
Abstract
Abstract
Background:
The unit dose dry powder inhaler (UD-DPI) is being considered as an alternative inhaler platform that, if developed, has the potential to improve access to inhaled respiratory medicines in developing countries.
Aim:
This study compared the systemic exposure of fluticasone furoate after delivery from the UD-DPI with that from the ELLIPTA® inhaler.
Methods:
This open-label, five-way cross-over, randomized, single-dose study in healthy subjects evaluated fluticasone furoate systemic exposure of three dose strengths (using four inhalations), 4 × 80 μg [320 μg], 4 × 100 μg [400 μg], and 4 × 140 μg [560 μg]), and two percentages of drug in lactose blends (0.6% and 0.8% by weight) after delivery from the UD-DPI compared with systemic exposures from the ELLIPTA inhaler (4 × 100 μg [400 μg] dose, 0.8% lactose blend). The primary treatment comparisons were area under the concentration–time curve from time 0 to 6 hours [AUC0–6] and maximum plasma concentration [Cmax].
Results:
After single-dose administration of fluticasone furoate, systemic exposure was lower from all UD-DPI formulations versus the ELLIPTA inhaler in terms of both AUC0–6 [AUC0–6 geometric least squares mean (GLM) ratios confidence interval (90% CI) for: UD-DPI (400 μg 0.8% blend)/ELLIPTA: 0.61 (0.55–0.67) and Cmax GLM (90% CI) for: UD-DPI (400 μg 0.8% blend)/ELLIPTA: 0.56 (0.49–0.64)]. Systemic exposures were ∼10% lower for fluticasone furoate UD-DPI for the 0.8% blend versus the 0.6% blend [GLM ratio (90% CI); 0.90 (0.81–1.00) for AUC0–6 and 0.89 (0.77–1.01) for Cmax], and increasing doses of fluticasone furoate from the UD-DPI showed systemic exposures that were approximately dose proportional. All treatments were well tolerated.
Conclusions:
Fluticasone furoate systemic exposure was lower from the UD-DPI than from the ELLIPTA inhaler, but the UD-DPI formulations did demonstrate detectable systemic levels and approximate dose proportionality. Together with the good tolerability shown, these data support further evaluation of the UD-DPI as a potential device for delivering inhaled respiratory drugs.
Introduction
A
There are many challenges to managing asthma in developing countries that include underdiagnosis of asthma, availability and affordability of inhaled therapy, education of the public and healthcare providers, and cultural factors.(5,6) Tackling poor asthma control is particularly challenging when there is poor access to essential inhaled therapy, especially inhaled corticosteroids (ICSs), which are the most effective anti-inflammatory medication therapy for controlling asthma symptoms and reducing the risk of future exacerbations, in patients with persistent asthma.(1)
Affordability of inhaled therapy in developing countries, especially for low- and middle-income families, may be improved by making drugs available in a unit dose formulation. This would allow patients to purchase a lower number of dose units, but on a more frequent basis, and in quantities sufficient to provide chronic once-daily treatment, that is, a minimum of 7 days' treatment for an ICS therapy, compared with delivery through a multidose dry powder inhaler (DPI), which involves purchasing a month of treatment upfront.
Fluticasone furoate is a once-daily ICS therapy, approved for use in some countries as a monotherapy for the treatment of asthma, and/or in combination with vilanterol for the treatment of asthma and chronic obstructive pulmonary disease (COPD).(7–9) Fluticasone furoate displays a great affinity for the glucocorticoid receptor and high retention in human lung tissue; data for bioavailability represent absorption from the lung as the oral bioavailability from the swallowed portion of the inhaled dose is negligible (∼1%).(10) Fluticasone furoate is formulated in lactose for oral inhalation through a multidose dry powder ELLIPTA® inhaler *
The unit dose-DPI (UD-DPI) is intended to be a reuseable, reloadable low-cost unit dose inhaler with a bespoke double foil blister pack containing powder for oral inhalation. The UD-DPI device and blister system allows patients to buy a smaller quantity of doses than currently offered in DPIs that contain a monthly supply. The UD-DPI is molded from medical-grade polypropylene and is prepared for use by placing a blister into it. Once the blister has been inserted, the UD-DPI can be closed that automatically pierces the blister and exposes the medication for delivery. The UD-DPI is being developed as an alternative platform for delivering inhaled drugs, and has the potential to improve access to inhaled respiratory medicines in developing countries.
The aim of this study was to obtain preliminary pharmacokinetic information on the comparability of the UD-DPI system relative to the ELLIPTA inhaler in delivering fluticasone furoate to healthy subjects.
Materials and Methods
Study design and subjects
This was an open-label, five-period, cross-over, randomized, single-dose study in healthy subjects (GSK protocol 200939; NCT02218723). The study compared the systemic exposure of fluticasone furoate delivered by the UD-DPI (four different formulations) and the ELLIPTA inhaler. The four blister formulations investigated with the UD-DPI included three dose strengths and two different percentages of drug in lactose blends:
• Fluticasone furoate through the UD-DPI, 4 × 100 μg per blister from a 0.6% blend (total dose 400 μg) • Fluticasone furoate through the UD-DPI, 4 × 80 μg per blister from a 0.8% blend (total dose 320 μg) • Fluticasone furoate through the UD-DPI, 4 × 100 μg per blister from a 0.8% blend (total dose 400 μg) • Fluticasone furoate through the UD-DPI, 4 × 140 μg per blister from a 0.8% blend (total dose 560 μg) • Fluticasone furoate through the ELLIPTA multidose DPI, 4 × 100 μg per blister from a 0.8% blend (total dose 400 μg)
The total duration for dosing was 4 minutes for both the ELLIPTA inhaler and the UD-DPI, in which four inhalations were administered 60 seconds apart. The doses administered were higher than therapeutic doses of fluticasone furoate (100 or 200 μg) to ensure measureable plasma levels of fluticasone furoate, above the lower limit of quantification (LLQ, 10 pg/mL). Subjects were instructed to rinse their mouth with water and spit after dosing. There was a minimum 7-day washout period between each treatment and a follow-up visit, 7 to 14 days after completion of the last treatment.
For each treatment evaluation, subjects were admitted to the clinical unit the evening before and were dosed in clinic on the following morning, and remained at site until completion of the 48-hour postdose pharmacokinetic (PK) sample collection. Subjects underwent training on how to use the ELLIPTA inhaler and UD-DPI devices, and were only included in the study if they could use the devices correctly.
Eligible subjects were healthy male or female subjects aged 18 to 65 years with a body weight ≥50 kg and a body mass index of 19–34 kg/m2. Subjects were required to be nonsmokers (former smokers had not smoked in the preceding 6 months and had a pack history of ≤5 pack years).
Key exclusion criteria included current diagnosis or history of liver disease, regular alcohol consumption in the previous 6 months (defined as an average weekly intake of >21 U for males or >14 U for females. One unit was defined as equivalent to 10 g of alcohol, for example, 270 mL of full strength beer (4.8%), 100 mL of wine (13.5%), and 30 mL of spirit (40%)), a positive smoking breath test, a positive test for hepatitis B or C, or to human immunodeficiency virus, and a clinically significant abnormal electrocardiogram (ECG). Subjects were not permitted to take any prescription or nonprescription drugs (other than paracetamol ≤2 g/day), red wine, grapefruit- or exotic citrus fruit-containing products for at least 7 days before the first study treatment, systemic corticosteroids in the 12 weeks before screening, and inhaled or topical steroids in the 4 weeks before screening, until completion of the follow-up visit.
All subjects gave written informed consent before participation and the study was approved by Bellberry Ethics Committee, Eastwood, South Australia, Australia.
Pharmacokinetic assessments
For each single-dose treatment, blood samples were collected into tripotassium ethylenediaminetetraacetic acid tubes at predose, 5, 10, 20, 30, and 45 minutes, 1, 1.5, 2, 3, 4, 6, 8, 10, 12, 16, 24, 36, and 48 hours postdose, relative to the beginning of treatment inhalation. Samples were centrifuged in a refrigerated centrifuge at 1500 g (3000 rpm) for 10 minutes at 4°C, and stored at −20°C before shipment to York Bioanalytical Solutions Ltd. (York, United Kingdom) for analysis. Plasma samples were analyzed for fluticasone furoate using a validated analytical method based on protein precipitation, followed by high-performance liquid chromatography/mass spectrometry analysis.
The following PK parameters were determined from the plasma fluticasone furoate concentration–time data using noncompartmental Model 200 (for extra vascular administration) for fluticasone furoate in Phoenix Build 6.3.0.395, WinNonlin 6.3 (Pharsight Corporation, St. Louis, MO): area under the concentration–time curve from time 0 to 6 hours (AUC0–6) and 24 hours (AUC0–24), maximum plasma concentration (Cmax), and time at which Cmax was observed (tmax).
Safety
On each treatment day, vital signs (heart rate and blood pressure) were measured at predose and at the end of the observation period, 48 hours postdose. Twelve-lead ECG measurements were made premorning dose and 1 hour postdose on each treatment day. Routine laboratory assessments were performed the evening before each treatment and during follow-up postlast dose. Adverse events (AEs) were monitored throughout the study from the first treatment period.
Aerodynamic particle size distribution
Aerodynamic particle size distribution of the delivered doses from the UD-DPI and ELLIPTA inhaler was characterized using the next-generation impactor (NGI) at a flow rate of 60 L/min. Fine particle mass (FPM) data were generated from NGI by summing the mass of fluticasone furoate deposited on impactor stages 3 to 5, leading to an aerodynamic particle size range from 0.9 to 4.5 μm based on the effective cutoff diameter of each impactor stage at a flow rate of 60 L/min.
Statistical analyses
Based on a previous GSK fluticasone furoate study (NCT01485445), it was estimated that with a sample size of 24, the precision for the comparisons of interest would be within 15% (for AUC) and 10% (for Cmax) of the observed point estimate, where precision was expressed as the half-width of the 90% confidence interval (CI). Thirty healthy volunteers were planned to ensure 24 evaluable subjects.
After loge transformation, AUC0–6, AUC0–24, and Cmax of fluticasone furoate were separately analyzed using a mixed effects model with fixed effect terms for period and treatment. Subject was treated as a random effect in the model.
Point estimates and their associated 90% CIs were constructed for all treatment comparisons; these were then back transformed to provide point estimates and 90% CIs for the geometric mean ratios (all formulations of UD-DPI vs. the ELLIPTA inhaler). The same method was used to explore the effect of blend [ratio of UD-DPI (4 × 100 μg 0.8% blend) vs. UD-DPI (4 × 100 μg 0.6% blend)]. tmax was analyzed separately using Wilcoxon's matched pair method.
Results
Thirty subjects were randomized to treatment and 26 completed all five treatments as planned. Of the four subjects withdrawn, one withdrew because of finding the study requirements too restrictive after receiving two treatments (assessments not completed for the second treatment visit), one withdrew consent for personal reasons after two treatments, one was withdrawn after a positive drug screen and having received four treatments, and one was withdrawn because of an AE of upper respiratory tract infection after one treatment only. The mean age was 28.3 years, 60% were male and 90% were Caucasian, with a mean body mass index of 24.5 kg/m2 (Table 1).
Pharmacokinetics data
The bioanalytical method, with LLQ of 10 pg/mL, was not sensitive enough to fully characterize the PK profile of fluticasone furoate because of low plasma levels after single-dose administration, particularly after delivery from the UD-DPI (31% of samples nonquantifiable) versus the ELLIPTA inhaler (9% of samples nonquantifiable). Owing to a large number of plasma concentrations less than LLQ in the terminal phase, AUC0–6 was used as the primary comparator.
After single-dose administration of fluticasone furoate, absorption was faster from the ELLIPTA inhaler (median tmax = 0.5 hour) than from the UD-DPI (median tmax = 0.75 hour for all formulations; Table 2). Fluticasone furoate systemic exposure was lower from all the UD-DPI formulations versus the ELLIPTA inhaler in terms of both AUC0–6 and Cmax (Fig. 1 and Tables 2, 3). Inhalation of the same dose and blend of fluticasone furoate (400 μg, 0.8% blend) from the ELLIPTA inhaler and UD-DPI resulted in geometric least squares mean (GLM) ratios (90% CI) for UD-DPI/ELLIPTA of 0.61 (0.55–0.67) for AUC (0–6) and 0.56 (0.49–0.64) for Cmax, suggesting 39%–44% lower fluticasone furoate systemic exposure after UD-DPI (Table 3).
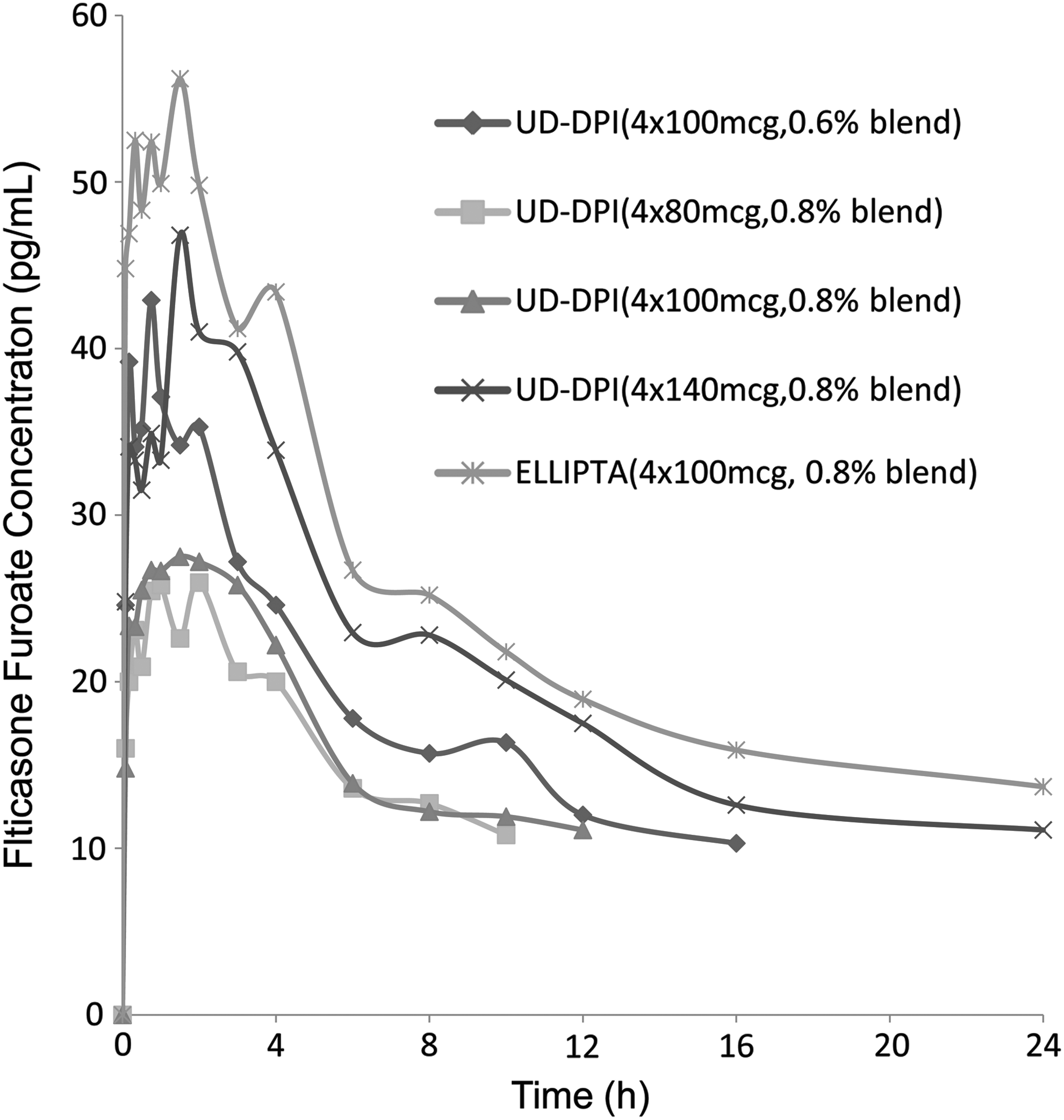
Plot of fluticasone furoate median concentration–time profile UD-DPI, unit dose dry powder inhaler.
Data presented as geometric mean (% coefficient of variation between subjects [CVb]), 95% CI except tmax, presented as median (range).
AUC0–6, area under the concentration–time curve from time 0 to 6 hours; CI, confidence interval; FF, fluticasone furoate; UD-DPI, unit dose dry powder inhaler; AUC0–24, area under the concentration-time curve from time 0 to 24 hours; Cmax, maximum plasma concentration; tmax, time at which Cmax was observed.
Data presented as geometric least squares mean ratio [90% CI]. UD-DPI, unit dose dry powder inhaler; AUC0–6, area under the concentration-time curve from time 0 to 6 hours; AUC0–24, area under the concentration-time curve from time 0 to 24 hours; Cmax, maximum plasma concentration.
Systemic exposures were ∼10% lower for fluticasone furoate UD-DPI for the 0.8% blend than for the 0.6% blend [GLM ratio (90% CI); 0.90 (0.81–1.00) for AUC (0–6) and 0.89 (0.77–1.01) for Cmax] (Fig. 1). Delivery of increasing doses of fluticasone furoate from the UD-DPI showed systemic exposures that were approximately dose proportional (∼10%–15% less from the UD-DPI vs. the ELLIPTA inhaler) (Table 4).
AUC0–6, area under the concentration-time curve from time 0 to 6 hours; AUC0–24, area under the concentration-time curve from time 0 to 24 hours; Cmax, maximum plasma concentration.
Safety
Similar AEs were reported across all treatment groups; the most frequently reported AEs were catheter site pain, reported by 40% of subjects, and headache, reported by 37% of subjects (Table 5). There were no reported serious AEs, and no clinically significant findings for vital signs, ECG, or laboratory data.
Aerodynamic particle size distribution
Fluticasone furoate UD-DPI 100 μg product strength (0.8% blend) produced lower FPM than the equivalent dose and blend delivered through the ELLIPTA inhaler (Fig. 2), consistent with the data shown for total systemic exposure. There was good dose proportionality across the three fluticasone furoate UD-DPI doses for the 0.8% formulation and small differences between the fluticasone furoate UD-DPI 100 μg product strength (0.6% and 0.8% blends), also consistent with the data shown for total systemic exposure (Figs. 1 and 2).

Variability plot showing fluticasone furoate FPM (as μg/blister) for UD-DPI and ELLIPTA inhaler clinical batches. FPM, fine particle mass. UD-DPI, unit dose dry powder inhaler.
Discussion
The UD-DPI is a novel DPI system that is being considered for development to help meet the need for improved access to inhaled respiratory medicines for patients in developing countries. The main finding of this study was that systemic exposures after inhalation from the UD-DPI formulations were lower than those from the ELLIPTA inhaler. This was partly explained by differences in the in vitro data, but there may be differences in other characteristics that could not be determined in this study. With respect to the UD-DPI formulations tested, there was only a small difference in the effect of two different blends, and there was a trend for higher systemic exposures with higher doses of fluticasone furoate, that is, approximate dose proportionality. Importantly, all UD-DPI treatments were well tolerated with no reports of clinically significant systemic side effects.
The bioanalytical method used in this study was not sensitive enough to determine fluticasone furoate plasma concentrations in approximately one-third of the UD-DPI PK samples, even though higher single doses than the recommended therapeutic dose of fluticasone furoate were used. This is a challenge for studies evaluating ICS therapies.(11,12) Despite this, detectable plasma levels were observed for a majority of the samples, and the demonstration of approximate dose proportionality suggests that the PK profiling results achieved after UD-DPI administration were robust. However, no formal dose proportionality testing was done. In another study that evaluated the PK performance of the UD-DPI in delivering salbutamol to healthy volunteers, comparable total systemic exposure to the DISKUS®† inhaler and no greater systemic exposure than that shown with the metered dose inhaler were demonstrated, in addition to similar systemic exposure with the two salbutamol blends tested with the UD-DPI and approximate dose proportionality with ascending dose levels.(13)
These results together with the results of this study suggest that the UD-DPI device has the potential to deliver inhaled drugs for the treatment of respiratory disease, although further evaluation of the novel UD-DPI is still required. The sample size in this proof of technology study was too small to assess covariate effects using population pharmacokinetic methodology, and the large variability observed in PK parameters was also attributed to the small sample size. Larger studies in later phases of clinical development would be required to fully characterize pharmacokinetics in patient populations.
In this study, data for systemic exposure and FPM were broadly aligned with each other, although the correlation between in vitro and in vivo parameters was not consistent. Other comparative studies of inhalers containing corticosteroids have shown poor correlations between in vitro and in vivo data, suggesting that in vitro data alone are insufficient to predict comparability between two different devices.(14) In a comparative bioavailability study of Seretide®†† 50/250 μg Diskus and Seretide 50/250 μg delivered through the Rotacaps®/Rotahaler®††† in subjects with asthma and COPD, no major differences in in vitro aerodynamic particle size profiles or systemic pharmacodynamic end points were demonstrated, but this study failed to show pharmacokinetic bioequivalence in terms of fluticasone propionate and salmeterol systemic exposure, highlighting a requirement for further refinement of the Rotacaps/Rotahaler performance.(15)
A lack of agreement between PK and FPM data in the UD-DPI salbutamol study was also observed, reiterating the importance of providing a complete package of data, including device comparability, in vitro and PK performance, together with clinical efficacy and safety evaluations in relevant patient populations, when assessing two inhalers for therapeutic bioequivalence.(16)
In conclusion, this exploratory study showed that administration of fluticasone furoate UD-DPI resulted in lower systemic exposures than administration of fluticasone furoate through the ELLIPTA inhaler, but did achieve detectable systemic levels and approximate dose proportionality. These data, together with the results from the corresponding salbutamol study, suggest that the UD-DPI has the potential to be developed as an alternative inhaler platform.
Footnotes
Acknowledgments
The authors thank Jon Hall for providing the in vitro data (R&D, GSK, United Kingdom). Editorial support in the form of draft article development, collating of author comments and copyediting, assembling tables, and referencing was provided by Kate Hollingworth of Continuous Improvement Ltd., and was funded by GSK.
Author Disclosure Statement
This study was funded by GSK (Protocol 200939; NCT02218723). All authors are GSK employees and shareholders.