
Abstract
Abstract
Background:
Particles in exhaled air (PEx) provide samples of respiratory tract lining fluid from small airways and offer a new opportunity to monitor pathological changes. The exhaled particles are produced by reopening of closed small airways and contain surfactant. The amount of PEx varies by orders of magnitude among subjects. A standardized breathing pattern reduces the variation, but it remains large and the reasons are unknown. The aim of the present study was to assess to what extent sex, age, body size, and spirometry results explain the interindividual variation of PEx among healthy middle-aged subjects.
Methods:
The PExA® instrument was used to measure PEx in 126 healthy middle-aged nonsmoking subjects participating in the European Respiratory Community Health Survey (ERCS-III). The subjects performed a standardized breathing maneuver involving expiration to residual volume, a breath-hold of 3 seconds, a full inspiration, and then a full expiration into the PExA instrument. PEx number concentrations were expressed per exhalation and per exhaled liter. Age and anthropometric and spirometric variables were analyzed as potential predictors.
Results:
PEx/L was consistently and negatively associated to lung size-related variables and accordingly lower in men than in women. PEx/Exhalation was similar in women and men. Increasing age was associated with increasing PEx. Reference equations are presented based on age, weight, and spirometry variables and independent of sex. These predictors explained 28%–29% of the interindividual variation.
Conclusions:
The interindividual variation of PEx after a standardized breathing maneuver is large and the considered predictors explain a minor part only.
Introduction
S
The number of exhaled particles per breath has been found to vary among subjects by orders of magnitude,(3,15–18) apparently depending to a great extent on the breathing maneuver preceding the exhalation when particles are being counted.(6,11) The deeper the expiration the larger the number of particles counted during the following exhalation. Furthermore, breath holding at full inspiration before the final exhalation reduces the amount of exhaled particles, whereas breath holding at maximal expiration increases the amount of exhaled particles.(19) However, also when the breathing maneuvers are carefully standardized, the variation between subjects appears to be large as shown in studies of small numbers of healthy subjects.(6,11,20) Reasons for the large variation between subjects have been insufficiently investigated. Only the effect of age has been studied in small samples of healthy subjects but with inconsistent results,(4,6) and in a recent study, pollen season and outdoor temperature were found to have an effect.(18)
The aim of the present study was to find out to what extent sex, age, body size, spirometry results, pollen season, and outdoor temperature could explain the variation between subjects using a standardized breathing maneuver.
Materials and Methods
Participants
The present study represents a subsample of the European Community Respiratory Health Survey III, investigated in Gothenburg between March 2011 and October 2012, when the participants were 41–66 years of age. The participants were randomly selected from the population in the Gothenburg area but enriched by subjects reporting asthma symptoms. Eight hundred eleven subjects were invited to the clinical visit and 278 responded to the invitation. Exhaled particles were measured in 211 subjects of whom 207 had acceptable recordings without technical problems.
At the clinical visit, height without shoes and weight with light clothes were measured. A questionnaire was administered by a trained interviewer in a quiet room. It contained detailed questions on respiratory symptoms, self-reported asthma and allergic disorders, smoking habits, indoor environmental exposure, occupation, and asthma treatment. Subjects were excluded from the present analyses who answered any of the following questions affirmative (1) “ever have breathing trouble,” (2) “ever had asthma,” (3) “doctor diagnosed with chronic bronchitis,” (4) “doctor diagnosed with COPD,” (5) “doctor diagnosed with emphysema,” and (6) “doctor diagnosed with any other lung disease.” Thus, the present analysis concerns the 126 healthy nonsmokers and ex-smokers.
Daily outdoor temperature at a central measuring site on the date of each investigation was obtained from the Swedish Meteorological and Hydrological Institute. Written informed consent was obtained from each participant and the study was approved by the Central Ethics Review Board in Uppsala, as a part of a national study.
Exhaled particles
The equipment for counting exhaled particles, PExA® (PExA AB, Gothenburg, Sweden),(21) has been described previously in detail.(2) In short, a reservoir of 3.4 L is located inside a thermostatted box set at 36°C. An optical counter (Grimm model 1.108; Grimm Aerosol Technik GmbH & Co, Ainring, Germany) draws samples from the reservoir at the mouth end. At the other end of the reservoir, 36°C fully saturated air makes up for the sampling. The Grimm counter measures particles every second and covers diameters between 0.41 and 4.55 μm. Exhalation flow is measured by an ultrasonic flow meter (OEM flow sensor; Spiroson-AS, Medical Technologies, Zürich, Switzerland), enabling visualization of the expiratory flow and volume.
The standardized breathing maneuver applied has been described previously in detail(11,19) and starts with exhalation at normal flow rate to residual volume, a breath holding period for 3 seconds, followed by a maximal inhalation at optional flow rate to total lung capacity, and immediately followed by a slow exhalation to residual volume when the exhaled particles are being measured.
Two sampling sessions were performed consecutively, each to achieve 60 L of exhaled air. Each sampling session consists of repeated breathing maneuvers as described above, interrupted by short periods of tidal breathing of particle-free air until all particles in the reservoir had been counted. Measurements of exhaled particles were obtained before the administration of the bronchodilator. PEx number concentrations are expressed as n*1000 per liter exhaled air (kn/L) or kn/Exhalation (kn/Exhal). Furthermore, to assess major shifts in the particle size distributions, the mean particle mass was calculated for each subject, that is, (ng/L)/(kn/L) = pg. Average results of the two sampling sessions are presented.
Spirometry
Spirometry was performed with an EasyOne spirometer (EasyOne® Plus Diagnostic, Zurich, Switzerland). The forced vital capacity (FVC) and forced expired volume in 1 second (FEV1) were obtained before and 15 minutes after administration of a bronchodilator, 3*0.5 mg Bricanyl® (AstraZeneca, Södertälje, Sweden). The procedures complied with international guidelines.(22) The effect of bronchodilation (ΔFVC and ΔFEV1) was expressed as the difference between the value obtained after minus the value obtained before bronchodilation and expressed as a percentage of the value before bronchodilation, ΔFVC (%) or ΔFEV1 (%). FVC and FEV1 were expressed as a percentage of the reference value (% pred) according to Brisman et al.(23)
Analysis and statistics
The distribution of PEx among subjects is clearly skewed, as illustrated for PEx number concentrations among women in Figure 1. The natural logarithm of PEx (lnPEx) was not different from the normal distribution (Shapiro–Wilk test). PEx variation between subjects is described by the ratio of the maximum value and the minimum value and by the ratio of the 95th percentile and the 5th percentile. Comparisons between groups were tested by the Mann–Whitney test and two-sided p-values are reported. The association between lnPEx and various potential predictors is reported by the Pearson parametric correlation coefficients and the associated p-values. Potential predictors (p < 0.1) from univariate correlations were included in multiple regression analyses as was sex (female = 0 and men = 1). A backward selection process and considering a high variance inflation factor (>10) determined the remaining significant predictors. Parameter estimates, the residual standard deviation (RSD), and adjusted R2 are reported. The analyses were performed with SAS software (SAS 9.4, Cary, NC).
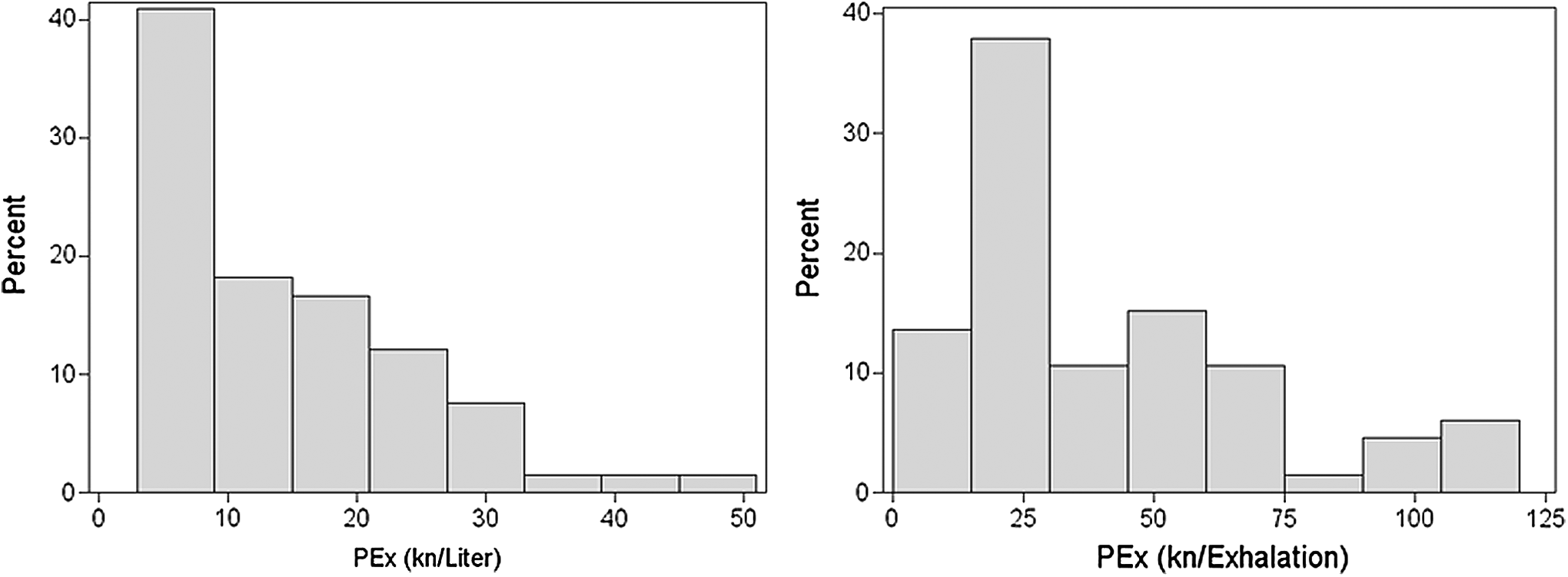
Distribution of exhaled particles of 66 healthy normal women, 41–66 years of age. Number of thousands of particles (kn) of exhaled particles is expressed either per exhaled liter or per exhalation and illustrates the non-normal distributions.
Results
The number of PEx in nonsmokers and ex-smokers did not differ, neither among women nor men, as illustrated in Figure 2. Furthermore, there was no association between PEx and pack-years among ex-smokers. Therefore, nonsmokers and ex-smokers have been merged in the analyses.
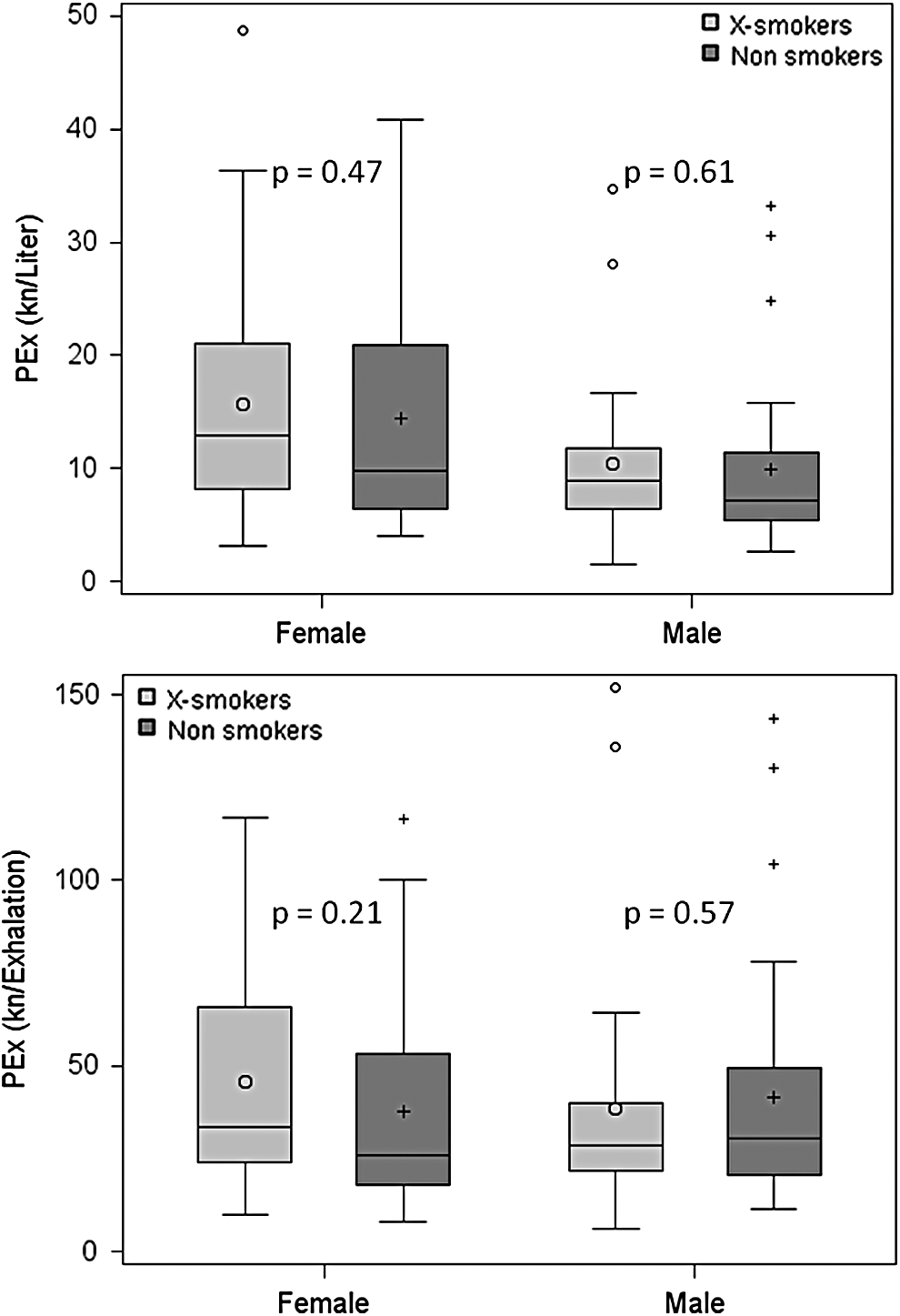
Box plots comparing PEx of nonsmokers with ex-smokers separately among women and men. PEx is expressed in terms of number concentration per exhaled liter (upper panel) and per exhalation (lower panel). p-Values from Mann–Whitney two-sided tests are given.
General characteristics and spirometry and PEx results are presented for women and men in Table 1. PEx amount differed significantly between women and men when expressed in terms of number concentration per exhaled liter but not when expressed in terms of number concentration per exhalation. The interindividual variation of the PEx variables was within one order of magnitude but considerably higher than the corresponding spirometric ratios (Table 2).
The table presents age, anthropometric characteristics, spirometric results, including the effects of bronchodilatation, PEx number concentrations and mean particle mass among healthy subjects subdivided by sex. Median values, the 5th and 95th percentiles are presented.
p-values refer to Mann–Whitney two-sided test for comparison between women and men.
FEV1, forced expired volume in 1 second; FVC, forced vital capacity; PEx, particles in exhaled air.
Factors of variation, as defined by the ratio between the maximum and minimum value and the ratio of the 95th percentile and the 5th percentile.
Age was significantly correlated to lnPEx, as illustrated in Figure 3. FEV1 (% pred) was positively correlated and reversibility of FEV1 (%) negatively correlated to lnPEx/Exhalation as illustrated in Figure 4. Potential predictions of PEx/L, PEx/Exhalation, and mean particle weight are presented in Table 3. PEx/L, but not PEx/Exhalation, is negatively correlated to the variables associated to lung size, that is, FVC, FEV1, height, and weight. Age is positively correlated to both PEx/L and PEx/Exhalation and weakly also to mean particle weight. No effect was found of time of the year of the investigation and there was no relationship with outdoor temperature.
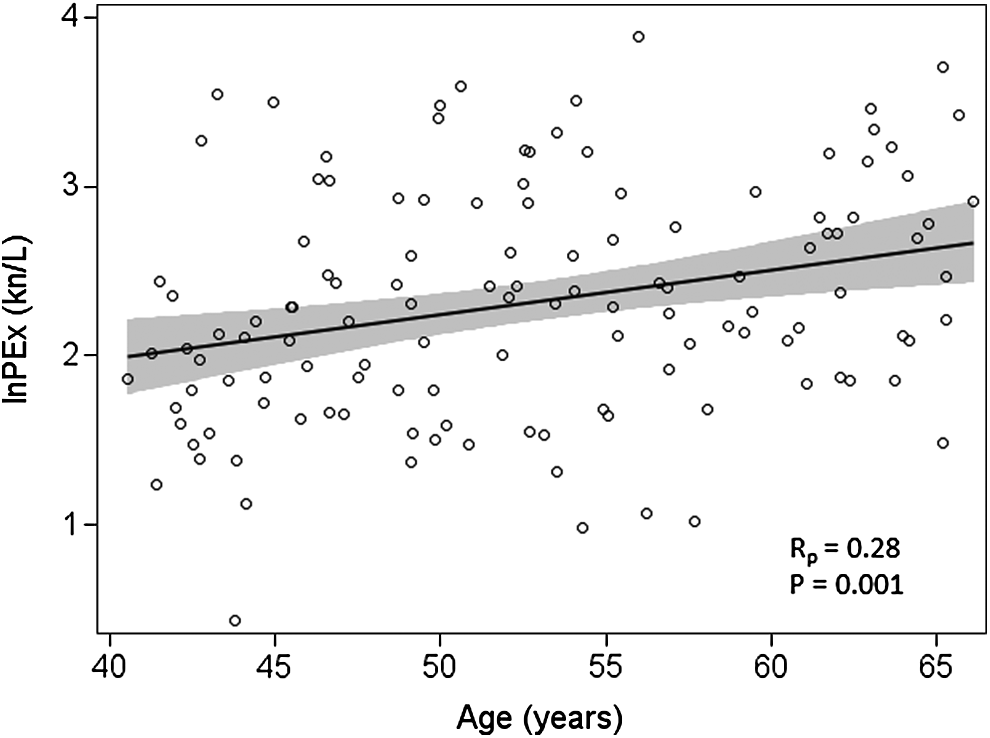
Plot illustrating the relationship between PEx and age. The natural logarithm of individual PEx number concentration per exhaled liter is plotted against age. The Pearson correlation coefficient and the associated p-value are given and the resulting regression line and the associated confidence interval are illustrated.
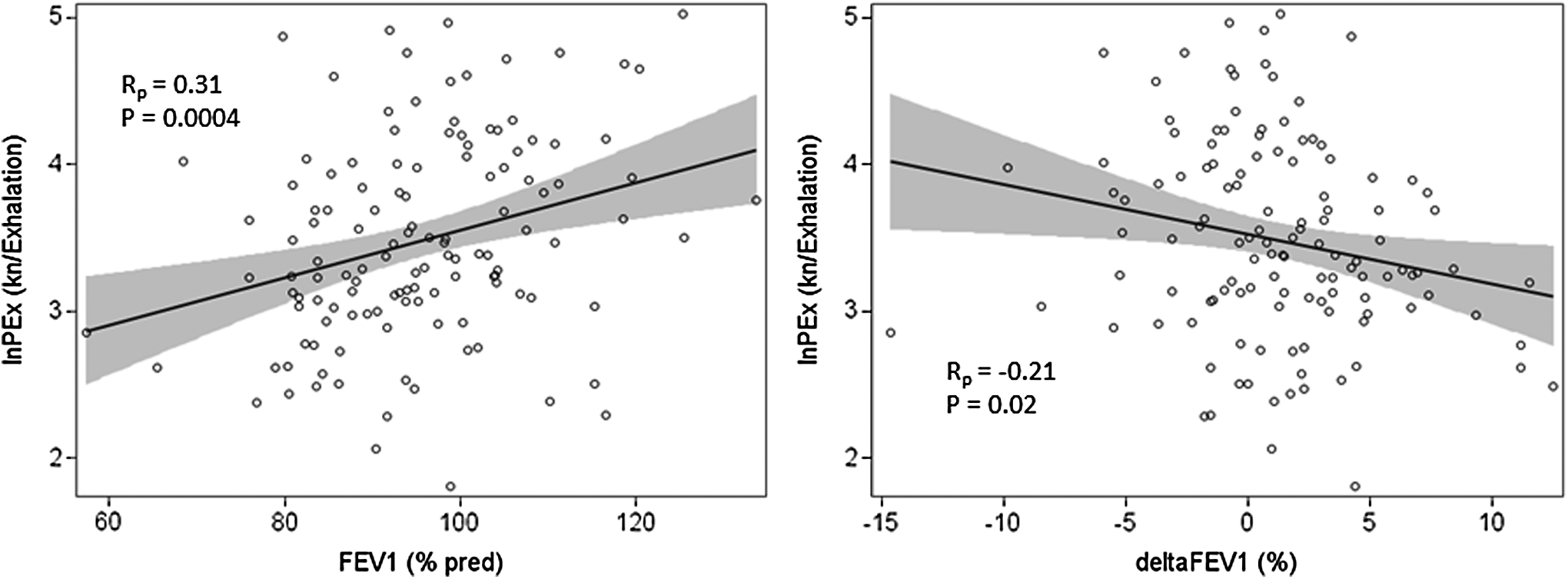
Plots illustrating the relationship between PEx and spirometric variables. In the left panel, the natural logarithm of individual PEx number concentration per exhalation is plotted against FEV1 (% pred) and in the right panel against the effect of bronchodilatation, that is, delta FEV1, expressed as a percentage of the value before bronchodilatation. The Pearson correlation coefficient and the associated p-value are given. Regression lines and associated confidence intervals are illustrated. FEV1, forced expired volume in 1 second.
Pearson correlations between the natural logarithms of particle number, mass concentrations, and mean particle mass. Correlation coefficients and associated p-values are presented.
Significant predictors remaining after the multiple regression analysis are presented in Table 4 with parameter estimates, adjusted R2, and RSD. Sex was not significant.
lnPEx number concentrations and mean particle mass regressed by the potentially significant predictors as selected by the univariate correlations presented in Table 3. The estimated coefficients of the remaining significant predictors are presented.
For example, a subject, 50 years of age, weight = 70 kg, and ΔFVC (%) = 8: PEx (kn/L) = exp(1.937 + 0.03100*50 − 0.01650*70 − 0.04919*8), that is, = 6.9 kn/L. The 5th percentile is calculated by inserting −1.645*0.34 within the parenthesis, that is, 5th percentile = 4.0 kn/L and the 95th percentile by inserting +1.645*0.34, that is, 95th percentile = 12.2kn/L.
PEx, particles in exhaled air; RSD, residual standard deviation.
Discussion
The present study shows that the interindividual variation of exhaled particle amount of a standardized maneuver is in the order of one magnitude and is considerably larger than that of spirometric variables. Age and anthropometric and spirometric variables explained 28%–29% of the interindividual variation.
Previous studies reported the interindividual variation of exhaled particles in terms of a maximum/minimum ratio to be orders of magnitude.(3,15–17) This extremely large variation is, however, to a considerable degree due to the various breathing maneuvers applied. A standardized breathing maneuver producing high number concentrations of PEx,(11) as in the present study, results in maximum/minimum ratios in the order of 15–29 when women and men are analyzed separately (Table 2). The variation is much larger than that of spirometric variables. The maximum/minimum ratio is, however, a crude index of variation and dependent on two values only, resulting in unreliable ratios when applied to the present irregularly distributed sample (Fig. 1). The 95th/5th ratios are less dependent on the extreme values but nevertheless dependent on a few values only and results in ratios between 7 and 14, reasonably similar in women and men (Table 2). More reliable measures of variation, that is, SD or coefficient of variation (CoV), are not appropriate because of the skewed distributions of PEx.
Men showed lower amounts of exhaled particles than women when expressed per exhaled liter, but there were no such differences when expressed per exhalation (Table 1). From the univariate associations presented in Table 3, it is obvious that all variables more or less related to lung size are significantly and negatively related to PEx/L, but no such associations are found regarding PEx/Exhalation. A possible explanation is that particles become more diluted in the larger lungs of men. Assuming that the amount of particles actually produced is similar in men and women and equally distributed in the lungs, PEx/L will be inversely proportional to total lung capacity. On the contrary, the amount of particles per exhalation, that is, per exhaled vital capacity, will depend on the quotient vital capacity/total lung capacity, that is, almost independent of lung size. The reasoning above pertains to the specific breathing pattern of the present study.
During tidal breathing, however, and again assuming particle production to be independent of lung size and equally distributed in the lungs, then both PEx/L and PEx/Exhalation will depend on the volume of functional residual capacity. The difference between PEx/L and PEx/Exhalation will depend on the size of the tidal volumes. If the tidal volume is 0.5 L then PEx/L = 0,5*PEx/Exhalation, but both will be equally dependent on the volume of the functional residual capacity.
Is it reasonable to assume that men and women produce similar amounts of particles by the opening of closed airways? If the particle production by the opening process in each terminal bronchiole in men and women is similar, then the amount of terminal bronchioles that close and open would be similar in men and women despite the difference in lung size. The number of alveoli is proportional to lung size,(24) but to the best of our knowledge, the relationship between lung size and the number of terminal bronchioles is unknown. Thus, the results indicate that the number of terminal bronchioles that close and open is similar among men and women.
The amount of exhaled particles is expressed per breath in most reports,(4–6,17) whereas we have previously expressed the exhaled amount per unit exhaled volume(2,11,19) as has other authors.(3) The explanatory power of the models presented in Table 4 is similar for lnPEx/L and lnPEx/Exhalation and both ways of expressing the amount of exhaled particles may be appropriate depending on the context.
Age was significantly and positively related to PEx, despite the relatively narrow age span of the present material (Fig. 3). In a previous study on 17 subjects, a positive correlation between PEx and age was found,(4) whereas another study of a similarly small number of subjects showed inconclusive correlations between PEx and age.(6) The relationship between PEx and age is in agreement with data showing increasing closing volume with age.(25–27) Closing volume is admittedly not a measure of the number of airways that close and open but indicates the volume at which a massive amount of closure occurs. Nevertheless, there is probably a rough relationship between the magnitude of closing volume and the amount of airway closure, thereby explaining the association between age and PEx. Thus, considering the present results and the reasonable mechanism, we feel confident in that the association between PEx and age is real and causally connected.
FEV1 (% pred), that is, corrected for sex, age, and height, correlated positively to PEx (Fig. 4, left panel). High FEV1 (% pred) may be due, for example, to relatively high lung elastic retraction forces, but it is not apparent why this quality should result in more airway closure and opening or less deposition of produced particles.
The effects of bronchodilation (Fig. 4 right panel) were significantly and negatively related to PEx/L and PEx/Exhalation, notwithstanding the limited effects of bronchodilation among these healthy subjects. There were, for example, four subjects only with ΔFEV1 (%) >10%. An effect of a bronchodilator signifies increased tonus of the bronchial muscles. A relatively high ΔFEV1 may therefore indicate increased stiffness of the airways before the bronchodilation, that is, when the PEx measurements were obtained. Stiff airways may conceivably reduce the amount of airway closure. An alternative explanation could be that the amount of small airways available for closure and opening is dependent to airway tone such that diminished bronchoconstriction makes it easier for closed airways to be reopened. Anyhow, the effects of bronchodilation should be interpreted with caution.
Mean particle weight was positively correlated to age and FEV (% pred) (Table 4), indicating that the particle size distribution is slightly shifted toward larger particles with increasing age and lung size. The explanatory power (adjusted R2) is, however, very low, 5%. More detailed knowledge of effects on particle size distribution is warranted.
The predictors considered in the present study explained 28%–29% of the interindividual variation. Thus, there is considerable unexplained variance. The number of terminal bronchioles that close and open may be very different between subjects. If, for example, the airway closure and opening processes in one subject is located mainly in airway generation 15 and in another subject in airway generation 18, the number of airways that close and open will differ by a factor 8,(28) other circumstances will equal. Furthermore, the number of airways that close and open of a given airway generation may vary considerably among subjects, and also, the particle production of a given airway opening may vary depending on viscoelastic and surfactant properties of the RTLF.(16,29)
It is also important to note that the particles are produced during inhalation and hence inhaled before being exhaled and that differences in exhaled particle number concentrations may be due to differences in production or deposition of produced particles or most likely both. Small variations of the procedures, for example, the breath hold time at residual volume or the inspiratory and expiratory flow rates will also influence the results, despite the standardization. As opposed to the study by Wurie et al.,(18) we found no association with environmental factors, for example, pollen season or outdoor temperature.
Meaningful within-subjects variation is unfortunately not available in the present study. It is our impression from isolated observations of PEx of laboratory members that the intraindividual variation is relatively low in most subjects who are familiar with breathing maneuvers and the differences in inhalation and exhalation flow between each breath are small, but may be very high in occasional subjects. Schwarz et al. reported an average intraindividual CoV of 35% based on three measurements, two within the day and one within a month, of a standardized tidal breathing maneuver of 57 subjects.(17) The range of CoVs was unfortunately not presented. A large intraindividual variation in some subjects may contribute to cause the large variation between subjects.
Interestingly, the number concentration of exhaled particles has been found to be reduced in COPD(21) and in asthma,(30) presumably indicating that inflammation or destruction of small airways affects the extent of airway closure and opening and/or increased airway deposition of produced particles.
There are many limitations of the present study. The standardized breathing maneuver could possibly have been more rigorous, particularly in terms of flow rates. Also, comparison with a quite different breathing maneuver, for example, tidal breathing, would have been of interest and perhaps more physiological. The age interval in the present material is relatively small, in particular older subjects would have been important. Reference equations based on 126 subjects will be uncertain, in particular the 5th and 95th percentiles. A more detailed analysis of size distribution would have been interesting.
In conclusion, the interindividual variation of exhaled particle amount is considerable among middle-aged healthy subjects performing a standardized breathing maneuver and a minor part only is explained by age and anthropometric and spirometric variables. The amount of produced particles is probably closer related to particle number concentration per exhalation than to particle number concentration per exhaled liter.
Footnotes
Acknowledgments
This research was supported by the following funding organizations: the Swedish Heart-Lung Foundation, the Swedish Research Council Formas, the Swedish Research Council for Health, Working life Welfare, and Swedish Asthma and Allergy Foundation.
Author Disclosure Statement
Anna-Carin Olin is a shareholder and board member in the PExA AB. Björn Bake, Evert Ljungström, and Annika Claesson are shareholders in PExA AB.