
Abstract
Abstract
Aim:
To compare the systemic exposure of salbutamol following delivery from the unit dose dry powder inhaler (UD-DPI) system with that from the Diskus® and metered dose inhaler (MDI).
Materials and Methods:
This open-label, two-part, six-way crossover, randomized single-dose study in healthy subjects evaluated salbutamol systemic exposure of three dose strengths (using three inhalations: 3 × 150 μg [450 μg], 3 × 200 μg [600 μg], and 3 × 250 μg [750 μg]) and 2% of drug in lactose blends (1.6% and 1.0% [600 μg dose only] by weight) following delivery through the UD-DPI compared with systemic exposure from the Diskus and MDI (600 μg dose). Systemic exposure in the presence of charcoal block was also evaluated. Primary treatment comparisons were area under the concentration–time curve from time zero to 12 hours [AUC0–12] and maximum plasma concentration [Cmax].
Results:
Delivery of salbutamol 600 μg from the UD-DPI resulted in total systemic exposure similar to that from the Diskus and approximately half of that from the MDI (AUC0–12 geometric least squares mean ratio [GMR] [90% confidence interval (CI)] for UD-DPI [1.6% blend]/Diskus: 0.91 [0.83–1.00]; UD-DPI [1.6% blend]/MDI: 0.46 [0.42–0.50]. Cmax GMR [90% CI] for UD-DPI [1.6% blend]/Diskus: 1.20 [1.07–1.33]; UD-DPI [1.6% blend]/MDI: 0.58 [0.52–0.64]). Results were consistent between the 1.6% and the 1.0% blends and systemic exposure for the 3 dose strengths of salbutamol (1.6% blend) showed increases that were 12–16% greater than dose proportional. Systemic exposure due to pulmonary absorption (as calculated from AUC0–12 in the presence and absence of charcoal block) was 48% for the UD-DPI, 24% for Diskus, and 37% for MDI of the total salbutamol systemic exposure, and the corresponding estimated lung dose was 65% for the UD-DPI and 34% for the Diskus relative to the MDI.
Conclusions:
Salbutamol total systemic exposure following UD-DPI was similar to that from the Diskus and was lower than that following the MDI. The different blend formulations tested resulted in consistent salbutamol systemic exposure. The contribution of the lung and gut to systemic exposure revealed a different profile for the three inhaler platforms. These data suggest that the UD-DPI warrants further evaluation.
Introduction
A
Although neither asthma nor COPD are curable, both diseases can be effectively treated to minimize symptoms and impact on quality of life and to prevent future risk of exacerbations.(2,3) However, despite this, asthma is often not well controlled(7,8) and COPD is frequently underdiagnosed and mismanaged.(9–12) In developing countries, particularly, there are issues of insufficient attention being paid to risk factors for asthma and COPD and inadequate standards of healthcare for chronic disease management.(4) Part of the problem is a lack of access to affordable medications,(1,13) where patients on low incomes may not manage the high upfront acquisition cost of a multidose inhaler.
Salbutamol is a recognized and licensed rescue inhalation therapy for the prevention and relief of bronchoconstriction in patients with asthma and COPD. The efficacy of salbutamol has been established through the inhaled route, which includes the metered dose inhaler (MDI), multidose powder inhaler (Diskhaler® and Diskus®), Rotacaps®/Rotahaler® system, and nebules. The unit dose dry powder inhaler (UD-DPI) is a novel passive dry powder inhaler system consisting of a reusable device and separate, single-use foil blisters containing the powder for inhalation. The provision of inhaled medicines such as salbutamol with the UD-DPI system provides patients with more treatment options and, in a small part, could potentially assist in reducing the cost barrier associated with accessing medications.
This study was a first-time-in-humans study of the UD-DPI system designed to provide preliminary information on the lung delivery and systemic pharmacokinetics (PK) of the UD-DPI system using different blister formulations relative to the Diskus and MDI in delivering salbutamol to healthy volunteers.
Materials and Methods
Subjects
Eligible subjects were aged 18 to 65 years with a body weight ≥50 kg, a body–mass index (BMI) of 19–34 kg/m2, and were judged to be healthy by an experienced physician based on medical evaluation. Key exclusion criteria included a current diagnosis or history of liver disease, a positive test for hepatitis B or C (within three months of study entry), a positive test to human immunodeficiency virus, or a positive prestudy breath carbon monoxide test or urine drug or breath alcohol screen. An electrocardiogram PR interval outside the range, 120 to 240 msec, at screening also precluded subjects. Subjects were asked not to use prescription or nonprescription drugs within 7 days of the first dose of study medication until study completion other than paracetamol (≤2 g/day permitted).
Written informed consent was obtained from all subjects before participation and the study was approved by Bellberry Ethics Committee, Eastwood, South Australia, Australia.
Study design
This was an open-label, two-part, six-way crossover single-dose study in healthy subjects designed to evaluate the systemic exposure of salbutamol delivered through the UD-DPI compared with systemic exposure following delivery from the Diskus or MDI (GSK Protocol 200921; NCT01984086). Subjects were not allowed to participate in more than one part of the study. A range of blister formulations were investigated with the UD-DPI, including three dose strengths (total dose: [three inhalations each] 3 × 150 μg [450 μg], 3 × 200 μg [600 μg], and 3 × 250 μg [750 μg]) and two different percentages of drug in lactose blends (1.6% [450, 600, and 750 μg doses] and 1.0% [600 μg dose]). Multiple inhalations were required to obtain measurable salbutamol plasma levels for the estimation of PK parameters; however, all doses were below the maximum approved daily dose for salbutamol through inhalation (1600 μg). Subjects underwent training on how to use the UD-DPI, Diskus, and MDI devices and were only included in the study if they could use the devices correctly.
Part A: Systemic exposure of salbutamol
Subjects received a single dose of the following 6 treatments in a randomized crossover design:
• Salbutamol three inhalations (200 μg per blister from 1.6% blend) through UD-DPI (total dose 600 μg) • Salbutamol three inhalations (200 μg per blister from 1.0% blend) through UD-DPI (total dose 600 μg) • Salbutamol three inhalations (150 μg per blister from 1.6% blend) through UD-DPI (total dose 450 μg) • Salbutamol three inhalations (250 μg per blister from 1.6% blend) through UD-DPI (total dose 750 μg) • Salbutamol three inhalations (200 μg per blister) through Diskus (total dose 600 μg) • Salbutamol six inhalations (100 μg per actuation) through MDI (total dose 600 μg)
The total duration for dosing was 3 minutes and was identical for all treatments tested; for MDI, this involved six inhalations 30 seconds apart, and for Diskus and UD-DPI, this involved three inhalations 60 seconds apart.
Subjects were screened for eligibility up to 28 days before the first treatment. There was a minimum 3-day washout period between each treatment and a follow-up visit 7 to 14 days after completion of the last treatment.
Part B: Systemic exposure of salbutamol with and without charcoal block
This part of the study was designed to explore the PK profile of the UD-DPI with the Diskus or MDI in the presence and absence of a charcoal block to determine the proportion of total systemic exposure arising from lung and gut absorption, respectively. The measurement of AUC0–0.5 with and without charcoal was measured to provide an indication of the systemic exposure due to lung absorption during the first 30 minutes—as plasma concentrations not influenced by charcoal block indicate that systemic exposure is due to lung absorption only.(15)
Treatments chosen for evaluation in Part B were based on PK results in Part A.
Subjects received a single dose of the following 6 treatments in a randomized crossover design:
• Salbutamol three inhalations (200 μg per blister from 1.6% blend) through UD-DPI without activated charcoal • Salbutamol three inhalations (200 μg per blister from 1.6% blend) through UD-DPI with activated charcoal • Salbutamol three inhalations (200 μg per blister) through Diskus without activated charcoal • Salbutamol three inhalations (200 μg per blister) through Diskus with activated charcoal • Salbutamol six inhalations (100 μg per actuation) through MDI without activated charcoal • Salbutamol six inhalations (100 μg per actuation) through MDI with activated charcoal
Dosing duration and intervals between inhalations were the same as for Part A.
Charcoal was administered as a suspension of 5 g activated charcoal (carbisorbX) in 25 mL water given 2 minutes before and 2 minutes after the completion of inhaled treatments, and then at 62, 122, and 242 minutes after the second administration of charcoal (predose and at 1, 2, and 4 hours postsalbutamol dose). At the predose and 2 minutes postdose administration, subjects were asked to swish fluid around in their mouth before swallowing to prevent buccal absorption of salbutamol.
Subjects were screened up to 28 days before the first treatment and there was a minimum 7-day washout period between each treatment and a follow-up visit 7 to 14 days after the last treatment.
Pharmacokinetic assessments
For each treatment evaluation, subjects were admitted to the investigation unit the day before treatment administration. The following morning, treatment was administered to fasting subjects, and serial 3 mL blood samples were collected at the following time points relative to the beginning of treatment inhalation: premorning dose and at 5, 10, 20, 30, and 45 minutes and 1, 1.5, 2, 4, 6, 8, 10, and 12 hours postdose. Subjects were given a meal at 4 and 10 hours postdose. Blood samples were collected into ethylenediaminetetraacetic acid tubes and centrifuged at 1500 g for 10 minutes at 4°C and the resulting plasma was stored at -20°C before shipping to York Bioanalytical Solutions Ltd., (York, United Kingdom) for analysis.
Plasma samples were analyzed using a validated analytical method based on solid-phase extraction, followed by liquid chromatography and tandem mass spectrometric detection analysis. The lower limit of quantification for salbutamol was 50 pg/mL.
The following PK parameters were derived from the plasma salbutamol concentration–time data using Phoenix WinNonlin 6.3 (Certara, Inc., CA): area under the concentration–time curve from time zero to 0.5 hour (AUC0–0.5) and 12 hours (AUC0–12), maximum plasma concentration (Cmax), and time at which Cmax was observed (tmax).
Safety
On each treatment day, vital signs (heart rate and blood pressure) were measured at predose and at 20 minutes, 1, 2, and 12 hours postdose. Twelve-lead electrocardiograph (ECG) measurements were made premorning dose and 1 hour postdose on each treatment day. Adverse events were monitored throughout each treatment period and during any follow-up.
Aerodynamic particle size distribution
Aerodynamic particle size distribution of the delivered doses from the UD-DPI and Diskus inhalers was characterized using the Andersen Cascade Impactor (ACI) at a flow rate of 60 L/min, an in vitro quality control test that can provide an estimate of the total lung dose. As the MDIs used in this study were from commercially supplied stock, a complete ACI aerodynamic particle size distribution analysis was not available.
Fine particle mass (FPM) data were generated from the ACI by summing the mass of salbutamol deposited on impactor stages 1 to 5, leading to an aerodynamic particle size range from 0.8 to 6.2 μm based on the effective cutoff diameter of each impactor stage at a flow rate of 60 L/min.
Statistical analysis
Using data from previous GSK salbutamol studies, it was estimated that with a sample size of 24, the precision for comparisons of interest would be within 16.1% (for AUC) and 17.8% (for Cmax) of the observed point estimate, where precision was expressed as the half-width of the 90% confidence interval (CI). Thirty healthy volunteers were planned for each part of the study to ensure 24 evaluable subjects.
Following loge transformation, AUC and Cmax of salbutamol were separately analyzed using a mixed effects model with fixed effect terms for period and treatment. Subject was treated as a random effect in the model. Point estimates and their associated 90% CIs were constructed for all treatment comparisons. The point estimates and their associated 90% CIs were back transformed to provide point estimates and 90% CIs for the geometric mean ratios, UD-DPI/DISKUS and UD-DPI/MDI, and for the blend comparison UD-DPI 1.6%/UD-DPI 1% (for the 3 × 200 μg doses). Tmax was analyzed separately using Wilcoxon's matched-pair method.
Results
Part A: Systemic exposure of salbutamol
Subjects
Thirty subjects were randomized to treatment and 29 completed Part A as planned. One subject was withdrawn at the investigator's discretion after the subject developed a rash ∼36 hours after dosing in treatment period 5 (salbutamol 600 μg through MDI). The rash was not considered related to study treatment.
Mean age of subjects was 26.8 years, 73% were males, and 90% were Caucasians, with a mean BMI of 24.7 kg/cm3 (Table 1). All subjects used the inhaler devices correctly with no reported errors in technique.
PK data
Following single-dose administration, salbutamol was more rapidly absorbed following inhalation from UD-DPI (median tmax 0.17 to 0.33 hour) compared with Diskus (1.5 hours) and MDI (0.63 hour) (Table 2). Delivery of salbutamol (total dose 600 μg) from the UD-DPI resulted in total systemic exposure within 10% of that from the Diskus and 54% lower than that following the MDI in terms of AUC0–12 (Fig. 1; Tables 2 and 3). Cmax was 16% lower following inhalation from the Diskus, and 42% higher following the MDI, compared with the UD-DPI. Systemic exposure during the first 30 minutes (AUC0–0.5), indicative of pulmonary absorption, from the UD-DPI was 43% higher than that from the Diskus and 34% lower than that from the MDI (Fig. 2; Table 2).
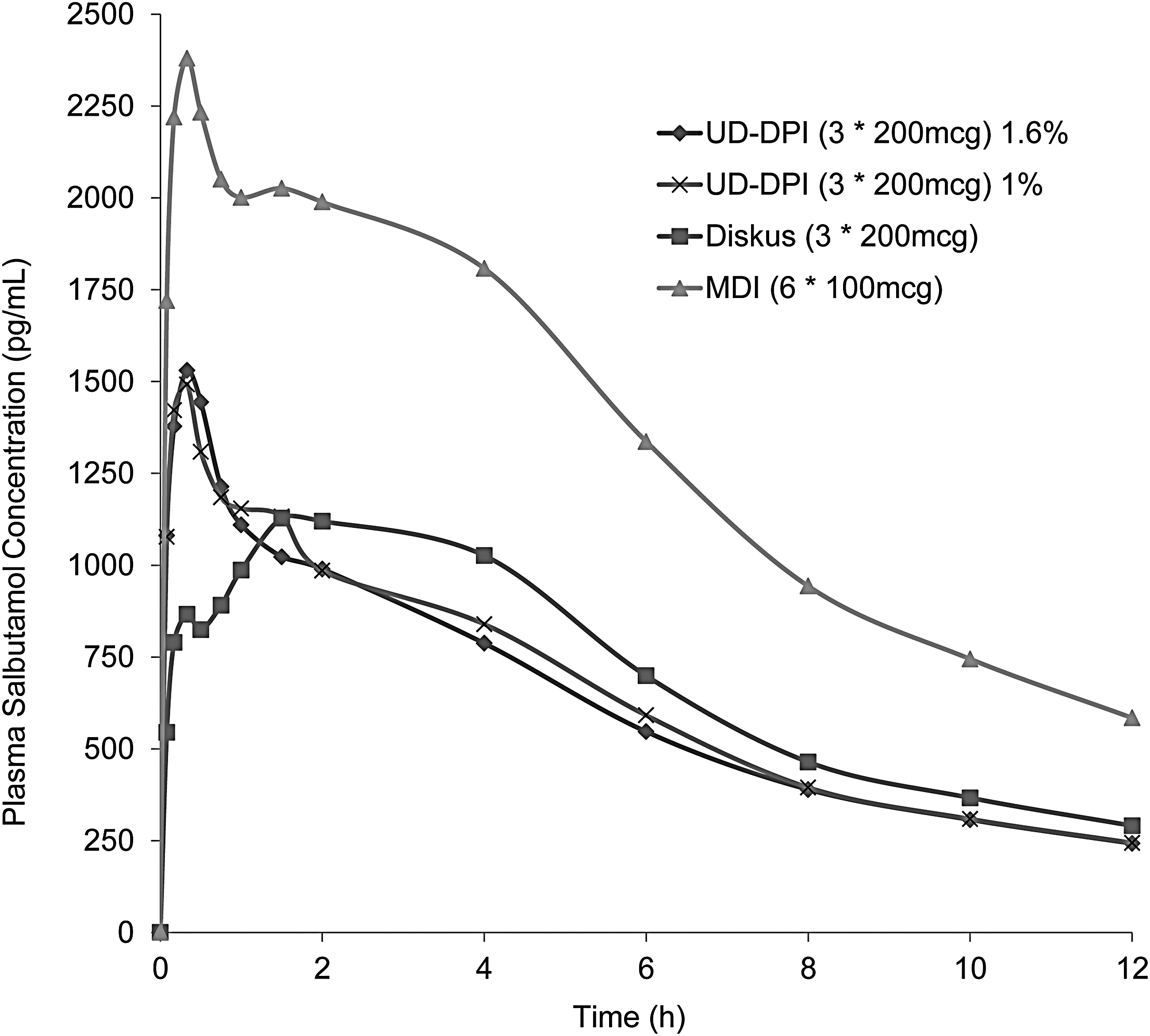
Plot of salbutamol median concentration–time profile (Part A). MDI, metered dose inhaler; UD-DPI, unit dose dry powder inhaler.
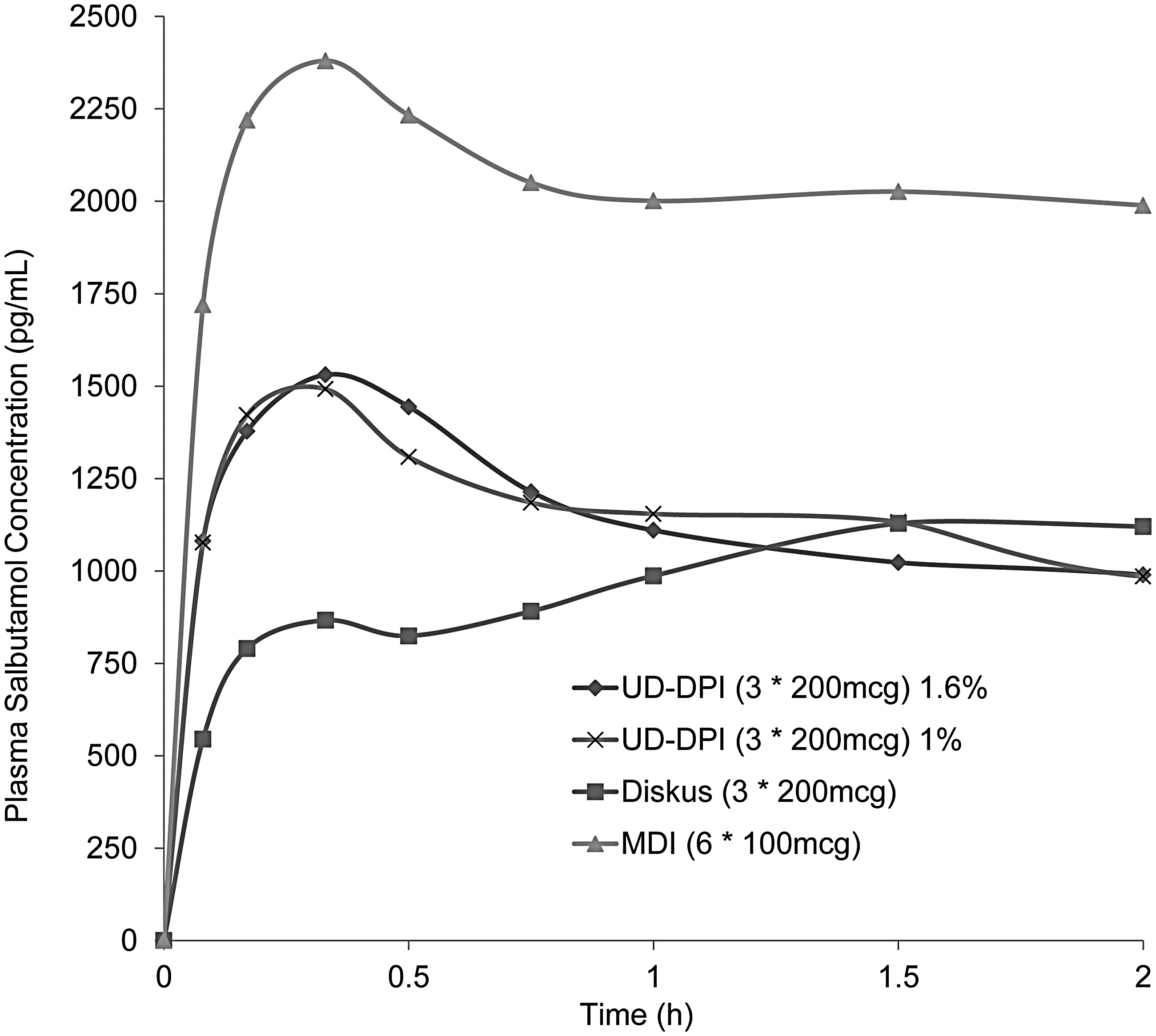
Plot of salbutamol median concentration–time profile over 0–2 hours (Part A).
Data presented as geometric mean (95% CI), except tmax presented as median (range).
Same superscripted alphabet in Part A and Part B indicates consistent systemic exposure between two parts and reproducible results with the Diskus, MDI, and UD-DPI.
CI, confidence interval; MDI, metered dose inhaler; UD-DPI, unit dose dry powder inhaler.
Data presented as geometric least squares mean ratio (90% CI).
The concentration–time profiles for the salbutamol UD-DPI 600 μg 1% and 1.6% blends were consistent (Figs. 1 and 2). Delivery of increasing doses of salbutamol from the UD-DPI showed that salbutamol systemic exposure was 12%–16% greater than dose proportional (Table 4).
Part B: Systemic exposure of salbutamol with and without charcoal block
Based on the similarities in salbutamol systemic exposure with the salbutamol UD-DPI 600 μg 1% and 1.6% blends, the 1.6% blend was used in Part B of the study. This is the same blend as used in the Diskus.
Subjects
Thirty subjects were randomized to treatment and 28 completed Part B as planned. Of the two subjects withdrawn, one was due to investigator's discretion following an adverse event of seasonal allergy. The other subject withdrew consent due to an inability to tolerate the charcoal administration; this subject completed all the remaining treatments that did not involve the use of charcoal block.
Mean age of subjects was 29.5 years, 73% were males, and 80% were Caucasians, with a mean BMI of 24.9 kg/cm3 (Table 1). All subjects used the inhaler devices correctly with no reported errors in technique.
PK data
PK data following all treatments without charcoal were similar to those reported in Part A of the study (Table 2). In the presence of charcoal, salbutamol delivered through UD-DPI, Diskus, and MDI showed median tmax of 0.33 hour (Table 2). AUC0–0.5 hour was similar following treatment administration with and without charcoal for all three inhaler platforms.
Systemic exposure in terms of AUC0–12 (without charcoal) confirmed that UD-DPI resulted in a total systemic exposure similar to that from the Diskus (difference of 4%) and approximately half of that following MDI (difference of 49%) (Table 2). In the presence of charcoal block, AUC0–12 indicated that for the UD-DPI, 48% of the total systemic exposure was due to pulmonary absorption compared with 24% and 37% for Diskus and MDI, respectively (Table 2, Fig. 3). Based on systemic exposure due to pulmonary absorption (calculated from AUC0–12 in the presence of charcoal block), relative to the MDI, the UD-DPI delivered 65% of the lung dose and the Diskus delivered 34% of the lung dose.

Plot of salbutamol median concentration–time profile:
Systemic exposure in terms of Cmax was similar after delivery of salbutamol from UD-DPI with and without charcoal (9% difference), indicating that maximum salbutamol concentration was primarily due to pulmonary absorption (Table 2, Fig. 4). This differed from the results shown with Diskus and MDI delivery with and without charcoal, which showed that 47% and 78%, respectively, of maximum salbutamol concentration were attributed to pulmonary absorption.

Variability plot showing salbutamol fine particle mass (as μg/blister) for UD-DPI and Diskus clinical batches. The Diskus product used is a composite of two batches of which the overall data summary is presented.
Safety
The most commonly reported adverse event was headache, followed by tremor (Table 5). No serious adverse events were reported, and there were no reports of clinically significant vital signs or ECG results following any treatment.
Aerodynamic particle size distribution
FPM data for salbutamol UD-DPI 600 μg 1.6% blend and Diskus 600 μg were comparable, and there was evidence of dose proportionality across the three salbutamol UD-DPI doses for the 1.6% formulation (Fig. 4), consistent with the data shown for total systemic exposure. FPM data differed between the salbutamol UD-DPI 600 μg 1% and 1.6% blends, unlike the results for systemic exposure, which showed almost identical concentration–time profiles for the two blends (Fig. 1).
Discussion
This study was the first evaluation in humans of the UD-DPI, a novel dry powder inhaler system. Total systemic exposure of salbutamol (in the absence of charcoal) following inhalation from the UD-DPI, in terms of AUC0–12, was similar to that from the Diskus and no greater than that from the MDI, but differences in the shape of the AUC suggested differences in the lung versus gastrointestinal absorption for the three inhaler platforms and this was confirmed by the results for AUC in the presence of charcoal block.
Combined results from Part A and Part B (or in the presence and absence of charcoal block) showed that for all treatments, systemic exposure during the first 30 minutes (AUC0–0.5) was mostly due to pulmonary absorption. Overall, these data suggest that delivery of salbutamol through UD-DPI would result in a delivered lung dose and systemic exposure midway between that achieved by the Diskus and MDI. This suggests that the efficacy and safety profile of salbutamol through UD-DPI would be acceptable; however, this assumption would need to be confirmed in phase 3 clinical efficacy and safety studies.
As this was the first trial of the UD-DPI in humans, a range of blister formulations were tested with the UD-DPI, including two different percentages of drug in lactose blends and three dose strengths. Systemic exposures were consistent following both blend formulations, allowing the 1.6% blend, the same as that used in the Diskus, to be progressed to the second part of the study. The results of the dose proportionality assessment showed that plasma salbutamol exposure following UD-DPI was 12–16% greater than dose proportional over the dose range tested of 150 μg to 250 μg. However, no formal dose proportionality testing was done. The comparable PK results shown in Part A and Part B (with and without charcoal) of the study with salbutamol UD-DPI suggest reliable reproducible dosing from the new device.
Systemic exposure in terms of AUC0–12 in the presence of charcoal block, (where oral component of absorption was blocked) measuring exposure due to lung absorption only, showed a differential profile for oral versus pulmonary absorption for UD-DPI, Diskus, and MDI. Assessments of salbutamol systemic exposure following inhalation from UD-DPI in the presence and absence of charcoal suggested that approximately half of the total systemic exposure attributed to pulmonary absorption compared with a quarter and a third for the Diskus and MDI, respectively, indicating that more drug is swallowed following inhalation through Diskus and MDI than with UD-DPI.
In terms of Cmax, results were similar following salbutamol UD-DPI with or without charcoal, suggesting that the rapid peak observed was almost entirely due to pulmonary absorption. In contrast, the differing Cmax results in the presence and absence of charcoal following administration of salbutamol from the Diskus and the MDI indicated that oral absorption also contributes to Cmax. For all treatments, AUC0–0.5 hour was similar when administered with and without charcoal, indicative of pulmonary absorption only, and suggesting that systemic exposure due to oral absorption occurs after the first half hour. This is consistent with reports that following inhaled short-acting ß2-agonists, gastrointestinal absorption is negligible with respect to the overall systemic absorption from the inhaled dose in the first 30 minutes after inhalation.(14)
Of note, the comparative PK data for salbutamol UD-DPI and Diskus did not correlate well with the FPM data (which were comparable for the two treatments) and indicate that a different inhaler design is highly influential and may result in significant variation in lung deposition as evidenced by the higher Cmax and sharper peak on the UD-DPI concentration–time curve compared with Diskus. This would support the observation that in vitro studies on their own have limited ability to predict comparability between two different devices.(15) Conversely, the approximate dose proportionality shown for salbutamol UD-DPI, consistently shown with the PK and FPM data, suggests that for the same inhaler device, in vitro studies are more predictive of eventual PK profiles. However, this does not account for the differences in in vitro data with the two UD-DPI blend formulations, which resulted in almost identical PK profiles.
It was not possible to perform in vitro analysis on the commercially sourced MDIs used in this study; however, the in vitro comparison of FPM between DPI and MDI is less important and less appropriate since additional factors, such as impaction flow rates(16) or need to actuate the MDI device, have a significant influence on drug delivery. Therefore, for the purpose of in vitro comparisons, comparing the performance between two types of DPIs where inspiratory/impaction flow rates can be standardized is more appropriate.
The similarities in total systemic exposure for the UD-DPI and Diskus devices accompanied by evidence of different lung and gastrointestinal absorption profiles may also question the value of PK data in predicting clinical efficacy data outcomes for the two inhalers and highlight the importance of providing clinical data to support PK data when developing a drug to show clinical or therapeutic equivalence.
Regulatory agencies have recommended using charcoal blockade to exclude absorption of the active moiety from the gastrointestinal tract to assess the pulmonary deposition of inhaled drugs with known gastrointestinal absorption in an effort to establish bioequivalence between two different inhaler platforms. This is in addition to comparing total systemic exposure of the same drug in two inhaler platforms to assess comparability in terms of systemic safety. The results of this study emphasize the need to evaluate both the total systemic exposure and systemic exposure associated with pulmonary deposition as part of a complete clinical evaluation of alternative versions of established inhaled drug products.
Although the contribution of the lung and gut to systemic exposure differed between the three inhaler types, the increased lung contribution observed with salbutamol UD-DPI was offset by a decrease in the amount swallowed and absorbed from the gut, resulting in the similar total systemic exposure to that following the Diskus and no greater than that following the MDI. This provides reassurance that the systemic safety of salbutamol when given with the UD-DPI does not exceed that observed when using the MDI and Diskus. This is supported by the other safety endpoints measured in the study—there were no observed differences in adverse events between treatments and no reports of clinically significant changes in vital signs or ECG results.
In conclusion, this first-time administration of the salbutamol UD-DPI in humans demonstrated comparable total systemic exposure to the Diskus and no greater systemic exposure than that shown with the MDI. The different blend formulations resulted in similar salbutamol systemic exposure and systemic exposure was 12%–16% greater than dose proportional over the dose range studied. The contribution of the lung and gut to systemic exposure revealed a different profile for the three inhaler platforms. These data suggest that the UD-DPI may have the potential to become an alternative inhaler platform for delivering inhaled drugs, but further evaluation in clinical efficacy and safety studies would be required.
Footnotes
Acknowledgments
This study was funded by GSK (Protocol 200921; NCT01984086). The authors would like to thank Dr Benjamin Van Hecke for his role as principal investigator. The authors also thank Jon Hall for providing the in vitro data and Peter Daley-Yates for his advice in interpreting the data (both R&D, GSK, United Kingdom). Editorial support in the form of draft manuscript development, editorial suggestions to draft versions of this article, assembling tables, copyediting, and referencing was provided by Kate Hollingworth of Continuous Improvement Ltd., and was funded by GSK.
Author Disclosure Statement
All authors are GSK employees and shareholders.