pulsed at the beginning of the next inhalation and ends after 50% of the predicted inhalation time has expired. In this way, airborne droplets are cleared from the flow passages with clean air, rather than remaining to deposit within the device during exhalation. For the prediction of the length of the next inspiration, the average length of the past three inspirations is used by the AAD algorithm.
Material and Methods
Study design
This was a Phase 1, single-center, randomized, uncontrolled, cross-over, single-dose study to investigate the lung deposition of A1-PI in healthy subjects and subjects with CF. The primary endpoint was to evaluate the total lung deposition relative to nominal (filling) dose (DL,N) of the drug using the I-neb AAD System in TIM and in TBM in healthy subjects and in subjects with CF. The secondary endpoints were extra-thoracic deposition (DE,N), exhaled drug fraction (MX,N), and nebulizer residual (DR,N) relative to nominal (filling) dose. Also, the central to peripheral ratio (C/P) as index of regional lung deposition, and variance of pixel counts (VAR) as index of homogeneity of deposition within the lung were evaluated, as well as total lung deposition (DL,E) and extra-thoracic deposition (DE,E) relative to emitted dose (ex-mouthpiece dose). Lung function before and after treatment was assessed.
Exploratory endpoints were treatment time (total time of treatment, including exhalation time and breaks, e.g., coughing) and the inhalation time (treatment time without breaks by coughing) in TIM and TBM. Also potential correlations between the lung function parameters treatment time, and lung deposition were investigated. Device handling (convenience of inhalation, mode preference) as derived from a handling questionnaire for the I-neb AAD System in TIM and in TBM was assessed. Safety was assessed by documenting all adverse events that occurred during the trial.
Eligible subjects were invited to two treatment visits during which the subjects inhaled the solution in one of the two inhalation modes in a randomized order on Day 1 and on Day 5. Furthermore, subjects returned for two safety follow-up visits. At the safety follow-up visits, physical examination, vital signs measurement, and lung function test were assessed. During the first treatment visit (Day 1), a krypton gas ventilation scan was performed to evaluate the boundaries of the ventilated regions of the lungs. At each treatment visit (on Day 1 and Day 5), subjects inhaled the Investigational Medicinal Product (IMP), radiolabeled A1-PI inhalation solution [99mTc-human serum albumin (HSA) and A1-PI]. The total filled dose was 77 mg (nominal dose of A1-PI). Immediately after inhalation of the IMP, a scintigraphic gamma camera scan was made in order to measure lung deposition.
The study was conducted in accordance with the Declaration of Helsinki, the ICH Harmonized Tripartite Guideline for Good Clinical Practice (ICH-GCP) and relevant regulatory requirements. The study protocol was approved by the Ethics Committee of the “Bayerische Landesärztekammer” (Munich, Germany) and the responsible regulatory authorities.
Subject selection
Both male and female subjects, willing to participate, without childbearing potential, aged 18–65 years, and able to properly use the nebulizer were recruited. Both healthy and CF subjects were required to be non-smokers or ex-smokers for at least 3 months (previous smoking history of <10 pack years). Subjects with CF had to have a confirmed diagnosis of cystic fibrosis with a sweat chloride test of ≥60 mEq/L, a genotype with two identifiable mutations and an FEV1 ≥30% of predicted. All subjects gave written informed consent.
Subjects were excluded from the study if they had any clinical significant abnormal laboratory values, or hepatitis, or HIV, or a history of seizure disorder or significant cardiovascular, cerebrovascular, or renal disease, or any other condition that would have interfered with the subject's ability to participate or interfere in the evaluation of the study results. Subjects with a history of congestive heart failure and pulmonary edema were specifically excluded. Subjects had to have oxygen saturation above 85% and were not included if they changed any medication within 2 weeks prior to the screening visit, or if they had experienced an exacerbation in the last 4 weeks. Subjects with a persistent colonization with B. cepacia, defined as more than one positive culture within the past year before screening, were also excluded.
Radiolabeling technique, validation, and release procedure
Radiolabeling was performed at the Inamed laboratories in Gauting, Germany, considering Good Manufacturing Practice (GMP). Venticoll, a commercially available sterile labeling kit was used (GE Healthcare, Germany) because it provides a very stable binding of 99mTechnetium and human serum albumin (HSA) colloids. Therefore, leaching effects during the time of administration and image acquisition can be neglected. The Venticoll vials were suspended with sodium pertechnetate solution. After 30 min reaction time, a quality control using thin-layer chromatography was performed to verify that more than 95% of the Venticoll solution was labeled.
The radioactive concentration of the 99mTc-Venticoll-solution was measured with a gamma scintillation counter. Depending on the radioactive concentration of the 99mTc-Venticoll-solution, a certain volume of the 99mTc-Venticoll-solution was added to the A1-PI inhalation solution, whereas the ratio of 99mTc-Venticoll to A1-PI solution was smaller than 1:100 v:v. Thus, the final, radiolabeled inhalation solution was a mixture of a small volume of 99mTc-Venticoll and A1-PI inhalation solution with a target radioactivity of 8 MBq / 1.1 ml (at time of patient administration).
On the treatment visit, a two-phase release procedure for each manufactured batch was performed. The first phase was prior to inhalation and included as quality control two measurements: the determination of the specific radioactivity of the IMP (Specification: 4–7.7 MBq/mL), and the determination of identity of A1-PI by photometry. When all specifications were met, the labeled drug was released for inhalation by the designated head of manufacturing, designated head of quality control, and the investigator.
In the second phase which took place after the inhalation of the IMP, the fine particle fraction (FPF) of the IMP when nebulized with the I-neb AAD System was determined by cascade impaction and analysis of radioactivity per stage by scintigraphy and content by photometry (specifications: FPF ≥50%, difference between radioactivity and photometric FPF ≤10%). In addition, the microbiological load of the product was determined (specification: In accordance with European Pharmacopeia for inhalation products). When all additional specifications were met, the IMP was finally released.
The above mentioned procedure of radioactive labeling of the study medication was validated prior to the beginning of the study by comparing the generated droplet size distribution and emitted dose of the radiolabel and the drug to ensure that the deposition of radioactivity in the respiratory tract after inhalation of the radiolabeled solution represents the deposition of the active drug. In a pretest, the unlabeled A1-PI inhalation solution was compared with the radiolabeled A1-PI inhalation solution by spectrophotometry with respect to the generated droplet size distribution. The A1-PI content was analyzed using a spectrophotometric assay.
A1-PI was rinsed from the impactor stages using saline sodium chloride solution (0.9%) and subsequently the concentration of A1-PI was measured using a Genesis 10S UV/VIS spectrophotometer (Thermo Fisher, Germany) at 280 nm wavelength(10) (absorption coefficient 0.433/mg/mL). No relevant deviation was detected. Therefore the validation focused on the comparison of the spectrophotometric measured droplet size distribution and the radioactive measured droplet size distribution of the radiolabeled drug only.
Inhalation
Each subject inhaled in the two different breathing modes (TIM and TBM) of the I-neb AAD System until the I-neb AAD System stopped the inhalation automatically when the reservoir is empty. The inhalations utilizing TBM and TIM were performed in randomized order in the study center on two separate treatment days (Day 1 and Day 5) directly after the A1-PI inhalation solution was labeled with 99mTechnetium-Venticoll.
Prior to IMP inhalation, subjects were trained with placebo to use the I-neb AAD System in both inhalation modes (TIM and TBM) in order to assure that treatment time did not exceed 15 min. On study days, subjects inhaled the medication in an upright position through the I-neb AAD System in the respective mode until the I-neb AAD System stopped nebulization automatically. As a radiation protection measure, the I-neb AAD System was modified to support an exhalation filter in order to capture the exhaled aerosol. The administration of the drug including start and stop times was recorded by staff.
Krypton gas ventilation scan
A Krypton gas ventilation scan was performed once per patient to define the boundaries of the ventilated lung for the evaluation of the deposition images by drawing an ISO contour at 15% of the peak counts per pixel. For the C/P calculations whole lung rectangular regions of interests (ROIs) for the left and the right lung were drawn at the lung boundaries of the Krypton gas ventilation scan at a contrast of 15%.
Measurement of lung deposition
A posterior gamma camera image for 120 seconds of the chest (including oropharyngeal region and stomach) was taken immediately after dosing using a planar gamma camera with a field of view of 61 × 39 cm (MIE LFOV Digitrac 66-Scintron VI, MIE, Seth, Germany). ROIs for left lung and right lung were defined from the Krypton gas ventilation scan and copied and aligned to each deposition image. ROIs for mouth, trachea, stomach, and overlapping region of left lung and stomach were defined in the deposition image. Counts in the overlapping region of left lung and stomach were subtracted from the left lung region and therefore judged as extra-thoracic deposition.
This procedure adds on average an error for the determination of the extra-thoracic deposition of about 1% because the overlapping region is small compared to the left lung region or the stomach region. Resulting counts were corrected for background radioactivity and tissue attenuation. Tissue attenuation corrections were performed by measuring the chest thickness of the subject and calculating the attenuation factor according to the formula given by Pitcairn et al.(11)
Exhaled fraction and drug residue in I-neb AAD System was determined by measuring the radioactivity in the exhalation filter and the remaining radioactivity in the I-neb AAD System by using a scintillation counter (AM2005, MED, Dresden, Germany). Radioactive decay was corrected to time of inhalation.
Deposition values were calculated relative to filling dose using the following equations:
Absolute activity deposited in the lungs (ARe,L):
CL = Background and tissue attenuation corrected counts in the lung.
CE = Background and tissue attenuation corrected counts in the extra-thoracic region.
AI = Radioactivity emitted by the inhaler AI = AN -AR
AF,X = Radioactivity found on the exhalation filter
AN = Radioactivity filled into the nebulizer
AR = Radioactivity of nebulizer residual
Intrapulmonary deposition relative to filling dose (DL,N):
Absolute activity deposited in the extra-thoracic region (ARe,E):
Extra-thoracic deposition relative to filling dose (DE,N):
Additional deposition values relative to emitted dose from the I-neb AAD System were calculated using the following equations:
Intrapulmonary deposition relative to emitted dose (DL,E):
Extra-thoracic deposition relative to emitted dose (DE,E):
C/P ratio
C/P ratio is a measure normalized to the krypton ventilation scan to display the relation deposition in the central lung region that contains large bronchi compared to deposition in the peripheral region that does not contain large bronchi but the majority of the alveolus. That means that a C/P ratio which equals one (1) reflects an evenly distributed deposition pattern in both regions compared to the krypton ventilation scan. C/P values greater than one (1) indicate a shift in deposition towards larger airways, whereas C/P values below one (1) reflect a more peripheral deposition pattern compared to krypton ventilation scan.
Determination of C/P ratio of deposited activity after inhalation was performed according to Newman et al.(12) The rectangular ROIs from the Krypton gas ventilation scan were copied and aligned to each deposition image. Additional central ROIs (C) were positioned in the middle on the interior boundary of the rectangular whole lung ROI and correspond to 25% of the area of the rectangular whole lung ROI. The peripheral region (P) was that area lying between the rectangular central and whole lung ROI outline. The measured counts in the central ROIs were divided by the counts in the peripheral lung region. These calculated ratios were then normalized using the ratios calculated in the same way for the Krypton gas ventilation scan.
Variance of pixels (VAR)
As an additional analysis for general homogeneity of deposition, the variance of pixel counts (VAR) in the left and right lung was calculated from the histogram distribution of number of pixels vs. counts/pixel.(13,14) As the VAR decreases, homogeneity of deposition within the lung improves. In comparison to the C/P ratio, the variance of pixel counts is not limited to central vs. peripheral inhomogeneity but reflect the general inhomogeneity, for example, caused by deposition hot spots in severe CF subjects.
Measurements of lung function
Spirometric lung function parameters were measured using a Jaeger-Masterlab or Master-Scope (both CareFusion, Würzburg, Germany) at screening visit, on both treatment visits, and at all follow-up visits. The inspiratory and expiratory lung function including FEV1, MEF25, MEF50, MEF75, FEV1/FVC, FVC, TV, ERV, IC, and IVC were assessed before treatment and 2 hours (±15 min) after the completion of the inhalation of the study drug. Lung function test was conducted at each visit in accordance with current ATS/ERS recommendations.(15) Values were corrected for BTPS conditions (barometry, temperature, pressure standardization). Predicted values were calculated according to the formula of the European Coal and Steel Community.(16)
Statistical and analytical plans
Descriptive statistics (N, mean, standard deviation, median, minimum, and maximum) for all endpoints were calculated in each subject group (healthy subjects and CF subjects) and treatment group (TIM and TBM).
In order to explore the relationship between each parameter and inhalation mode (TIM and TBM), the parameter was compared between inhalation methods by an analysis of variance (ANOVA) model, with inhalation method, period, and sequence as fixed effects and subject effect nested within sequence as random effect. The descriptive statistics and statistical analysis was done for ITT (intention to treat) and PP (per protocol) population. The exploratory endpoints were summarized by descriptive analysis for each inhalation mode, subject group and at each visit. Spearman correlation to screen for potential correlations between lung function parameters, treatment time and drug deposition in each mode was calculated using SAS “proc corr”.
Results
Patients
A total of 21 subjects were recruited into the study: 6 healthy subjects and 15 subjects with CF. 19 subjects were in the per protocol (PP) population: 6 healthy volunteers and 13 subjects with CF, excluding 2 subjects with CF with missing primary endpoint data. All 21 subjects were treated with the labeled drug using an I-neb AAD System in the two different modes (TBM and TIM) applied in a randomized order (treatment sequence TIM-TBM: 3 healthy subjects, 7 CF subjects; treatment sequence TBM-TIM: 3 healthy subjects, 8 CF subjects). All 21 subjects received treatment in both inhalation modes and completed the study; no subject was prematurely withdrawn from the study. Healthy volunteers were younger (23.5 ± 2.2 years) than subjects with CF (32.9 ± 6.2 years). The overall gender distribution in the study was: male n = 14 and female n = 7. All subjects were Caucasian. Baseline data are presented in Table 1.
Results are expressed as mean ± standard deviation. FEV1, forced expiratory volume in one second; FVC, forced vital capacity; IC, inspiratory capacity, ITT, intention to treat.
Validation of radiolabeling procedure
The NGI measurements as illustrated in Figure 1 showed a close agreement in radioactive and photometric droplet size distribution and the validation proved that radiolabeling of the A1-PI inhalation solution with 99mTechnetium-Venticoll reproducible fulfilled the set criteria of FPF ≥50%, emitted dose relative to filling dose between 65% and 115% and the maximum deviation between photometric and radioactive measurement ≤10% (Table 2). All batches met the specifications for microbiological load according to European Pharmacopeia for inhalation products.
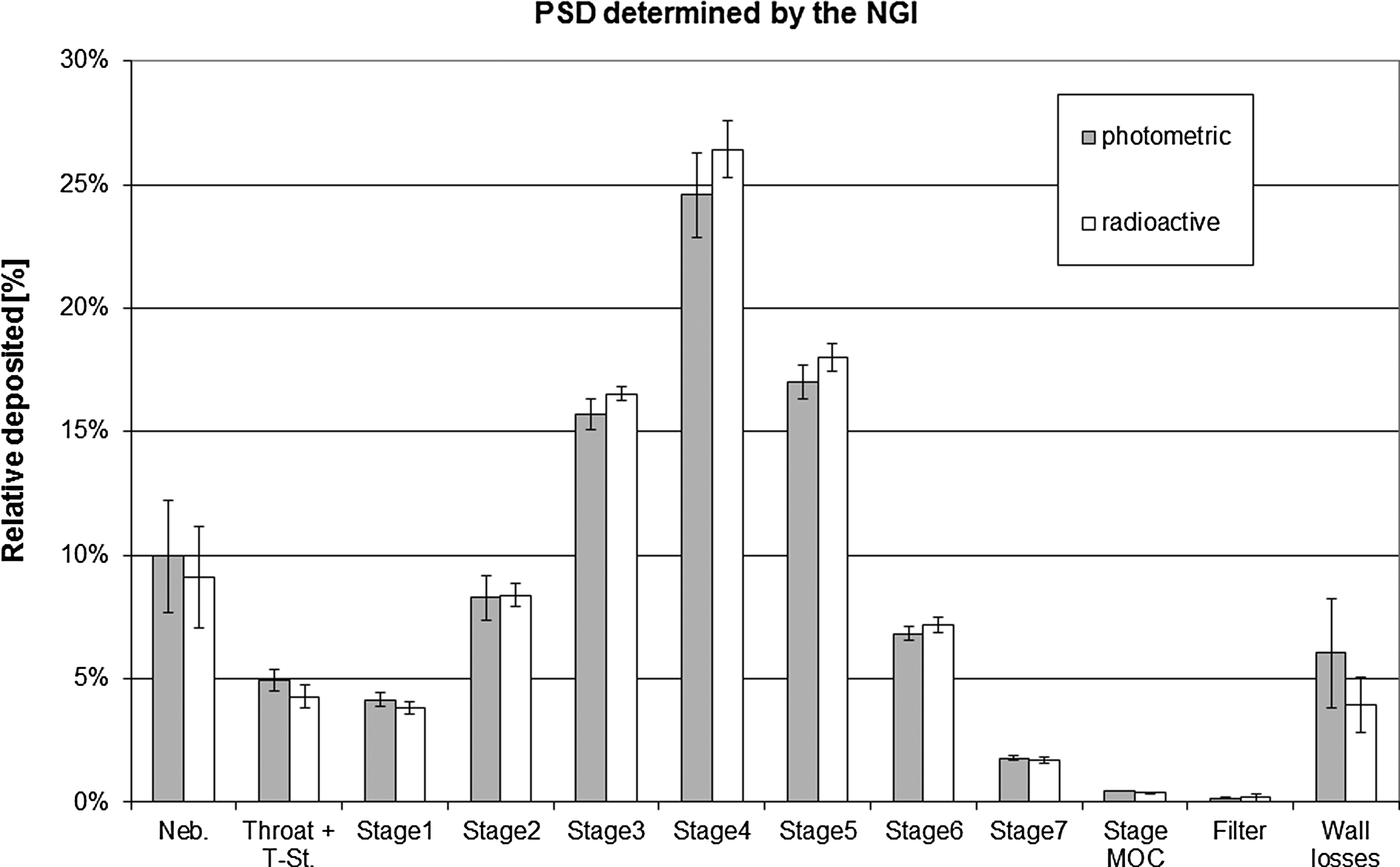
Particle size distribution PSD of 99mTc-Venticoll labeled Alpha1-proteinase inhibitor (human) (A1-PI(H)) inhalation solution as measured by NGI, radioactively, and photometrically (mean of three batches).
FPF, fine particle fraction; GSD, geometric standard deviation; MMAD, mass median aerodynamic diameter; rel. ED, emitted dose relative to filling dose.
Deposition data
The intrapulmonary deposition relative to filling dose (DL,N) (mean ± SD) in subjects with CF accounted for 47.0% ± 6.6% and 46.7% ± 10.3% in TIM and TBM, respectively. In healthy subjects, total lung deposition was comparable to CF subjects with depositions in TIM and TBM of 50.0% ± 6.7%, and 54.8% ± 7.0%, respectively. Statistics showed neither difference between both modes (TIM and TBM) nor any influence of the day of inhalation.
The extra-thoracic deposition relative to filling dose (DE, N) (mean ± SD) in subjects with CF, accounted for 19.9% ±5.1% and 27.0% ± 8.3% in TIM and TBM, respectively. In healthy subjects, extra-thoracic deposition was comparable to CF subjects with depositions in TIM and TBM of 16.3% ± 4.5%, and 23.7% ± 7.5% respectively (Fig. 2). DE,N was lower in TIM than in TBM, with similar least square mean differences in both subject groups (healthy subjects: -7.5%; CF subjects: -7.2%). These differences between the inhalation modes were statistically significant in both subject groups (healthy subjects: 95% CI [-13.7%, −1.3%]; p = 0.029; CF subjects: [-11.6%, −2.9%]; p = 0.004).
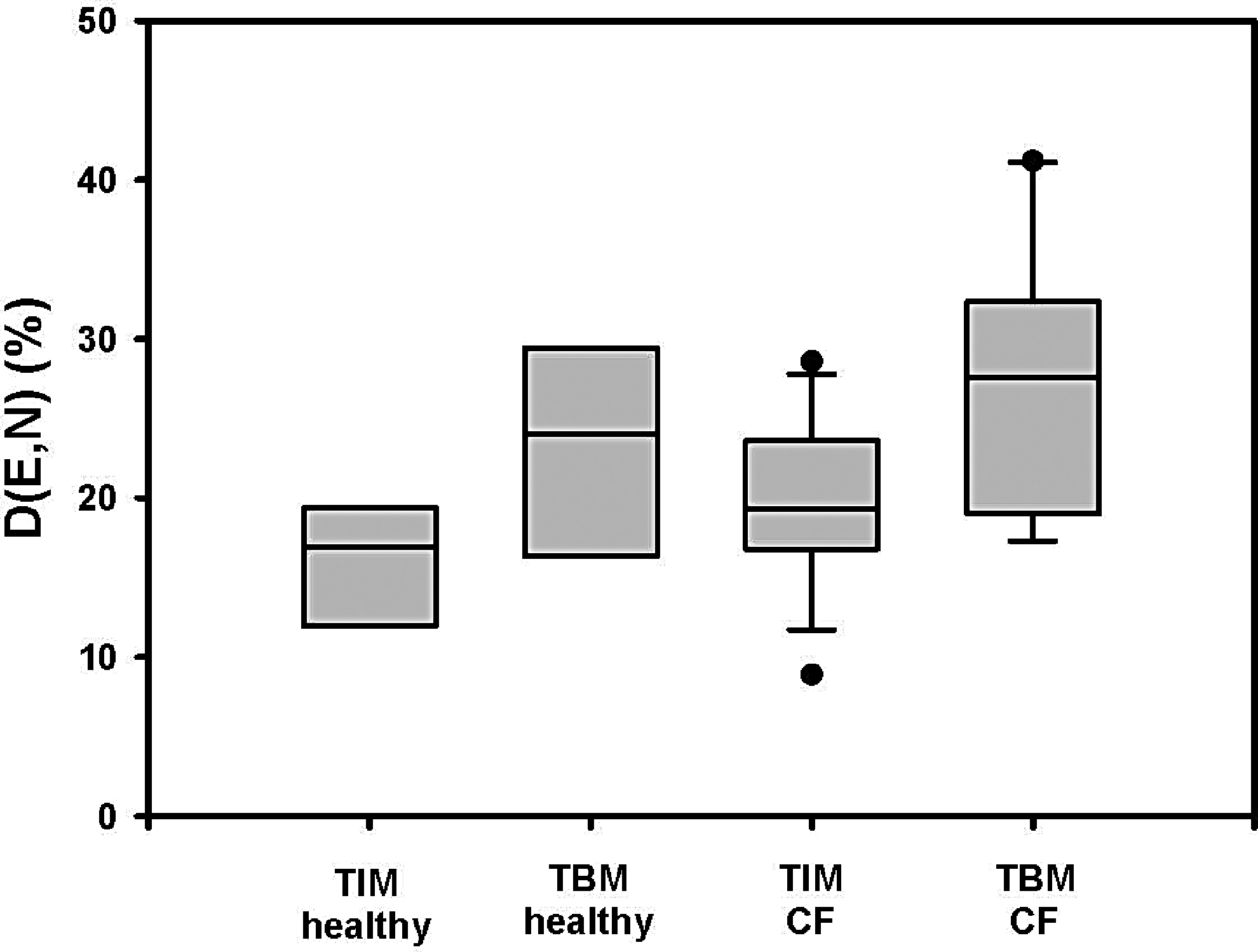
Extra-thoracic deposition in healthy subjects and subjects with CF. Drug was inhaled using the I-neb AAD System in the inhalation modes TIM and TBM.
Exhaled drug fraction relative to filling dose (MX,N) was overall very low for all groups. It was 0.8% ± 0.5% and 1.7% ± 0.7% in subjects with CF in TIM and TBM, respectively. MX,N in healthy subjects was 0.7% ± 0.2% and 2.4% ± 1.1% in TIM and TBM, respectively. Therefore, MX,N was significant lower in TIM than in TBM in both groups (healthy subjects: 95% CI [-2.6%, −0.9%]; p = 0.002; CF subjects: [-1.3%, −0.5%]; p = 0.001). Nebulizer residue relative to filling dose (DR,N) after the I-neb AAD System stopped nebulization automatically was 32.3% ± 6.5% and 24.7% ± 7.2% in subjects with CF in TIM and TBM, respectively, and in healthy subjects 33.0% ± 5.3% and 19.1% ± 7.5% in TIM and TBM, respectively. Therefore, DR,N was significantly higher in TIM than in TBM in both subject groups (healthy subjects: 95% CI [4.5%, 23.4%]; p = 0.015; CF subjects: [2.4%, 12.6%]; p = 0.008).
The distribution of drug disposition for healthy subjects and CF subjects in TIM and TBM is presented in Figure 3. The total lung deposition and extra-thoracic deposition relative to emitted dose can be seen in Table 3.
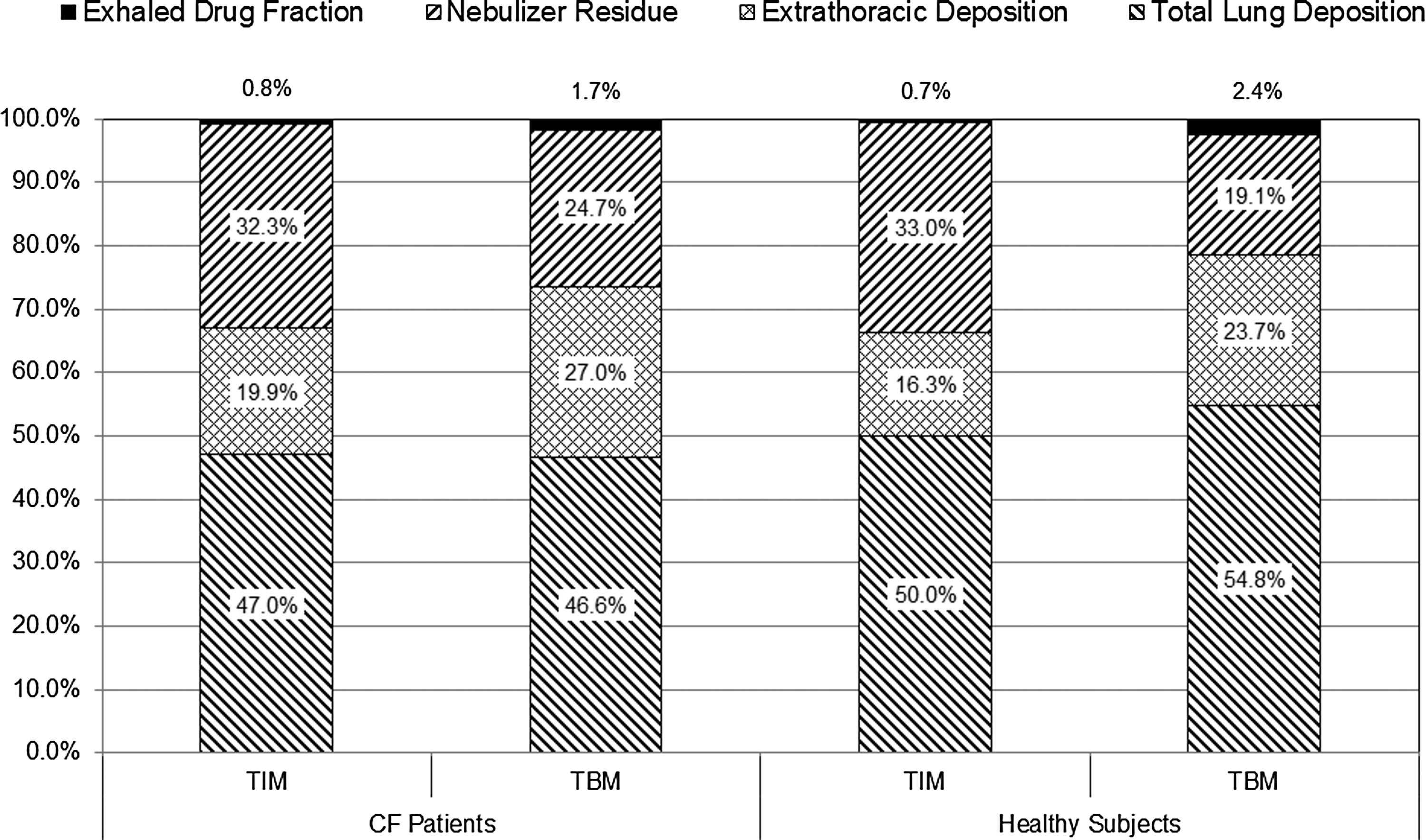
The distribution of drug disposition for healthy subjects and CF subjects in TIM and TBM.
In subjects with CF, the C/P ratio was 1.2 ± 0.2 and 1.4 ± 0.4 in TIM and TBM, respectively. The C/P ratio in healthy subjects was 1.4 ± 0.3 and 1.4 ± 0.2 in TIM and TBM, respectively. There was no significant difference, regardless of the state of disease and the inhalation mode. The variance of pixel counts (VAR) was 2.3 ± 2.4 and 2.4 ± 2.4 in subjects with CF in TIM and TBM, respectively. VAR in healthy subjects was 1.4 ± 0.7 and 1.6 ± 1.0 in TIM and TBM, respectively.
Lung function
In healthy subjects, the mean FEV1 and FVC (% of predicted) values were higher than in CF subjects, and no post-treatment changes of FEV1 (% of predicted) values were measured either in TIM or TBM 2 hours after inhalation. In CF subjects there was a small, 2 hour pre- to post-treatment decrease of FEV1 (% of predicted) in TIM and TBM. Additionally, a small 2 hour pre- to post-treatment decrease in FVC and MEF75 could be observed in TIM. In healthy subjects, the mean IC (% of predicted) values and the IVC (% of predicted) values were higher than in CF subjects, and no post-treatment changes of either value were observed in any group 2 hours after inhalation. All other lung function parameters remained stable throughout the study for TIM and TBM in healthy subjects and CF patients.
Additional endpoints
In both subject groups, treatment time was lower in TIM than in TBM for healthy subjects and CF subjects. In both subject groups, the overall inhalation time was lower in TIM than in TBM.
The mean value of inhaled volume per breath was higher in TIM (healthy subjects: 3.4 ± 0.8 L; CF subjects: 2.8 ± 1.5 L) than in TBM (healthy subjects: 1.1 ± 0.4 L; CF subjects: 2.2 ±1.2 L). The number of breaths was lower in TIM (healthy subjects: 27.8 ± 9.7 breaths; CF subjects: 22.6 ± 6.8 breaths) than in TBM (healthy subjects: 121.4 ± 20.7 breaths; CF subjects: 92.8 ± 87.0 breaths. No clear correlations between the lung function parameters, treatment time (inhalation of placebo at training and inhalation of study drug at treatment), and drug deposition (for randomized subjects) in each mode, including all measurements evaluated in subjects classified as enrolled population, were observed.
Device handling questionnaire
A handling questionnaire, which was completed by each subject on the second treatment visit, was used to evaluate device handling (convenience of inhalation, mode preference). In Table 5, only the statistical evaluation for CF subjects is reported.
N = individual number of answer per question.
Safety evaluation
Safety assessment demonstrated that a single inhalation treatment by either TIM or TBM with 77 mg of A1-PI had a good safety profile in healthy subjects and CF subjects. There were no withdrawals due to adverse events, nor was any adverse event considered related to the study drug. In total, 7 subjects experienced Treatment Emergent Adverse Events (TEAEs). One TEAE was related to study procedures. No TEAEs were considered related to A1-PI. No consistent or clinically relevant changes in lung function parameters, vital signs, and ECG were reported, and no clinically relevant changes from baseline were measured.
Discussion
This study showed that A1-PI delivered through the I-neb AAD System led to a high lung deposition of the drug. In healthy subjects, approximately 55% and 50% of filling dose in TIM and TBM, respectively, was deposited in the lungs. In subjects with CF, 47% of filling dose was deposited in the lungs, irrespective of the inhalation mode. For continuous operating jet and mesh nebulizers, a lung deposition of 5%–32% relative to the filling dose is reported depending on device type, breathing maneuver, and nebulized solution,(17–19) suggesting the advantage of a breath triggered nebulizer. The difference between TIM and TBM was not statistically significant for either healthy subjects or subjects with CF, nor between the subject groups. Therefore, a mean amount of 36–42 mg of A1-PI was delivered to the lung. This is equivalent to the previously published amount of 20–40 mg, needed to achieve local concentrations well above 8 μM, which is suggested to be the therapeutic threshold.(7,8)
Moreover, all subjects, even CF subjects with more severe lung function impairment (FEV1 < 40%) managed to inhale in TIM for the whole treatment and achieved the required lung dose. Drug distribution throughout the lung, as expressed by C/P ratio, was the same for both breathing modes within each population. In both populations, there was no difference in the variance of pixel counts between TIM and TBM. These findings indicate that the site of deposition is independent of TIM or TBM. The exhaled drug fraction relative to nominal (filling) dose (MX,N) was in general low, and similar to previous observations with the I-neb AAD System.(9)
As expected, FEV1 was generally higher in healthy subjects than in subjects with CF, and healthy subjects did not show any post treatment effects. Subjects with CF showed a small but statistically significant 2 hour post-treatment decrease of FEV1 in TIM and TBM. However, since this change is small and transient, it is not considered to be of clinical relevance. The same is true for TIM with respect to FVC and MEF75 values, again here the changes seen in subjects with CF were significant, but not of clinical relevance.
FEV1/FVC ratio measured at pre-treatment and post-treatment remained stable in healthy subjects and CF subjects.
These lung function measurements lead to the conclusion that there is no short-term effect of A1-PI inhalation on lung function. Together with the fact, that there were no adverse events related to the A1-PI inhalation, it leads to the conclusion that the safety profile of single inhalation treatment with 77 mg of A1-PI is good, for either TBM or TIM, in healthy subjects as well as subjects with CF.
Generally, TIM resulted in an about 40% shorter treatment time in healthy subjects and an even 50% shorter treatment time in CF subjects compared to TBM. In both subject groups, less extra-thoracic deposition and a higher residue of drug in the nebulizer compared to TBM was observed. The reason for the shorter treatment time in TIM mode is that the inhalation time per breath and therefore the volume inhaled per breath was lower in TBM than in TIM. In consequence, the treatment time was longer and the number of breaths needed was higher for TBM compared to TIM.
It was demonstrated that CF subjects inhaled more deeply and slowly in TIM than in TBM. TIM is consistently more efficient and less time-consuming than TBM as reflected by treatment and inhalation time and number of breaths. A treatment time of 5 minutes to inhale a dose of 77mg is considered to be very short, as also reflected in the opinion of the subjects in the questionnaire.
The evaluation of the questionnaire showed that for both inhalation modes a high percentage of CF subjects classified the use of the I-neb as “easy” and “very easy” (TIM: 71.5%, TBM: 86.7%). This shows that the TBM is still preferred over the TIM even though the treatment time is shortened by half. This may be due to the fact that, in TBM, CF patients rated the difficulty to inhale through the mouthpiece “easy” or “very easy” with 86.7% and with TIM 40%. Therefore, easiness of inhalation seems to be more important here than the reduction of treatment time by half. This leads to the conclusion that both treatment times were in an acceptable time range.
Conclusions
A filling dose of 77 mg A1-PI into the I-neb AAD System resulted in around 40 mg of drug being deposited in the lungs. This should be adequate to achieve the required local concentrations above 8 μM.
There was no significant difference in lung deposition between TIM and TBM, both in quantitative (amount) and qualitative aspects (peripheral vs. central deposition). In TBM, there was a lower device residue than in TIM, but a higher extra-thoracic deposition. Overall, TIM is the more efficient mode since treatment time is up to 50% shorter due to longer and fewer inhalations and can be handled even by subjects with FEV1 lower than 40%.
In both subject groups, treatment time and inhalation time were lower in TIM than in TBM. The fact that there was neither correlation of lung deposition nor treatment time with lung function parameters strongly indicates that CF patients can efficiently use this drug/device combination. The I-neb AAD System received positive user ratings in each treatment mode by both healthy and CF subjects. Single doses of A1-PI (77 mg nominal dose) were safe and well tolerated in TIM and TBM, in healthy subjects and in subjects with CF.
Footnotes
Acknowledgments
Source of work: A Randomized, Open Label, Cross-over Scintigraphic Evaluation of Lung Deposition of Alpha1-Proteinase Inhibitor (Human) (A1-PI(H) Inhalation Solution) using Two Inhalation Modes of the I-neb® Nebulizer in Healthy Subjects and Subjects with Cystic Fibrosis: EudraCT Number: 2010-021262-29.
Author Disclosure Statement
Sabine Häußermann, Dominik Kappeler, Christiane Herpich, Hilke Ehlich, Daniela Zanker, Claudius Kietzig, and Knut Sommerer are employees at Inamed GmbH. Jonathan Edelmann is an employee of CSL Behring LLC, King of Prussia, PA, USA. Cornelis Winnips is an employee of CSL Behring AG, Bern, Switzerland. The study was funded by CSL Behring LLC, King of Prussia, PA, USA.