
Abstract
Abstract
Background:
Hypertonic saline (HS) has been established as a therapy aimed at restoring the surface liquid of airways liquid and enhancing mucociliary clearance in patients with cystic fibrosis (CF). A formula containing 7% HS and 0.1% hyaluronic acid (HA) is also available, basing its use on the protective effects of HA against elastin injury and on its greater ease of administration (i.e., the perceived acceptability of inhalation). This study explores the effect of HA+HS in reducing the inflammation of airways, by measuring cytokine levels in sputum, its safety profile, and the prevalence of commonly reported symptoms like cough, throat irritation, and saltiness.
Methods:
In a pilot, double-blind, randomized controlled, parallel-group, 1:1 trial, clinically stable CF patients older than 6 years of age and with a FEV1pred. >40% were randomized to one of the treatment arms, HS or HS+HA, to be administered twice a day at home. Clinical data, inflammatory markers (IL-1β, IL-6, IL-8, IL-10, TNF-α, VEGF) in sputum, and judgments on the tolerability and pleasantness were collected at the beginning and after 28 days.
Results:
HA+HS had no significant effect on inflammatory markers versus HS alone, as shown by broad confidence intervals. In the HS+HA group, the highest decrement from baseline values was observed for IL-1β (−58.8%) followed by VEGF (−49.9%), whereas in the HS group a significant increment of IL-10 levels (+83.0%; p = 0.011) was the only significant finding. Prevalence of unfavorable scores was 36.8% in HA+HS versus 55% in HS group (p = 0.207); no significant differences were detected in the prevalence of moderate/severe symptoms of cough, saltiness, and throat irritation in pulmonary functions tests after 28 days.
Conclusions:
HS+HA administration in CF patients does not show any significant effects on lung inflammation and function as compared to HS alone.
Introduction
L
The role of epithelial cells, macrophages, and other immune cells in the pathogenesis of CF lung disease has been revealed in recent years. However, these cell-mediated immune responses may not remove pathogens or are diverted and/or disabled. For example, neutrophils are activated and give off high amounts of elastase when they enter the airways attracted by high levels of chemotactic factors. Increased neutrophil elastase levels are considered a biomarker of disease progression, predicting the decline of lung function and bronchiectasis.(2) The dysfunction in the inflammatory and immune responses leads to secretion of growth factors, including vascular endothelial growth factor (VEGF) and epidermal growth factor (EGF), which are believed to contribute to the remodelling of CF airways.(3)
Current therapy for CF targets the restoration of the proper intraluminal hydration of the airways.(4) Thus, regular inhalation of hypertonic saline (HS) improves lung function within 2 weeks,(5,6) and its beneficial effects are maintained as long as inhalation is continued, at least for 48 weeks.(7) For patients with CF older than 6 years of age, the Cystic Fibrosis Foundation recommends the chronic use of inhaled HS to improve lung function and to reduce exacerbations.(8) However, a European consensus document concluded that, based on large individual differences in response to dornase alfa and hypertonic saline found in a comparative study,(9) long-term prescription patients should firstly be tested on an individual basis.(10) Moreover, tolerability of HS treatment is still an issue, since a meta-analysis of studies examining regular HS inhalation for patients with CF indicated intolerance due to cough or other respiratory symptoms only in 3% and 8% of patients, respectively.(11)
The potential usefulness of hyaluronic acid (HA), a glycosaminoglycan responsible for water content and homeostasis in the extracellular matrix, in improving airway hydration and reducing the effect of neutrophil elastase has been described in vitro and in vivo.(12–14) In addition, treatment of CF mice with nebulized high molecular weight HA for 3 days was sufficient to reduce lung inflammation.(15) Clinical experience of HS with or without HA in CF so far indicates higher tolerability and pleasantness of the former,(16,17) documented as perceived acceptability of inhalation, as well as reduction in the need for other medications.(18,19) So far, no study has been carried out on the effect of HS+HA on the inflammatory response in CF patients' airways.
The aim of the present study is to estimate the treatment effects of HS with or without HA in reducing airway inflammation, as measured by cytokine levels in sputum. Secondary aims are safety outcomes (adverse effects with the treatment), assessment of the prevalence of commonly reported symptoms like cough, throat irritation, and saltiness, and changes in pulmonary function.
Materials and Methods
Study design
This was a pilot, double-blind, randomized controlled, parallel-group study, carried out at the Regional Reference Centre for Cystic Fibrosis in Milan, Italy, between June and October 2012, comparing the role of HS+HA (Hyaneb, Eupharma s.r.l., Bologna, Italy) versus 7% HS alone in modifying airway inflammation. The study was approved by the local regulatory authority and ethics committee of the Fondazione IRCCS Cà Granda Ospedale Maggiore Policlinico (nr 685, 618/11-all.3). Written informed consent was obtained from patients, parents, or legal representatives before the enrollment of patients into the study.
Study population
Enrolled patients were clinically stable, older than 6 years, and with predicted forced expiratory volume in 1 sec (FEV1pred.) >40%, with no previous exposure to HS or rhDNase therapy. Patients were excluded from the study if they presented any of the following: Burkholderia cepacia infection, uncontrolled bronchospasm, pulmonary exacerbation, hemoptysis, or change in chronic therapy in the 30 days preceding inclusion. Subjects on lung transplant waiting list or on non-invasive ventilation were also excluded.
Randomization
Eligible patients were randomly assigned by means of a computer-generated randomization list to receive one of the two treatment regimens with a 1:1 allocation ratio. Identical sterile vials containing 5 mL of water solution of 7% NaCl (HS) or 7% NaCl plus 0.1% sodium hyaluronate 400 kDa (HS+HA) were prepared, packaged, labelled by C.O.C. Farmaceutici S.r.l. and supplied free of charge by Eupharma S.r.l., which did not take part in the study in any of its stages.
Participants, study coordinator, and outcome assessors were not aware of the assigned treatment. Investigator had access to a sealed envelope containing the randomization code of patients, to be opened in case of a medical emergency. Data entry and analysis were performed before breaking the randomization codes.
Procedure
Subjects received either treatments by PARI TurboBOY® device with PARI LC® Plus nebulizer, twice a day for 28 days.
During the screening visit, subjects inhaled 200 μg of salbutamol with a valved-holding chamber before test formulations. Spirometry was performed three times at the first administration: basal, 15 min after salbutamol, and 15 min after the administration of the test products. Body plethysmography was performed at study initiation and after 28 days. Lung volumes were measured by a 830 liters plethysmograph (Master Screen Body 4.2, E. Jaeger GmbH) in the sitting position, according to ATS/ERS guidelines.(20) Flow and volume were measured by a pneumotachograph with a 0.036 kPa L/-1s resistance and 160 ml dead volume. Calibration with three liters syringe was performed every day before testing.
Patients who tolerated the assigned treatment were given 59 blinded vials to be used twice daily for 28 days. After the first inhalation of the blind vial, each patient was asked to complete a questionnaire regarding symptoms (cough, throat irritation, and saltiness) using a four-point ordinal score: 1 = absent, 2 = light, 3 = moderate, and 4 = severe. Patients also expressed a pleasantness judgment on the treatment through a visual analogic scale (VAS).
Sputum samples from each patient were collected during the first and last visit, and processed as previously published.(21) One was used for microbiological culture and the other for qualitative and quantitative analysis of inflammatory markers. Sputum sampling occurred during spontaneous cough.
The last administration of the test products was given in the hospital, where patients repeated all the measurements described and underwent clinical examination, including spirometry as performed during the screening visit. Patients were asked to bring all remaining vials to assess for adherence to the procedure.
Study outcomes
To address the primary outcome, inflammatory marker (IL-8, IL-1β, IL-6, IL-10, TNF-α, VEGF) levels were measured in sputum samples before and after assigned treatment for 28 days. Analyte levels were measured by the Magnetic bead-based Multiplex immunoassay Bio-plex (Bio-Rad).
Safety of the treatment was assessed by adverse events that occurred after receiving the trial treatment. These included: bronchospasm, defined as a drop in FEV1 pred. of >15% after the first administration of the test products, hemoptysis, highly distressing cough or vomiting, and clinical signs and symptoms causing concern.
Secondary outcomes included prevalence of moderate/severe cough, throat irritation, and saltiness, measured by the four-point ordinal score, prevalence of unpleasantness score by VAS and spirometric data obtained after 28 days.
Statistical analysis
As recommended by Julious, we have based this study on a sample size of at least 12 patients per group.(22) To compare treatment groups, change from baseline as well as analysis of 95% confidence intervals for mean difference or generalized Hodges-Lehmann median difference were considered. Between and within-groups analysis used unpaired and paired-analysis based on the t and U distribution; normality of data was checked through Shapiro-Wilk test. The Cochran-Mantel-Haenzel test corrected for the number of administered vials was applied to analyze prevalence of moderate/severe symptoms (score 3 and 4) of cough, throat irritation, and saltiness after 28 days; the same test was applied to analyze prevalence of unpleasant score, defined as VAS <6. Likewise, prevalence of unfavorable symptoms from and overall pleasantness of the study product was assessed after the first inhalation, and corrected for disease severity (FEV1 pred.). All group comparisons were performed by intention-to-treat (ITT) analysis through mean imputation. Data were analyzed with STATA®11.2 (StataCorp, College Station, TX, USA).
Results
Demographic characteristics, pulmonary function tests, presence of Pseudomonas aeruginosa respiratory infection, and inflammatory marker levels at baseline are shown in Table 1. Groups were similar with the exception of age, pancreatic sufficiency, and disease severity, as expressed as FEV1 pred. and FEF25-75. Patients in HS+HA group were younger, with normal pulmonary function (mean FEV1 pred. >90%), while 25% of patients in the HS group showed moderate lung disease. Because this was a randomized trial, this difference occurred purely by chance. The flow diagram(23) for this clinical trial is displayed in Figure 1.
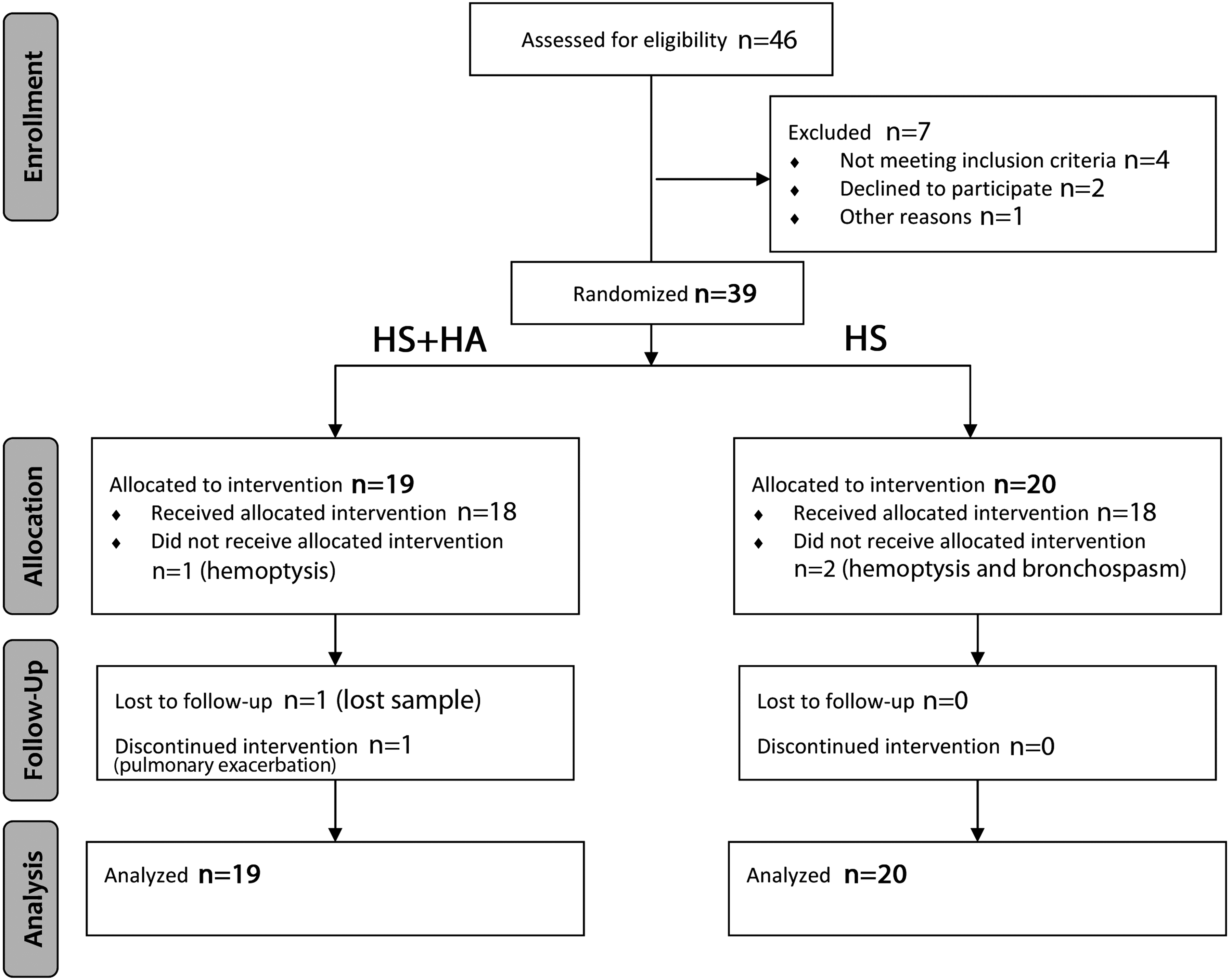
Flow chart for randomization procedure.
ERV, expiratory reserve volume; FEF25–75, forced expiratory flow between 25 and 75 percent of FVC; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; IQR, interquartile range; RV, residual volume; SR tot, total airway resistance; TLC, total lung capacity; SD, standard deviation.
One subject in each treatment arm did not receive allocated treatment due to scanty hemoptysis after first inhalation. One episode of bronchospasm occurred after first inhalation in the HS arm while one pulmonary exacerbation led to treatment discontinuation in the HS+HA arm (Fig. 1).
ITT analysis for 39 subjects showed no influence of HA+HS on inflammatory markers (Fig. 2) versus HS alone, and this was confirmed by analysis of confidence intervals (Table 2). A within-group analysis showed that, in the HS+HA group, the highest decrement from baseline was observed for IL-1β (−58.8%) followed by VEGF (−49.9%) and IL-8 (−12.9%). Within-group analysis of the HS revealed that only IL-10 median level increased significantly from baseline (+83%; p = 0.0111) (Table 3). In the HS group IL-1β levels did not show any variation and VEGF levels increased.
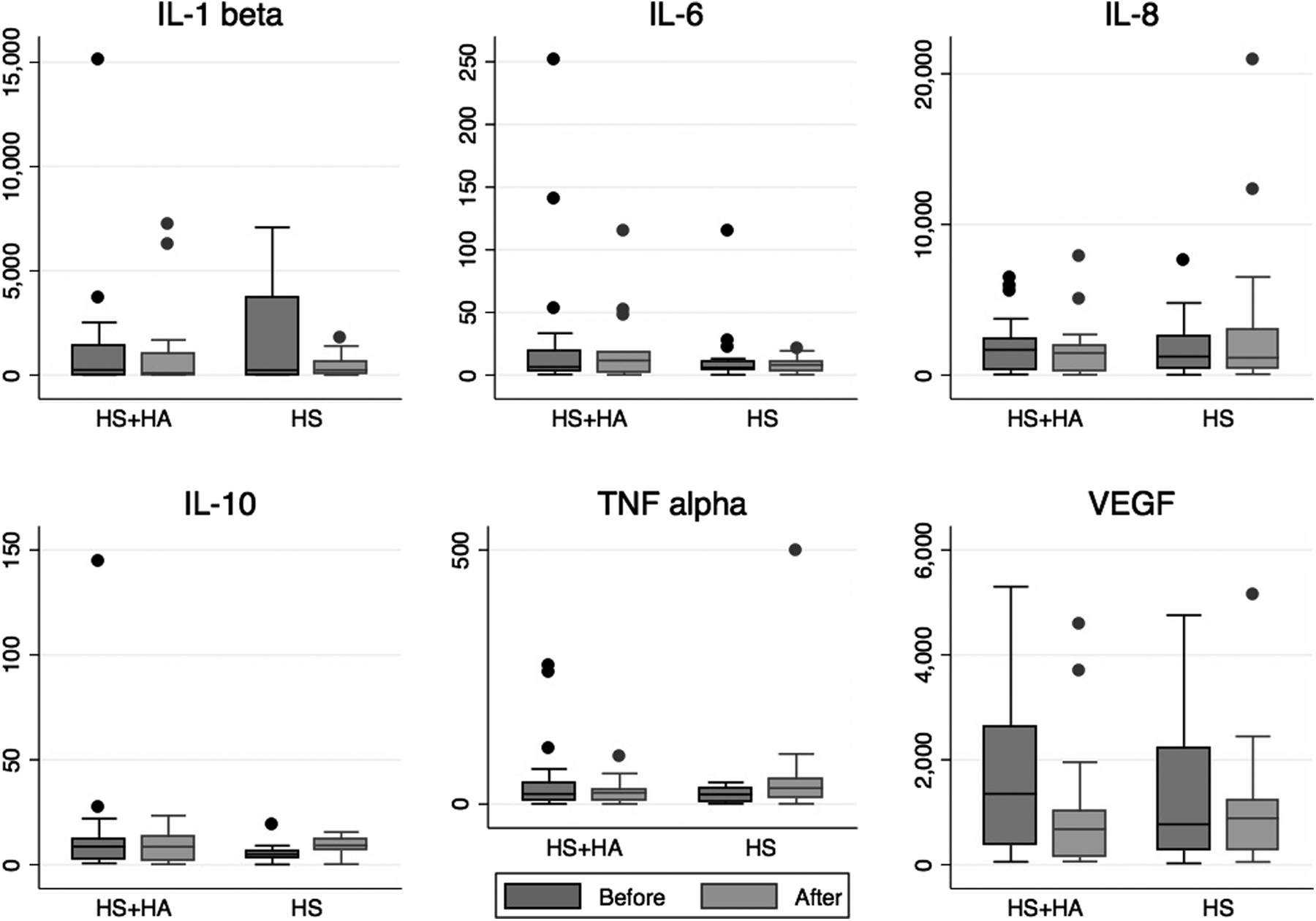
Box and Whiskers Plot of inflammatory markers (pg/mL) at baseline (before) and at the end of the study (after). The length of the box represents the interquartile range, horizontal line in the box represents the median, end of the whiskers are adjacent values. Outliers, defined as observations more than 1.5 (IQR) beyond the first or third quartile, are plotted individually (circles).
Values (pg/mL) are expressed as median (IQR); CI, Confidence interval.
Values (pg/mL) are expressed as median (IQR). *Wilcoxon matched-pairs signed-ranks test.
With regard to secondary outcomes, prevalence of unfavorable scores (VAS <6) was 36.8% in HA+HS versus 55% in HS group; no between-group differences were detected in the prevalence of moderate/severe symptoms of cough, saltiness, and throat irritation after 28 days (Table 4).
Comparison between groups at follow-up.
Pulmonary function showed the same behavior in both groups with the only exception of total airway resistance (SR tot%) (Table 5): no clear influence of HA+HS on pulmonary functions tests over confidence intervals was detected.
mean difference (95%CI); #median difference (95%CI).
ERV, Expiratory reserve volume; FEF25-75, forced expiratory flow between 25 and 75 percent of FVC; FEV1, forced expiratory volume in one second; FVC, forced vital capacity; IQR, interquartile range; RV, residual volume; SD, standard deviation; SR tot, total airway resistance; TLC, total lung capacity.
Subjects were considered fully adherent to test products inhalation if the number of empty vials returned after 28 days was zero. 50% of patients in the HS arm were fully adherent versus 57.9% in the HS+HA group (p = 0.397) with 2.5 ± 5.6 and 3.1 ± 5.5 vials not administered, respectively.
Discussion
Hypertonic saline has been established as a therapy aimed at restoring airway surface liquid, improving lung function, and reducing the rate of pulmonary exacerbations in patients with CF.(5–9,24,25) Besides its positive effect on mucus rheology,(26,27) HS has mucolytic, antimicrobial, and anti-inflammatory properties, and has been shown to inhibit growth, motility, and biofilm formation of Pseudomonas aeruginosa, partially explaining its favorable clinical effects.(28,29) Furthermore, HS was shown to stimulate mucin secretion via a direct effect on secretory cells or via the output of inflammatory mediators by glandular serous cells.(30) Nevertheless, two drawbacks of HS use remain to be resolved, namely its effectiveness in the long term and its unpleasantness. A formula containing HS +0.1% hyaluronic acid is also available and used in CF patients, basing use on its greater pleasantness.(16,17)
HA can prevent elastolysis in airways, decrease chemotaxis by reducing elastin fragmentation, and block elastase secretion by neutrophils and macrophages in humans.(12) Treatment of CF mice with high molecular weight HA for 3 days was sufficient to reduce lung inflammation, and this effect did not decrease during the 4 subsequent days of treatment, as well as after 24 hours following drug withdrawal.(15) Levels of TNF-α and MIP-2, analogous to human IL-8, mainly responsible for neutrophils recruitment into the mice lungs, were significantly reduced as well as leukocytes lung infiltration.
In this study, we sought to explore the effects of HS+HA on lung inflammation in CF patients. After 28 days of treatment, no clear influence of HS+HA on cytokine levels in sputum as compared to HS alone was observed. In addition, there was no significant change in cytokine levels within the two groups, with the only exception of IL-10, which increased in the HS group. Even removing the 25% of patients with moderate lung disease in the HS group (n = 5), the overall cytokine behavior was not modified (data not shown).
The airway inflammation in CF is directed by many cell types belonging to the innate immune system, including airway epithelial cells and macrophages. Some studies have pointed out that the CF lungs are characterized by an imbalance between pro-inflammatory and anti-inflammatory mediators, such as IL-10, which is produced by alveolar macrophages.(31) In this study, the most important finding was that sputum IL-10 levels were significantly increased only in the HS arm. Whether VEGF, a cytokine involved in monocyte activation and therefore in chronic inflammation,(32) is determining the increase in IL-10 sputum levels, should be the focus of further research in the HS field.
In a single-dose unblind randomized trial, HS+HA was preferred by CF patients with respect to HS alone, since HS+HA intervention reduced severity of cough, throat irritation, and salty taste, and also increased overall pleasantness.(16) In our study, we did not find a clear preference in favor of HS+HA treatment concerning tolerability, since reduction of unfavorable symptoms in HS+HA group vs. HS alone could not be documented. Our study is methodologically different from the study of Ros and colleagues, in which they reported that the addition of HA was beneficial in CF patients(17) who had already been exposed to HS and had shown poor tolerance. Furnari and colleagues also reported in a prospective, randomized, double-blind study a reduction in the incidence of throat irritation and in the use of bronchodilator after inhalation of HS+HA.(19) Although they did not enroll patients using HS in the 15 days preceding enrolment, these subjects cannot be considered blinded to HS taste.
Although an imbalance in the randomization flow occurred for age and spirometric values, we did not observe any influence of HS+HA over confidence intervals of pulmonary function tests, both static and dynamic, as already reported elsewhere.(17,19) However, the same conclusions can be drawn after removing the 25% of patients with moderate disease from HS group.
This is the first study to explore the influence of HS with or without HA on inflammatory markers. Concentration of inflammatory cytokines in different body fluids have been used for the early detection of pulmonary exacerbation and to predict the response to antibiotic therapy in CF.(33) Indeed, if we based our calculation on the 24.5% decrement of IL-8 associated to a significant improvement in lung function(34) and considered the IL-1β and VEGF sputum level detected in the group of CF patients enrolled in the present study (IL-1β mean 1613.573 with standard deviation 2983.893 pg/mL, VEGF mean 1544.113 with standard deviation 1538.335 pg/mL), we would need more than 300 subjects in each group to be able to detect that 24.5% meaningful reduction of IL-1β and VEGF under HS+HA treatment, with a power (1-β) of 90% and a significance level (α) of 5%.
In conclusion, according to our results HS+HA treatment is safe for CF patients, but we were unable to show any effects that influence lung inflammation and function as compared to HS alone.
Although previous studies showed that HA significantly improves the tolerability and efficacy of HS, we could not confirm this finding. It is worth noting that a one-month treatment with HS did not cause an increase in sputum inflammatory markers from baseline levels.
Footnotes
Acknowledgments
All products were supplied free of charge by Eupharma S.r.l.
Author Disclosure Statement
No financial conflicts of interest exist.