
Abstract
Abstract
Purpose:
Many methods have been developed to evaluate dry powder inhalation techniques and their efficiency for disease control in asthma patients. However, it is difficult to apply these methods to clinical practice and research. In this study, we introduce a simple new method that can be applied to dry powder inhalation techniques to evaluate their efficiency in clinical practice.
Methods:
Twenty volunteers were recruited to evaluate the reliability of this new method. One hundred one asthma patients who met the inclusion criteria participated in this study. A dark cloth covered the outlet of the inhaler during dry powder inhalation. The image formed by the inhalation process was evaluated using analysis software and converted into integrated optical density (IOD). Inhalation techniques were scored before and after inhalation technique training, and asthma control was evaluated using the Asthma Control Questionnaire (ACQ) before inhalation technique training.
Results:
The relative standard deviation of IOD ranged from 3.8% to 7.8%. In patients with or without inhaler prior use, both the IOD and inhalation technique scores improved significantly after inhalation technique training (p < 0.05). Inhalation technique scores were positively correlated with IOD before (r = 0.80, p < 0.001) and after inhalation technique training (r = 0.52, p < 0.001). In patients with prior inhaler experience, ACQ results were negatively correlated with inhalation technique scores (r = −0.44; p < 0.05) and IOD (r = −0.52; p < 0.05).
Conclusion:
The results from this study demonstrated that this quantitative method is equivalent to traditional methods for dry powder inhalation evaluation. This study also indicated that training significantly improved the inhalation technique and efficiency in asthma patients with or without prior inhaler use.
Introduction
I
To improve inhalation technique,(16,17) errors made in inhalation processes should first be identified. With different inhaler devices, the critical inhaler handling errors may be different. Many methods have been developed to evaluate dry powder inhalation techniques. In one study, inhalation techniques were rated and scored according to seven omissions and five errors as quantified by trained physicians.(12,18) Other authors(19–21) have also evaluated inhalation techniques indirectly by following the clinical results of inhalation treatment; however, these observations were performed by the researchers and lacked objectivity. Furthermore, the data collected were not quantitative and were not applicable to clinical research.(22) Isotope-labeled medicines have been used to evaluate inhalation efficiency quantitatively; however, this method is not widely applied in clinical practice or clinical research due to radioactive contamination and the requirement for specialized equipment. New methods with quantitative data collection for inhalation techniques and efficiency evaluation are needed for asthma control in clinical practice.
Methods
In this study, a simple method was developed to evaluate dry powder inhalation techniques and efficiency in clinical practice. The outlet of the inhaler is covered with a dark cloth. Patients were asked to perform inhalation through the covered inhaler outlet. The medicine is blocked by and stuck to the cloth. Physicians evaluated the inhalation technique and efficiency by reviewing the medicine on the cloth; however, quantitative data cannot be collected using this method. As image analysis software has become more widely available, the image formed by medicine stuck to the cloth can be more easily evaluated quantitatively. To test the hypothesis that this method can be applied to the dry powder inhalation technique and efficiency evaluation, the repeatability of this method was initially evaluated in healthy volunteers. The method then was evaluated in 101 asthma patients, some with a history of prior inhaler use and some without.
Subjects
This study was approved by the medical ethics committee of the West China Hospital, Sichuan University. All subjects signed consents for taking part in the study. Twenty volunteers, including 10 using the Symbicort Turbuhaler (formoterol/budesonide, 80/4.5; AstraZeneca) and 10 using the Handihaler (tiotropium; Boehringer-Ingelheim), were recruited. One hundred one asthma patients who met the diagnostic criteria took part in the study. Asthma was diagnosed based on symptoms and lung function tests.(23,24) Asthma patients with a severity of more than GINA 3 were excluded. Patients with severe heart, kidney, liver, and other conditions, or age under 18 years old were also excluded from the study.
Asthma Control Questionnaire
Asthma control was evaluated using the Asthma Control Questionnaire (ACQ).(25,26) Nurses and doctors who had been trained on questionnaire administration assisted the patients in completing the forms.
Inhalation technique evaluation by steps scoring method
Inhalation techniques were evaluated by two doctors who were trained on the evaluation approach. Inhalation technique was rated and scored according to previous reports with some modifications(12,18) (Table 1). The points of the evaluation were based on identified errors or omissions in the technique that could affect medicine inhalation. The scores for one patient collected by two doctors were averaged for analysis. All patients were trained on inhalation techniques by doctors who knew the technique well. And after the correct instruction of the doctors, the patients got a period of time to exercise. After they completed inhalation correctly, they were permitted to go home. And then after 1 week, the patients completed retesting in the clinic. The patients' inhalation technique was evaluated before and after training.
Quantitative evaluation of inhalation efficiency using the integrated optical density method
Patients were asked to perform the inhalation before and after inhalation technique training. The Symbicort Turbuhaler and Handihaler were used in this study. A dark cloth covered the outlet of the inhaler. During inhalation, medicine particles stuck to the cloth and an image was formed. The image was digitally photographed (Canon PC1438). The distance between the cloth and the camera lens was fixed at 20 cm. The pictures recorded by the camera were analyzed using Image Pro Plus software (IPP, V6.0; Media Cybernetics, Inc.). Count/size order was used for the analysis. The color of the medicine stuck to the cloth was manually selected to include as much medicine as possible but excluded the background of the cloth (Figs. 1 and 2). The image files were saved as Color Segment Files (as RGE) and then loaded for automatic color selection for later analysis to keep consistency. Then, integrated optical density (IOD) (equal to the area times the density) was calculated automatically. Every image was analyzed by three different researchers who were trained on the analysis, and the average IOD value was used for analysis.

Images analyzed using Image Pro Plus. The medicine stuck to the cloth and an image was formed on the cloth. The image was recorded using a digital camera and was analyzed using Image Pro Plus software. Count/size order was used for the analysis. The color of the medicine that was stuck to the cloth was selected manually to include as many images as possible, but the background was excluded.

Images formed by the medicine stuck to the cloth and recorded using a digital camera. Asthma patients were asked to use the Turbuhaler through a dark cloth covering the outlet. The medicine stuck to the cloth and an image was formed on the cloth. The image was recorded using a digital camera.
Statistical analysis
Results are shown as mean ± standard deviation (SD). Differences before and after the training were statistically analyzed using a paired Student's t-test. Correlations were performed using a Spearman or Pearson correlation test. Significance was determined at the level of 5%. Data were analyzed using SPSS (Statistical Package for the Social Sciences, version 17.0 for Windows; SPSS, Inc., Chicago, IL).
Results
Demographic characteristics of the volunteers
Twenty volunteers (10 using the Symbicort Turbuhaler and 10 using the Handihaler) were recruited and their characteristics are shown in Tables 2 and 3. All volunteers completed the pulmonary function test and the FVC (L), FEV1/FVC (%), and peak expiratory flow (PEF) (L/min) were 2.91 ± 0.57, 85.3 ± 5.4, and 399 ± 133, respectively, in the Symbicort Turbuhaler group and 4.50 ± 1.11, 85.8 ± 2.3, and 496 ± 116, respectively, in the Handihaler group.
Values presented are mean ± SD.
FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; PEF, peak expiratory flow; SD, standard deviation.
Values presented are mean ± SD.
Repeatability of the IOD method on inhalation efficiency evaluation
All volunteers performed five inhalations and were evaluated using the IOD method. The relative SD, also known as the coefficient of variation (CV), was used to represent the precision of test results, as well as the intraclass correlation coefficient (ICC). The CV ranged from 1.6% to 7.8%, with eight of the patients having CV between 5.0% and 6.0%. These data prove the repeatability of the new methods. The ICC of volunteers using the Turbuhaler was 0.991 and the 95% CI was 0.979–0.998. The ICC of volunteers using the Handihaler was 0.984 and the 95% CI was 0.962–0.996.
Demographic characteristics of the asthma patients
One hundred one asthma patients (46 with prior inhaler use and 55 without) were recruited and their characteristics are shown in Table 4. The history of asthma in patients with prior inhaler use is 9.64 + 12.5 years and the inhaler use history is 20.61 ± 25.62 months. Among the 55 patients without prior inhaler use (20 males and 35 females), the history of asthma was 10.34 ± 12.67 years.
Inhalation efficiency evaluated using traditional methods in asthma patients
The inhalation efficiency was first evaluated using the traditional score method. The inhalation technique scores of patients with prior inhaler use were higher than patients without prior inhaler use (Fig. 3; p < 0.05). The inhalation technique scores of patients with or without inhaler use increased significantly after inhalation technique training compared with the scores before training (Fig. 3; p < 0.05). These results indicate that inhaler use history and inhalation technique training are important factors to consider in inhalation efficiency.
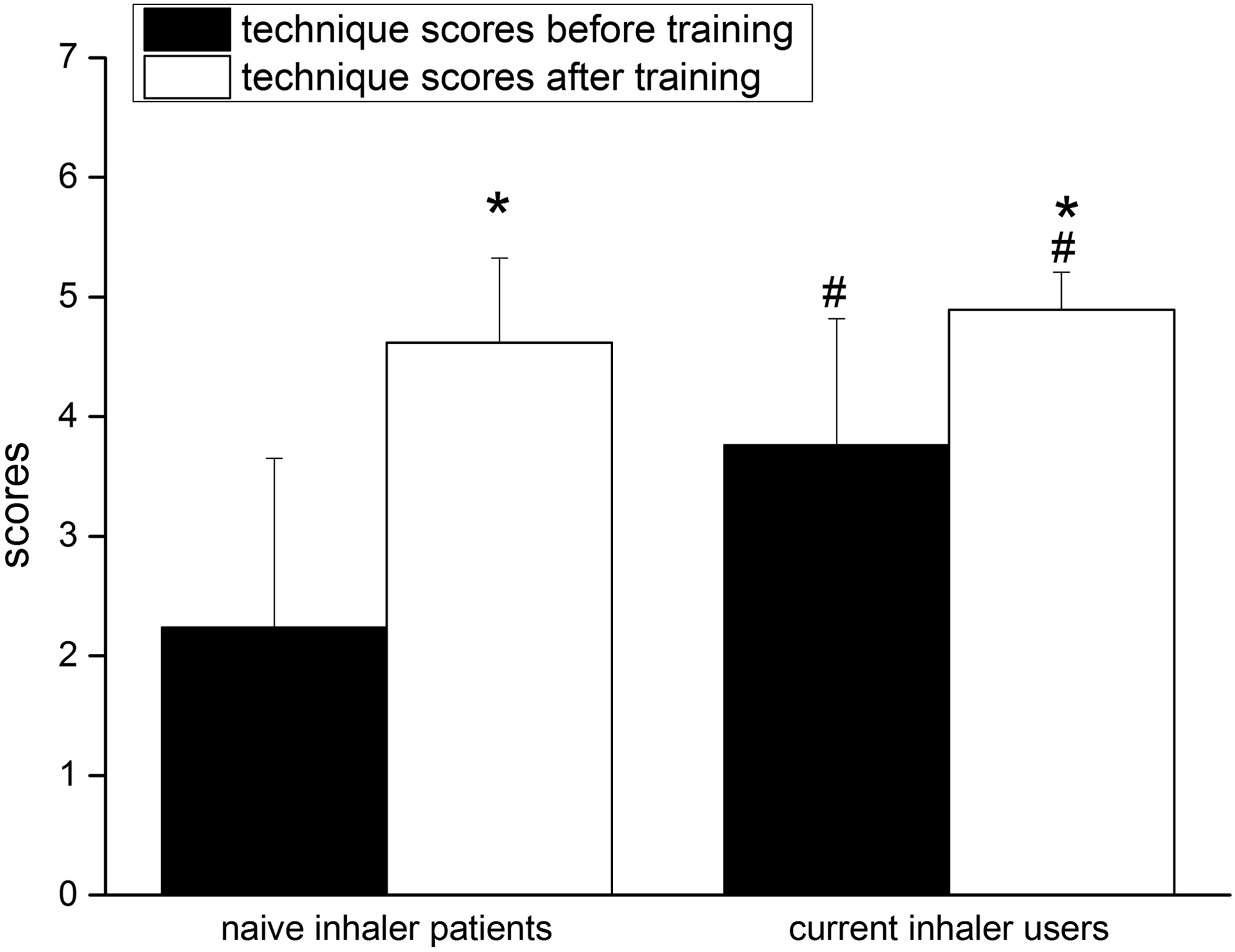
Inhalation efficiency was evaluated using the inhalation technique score method in asthma patients. The inhalation technique scores were evaluated in 46 asthma patients with prior inhaler use and 55 without prior inhaler use before and after inhalation technique training (*p < 0.05, compared with before training; #p < 0.05, compared with patients without prior inhaler use).
Inhalation efficiency evaluated using the IOD method in asthma patients
Patients with a prior history of inhaler use performed the inhalation before and after technique training. The IOD of the patients with prior inhaler use was higher than that in patients without prior inhaler use. This difference was still significant after factoring in inhalation technique training (Fig. 4; p < 0.05). These data demonstrate that inhaler use experience improves performance in dry powder inhalation. Furthermore, the IOD of the patients with or without inhaler use increased significantly after inhalation technique training compared with that before training (Fig. 4; p < 0.05), indicating that inhalation technique training can improve inhalation efficiency in asthma patients both with or without prior inhaler use.
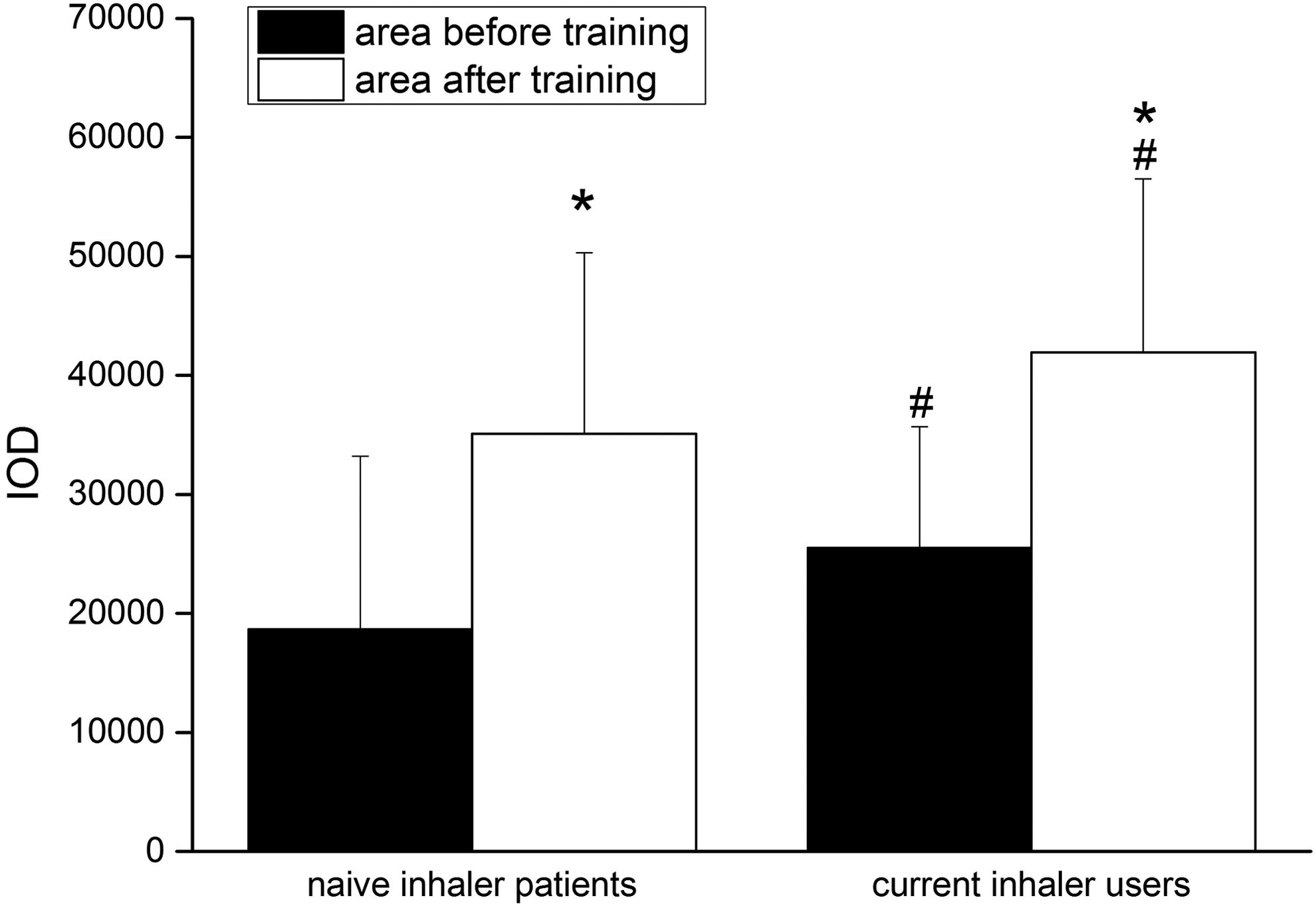
Inhalation efficiency evaluated using the IOD method in asthma patients. The inhalation efficiency was evaluated using the IOD method in 46 asthma patients with prior inhaler use and 55 without prior inhaler use before and after inhalation technique training (*p < 0.05, compared with before training; #p < 0.05, compared with patients without prior inhaler use). IOD, integrated optical density.
Correlation analysis between inhalation technique scores and IOD
Inhalation technique scores were positive correlated with IOD before (r = 0.80, p < 0.001) and after inhalation technique training (r = 0.52, p < 0.001).
Correlation analysis between inhalation technique scores, IOD, and ACQ in patients with prior inhaler use
ACQ was negatively correlated with inhalation technique scores (r = −0.44, p < 0.05) and IOD (r = −0.52, p < 0.05).
Discussion
Previous studies have indicated that the inhaler use method is related to asthma symptom control.(27,28) Evaluation of inhalation efficiency is a challenge both for physicians and clinical researchers. The traditional method used to evaluate inhalation efficiency in asthma patients involves measuring isotope radioactivity in the lungs after isotope-labeled drug inhalation. Due to its high sensitivity and specificity, the isotope-labeled medicine method has been applied to some pharmaceutical studies. However, it is not widely applied in clinic practice or research due to the radioactive contamination and specialized equipment requirements.
Scoring the key steps, which may affect the efficiency of dry powder inhalation, has been used in evaluating the process of dry powder inhalation. This semiquantitative method is based on the hypothesis that following the correct steps of inhalation will lead to higher efficiency of medicine delivery. Although it has been used widely in clinical practice and research, this method cannot directly measure the outlet of the medicine from the inhaler. Furthermore, this method is based on the subjective observation of the steps of the inhalation, not on the quantity of the medicine delivered by inhalation. Other indirect methods for the inhalation efficiency evaluation include the change in clinical symptoms and a series of indices, such as pulmonary function, fraction of exhaled nitric oxide (FeNO),(29,30) and peripheral blood eosinophils.(31)
In this study, we developed a new quantitative method for evaluating dry powder inhalation efficiency in asthma patients. We used imaging analysis software to objectively measure the medicine delivered by inhalation. After inhalation, the medicine stuck to a dark cloth and an image was formed on the cloth. The image was recorded using a digital camera and analyzed using image analysis software. With this method, the IODs of volunteers and asthma patients were calculated. The results indicate that this method has good stability and repeatability. The data collected by this method were correlated with those acquired by the score method developed by Giraud et al.(32) All of our results indicate that this method is equivalent to the traditional method.
The ACQ is a patient self-assessment questionnaire designed to evaluate asthma control based on symptoms and pulmonary function.(33) The ACQ was applied in evaluating the condition of asthma patients and their symptom control.(2,34) It has been reported that misuse of inhalers is one of the most important reasons for loss of asthma control.(12) The ACQ may also reflect the efficiency of medicine inhalation in asthma patients with prior inhaler use, as the scores of inhalation steps were negatively correlated with the ACQ results in patients with prior inhaler use. A significant negative correlation was also found between ACQ and IOD. The correlation coefficient of IOD and ACQ was greater than that of the ACQ and score of inhalation steps, suggesting that the IOD method may better reflect inhalation efficiency than the scoring inhalation steps method. The results indicate that this method can be applied to the dry powder inhalation technique and efficiency evaluation objectively and quantitatively. However, this method should be further investigated in more asthma patients using dry powder inhalers.
In this study, we also found that patients with prior inhaler use made fewer mistakes during the inhalation process than those without prior use. This result indicates that inhalation technique training is very important for patients using inhalers. This conclusion is also supported by the fact that inhalation technique training improved IOD and scores of inhalation steps, not only in patients without prior inhaler use but also in patients with prior inhaler use. Dompeling et al.(18) also stress the importance of regular instruction in inhaler technique during the treatment of asthma. Correct inhalation techniques contributed to good asthma control, reduced the waste of medicine, improved compliance, and subsequently reduced the overall disease burden of asthma.
Misuse of inhalers is very common in asthma patients. Many factors affect the correct use of inhalers, such as lack of accurate guidance from professional staff at initial use, multiple inhaler types, and complicated operation steps. Lenney et al.(35) also found that patient preference and economic conditions also affect correct inhaler use. Yildiz and Asthma Inhaler Treatment Study(36) also found that asthma control was improved after inhalation education, with significant improvement in inhalation technique and a reduction in basic errors, regardless of the inhaler type. Therefore, inhalation technique education should be emphasized in the clinical practice of asthma control.
Conclusion
The results from this study demonstrated that this quantitative method is equivalent to traditional methods. This study also indicated that training significantly improved the inhalation technique and efficiency in asthma patients with or without prior inhaler use. A future study should include larger sample or longer follow-up.
Footnotes
Acknowledgments
This work was supported by grants from the National Natural Science Foundation of China, Nos. 81470268, 30871118, 30971325, and 81270129, and grants from Ministry of Education of the People's Republic of China, No. NCET-08-0374 (F.L.). Dr. Ke Yao helped us in data analysis.
Author Disclosure Statement
No competing financial interests exist.