
Abstract
Abstract
Background:
Mechanically ventilated patients commonly suffer from ventilator-associated pneumonia, hypoxemia, and other lower respiratory tract infection as a result of pathogen colonization and poor sputum clearance. Consequently, there is a high rate of morbidity and mortality in these patients. Dry powder mannitol increases sputum clearance, and therefore, we developed a system to administer it to mechanically ventilated patients without disconnection from the ventilator.
Methods:
The inspiratory line from a ventilator was split by using a three-way valve into two parallel lines where one contains a humidifier for normal breathing cycle and the other line contains a dry powder inhaler (Osmohaler™). The inspiratory air went through the dry powder line and aerosolized the mannitol powder only when its administration to a patient is required. We determined the delivered dose and particle size distributions of emitted aerosols in vitro from 9.5 mm endotracheal and 7.5 mm tracheostomy tubes, with inspiratory airflow of 60, 70, and 80 L/min.
Results:
This novel setup was able to deliver 24.6% ± 3.33% of the 160 mg loaded dose mannitol powder (4 × 40 mg capsules) and 26.7% ± 2.19% of the 320 mg dose (4 × 80 mg capsules) when the endotracheal tube was used. With the shorter tracheostomy tube, the delivery dose increased to 35.6% ± 3.01% and 39.5% ± 2.04% of the 160 and 320 mg doses, respectively. The volume median diameters of the aerosols were in the respirable range with the largest value being 5.17 ± 0.87 μm.
Conclusions:
This delivery system has been shown to consistently deliver a high respirable dose of mannitol powder. Since this setup does not require disconnection of patients from the ventilator, it is safer for hypoxemic patients and easier to be adapted in a real clinical use.
Introduction
C
Suction, commonly used to clear airway secretions in mechanically ventilated patients, can be traumatic as it is painful and potentially causes tracheal injury.(5) Other techniques such as manual hyperinflation,(7) vibration and percussion,(8) gravity-assisted drainage or postural drainage(7,9) have not been shown effective.(10–14) Administration of mucolytic agents such as acetylcysteine to decrease sputum viscosity has been reported but it increased inspiratory airway resistance.(15,16) Recombinant human DNase has been reported to improve mucus clearance,(17) however, it has not been widely used due to its high cost.(5)
Mannitol, a naturally occurring sugar alcohol, is an osmotic agent that has been shown to improve sputum clearance when delivered as a dry powder aerosol to patients with bronchiectasis and cystic fibrosis (CF).(18,19) Mannitol stimulates cough and improves innate mucociliary clearance by optimizing ciliary efficiency and altering sputum rheology.(18,20) Mannitol powder has been approved by the U.S. Food and Drug Administration agency for use as a diagnostic test for asthma(21,22) and by the European Union as a new CF treatment for patients 18 years and older.(23) It is commercially available as Aridol™ and Bronchitol™ (Pharmaxis Ltd, Sydney, Australia), respectively. However, its use in mechanically ventilated patients is novel and has not been approved yet. Since mannitol stimulates cough and can cause bronchoconstriction, not all patients would be suitable for mannitol administration. Patients with asthma, chronic obstructive pulmonary disease (COPD), or other obstructive airway disease and where coughing maybe a contraindication should be excluded.
We have shown previously that we could successfully deliver 50%–60% of the loaded mannitol powder, containing 20%–31% fine particles below 5 μm, to the distal end of the tracheal (endotracheal and tracheostomy) tubes.(24) Our delivery system consisted of a standard adult manual ventilation bag to provide the dispersive air to aerosolize the mannitol powder, a one-way duck-billed valve, and a dry powder inhaler (Osmohaler™) contained within a delivery chamber, which in turn was connected in series to an endotracheal or tracheostomy tube. However, this setup required the patients to be disconnected from the mechanical ventilator, which can compromise the safety of patients who suffer from severe hypoxemic respiratory failure.(25) Therefore, we have modified our previous setup so that the disconnection is not necessary. The improved in-line system incorporated a new line parallel to the normal inspiratory line. The air from the ventilator will flow through this line only when administration of the powder to the patient is required.
To the best of our knowledge, there is no published method on delivering dry powder aerosol to mechanically ventilated patients. When a pressurized Metered Dose Inhaler (pMDI) is used, synchronization with the onset of inspiration from the ventilator is crucial for optimum aerosol delivery.(26) This issue is eliminated with our proposed system because no coordination to synchronize between powder aerosolization and inspiration from the ventilator is required. Orderly actions that include closing the valve to the humidifier line and opening the valve to the dry powder line are necessary. Nebulizers, on the contrary, are not synchronized to the inspiratory phase(6) and hence leads to high drug loss. With our proposed setup, the dry powder is only delivered during the inspiration cycle. If this setup was to be commercially available, an automatic three-way valve can be installed at the point where the inspiratory line was split into the dry powder inhaler (DPI) and humidifier lines. The manual action of opening and closing the valves by an operator will not be required then.
Materials and Methods
Dosage rationale
A single dose of 120–480 mg of mannitol has been shown in multiple studies to increase mucociliary clearance in patients with bronchiectasis.(18,27) Nonetheless, the effect of inhaled dry powder mannitol in intubated patients is not completely known. As in our previous study where we used ventilation bag to deliver mannitol to intubated patients,(24) four capsules containing 40 or 80 mg dry powder mannitol will be delivered.
Materials
The spray-dried mannitol, supplied by Pharmaxis Ltd (Sydney, NSW, Australia), has a volume median diameter of 3.20 ± 0.03 μm and span [(D90−D10)/D50] of 1.41 ± 0.01. Mannitol powder was loaded into hydroxypropyl methylcellulose capsule size 3. A dry powder inhaler (Osmohaler; Pharmaxis Ltd, Sydney, Australia) was used to disperse the powder. Osmohaler operates on a piercing mechanism, which pierces two holes, one at each end of the capsule, of diameter 1.0 mm, through which the powder will exit as the capsule spins resulting from the air entrained into the inhaler during inspiration. Using this device, the 40 mg capsule was emptied within 5 ± 2 puffs, while the 80 mg required 8 ± 1 puffs. The endotracheal (350 mm in length) and tracheostomy (115 mm in length) tubes (Portex; Smiths Medical International Ltd, Kent, United Kingdom) with an internal diameter of 9.5 and 7.5 mm, respectively, were chosen because they are among the sizes most commonly used in intensive care units.
Experimental setup
Medical-grade oxygen and air were supplied to the ventilator (800 Series Ventilator; Puritan-Bennett Corporation, Carlsbad, CA). Figure 1 shows that the inspiratory line was split to the dry powder inhaler and the humidifier lines (Fisher & Paykel Healthcare, Melbourne, Australia). The humidifier was initially filled with warm water and then submerged in a warm water bath to ensure that the humidity of the air was 100%. The first ball valve was closed during the normal inhalation cycle where air would go through the humidifier and to the tracheal tube. When inspiratory air was needed to dispense the dry powder, the first ball valve was opened and the second ball valve was closed. A one-way duck-billed valve was positioned after the DPI chamber to prevent the humidified expiration air from entering the chamber and wetting the inhaler.

Experimental setup to determine the deposition profile of mannitol aerosol emitted from the tracheal tubes (endotracheal and tracheostomy tubes). Endotracheal tube was used in this illustration.
To capture the aerosolized powder exiting the tracheal tube, it was inserted into a 750 mL Volumatic™ inhalation device (GlaxoSmithKline Australia, Abbotsford, Australia). A collection filter (Sureguard®; Bird Healthcare, Port Melbourne, Australia) was fitted to collect all the aerosols emitted. The cuff of the tracheal tube was expanded to create an airtight seal between the tube and the holding chamber. The end of the circuit was fitted with an inflatable bag (GE-Healthcare, Sydney, Australia), to provide a close circuit for the ventilator.
Powder dispersion
Before each dispersion run, the tracheal tube was humidified to mimic condensation in the tube in vivo by letting the air to go through the humidifier line and bypassing the disperser line. The humidified air wetted both T-junctions, Volumatic inhalation device, and collection filter. Wetting the latter two parts was needed to avoid the aerosol rebounce so as to ensure that most of the emitted aerosols would be captured. In addition, the wetting mimicked the real situation as the patient's lung is wet. To overcome a low aerosol delivery due to the depositions in wet T-junctions, a polyurethane adapter (197 mm in length and 8 mm in internal diameter) was used (Fig. 2). This adapter extended from the DPI all the way to the tracheal tube to bypass the wet T-junctions. Preliminary work showed that when this adapter was not used, the delivered dose was very low (<10% of the loaded dose). Therefore, this adapter was necessary to increase the delivered dose. The insertion of this adapter was performed when the air from the ventilator was flowing through the other parallel limb. Consequently, it did not interrupt the ventilator and therefore would not affect the patient in the real clinical setting.
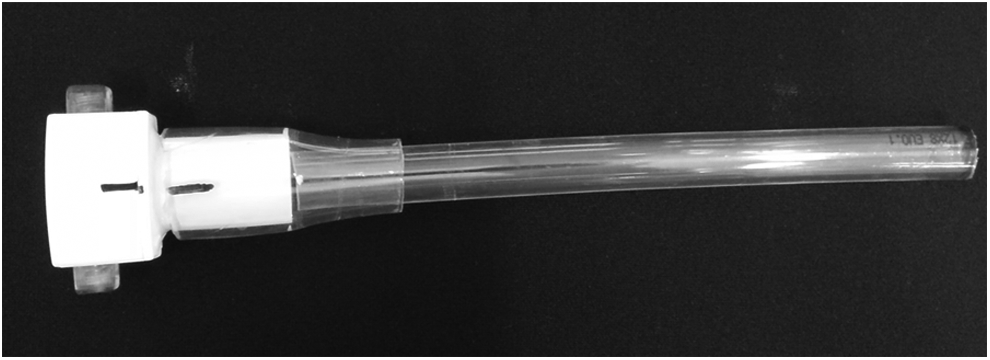
Polyurethane adapter connected to the DPI to bypass the wet T-junctions. DPI, .
Dispersion of mannitol was confirmed visually and aurally and the capsules were allowed to spin for the required number of puffs before the DPI was removed at the end of expiration phase (but before the inspiration phase). The first ball valve was then closed and the second ball valve was opened to allow replacement of new capsules without stopping the ventilator.
After having four capsules dispersed, the ventilator was turned off and all parts of the circuit, including capsules, DPI, perspex chamber, one-way valve, polyurethane adapter, both T-junctions, tracheal tube, Volumatic inhalation device, and all the filters, were washed using distilled water. Dispersions were performed in triplicate to ensure consistency of results.
Chemical assay
The amount of mannitol deposited in each part of the circuit was assayed by high-pressure liquid chromatography (LC-20AT; Shimadzu, Kyoto, Japan), using refractive index detection (RID-10A; Shimadzu, Kyoto, Japan). One hundred microliter samples were taken from each sample and injected into a C18 column (Kinetix 5 μm XB-C19 100Å 150 × 4.6 mm; Phenomenex, Torrance, CA) with a mobile phase consisting of filtered distilled water flowing at 1 mL/min for 3 minutes.(24)
Standards consisting of a known amount of mannitol were made and assayed in the same batch of samples in increasing concentrations to generate a standard calibration curve and the resultant equation was used to ascertain the amount of mannitol deposition.
Analysis of variance, followed by pairwise t-test, was carried out with a probability of <0.05 considered as statistically significant (Microsoft Excel 2003).
Ventilator settings
Table 1 lists the settings in the ventilator used in our study. The mixture of air delivered from the inspiratory line consisted of 21% oxygen and 79% air. The common flow rate used for patients connected to a ventilator ranges from 40 to 60 L/min.(28) A flow meter, located before the DPI, showed that the actual flow entering the dry powder inhaler was 20 L/min lower than the set ventilator flow rate. Therefore, the set flow rate in the ventilator was chosen to be 60–80 L/min to match the common flow rate used in the clinical situation. Square flow waveform, instead of descending ramp waveform, was selected to maximize the energy available to empty the mannitol powder from a capsule and to maximize powder aerosolization. Preliminary work showed that when a ramp flow with a peak flow rate of 80 L/min was used, the delivered dose was 32 ± 5.5 mg compared to 45 ± 5.2 mg using square flow.
The tidal volume should be set higher than the volume of the circuit between the dry powder inhaler and the patient to achieve optimum aerosol deposition in the lower respiratory tract as has been reported with MDI and nebulizer in-line with ventilator.(29–32) Ari and Fink added 50 mL to the circuit volume to ensure all the aerosols were able to reach the lung.(29) In our in vitro setup, the total volume between the dry powder inhaler and the inflatable bag (representing the patient's lung) was ∼834 mL (polyurethane adapter 9.9 mL; endotracheal tube 24 mL; Volumatic inhalation device 750 mL; collection filter 50 mL). We added 100 mL to the total volume to guarantee maximum aerosol delivery, which brings the total tidal volume to 950 mL and this is equivalent to 12 mL/kg for an 80 kg adult. Large tidal volumes in the range of 8–12 mL/kg have been used in mechanically ventilated COPD patients when MDI was used.(33) However, it was also reported that tidal volume greater than 8–10 mL/kg potentially causes volutrauma.(31) With this in mind, the high tidal volume of 950 mL used in our study should only be used during the introduction of dry powder inhaler and not during normal inhalation cycle.
Particle size distribution measurement
Particle size distribution of the powder coming out of the tracheal tube was measured on a laser diffractometer (Spraytec®; Malvern Instrument, Worcs, United Kingdom). The inlet and outlet ports of the inhalation cell of Spraytec were connected to the intubation tube and the Volumatic inhalation device, respectively. The inhalation device was consecutively connected to the collection filter and the inflatable bag. This setup provided a close circuit for the ventilator enabling a continuous operation. The Spraytec measured real-time, in situ particle size distribution of the aerosol passing through a laser beam. Acquisition frequency was 2.5 kHz. The material and absorption refractive indices (RIs) were 1.550 and 0.100, respectively. These values of RI were confirmed to be accurate indicated by the low residual values (<0.9%) for all measurements. The experiments were performed in triplicate. Particle size distributions were expressed as D10 (volume diameter under which 10% of the sample resides), D50 (volume median diameter), and D90 (volume diameter under which 90% of the sample resides). In addition to D10, D50, and D90, the percentages of particles with size smaller than 3 and 5 μm (the sizes conventionally considered for lung deposition via oral inhalation) obtained from the Spraytec software were included in this work.
Results
Displayed in Figure 3 is a comparison of deposition in each part of the setup with a 160 mg loading dose at three different flow rates (60, 70, and 80 L/min). Generally, there was only a small amount of mannitol deposited (<5% of the loaded dose) in both T-Junctions, the expiratory and humidified filters, and the one-way valve. Capsules were emptied after 5 ± 2 puffs, shown by the low amount of residual powder in the capsule (<5% of loaded dose). The depositions in the filter and the holding chamber, which gave the total dose delivered, were similar in all flow rates tested. The depositions in all parts were statistically insignificant except the deposition in endotracheal tube and the device between 60 and 80 L/min.
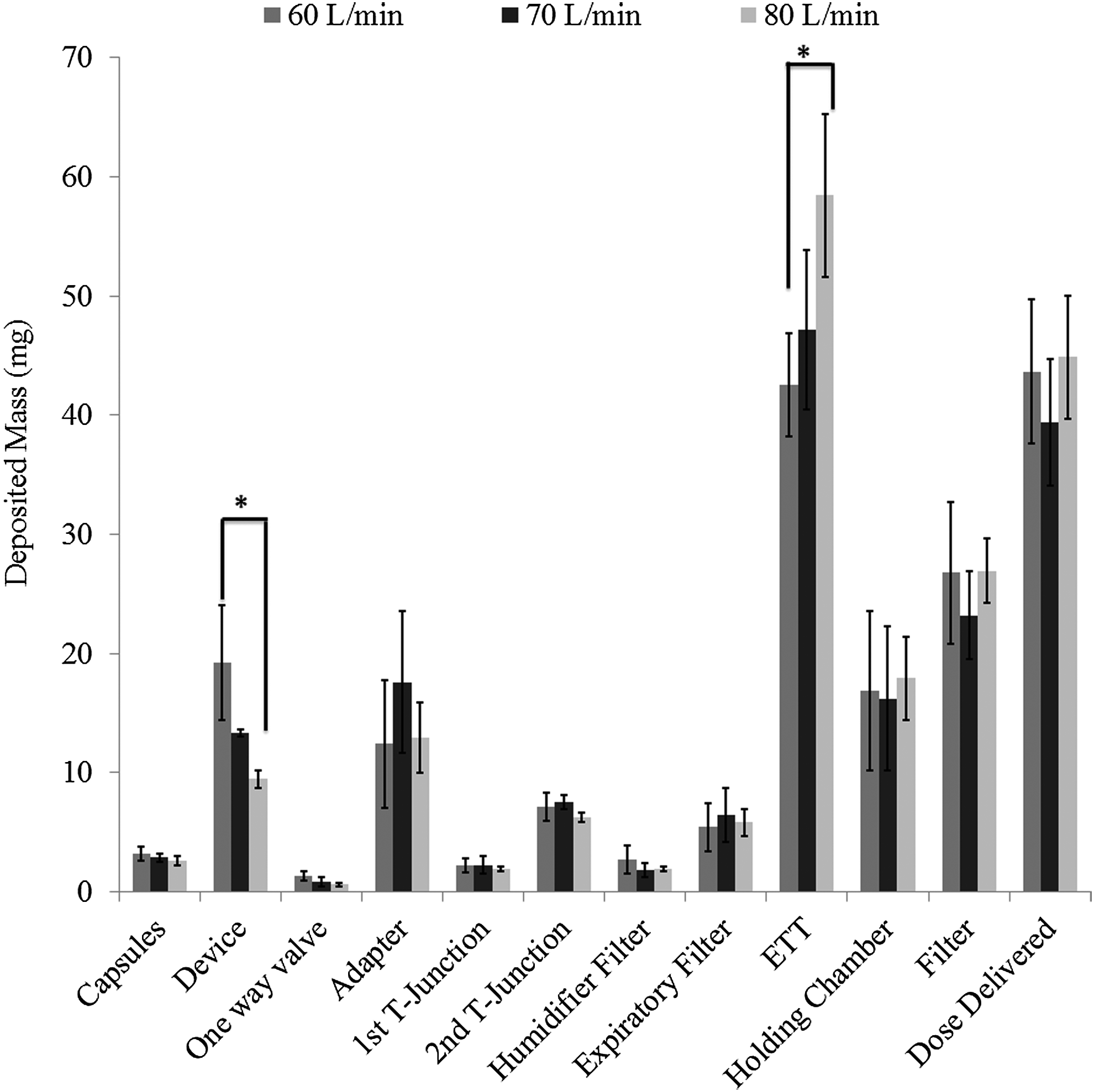
The deposition of mannitol in each part of the setup at flow rates of 60, 70, and 80 L/min. The loading dose was 160 mg and 9.5 mm endotracheal tube was used. Error bars represent ±1 standard deviation. *Denotes a statistically significant difference between the indicated results. ETT, endotracheal tube.
There is a trend of increasing deposition in the endotracheal tube with increasing flow rate, with 42.5 ± 4.36 mg at 60 L/min, 47.1 ± 6.69 mg at 70 L/min, and the 80 L/min having the highest deposition of 58.4 ± 6.79 mg. Statistical analysis showed that the depositions between the 60 and 80 L/min were statistically significant (p = 0.042) in the endotracheal tube. Conversely, the mannitol, which remained in the device, showed a decreasing trend with increasing flow rates (Fig. 3). Device retention ranged from 19.3 ± 4.81 mg at 60 L/min to 13.4 ± 0.28 mg at 70 L/min and down to 9.46 ± 0.76 mg at 80 L/min, with the difference approaching significance between 60 and 80 L/min (p = 0.052). As the flow rate increased, more powder left the device. However, this did not translate into more dose delivered. Instead, the powder deposited in the endotracheal tube, shown by the increased tube depositions.
The particle size distributions, obtained from the Spraytec, of the aerosol emitted from the endotracheal tube are shown in Table 2. The amount of aerosols having particle sizes smaller than 3 and 5 μm is also included. These are the sizes that are conventionally considered capable of depositing in the lungs via oral inhalation. The volume median diameters, D50, of the aerosols obtained at all the flow rates were smaller than 5 μm.
The loading dose was 160 mg (n = 3).
The best consistency, as evidenced by the small standard deviation in Table 2, in the dose delivered, was obtained when 70 L/min was used. For this reason, subsequent tests were done at this flow rate. A shorter tracheal tube, 7.5 mm tracheostomy tube, was tested at 70 L/min for comparison. A higher loading dose (four capsules, each filled with 80 mg) was also used to study the effect on the dose delivered.
The difference in deposition for each part of the setup before collection holding chamber and filter was shown to be statistically insignificant except for the tracheal tubes (p = 0.032 for the 160 mg dose and 0.010 for the 320 mg dose) and the humidified filter (p = 0.011 for the 160 mg dose). There was more powder deposited in the longer endotracheal tube (350 mm) than the shorter tracheostomy tube (115 mm) at both 160 and 320 mg. As a result, the delivered dose (Fig. 4) shows significant differences between the two tracheal tubes (p = 0.013 for 160 mg; p = 0.002 for 320 mg). The standard deviation in the delivered dose in all cases was <10%, which implies consistent delivery, except the delivery of 160 mg dose using the 9.5 mm endotracheal tube (14%). With the 160 mg dose, the delivered doses were on average 24.3% (39.4 ± 5.33 mg) and 35.6% (56.9 ± 4.82 mg) of the loaded dose for the endotracheal and tracheostomy tubes, respectively. With the 320 mg dose, the delivered doses were on average 26.7% (85.3 ± 7.01 mg) and 39.7% (126.6 ± 6.52 mg) of the loaded dose for the endotracheal and tracheostomy tubes, respectively. The particle size of the aerosols emitted from the tracheal tube is shown in Table 3. The amount of mannitol <3 and 5 μm, shown in Table 3, was higher for aerosols emitted from the tracheostomy tube than the endotracheal tube for the 160 mg dose but similar for 320 mg dose.
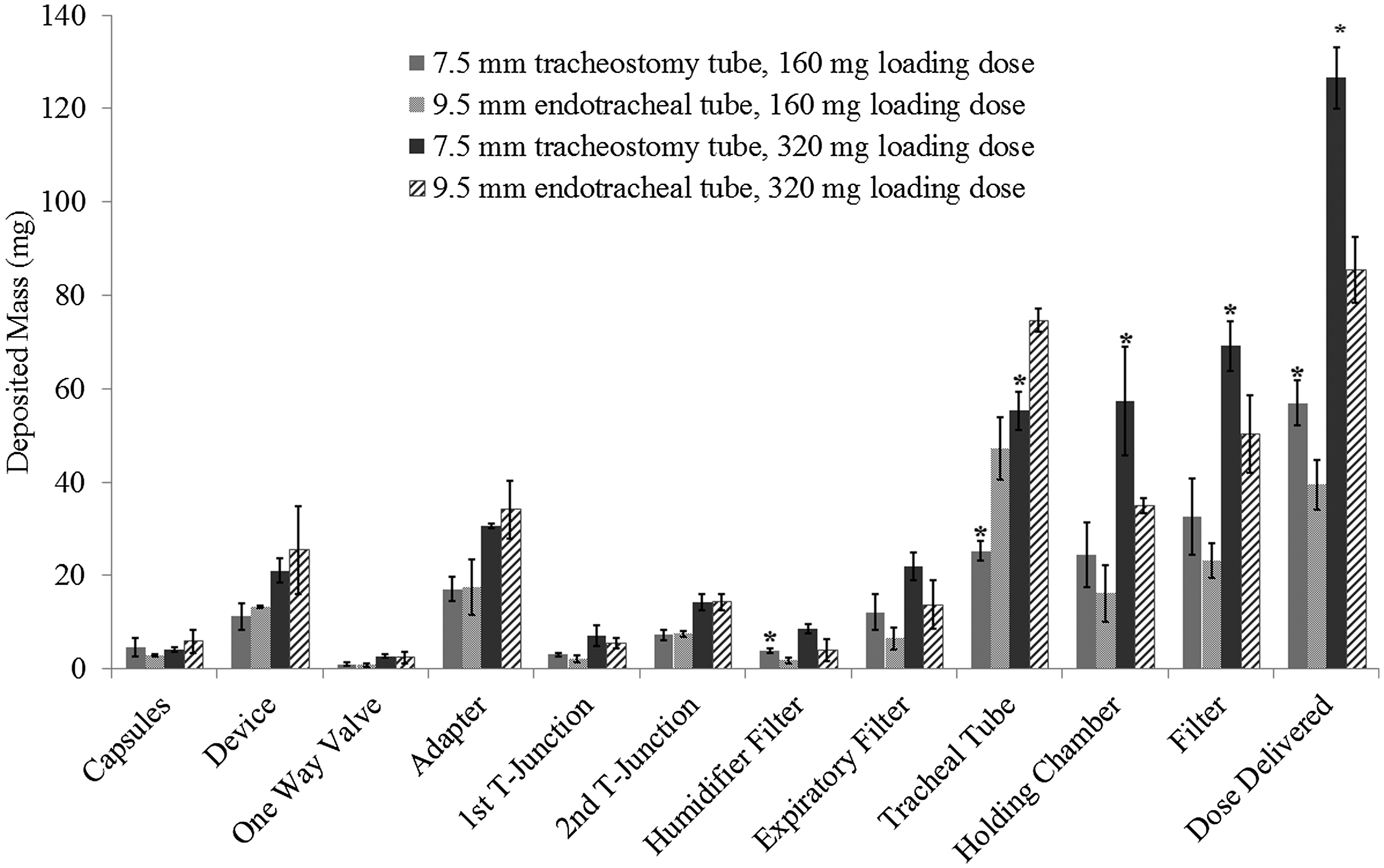
Comparison between different tracheal tubes using 160 and 320 mg loading doses and a flow rate of 70 L/min. N = 3. Error bars represent ±1 standard deviation. *Denotes a statistically significant difference to the subsequent indicated result.
Discussion
The deposition profiles in Figure 3 show that a higher flow rate from the ventilator provided more energy to empty out the powder from the device resulting in less device retention. At the same time, a higher flow rate caused more powder to deposit in the endotracheal tube. In the experimental setup, the endotracheal tube was in its natural curving position as it will be in a real clinical setting. The tube was also wet because of the humidified air from the ventilator. Consequently, powder entering the tube at higher flow rate would be more likely to deposit there. The deposition in the adaptor due to impaction was, however, found to be similar with different flow rates. The adaptor was drier than the endotracheal tube as it was inserted just before the introduction of dry powder to bypass the wet T-junctions. The humidified air from the ventilator wetted the endotracheal tube and the T-junctions.
The delivered doses obtained from the current setup were lower than the doses reported in our previous article where a ventilation bag was used to provide a positive pressure airflow to disperse the powder.(24) This is because a much higher flow rate could be achieved with a ventilation bag than with the ventilator. The flow rate entering the DPI ranged from 90 to 130 L/min and the dose delivered ranged from 84.5 ± 4.46 to 99.7 ± 12.5 mg.(24) In the current setup, the flow rate entering the DPI ranged from 40 to 60 L/min and the dose delivered ranged from 42.5 ± 4.36 to 58.4 ± 6.79 mg. The difference in the delivered dose can also be contributed by the difference between the setups. With the ventilation bag, there was no expiration cycle.
All the aerosols emitted from the tracheal tubes (endotracheal and tracheostomy tubes) were completely captured on the wet stages of multistage liquid impinger (MSLI). However, when a ventilator was used, an MSLI could not be used. If an MSLI was put in line, a vacuum pump would have to be connected and the ventilator will assume there was a leakage in the line and would not continue to work. In our current setup, the emitted aerosols from the tracheal tubes entered the holding chamber and collection filter. Although the holding chamber's wall and collection filter were wetted before the introduction of aerosols, some aerosols were carried away from the chamber during the expiration cycle. This was confirmed by the powder depositions in the expiratory and humidifier filters. However, the small amount deposited in these filters (≤7% of the total loading dose) showed that this in vitro aerosol collection to determine the delivery dose may be sufficient to represent the in vivo scenario.
Although the volume median diameter (D50) values of the aerosols emitted from the endotracheal tube were smaller than five micron, the D90 values are quite large (Table 2). The D90 values are much larger than the D90 of the primary particles of mannitol, indicating that the large mannitol agglomerates in the powder were not well dispersed. However, because the tracheal tubes bypass the oropharynx in vivo, essentially all the powder leaving the tube will deposit in the lungs.
There is a significant increase in the powder depositions in the long endotracheal tube compared to the short tracheostomy tube (Fig. 4). With the 160 mg dose, the powder retention increased from 25.3 ± 2.15 to 47.1 ± 6.69 mg and with the 320 mg dose, the powder retention increased from 55.3 ± 4.15 to 74.6 ± 2.46 mg. The lesser deposition in the short tracheostomy tube produced a higher delivered dose. With the 160 mg, the delivered dose increased from 39.4 ± 5.33 to 56.9 ± 4.82 mg, and with the 320 mg dose, the delivered dose increased from 85.3 ± 7.01 to 126.6 ± 6.52 mg. The difference in powder retention in the tube and delivered dose with the different length tracheal tube was not observed in our previous work.(24) This may be due to the finer aerosol particles (hence less inertial impaction) produced by a higher flow rate from the ventilation bag.
Moore et al.(34) performed an in vitro testing to elucidate the effect of adding 0%, 0.5%, 2%, 4%, 10%, and 20% (w/v)
The mannitol concentration w/v (%) based on the depositions in the tracheal tubes is shown in Table 4. The concentrations of mannitol in the tubes were all higher than 10% and mostly higher than 20%. This means that the proliferation of the common CF pathogens in the tube would be low. However, this would ultimately need to be confirmed in a clinical setting.
The deposition profiles in Figure 4 also show that the set flow rate of 70 L/min (the actual flow rate entering the DPI was 50 L/min) was sufficient to aerosolize the 80 mg powder contained in the capsule (four capsules were dispersed consecutively to make the 320 mg total loading dose). When the deposition amount in capsule, device, adapter, and T-junctions was expressed as a percentage of the loaded dose, there was no significant difference between the 160 and 320 mg doses. The percentage of dose delivered was also similar for both loading doses (35.6% ± 3.01% and 39.6% ± 2.04% with tracheostomy tube at 160 and 320 mg doses, respectively; 24.6% ± 3.33% and 26.7% ± 2.19% with endotracheal tube at 160 and 320 mg doses, respectively). This implies that the aerosolization of powder at the higher loading was as efficient as the lower loading. Table 3 shows that with both 160 and 320 mg loading doses, the D50 values of the aerosols emitted from the endotracheal and tracheostomy tubes were in the acceptable respirable range.
Conclusion
We have developed an in-line setup that successfully delivered dry powders of mannitol by using inspiratory airflow from the mechanical ventilator. This work serves as a technical proof-of-concept since mannitol is not approved yet for administration in mechanically ventilated patients. With the 9.5 mm endotracheal tube and 70 L/min, the delivered dose was 24.6% ± 3.33% and 26.7% ± 2.19% of 160 and 320 mg loaded dose, respectively. Using the shorter tracheostomy tube, the in-line system of delivery was able to deliver 35.6% ± 3.01% and 39.5% ± 2.04% of 160 and 320 mg loaded dose, respectively. The volume median diameter, measured by laser diffraction, of the particles emitted from the tracheal tubes showed that the delivered aerosols were in the respirable range with the D50 values varied from 3.65 ± 1.71 to 5.17 ± 0.87. Its ability to deliver high doses in a short period of time provides potential advantages over other aerosol generations using the pressurized metered dose inhalers and nebulizers. The consistent delivery and generation of a dose with suitable sizing characteristics allow it to deliver an efficient and safe dose to intubated patients.
Our proposed system can easily accommodate different DPIs that can replace the Osmohaler allowing for versatility. With this in mind, the system is also able to adapt to different doses that are required for different drugs through the utilization of different sized capsules and varying loading doses. However, one has to bear in mind that different drug formulations may generate different dispersion characteristics from what was reported here. Hence, in vitro testing is required to determine the delivered dose. Using our current setup, the patient will not need to be disconnected from the ventilator because of the two parallel inspiratory flow lines (one goes through the humidifier and the other one goes through the DPI). Therefore, it is more beneficial for the patients and potentially more attractive to clinicians for its adaptation for clinical use. Moreover, the dry powder will not be exposed to the wet humid air, which may potentially compromise effective aerosolization.
Footnotes
Acknowledgments
H.-K.C. is grateful to Mr. Richard Stenlake for his generous financial support. The authors thank Prof. Balu Bhaskar for the general advice provided in the beginning of this work. The authors are also very thankful to the Intensive Care Unit in the Prince Charles Hospital (Brisbane) for the donation of the Puritan Bennet Ventilator used in this work. The mannitol powder used in this work was kindly donated by Pharmaxis, Australia.
Author Disclosure Statement
No competing financial interests exist.