
Abstract
Abstract
Background:
Currently bronchial provocation testing (BPT) using mannitol powder cannot be performed in children under 6 years. A primary reason is it is challenging for children at this age to generate a consistent inspiratory effort to inhale mannitol efficiently from a dry powder inhaler. A prototype system, which does not require any inhalation training from the pediatric subject, is reported here. It uses an external source of compressed air to disperse mannitol powder into a commercial holding chamber. Then the subject uses tidal breathing to inhale the aerosol.
Method:
The setup consists of a commercially available powder disperser and Volumatic™ holding chamber. Taguchi experimental design was used to identify the effect of dispersion parameters (flow rate of compressed air, time compressed air is applied, mass of powder, and the time between dispersion and inhalation) on the fine particle dose (FPD). The prototype was tested in vitro using a USP throat connected to a next generation impactor. The aerosols from the holding chamber were drawn at 10 L/min. A scaling factor for estimating the provoking dose to induce a 15% reduction in forced expiratory volume in 1 second (FEV1) (PD15) was calculated using anatomical dimensions of the human respiratory tract at various ages combined with known dosing values from the adult BPT.
Results:
Consistent and doubling FPDs were successfully generated based on the Taguchi experimental design. The FPD was reliable over a range of 0.8 (±0.09) mg to 14 (±0.94) mg. The calculated PD15 for children aged 1–6 years ranged from 7.1–30 mg. The FPDs generated from the proposed set up are lower than the calculated PD15 and therefore are not expected to cause sudden bronchoconstriction.
Conclusion:
A prototype aerosol delivery system has been developed that is consistently able to deliver doubling doses suitable for bronchial provocation testing in young children.
Introduction
A
A diagnosis of asthma is made more likely in the presence of a family history of asthma and a personal history of food allergy, atopic dermatitis, and/or allergic rhinitis.(1) The Global Initiative for Asthma recommends a trial of treatment with short-acting bronchodilators and inhaled glucocorticosteroids.(1) The positive diagnosis is confirmed when there is a significant improvement in clinical outcomes during the treatment course followed by deterioration when the treatment is ceased.
Although an asthma diagnosis is commonly made based on the recurrence of characteristic symptoms, the diagnosis and management of asthma in older children and adults can be assisted by lung function testing including bronchodilator response. Formal tests of airway hyper-responsiveness (AHR) using direct or indirect stimuli to induce bronchoconstriction, commonly called a bronchial provocation test (BPT), may also aid in diagnosis, however the sensitivity and specificity of such tests for asthma vary with the agent used, as discussed below.
Measurement of AHR by a direct test involves administering pharmacological agents such as methacholine and histamine by inhalation. These agents act directly on smooth muscle receptors, causing the muscle to contract and the airways to narrow.(7) However, the airway response to these agents is not specific to asthma, cannot predict exercise-induced asthma, and can be affected by the drugs used to treat asthma.(7–9) Indirect tests involve administering agents such as adenosine monophosphate, or osmotic agents such as 4.5% saline wet aerosol or dry powder mannitol, that act indirectly via release of mediators (prostaglandins, leukotrienes) to cause the airways to narrow.(7) Tests that act indirectly are more sensitive than those that act directly for identifying airway inflammation and monitoring response to inhaled corticosteroids.(10–12)
The BPT using mannitol (Aridol®, Pharmaxis, Frenchs Forest, Australia) has practical superiority compared to other indirect agents delivered by nebulization. Mannitol is available as dry powder in a capsule, making the delivery simple and fast. Because of the fast administration, the rate of osmolarity change occurs quickly and makes mannitol a sensitive means of identifying AHR.(7) Mannitol is delivered in a doubling dose series: 5 mg, 10 mg, 20 mg, 40 mg, 80 mg, 160 mg, 160 mg, and 160 mg, with 635mg as the maximum cumulative dose in adults and older children. The cumulative dose causing a 15% reduction in forced expiratory volume in 1 second (FEV1) is known as the provoking dose (PD15) and is indicative of currently active asthma.(7,13) The mannitol challenge is well tolerated in asthmatic children aged 9 to 16 years(14) and 3–7 years old.(15) Children in these studies were trained before the test to generate a minimum flow of 30 L/min through the dry powder inhaler. While the mannitol standard challenge using a dry powder inhaler can be done in some young children, most are easily confused between the instructions to inhale maximally through the dry powder inhaler and expire maximally through a spirometer.
Following the inhalation of agents that act directly or indirectly, the response is measured by the subject performing a forced expiratory maneuver through a spirometer. The reliability of this test depends on the expiratory effort and therefore it is problematic to conduct in small children (≤5 years old) due to their inability to perform reproducible expiratory maneuvers.(1) Instead of using a spirometer, an alternative technique called forced oscillation technique (FOT) can be used. This technique does not require a forced expiratory maneuver, but instead measures impedance of the airway to the forced pressure oscillations produced by an acoustic speaker. It has been used successfully in children 2–5 years old(16) and 3–7 years old.(15)
Our study presents an alternative delivery system for dry powder mannitol where the powder is dispersed using an external source of air, and the pediatric subject does not need training to achieve a minimal inspiratory flow rate. These features avoid the difficulties in reproducing mannitol dispersion and deposition. The system disperses the mannitol powder into a holding chamber so the child is able to use tidal breathing to inhale the aerosol from the chamber. This research describes a novel BPT system suitable for use in children with the clinical aim of an early diagnosis.
The size distribution of the aerosols generated using this delivery system was used in a mathematical lung deposition model that predicts local lung deposition of the mannitol powder. The deposition results were then utilized to assess the maximum and minimum airway surface liquid concentration of mannitol in a pediatric model subject. Past work has included in silico models of breathing patterns and lung geometry in 4- and 8-year-old children using nebulizers.(17) Our work here used a new mathematical code to model lung deposition of dry powder in a 9-month-old infant.
Materials and Methods
Material and particle sizing
Spray-dried mannitol powder, supplied by Pharmaxis Ltd Frenchs Forest NSW Australia, was used in this work. The powder had a volume median diameter of 2.86±0.02 μm and span of 1.21±0.01. Prior to feeding the mannitol powder for the BPT system, it was first sieved through a 63 μm sieve to avoid large aggregates. The sieved mannitol was subsequently stored in a desiccator filled with silica gel until it was tested.
The particle size distributions of the mannitol powder were determined using a dry powder disperser (Scirocco 2000, Malvern, Worcs, UK) connected to a laser diffractometer (Mastersizer 2000, Malvern). The dispersive pressure was set at 3.5 bar, as this was found to be sufficient to give complete dispersion of mannitol powder without fracturing the particles. The particle and absorption refractive indices of mannitol are 1.544 and 0.100, respectively. The refractive index of air as the dispersant was 1.000.
Device components
The powder disperser used in this work is described in detail elsewhere.(18) The powder disperser (VCH10, Pisco, Illinois, USA) has two perpendicular inlets, one for compressed air and another for feeding in powder. It is available commercially and is relatively inexpensive. The compressed air flows through a small nozzle of 1.0 mm in diameter and draws the powder from the feed inlet. Then the powder is pulled through an orifice causing de-agglomeration.
A Volumatic™ inhalational device (GlaxoSmithKline Australia, Abbotsford, Victoria, Australia) was used as a holding chamber to capture the aerosolized powder exiting the disperser. It was immersed in diluted anionic detergent (1:250 v/v) for 2 hours and then drip dried. This technique has been shown in previous experiments to eliminate charge on the interior and there was no reduction in the delivery amount available from a Volumatic holding chamber when salbutamol was used.(19) The holding chamber was used within 24 hours of this detergent treatment to avoid electrostatic charge build up.
Device/experimental setup
The schematic diagram of the experimental set up is shown in Figure 1. In our prototype setup, the powder was dispersed into a holding chamber known to be suitable for inhalation via a subject's tidal breathing. A Next Generation Impactor (NGI) was used with a United States Pharmacopeia (USP) throat to simulate impaction in the throat and to support our particle characterization analysis. The components prior to the powder disperser (Fig. 1a) were used to control for the four parameters that determine the size and amount of mannitol powder delivered. These factors are (i) the flow rate of compressed air used to disperse the powder into the holding chamber, (ii) the amount of time this compressed air was applied, (iii) the amount of powder loaded into the disperser, and (iv) the time lag between powder dispersion into the holding chamber and activation of the flow that draws powder into the impactor.
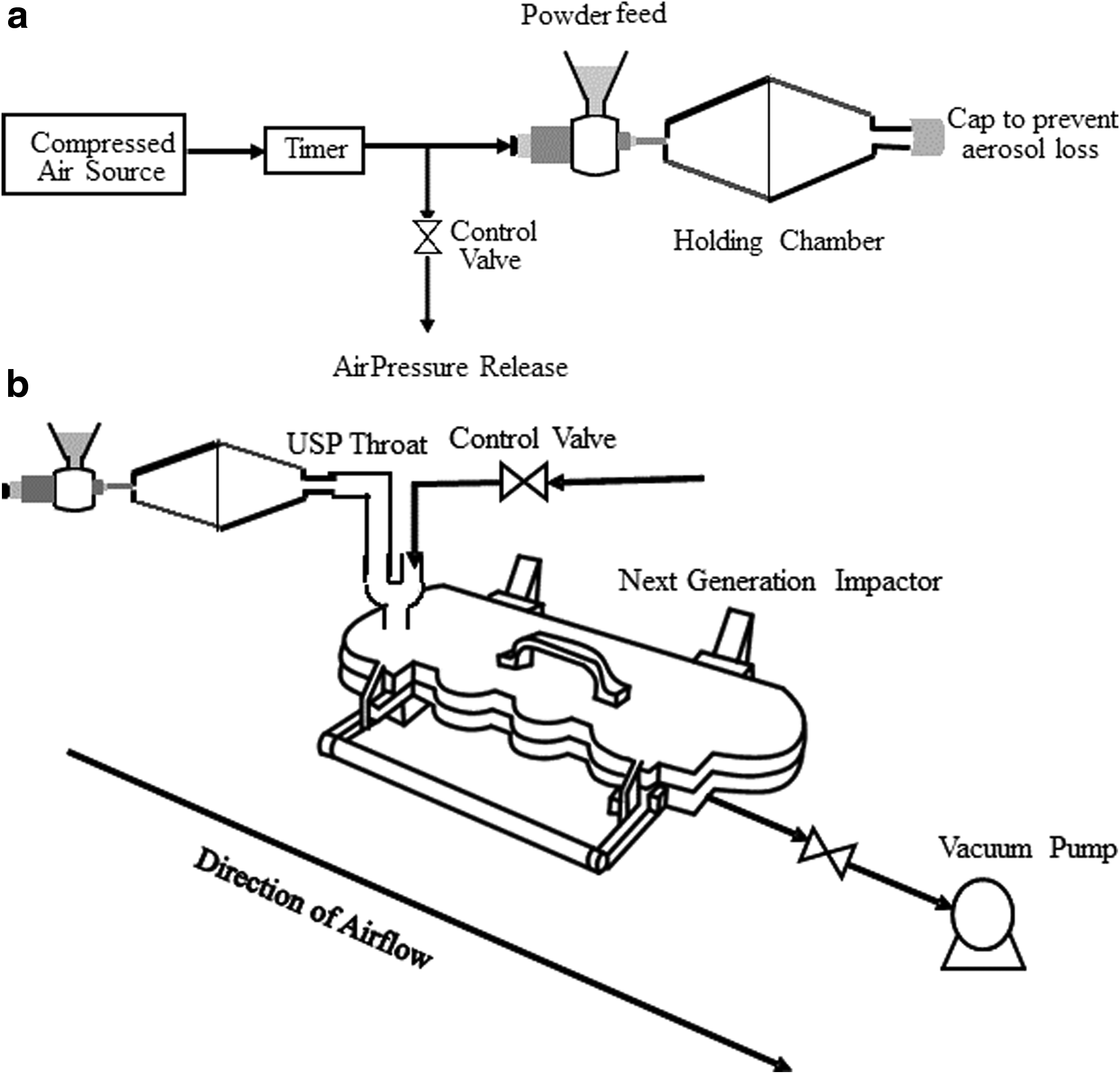
Schematic diagram of experimental setup.
Preliminary work determined viable ranges for each of these four factors. The viable flow rate of compressed air used to disperse the powder ranged between 10 L/min and 20 L/min. Flows rates below the minimum value did not force any powder through the orifice of the disperser, while the maximum flows caused high rates of impaction inside the holding chamber. The time used to apply the compressed air only yielded a reasonable output when applied for 0.2 to 0.8 seconds. Based on our previous experience in generating effective aerosolization of powders with this disperser, we chose powder loading masses between 160–650 mg.(18) The preliminary results proved the aerosols were still available, although reduced in dose, for inhalation after a lag time of 10 sec. It has been reported that a lag of 2 sec can reduce the oropharyngeal deposition of CFC-beclomethasone significantly from 84% to 3%–20% with only a slight reduction in lung deposition.(20) Therefore, the lag time between dispersion and inhalation was chosen to range from 2 to 10 seconds.
The powder was dispersed using compressed air and a timer to control the dispersion time. The holding chamber was capped before the powder dispersion to avoid the loss of aerosolized powder. After the powder dispersion was completed, the disperser and holding chamber were then disconnected from the timer. This was done in a closed chamber to avoid unintentional inhalation of the escaped aerosols. Next, the disperser and the capped holding chamber were taken out of the chamber and connected to the USP throat. The inhalation flow rate from the holding chamber was set at 10 L/min, as this was found to be the average peak of the inspiratory flow rate for children between 2–66 months.(21)
After each dispersion test, the remaining mannitol powder was sucked out of the powder disperser by using a vacuum pump until no powder remained in the disperser. The subsequent test was run with a newly treated holding chamber and done in triplicates.
The aerosols were separated based on their aerodynamic size using the NGI. The aerosols from the holding chamber were drawn at 10 L/min. However, the total flow rate through the NGI was set at 20 L/min by using a Y junction after the induction port to draw in additional air (Fig. 1b). The NGI is effective for particle size separation even at low flow rates of 15 L/min.(22) Each run lasted for 5 sec to ensure all the aerosol in the holding chamber was inhaled as would occur over several seconds of tidal breathing. At 20 L/min, the cut off diameters of the NGI from the first to the last stages are 12.2, 7.46, 4.67, 2.86, 1.80, 1.18, and 0.85 μm.
HPLC measurements and analysis
Mannitol was assayed by high performance liquid chromatography (HPLC) (Model LC-20; Shimadzu, Kyoto, Japan) using a refractive index detector (RID-10A, Shimadzu) and a C18 column (Kinetix 5 μ XB-C19 100A 150×4.6 mm, Phenomenex, Torrance, CA, USA) with filtered distilled water as the mobile phase. The sample injection volume was 100 μL and the elution time was approximately 3 minutes. A calibration curve was constructed using standard solutions of mannitol. This allowed mass determination of the powder deposited in the holding chamber, induction port, and each stage of the NGI. The fine particle dose (FPD) was then calculated as the mass of particles smaller than 5 μm.
Experimental design
The Taguchi experimental optimization method was used in this study to identify the influential factors affecting the FPD. It can be used to reduce the total number of experiments to a reasonable number when there are a large number of possible combinations of factors while capturing a representative set of conditions.(23) The four parameters with each of the values at different levels are shown in Table 1. The experimental conditions using the Taguchi design were generated using Matlab software (Table 2).
Mathematical modeling of mannitol deposition during BPT
A one-dimensional numerical dynamic lung deposition model, described by Javaheri et al.,(24) was used to simulate the effects of the various experimental cases on the deposition of mannitol in the respiratory tract for a subject inhaling tidally from the Volumatic inhalation device following powder aerosolization. Thoracic airway deposition was calculated considering inertial impaction, sedimentation, and diffusion, with the assumption that mannitol particles experience no hygroscopic size changes prior to deposition. Following the calculation of deposition in each tracheo-bronchial generation, the concentration of drug in the airway surface liquid was estimated using the model developed by Lange et al.(17) Simulations were performed using parameters representative of a 9-month-old infant inhaling tidally from the holding chamber. This age was selected due to the availability of a study for predicting nasal extra-thoracic deposition during tidal inhalation in subjects 3- to 18-months-old, with an average age of 9 months.(25) Simulations were performed using a breath profile defined by separate sinusoidal inhalation and exhalation portions and no breath hold, with an average inhalation flow rate of 10 L/min, a tidal volume of 83.3 mL, a respiratory rate of 30 breaths per minute, and a duty cycle of 0.25. Deposition and airway surface liquid concentration were calculated in each generation of the tracheo-bronchial region in lung morphologies representing 7- month and 22-month-old infants, based on the lung model of Hofmann et al.,(26) then linearly interpolated to obtain results representative of a 9-month-old infant.
Estimates of tracheal clearance velocity and daily mucus production were selected, as required in the Lange et al.(17) model, to provide both an upper and lower limit estimate of airway surface liquid concentration of mannitol in young patients. Sturm(27) described particle clearance as a function of age, speculating that for pediatric subjects, the tracheal clearance velocity increases from near zero at birth towards its maximum value in adulthood. Based on this notion, a lower bound of tracheal clearance velocity was estimated as 1.2 mm/min, while an upper bound was taken as the average value observed in adults, 5 mm/min.(27)
For daily mucus production rate, the 5 mL/day value used by Lange et al.(17) to represent typical daily mucus production in a healthy adult was used as the upper limit for a 9-month-old infant. While a lower limit of 1.5 mL/day was obtained by scaling down the 5 mL/day upper limit using the ratio of tracheo-bronchial airway volume in a 9-month-old infant (linearly interpolated based on 7 month and 22 month geometries) compared to an adult model based on the specifications of Hofmann et al.(26) The upper limit for airway surface liquid concentration corresponds to the case of high tracheal clearance velocity and low daily mucus production, with the opposite case corresponding to the lower limit.
In this work, aerosol was drawn from the Volumatic holding chamber at a rate of 10 L/min for 5 sec, yielding an inhaled volume of 833 mL. Compared to a constant inhalation flow rate, a subject inhaling tidally with an average flow rate of 10 L/min will require more than 5 sec to inhale an equivalent volume of air. In the 9-month-old breath profile defined above, 10 breaths were required to inhale 833 mL, with a total duration of 20 seconds. Particle sedimentation in the holding chamber, which acts to reduce the aerosol concentration over time, ultimately results in a lower dose of drug reaching the patient as compared to the case of a constant inhalation flow rate.
A mathematical model predicting the reduction in aerosol concentration in a holding chamber over time due to sedimentation and the removal of dose at each breath(28,29) was thus employed to account for this difference in inhaled mass. The results of this modeling revealed, as expected, a decrease in the mass inhaled from the chamber. This ranged from 38% to 54% of the experimentally measured inhaled mass, which was taken as the sum of deposition in the USP and on each plate of the NGI. This considerable difference reflects the long duration required for a patient to inhale tidally the entire volume of the holding chamber compared to a constant inhalation at 10 L/min.
After accounting for a reduction of the inhaled dose due to deposition in the Volumatic chamber, a deposition correlation(25) was used to estimate nasal extra-thoracic deposition in the 9-month-old infant model. The one-dimensional lung deposition model was then used to calculate trachea-bronchial deposition on a generational basis, while airway surface liquid concentration was estimated using the chosen model.(17) Particle size distributions were calculated assuming a log-normal distribution based on the MMAD and GSD derived from impactor measurements with the NGI.
Results
Validation of dosage parameters
The nine different conditions derived from the Taguchi method were tested with the USP throat to determine the amount and reliability of their FPD delivery rates (Fig. 2). Experiment ID 3 resulted in the lowest FPD (0.8±0.09 mg). Conditions 2, 1, and 5 were also selected for administered doses during BPT as the FPD roughly doubled in each step to 1.51 mg, 3.33 mg, and 6.39 mg.
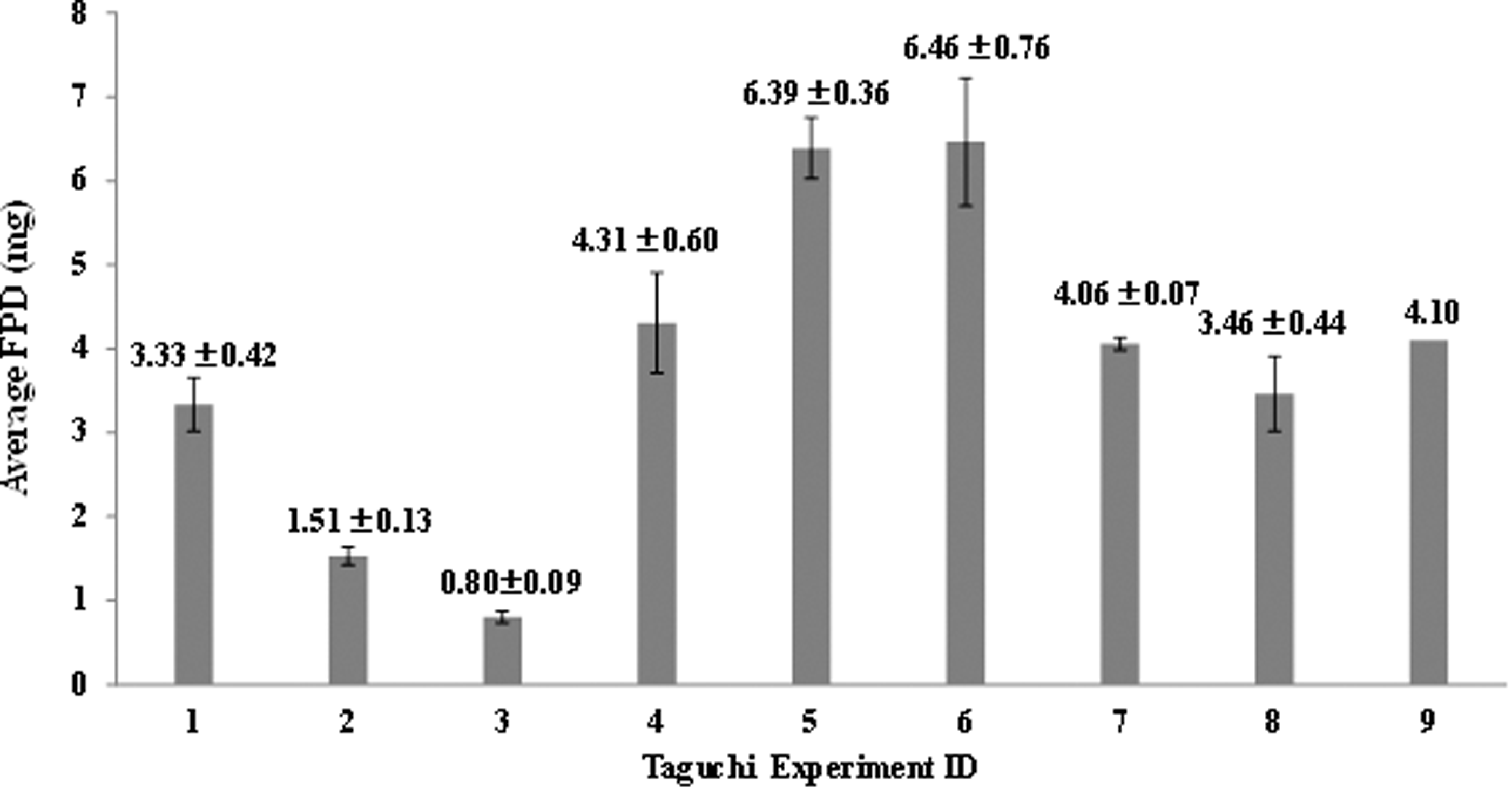
The FPD (<5 μm) obtained from different experimental conditions. N=3, except for ID 9 where n=1; the error bars represent±1 SD.
Notably, conditions 7–9 had 640 mg of loaded powder and delivered a lower FPD than the middle conditions 4–6 that had only 320 mg. There was a large amount of residual powder left in the disperser in the 640 mg feed powder condition. Although the powder disperser delivered a consistent dose, its delivery efficiency is very low (FPD/loaded dose <2%).
Potential dosage series testing
Table 3 shows the FPD and deposition in the holding chamber and the USP throat. This proposed dosage sequence mimics the adult BPT which starts with a low dosage that is then doubled after each inhalation cycle until the highest dose is reached. Although the highest reliable dose we could deliver was not as large as the equivalent adult dosage, we were able to reach the final dosage level by using two powder dispersers with the same holding chamber in quick succession. Separate dispersers were used for two reasons, (1) speeding up the process of dosing a child in a clinical setting, and (2) running two dispersions consecutively into the holding chamber without an inhalation cycle in between resulted in a higher impaction losses and a lower dose delivery. This disperse-inhale-disperse-inhale pattern was used for the highest dose testing with the USP throat.
Calculation of PD15 for children based on anatomical data
Anatomical data about airway surface area for children at various ages
30
was used to calculate their PD15. A scaling factor was developed based upon the surface area airway of an 18 year old. The calculation was done using the formula:
This scaling factor was then multiplied by the PD15 data for adults to create an estimated value for the amount of mannitol required to provoke a response in children (Table 4). This data informed the choices we made in the dose sequence described in Table 3.
Mathematical modeling of mannitol deposition during BPT
The simulation predicts considerable deposition of mannitol in the extra-thoracic region for each ID, with more deposition occurring for larger particles. As such, the mass median aerodynamic diameter of particles not depositing in the nasal extra-thoracic airways can be expected to decrease; a lower total mass of aerosol, consisting of particles with a smaller average size, continue distal to the extra-thoracic region as compared to the aerosol inhaled at the nose or mouth.
The results of the calculations are summarized in Figures 3 and 4. In general, increased FPD corresponded well to increased deposition and higher airway surface liquid concentration in the more distal portions of the conducting airways. In the first few generations of the respiratory tract, increased deposition is predicted to occur in cases ID 2 and ID 3 compared to trends observed in ID 1, ID 5, and ID 5x2. In all IDs, airway surface liquid concentration was highest in generations 0 to 6, the initial stages of the conducting airways. Low alveolar deposition was observed in all IDs. A summary of the overall deposition in the tracheo-bronchial region, along with extra-thoracic and alveolar deposition, is given in Table 5. The maximum airway surface liquid concentration was similar among ID 1 and ID 2. Clearly, the majority of deposition occurs proximally in the trachea-bronchial region in all IDs.
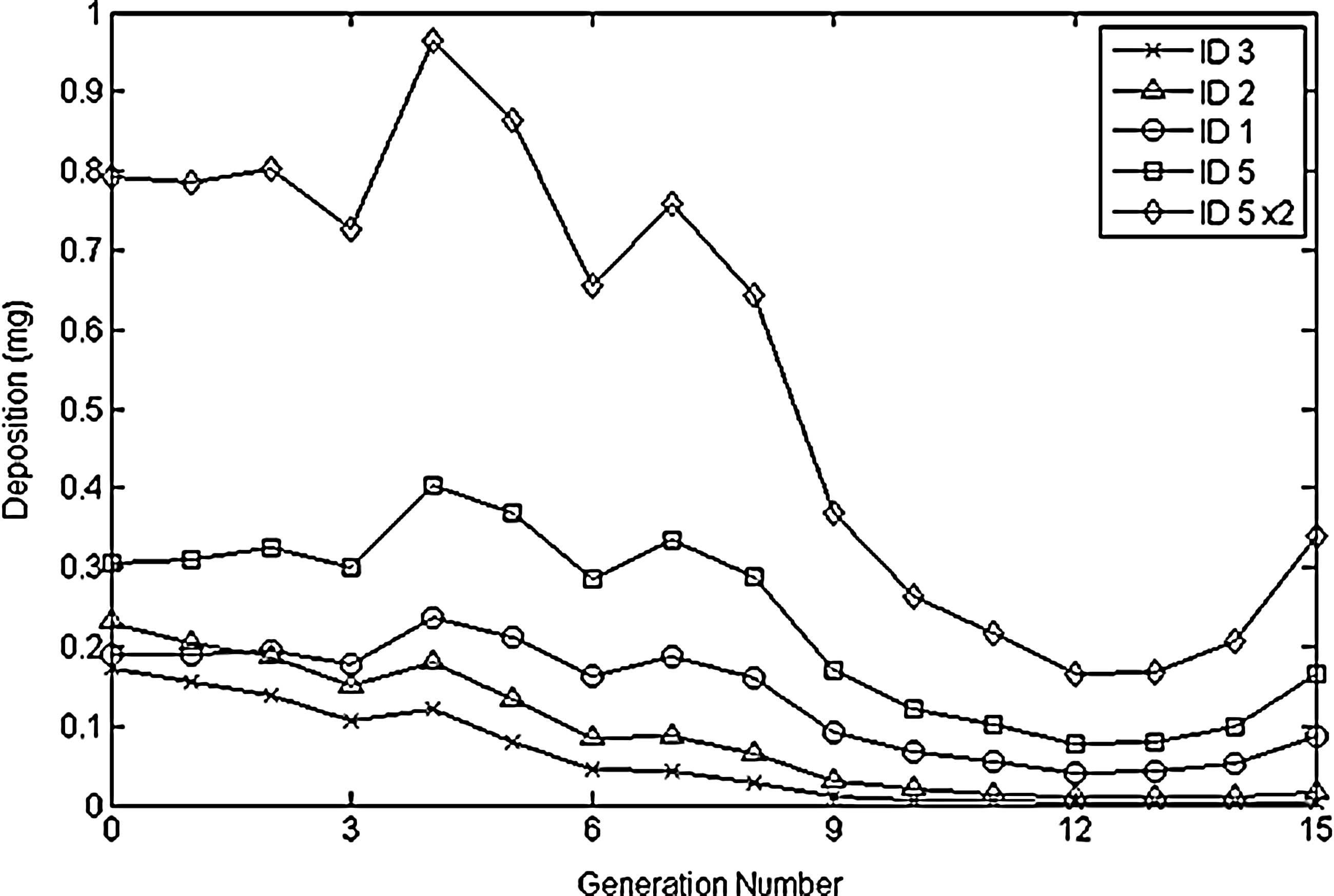
Predicted deposition of mannitol in the tracheo-bronchial region for a 9-month-old subject breathing tidally from a valved holding chamber during bronchial provocation testing.
Predicted upper (top) and lower (bottom) bounds of airway surface liquid concentration of mannitol in a 9-month-old infant during bronchial provocation testing.
Discussion
Validation of dosage parameters
In Taguchi experiment ID conditions 1–3 with 160 mg powder feed, the FPD is decreased with a combination of higher flow rates, longer dispersion times, and increased lag time. With higher flow rates, the powder exiting the disperser travelled faster, causing impaction loss and retention in the holding chamber as shown in Table 3. ID 1 with the compressed air flow rate of 10 L/min produced the highest FPDs. Figure 5 shows a large amount of mass deposition in stage 1 from experiment IDs 2 and 3, compared to ID 1. The particle size distribution reaching the impactor is the result of de-agglomeration in the disperser, sedimentation and impaction losses in the holding chamber, as well as deposition losses in the USP throat, with each depending on upstream effects on particle size. For this reason, it is thus difficult to identify the precise mechanism. The lower flow rate and shorter lag and dispersion times of experiment ID 1 do however appear to provide optimal dispersion of particle sizes that lead to minimal deposition losses, in comparison with IDs 2 and 3. Thus, 10 L/min is sufficient in providing effective de-agglomeration with 160 mg of powder feed.
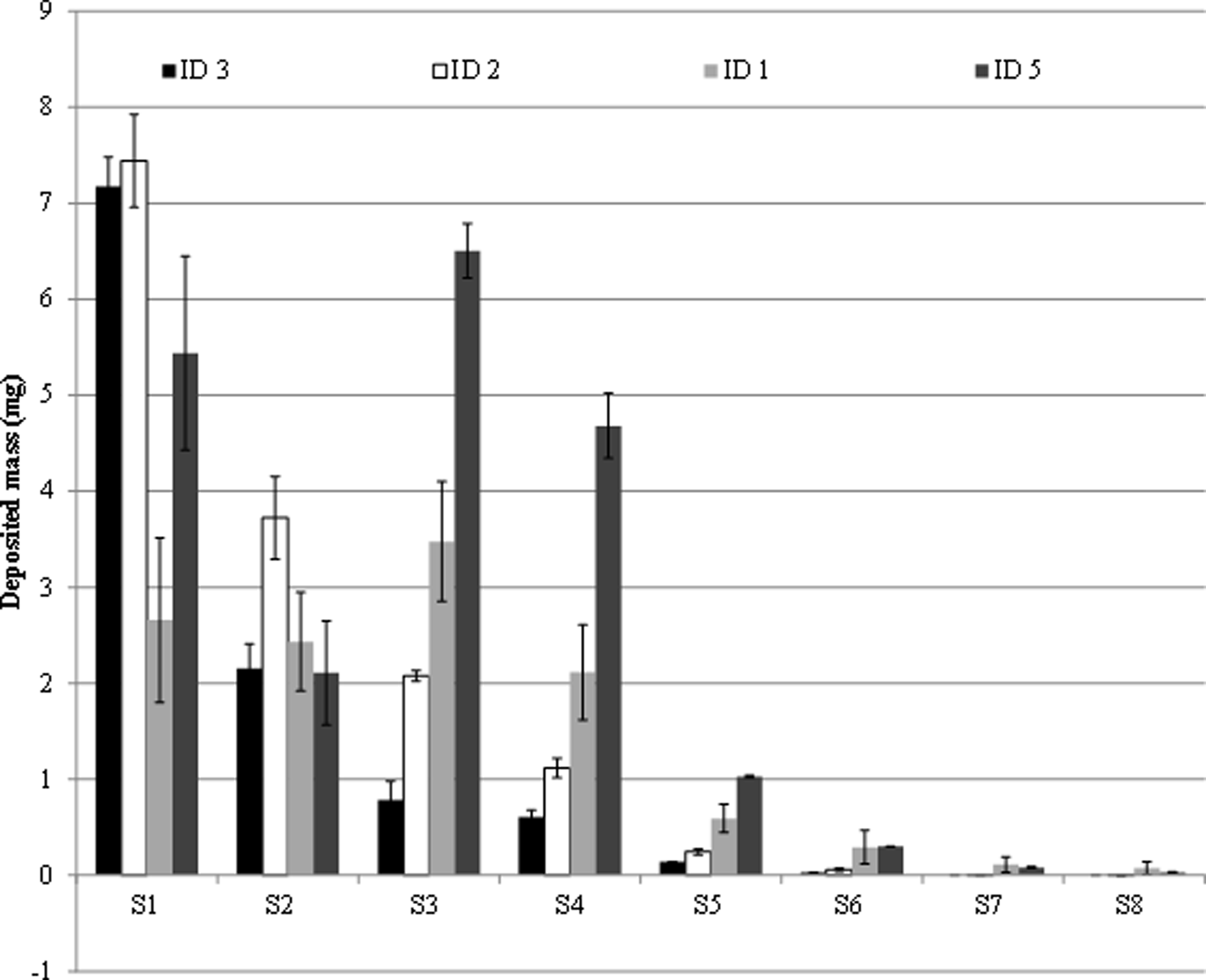
Mass deposition in each stage of the NGI for the Taguchi ID's used in our proposed dosage sequence.
Experimental ID 5 had the smallest standard deviation due to the use of a higher flow rate. This trend can be seen across all three sets of powder feed mass conditions: faster flow rates produce a smaller standard deviation. This indicates that higher flow rate aerosolizes a more consistent amount of powder into the holding chamber.
Although the powder feed in experiment ID 7 to 9 was high (640 mg), the FPD was very low. This is because the flow rate was not high enough to draw the powder through the disperser orifice. This was shown in the larger amount of powder left in the disperser (range: 75 to 88% for experiment IDs 7 and 8). Experiment ID 9 was only done once since the FPD obtained was also low. Due to the high levels of powder residue in Experiment IDs 7–9, we tried dispersing the powder twice, but the FPD did not increase.
Potential dosage series testing using the USP throat
The mass depositions in the USP throat (Table 3) from the chosen Taguchi experiment IDs were quite small (0.20±0.01 to 4.18±0.15 mg). The small throat depositions may minimize the chance of a significant cough response in pediatric subjects. Although Subbarao 31 found that coughing did not appear to affect the airway response to mannitol, the presence of excessive coughing will prolong the time between inhalation and measurement of FEV. This could lead to a decrease in the effectiveness of the osmotic stimulus and therefore generate false negatives.
Calculation of PD15 for children based on anatomical data
Phalen et al.(30) measured the length and diameter of human airway generations 0 to 8 (0 represents tracheal, 1–8 represent bronchi) based on 20 replica airway casts of cadavers aged 11 days to 21 years. The surface area was then calculated based upon the surface area of a cylinder. The airway dimensions versus body height were then fitted by linear regression (R2=0.97).(30) The surface area of our adult was calculated using an age of 18 years. The PD15 of 43 asthmatic patients aged 18 to 39 years of age who performed a BPT with mannitol was 64 mg (95% confidence interval of 45 to 91).(32) However, it has been pointed out that postmortem shrinkage of cadaver airways might take place and there can also be distortion of the airway geometry during the casting process.(33) We assumed the processes of shrinkage and casting distortion occurred at similar rates for adults and pediatric cadavers.
The calculated geometric mean values of PD15 between the age of 6 to 12 and between 6 to 14 years are 38.3 and 41.1 mg, respectively (Table 4). Our calculated values are in agreement with the in vivo values obtained from a clinical study where BPT was administered to 25 children aged 6 to 13 years old;(31) where the mean value of the PD15 was 38.5 mg (CI of 19.1 to 77.8).
The predicted values of PD15 listed in Table 4 should be used with caution. Pharmacokinetics and pharmacodynamics differences between adults, children, and infants might imply different treatment efficacy or risk.(34) Therefore, it would be best to start the BPT challenge from a low dose that could be repeated twice before introducing higher doses. The predicted PD15 value implies that in subjects younger than 4 years old the bronchoconstriction will take place after the administration of experiment ID 5(x2) with a cumulative FPD≤5 μm of 25.88 mg. The predicted maximum PD15 is much higher than any of the FPDs generated by the proposed dosage sequence, which indicates that our system should be safe.
The FPD generated by the proposed set up showed good reproducibility (standard deviation less than 16%). The Volumatic holding chamber used has a volume of 750 mL. For a child breathing at 10 L/min (167 mL/sec), the aerosol inside the holding chamber would be emptied in approximately 4.5 seconds. The FPDs in Table 3 were collected over 5 seconds. Since the powder was first dispersed into the holding chamber, instead of being inhaled directly by a subject, there is a more or less uniform distribution of aerosolized powder in the chamber. Assuming a constant rate of aerosol being inhaled, the calculated inhalation rate varied from 0.16 mg/sec (ID 3, Table 3) to 1.3 mg/sec (ID 5, Table 3). Taguchi ID 5(x2) was obtained by dispersing ID 5 two times (sequence: first 320 mg dispersed and inhaled, second 320 mg dispersed and inhaled). Therefore, the aerosol inhalation rate will also be 1.3 mg/sec. The FPD inhaled by the subject during each second of inhalation would be significantly lower than the calculated maximum PD15 (Table 4) and consequently the child should not experience sudden bronchoconstriction.
Mathematical modeling of mannitol deposition during BPT
From the results of the mathematical modeling, of interest is the observation of increased deposition in the initial few generations of the tracheo-bronchial region, corresponding to the region between the trachea and the segmental bronchi, in ID 2 and ID 3 compared to trends in other doses (Fig. 4). This is likely caused by the relatively large particle sizes measured in ID 2 (mass median aerodynamic diameter, MMAD, is 7.75±0.16 μm with geometric standard deviation, GSD, of 1.53±0.03) and ID 3 (MMAD=8.29±0.14 μm, GSD=1.34±0.04), resulting in increased impaction in the first few generations of the tracheo-bronchial region. The MMAD obtained for ID 1, 5, and 5(x2) are all smaller than 4.78 μm.
The low alveolar deposition is likely a consequence of considerable filtration by the bronchial airways combined with the short duration of periodic breathing. As no pause was included between breaths, the effective time for particle sedimentation and diffusion in the pulmonary airways was limited. As shown in Figure 4, the scenario of high airway surface liquid concentration corresponds to approximately an order of magnitude greater concentration in all generations as compared to the case of low airway surface liquid concentration. This indicates that daily mucus production and tracheal clearance velocities can have a large effect on the concentration of drug depositing in the respiratory tract. It is unknown as to what extent the increased deposition of mannitol in the initial few generations of the lung in IDs 2 and 3 will have on the BPT. Although the majority of deposition occurs proximally in the trachea-bronchial region in all IDs, the relative importance of deposition in the trachea and the first few generations compared to the more distal conducting airways requires further investigation.
Conclusion
We have developed a prototype of a delivery system for a BPT challenge using dry powder mannitol for children younger than 6 years old. The prototype uses an external source of air to disperse the powder and is independent of the subject's inspiratory effort. This system could be used for other subjects who are unable to generate an adequate inspiratory flow rate to inhale from a DPI. The FPDs were generated in a doubling dose sequence, as in the BPT challenge in adults, with standard deviation less than 16%. The FPD can be adjusted easily by a clinician within a relatively wide range of doses. The system uses commercially available parts with no modification required and the parts are readily assembled. This means the system can be adopted for use in a clinical setting with no specialized equipment. Future research, possibly paired with spirometry or FOT, could lead to a clinically sound asthma diagnostic test for children under 6 years old not requiring any inhalation training.
We recognize several limitations of this work and note several potential improvements for future research. A breath simulator, if available, could be used to better represent the tidal breathing generated by the pediatric subjects. Modifications in the powder disperser, such as adding a baffle to capture the large particles before exiting the disperser, or introducing a swirling air pattern to enhance the de-agglomeration, could be explored in future research to improve delivery efficiency.
Footnotes
Acknowledgments
The study was financially supported by the National Health and Medical Research Council (NHMRC) through a Development Grant. H.-K. Chan is also grateful to Mr. Richard Stenlake for his generous financial support. The mannitol powder used in this work was kindly donated by Pharmaxis, Australia.
Author Disclosure Statement
No known conflict of interest exists between any author and supplier used in this study. Drs. Anderson, Brannan, and Chan currently receive royalties related to the Aridol® test for people 6 years and older.